
Abstract
Purpose
Transforaminal epidural steroid injections (TFESI) are commonly used to treat patients with lumbar spinal stenosis. It is the aim of our study to prospectively evaluate the effectiveness of TFESI using subpedicular and Kambin's triangle approach in patients with radiculopathy due to lateral recess stenosis.
Methods
Participants undergoing TFESI were randomized into two groups: the subpedicular approach group (n = 24) and the Kambin's triangle approach group (n = 24). The primary outcome measure was the numerical rating scale (NRS) pain score at 3 and 6 weeks post-injection. A ≥50% reduction in the NRS pain score from baseline indicated a successful therapeutic effect. The secondary outcome measure was the requirement of surgery at 6 months post-injection.
Results
All participants reported a significant reduction in the NRS pain score at 3 and 6 weeks after the injection (P < 0.05). The proportion of patients who experienced pain reduction ≥50% in the Kambin's triangle approach group was higher than that in the subpedicular approach group at 3 and 6 weeks post-injection. The difference was statistically significant at 3 weeks (P < 0.05) and borderline significant (P = 0.057) at 6 weeks. There was no significant difference in the proportion of patients eventually requiring surgery at 6 months and the complication rate between the two groups.
Conclusions
These results suggest that TFESI using Kambin's triangle approach is more effective in providing short-term pain alleviation for patients with radiculopathy due to lateral spinal stenosis.
Keywords
Introduction
Lumbar spinal stenosis is a common, benign, debilitating condition associated with degeneration of the spine and a significant cause of disability in the world.1,2 It refers to the narrowing of the central spinal canal, lateral recess, or intervertebral foramen, 3 resulting in compression of associated neurovascular structures. The lateral recess constitutes the entrance zone for lumbar nerve roots entering the nerve root canal, which is confined by the annulus of the disc anteriorly and the superior articular process posteriorly. 4 Lateral recess stenosis commonly manifests as radicular pain in the lower extremities as well as neurological symptoms, including sensory loss and muscle weakness in the lower extremities. 5 The development of symptoms is believed to be due to a combination of mechanical compression, inflammatory irritation of neural elements, vascular congestion, and segmental instability.6,7 Therefore, transforaminal epidural steroid injection (TFESI) can serve as a reasonable option for short-term symptom relief or bridge therapy to surgery for patients who fail conservative treatment. 8 The TFESI is a procedure performed under fluoroscopic guidance designed to deliver corticosteroid preparation to the immediate vicinity of a targeted lumbar nerve root via the intervertebral foramen. Two principal techniques are available for TFESI in patients with lateral recess stenosis: the subpedicular approach and Kambin's triangle approach. Subpedicular approach refers to an injection performed to the neural foramen at the exit zone of the compressed nerve root, while Kambin's triangle approach refers to an injection performed to the neural foramen at the compression level. 9 Few studies have investigated the ideal injection approach and level in lateral recess stenosis. Therefore, it is the aim of our study to prospectively evaluate the effectiveness of TFESI using subpedicular and Kambin's triangle approach in patients with radiculopathy due to lateral recess stenosis.
Material and methods
Participants
Local institutional research Ethics committee approval was obtained for this prospective randomized controlled study. Patient recruitment and data collection were performed from May 2016 to December 2017 at a single hospital. All participants were provided with written and verbal information on the trial before obtaining their written consent. They were diagnosed with radiculopathy as a result of impingement of the traversing nerve root within the lateral recess based on clinical manifestations and magnetic resonance imaging findings and had failed conservative therapy, including at least 6 weeks of physiotherapy. Patients were excluded if they had symptomatic central canal stenosis, symptomatic contralateral lateral recess stenosis, dynamic instability on flexion/extension radiographs, cauda equina syndrome, use of anticoagulant agents, cutaneous disorders around the injection site, uncontrollable medical or psychiatric illness, and previous adverse effects from local anesthetics, contrast medium, or steroids. A total of 48 patients with unilateral lateral recess stenosis were enrolled in this study and were assigned to the subpedicular approach and Kambin's-triangle-approach groups, comprising 24 patients each by permutation randomization using lottery. This was a single-blinded study in which only the participants were blinded to the group allocation. Patient's demographics and preoperative imaging findings were detailed at the initial clinical evaluation. None of the patients was lost to follow-up.
Interventions
Transforaminal epidural steroid injection was performed as a day procedure in the operation theater under fluoroscopy guidance by orthopedic surgeons who were experienced in spine surgery. All patients were placed in the prone position, and local anesthetic was administered. The C-arm was rotated obliquely at the neural foramen to allow a perpendicular needle tract toward the target injection site. In the subpedicular approach, the intended injection site lies underneath the pedicle, medial to the lateral border of the vertebral body, and lateral to the target exiting spinal nerve. In the Kambin's triangle approach, the target injection site lies underneath and medial to the exiting nerve root, lateral to the superior articular process, and above the superior endplate of the inferior vertebral body. In both cases, a 22-gauge spinal needle was then advanced to the target under fluoroscopic guidance. Correct needle tip position was verified by anterior–posterior and lateral radiographs. Injection of 1–2 ml contrast material was used to ensure epidural flow of contrast with no intravascular, intradural, or subcutaneous infiltration. A mixture of 40 mg Methylprednisolone acetate and 5 mg Levobupivacaine was then slowly injected (Figures 1 and 2). Finally, the intact spinal needle was removed. Operation details and complications were documented by the operative surgeon.
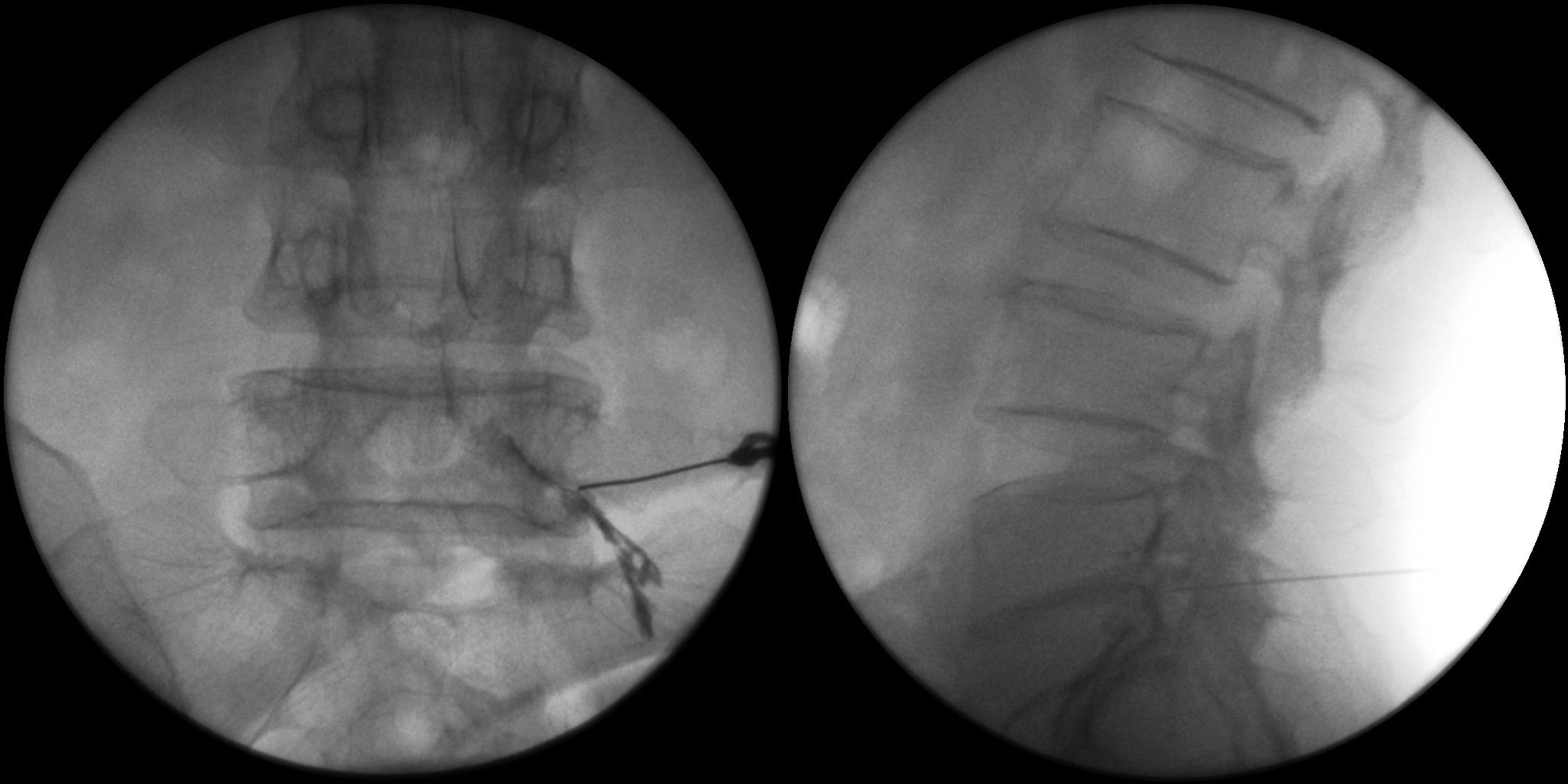
Subpedicular approach to the L5 nerve root. Fluroscopy showing the proper location of the needle at the base of the pedicle in the anterior–posterior view and at the antero-superior aspect of the intervertebral neural foramen. Contrast injection confirming epidural spread.
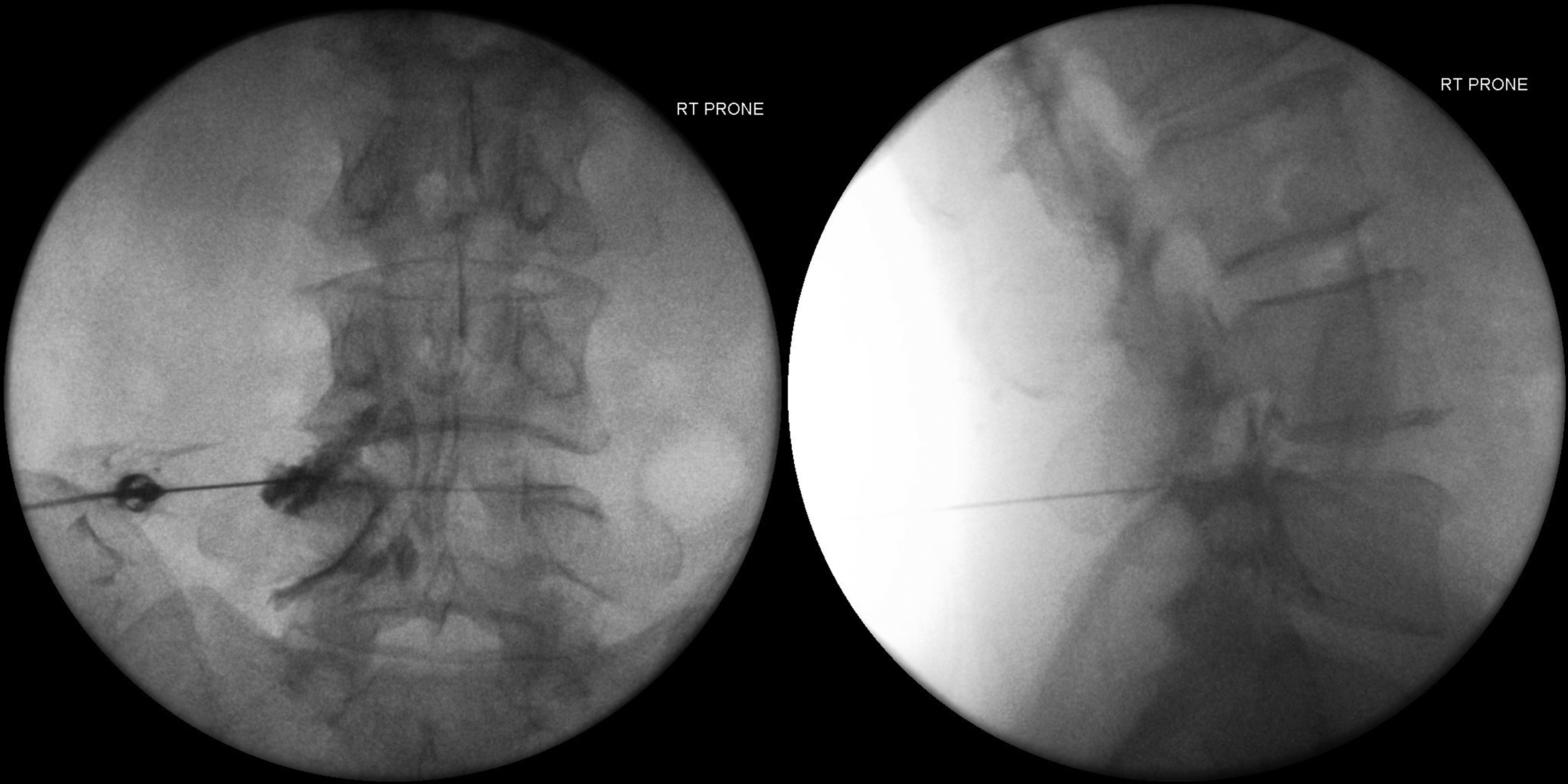
Kambin's triangle approach to the L5 nerve root. Fluroscopy showing the proper location of the needle between the lateral and midpedicular line in the anterior–posterior view and at the postero-inferior aspect of the intervertebral neural foramen. Contrast injection confirming epidural spread.
Outcomes
Pain severity, which is the primary clinical outcome, was measured using an 11-point numerical rating scale (NRS) at pre-op, 3 weeks, and 6 weeks after the procedure. The NRS was scored from 0 to 10, where “0” represented no pain and “10” represented the worst possible pain. A ≥50% reduction in the NRS pain score from baseline indicated a successful therapeutic effect. Patients who eventually required surgery, whether decompression alone or with spinal fusion at 6-month time, were recorded.
Statistical analysis
An appropriate sample size was determined based on the previously reported pain relief rate of TFESI.10,11 With a significance level of 0.05, a power of 80%, and an allocation ratio of 1:1, it was estimated that 22 patients in each group were required. 12 Taking into account a 10% dropout rate, each arm would need to include 24 patients. Comparison of numeric parameters between the treatment groups was performed using the independent t-test. The Chi-square test and Fisher's exact test were used to compare the differences in categorical variables between the groups. Changes in pain score relative to the baseline were analyzed using the paired-sample t-test within each group. A P-value <0.05 was considered statistically significant. All statistical tests were performed using Statistical Product and Service Solutions software (SPSS Inc., Chicago, IL, USA), version 26.0.
Results
The current study included 48 patients with unilateral symptomatic lateral recess stenosis. The patient group consisted of 22 men and 26 women with an average age of 58.2 (range: 24–73). L4/5 was the most commonly affected level of lateral recess stenosis (n = 40, 83%), and the average pre-procedure pain score was 7.5 (range: 5–10). There were no statistical differences between the Subpedicular and Kambin's approach groups in terms of age, gender, level of stenosis, duration of symptoms and the baseline NRS pain score. The clinical and demographic characteristics of the study population are shown in Table 1.
Clinical and demographic characteristics of the study population.
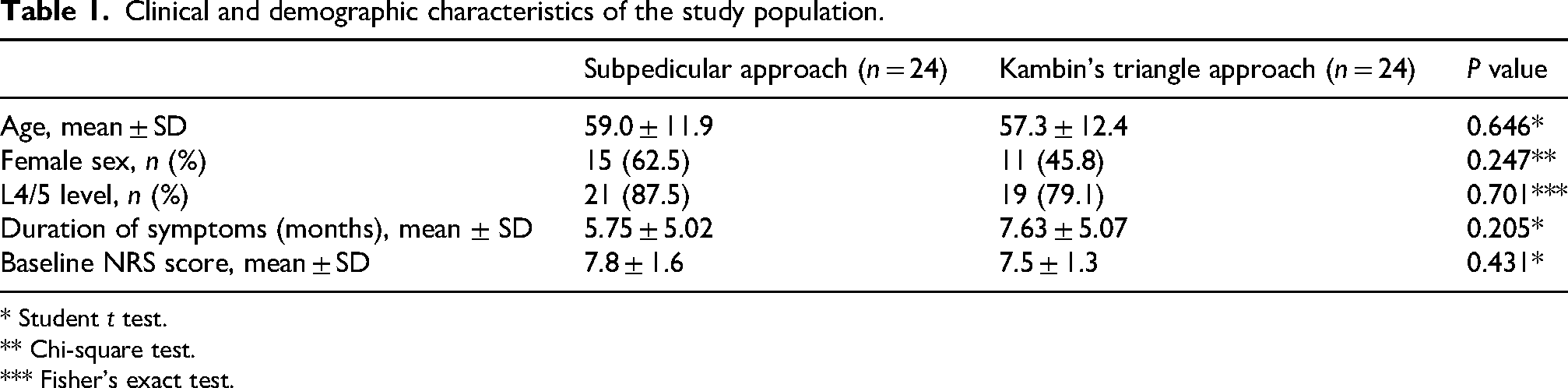
* Student t test.
** Chi-square test.
*** Fisher's exact test.
In both treatment groups, the NRS pain score reduced significantly at 3 and 6 weeks after the injection (P < 0.05). Both post-injection NRS pain scores of Kambin's triangle approach group at 3 and 6 weeks were found to be lower than those of the subpedicular approach group. However, the differences were not statistically significant. The proportion of patients who experienced at least 50% improvement in NRS pain score was 79.2% and 70.8% at 3 and 6 weeks after injection, respectively. When comparing the two treatment groups, the proportion of patients who experienced pain reduction ≥50% in the Kambin's triangle approach group was higher than that in the subpedicular approach group at 3 and 6 weeks post-injection. The difference was statistically significant at 3 weeks (P = 0.03) and was borderline significant (P = 0.057) at 6 weeks. There was no significant difference in the proportion of patients eventually requiring surgery at 6 months between the two groups. The comparison results are summarized in Table 2.
Comparison of patient outcome after the procedure in the subpedicular approach and Kambin's triangle approach groups.
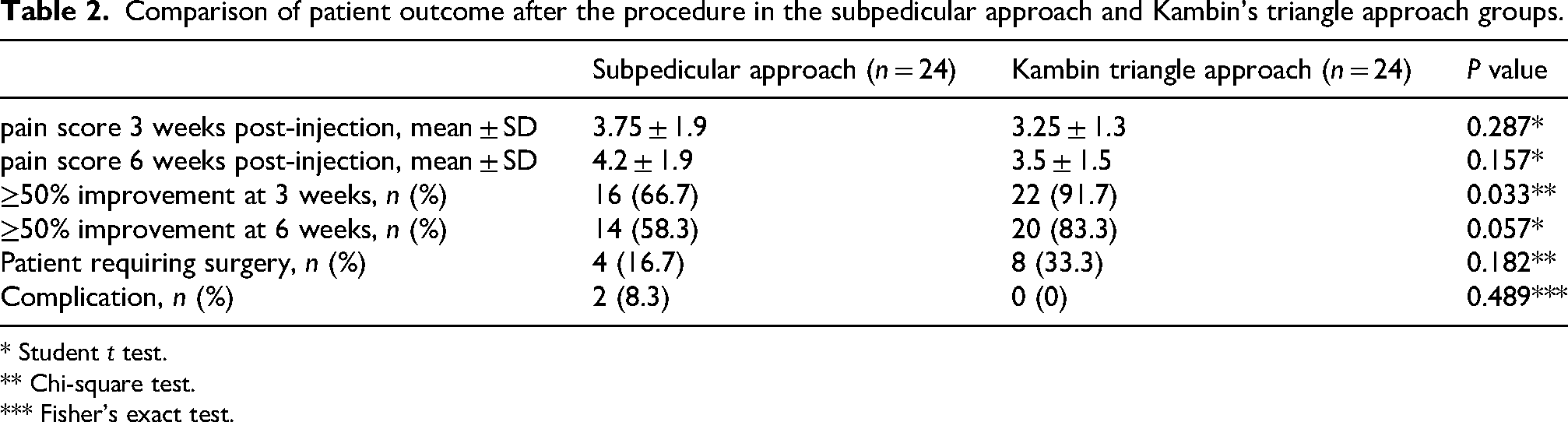
* Student t test.
** Chi-square test.
*** Fisher's exact test.
There were two instances of nerve prick when performing the subpedicular approach; however, the difference in complication rate was not statistically significant (P = 0.49).
Discussion
The results of this randomized trial suggest that Kambin's triangle approach is more effective than the subpedicular approach in providing short-term pain alleviation in patients with lateral recess stenosis. However, the differences decrease over time.
The TFESI is an effective treatment modality for pain relief and functional improvement in patients with spinal stenosis13,14 It is believed to provide pain relief by suppressing pro-inflammatory cytokines, blocking nociceptive C fibers, and decreasing edema around the nerve root.15,16 In the present study, our cohort shows a ≥50% reduction in pain in 79.2% of patients at 3 weeks after TFESI, which is comparable to that of previous studies.17,18 It has been theorized that, in contrast to the subpedicular approach, utilizing Kambin's triangle approach allows injectate to be placed closer to the site of neural impingement and to address the primary pathology directly. 9 Several studies have evaluated the effects of TFESI using Kambin's triangle and subpedicular approach in patients with lumbar stenosis. Lee et al. retrospectively reviewed 33 patients and reported that the Kambin's triangle approach has a borderline better therapeutic effect on lumbar radiculopathy than the subpedicular approach. 19 In the prospective trial by Park et al. that compared Kambin's triangle approach versus subpedicular approach, no significant differences in pain or functional improvement were observed between the two groups during the 12-week follow-up in patients with lumbar radicular pain. 20 However, the study by Park et al. included both foraminal stenosis and lateral stenosis in their analysis. We are one of the few randomized controlled studies that demonstrate Kambin's triangle approach is more effective than the subpedicular approach in treating lateral recess stenosis. 21
As demonstrated in this study, despite a difference in short-term pain relief, the rate of subsequent operation in the groups was similar. This is expected as TFESI does not alter the ultimate need for surgery, 22 especially in patients with significant mechanical compression where surgical decompression is required. With that said, given the high rate of immediate response, the current study still supports TFESI as an antecedent procedure to definitive spinal surgery. Regarding the safety of Kambin's triangle approach, Park et al. also reported less instances of nerve prick with Kambin's triangle approach, similar to the results of the current study. In the event of severe foraminal stenosis, epidural adhesions or marked disc degeneration, accessing the epidural space through Kambin's triangle could potentially be safer with less irritation to the exiting nerve root.
There are several limitations of this study. First, this is a single-center study with a relatively small sample size, so our study may have been underpowered and failed to detect smaller differences in efficacy. This can be the reason why the difference in successful outcomes between the two approaches at 6 weeks was found to be borderline significant with a P-value just above 0.05. Second, additional functional outcome assessments such as the Oswestry Disability Index were not evaluated, which can provide a more complete picture of the clinical outcome of the injection. Third, the patients were followed up only for a limited time after the procedure; hence, only the short-term results were evaluated.
Further studies should be conducted to overcome the aforementioned limitations. These studies should include more patients, include more outcome measures, and have a longer observation period.
Conclusion
In conclusion, the results of our study support that TFESI with Kambin's triangle approach is more effective than the subpedicular approach at short-term follow-up for patients with radiculopathy due to lateral recess stenosis.
Footnotes
Ethics approval
This study received institutional ethics committee approval (Reference number: KW/FR-16-075(98-18)). Written informed consent was obtained of all patients before entering the study in accordance to the guidelines of the institution with which all the authors are affiliated. There is no identifiable information about participants revealed in this submission.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Tung Wah Group Hospital Research Fund.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.