
Abstract
Background
Cervicogenic headaches are common, persistent headaches that usually start when you move your neck. One symptom is numbness or tingling on one side of the neck; other symptoms include a loss of mobility, stability, and function.
Objective
The study aims to explore the efficacy of pressure point release in patients with CGH as a separate illness.
Design
A double-blinded, randomized controlled trial study.
Participants
Fifty-two female patients with chronic cervicogenic headache, aged 20–45 years, experiencing neck pain and headache were randomly assigned to two groups: the experimental group (A) will receive pressure point release on the sternocleidomastoid muscle, while the control group (B) underwent a traditional cervical pain management program. All evaluations were conducted before and following 4 weeks.
Results
Significant reduction of pain and increased neck function with improved posture stability in both groups after treatment was obtained, with better improvement in group A.
Conclusion
The manual pressure point release technique was helpful in the treatment of patients with CGH.
Keywords
Introduction
Common headaches caused by problems with the cervical spine include cervicogenic headaches (CGHs), which manifest as pain in the head and sometimes the neck as well. Estimates put the number of people affected at 2.5% overall and 17.8% of chronic headache sufferers. 1 Middle-aged individuals, especially women, are more predisposed to CGH, characterized by unilateral headaches devoid of lateral shift and pain that intensifies with neck movements or atypical postures. 2 CGH is a secondary headache predominantly defined by pain elicited by pressure to the super-posterior neck, accompanied by a limited cervical spine (ROM). 3
The headache originates from cervical nociceptive structures, including the facet joints, intervertebral discs, muscles, fascia, ligaments, the atlantoaxial joint, and the atlanto-occipital joint. 4 CGH’s pathogenesis may stem from multiple structures in the cervical spine; the convergence of afferent signals from the upper three cervical nerves onto the 2nd-order neurons in the trigeminocervical nucleus in the upper cervical is likely to precipitate the headache. 5
CGH is a unilateral cephalalgia that varies in intensity with head movement, typically transitioning from the occipital region to the frontal area. It is characterized by significant severity, restricted cervical motion, cervical and thoracic subluxations, impaired proprioceptive balance, and altered neck flexion resulting from tightness in the sternocleidomastoid muscle. 6 Individuals who experience CGH also suffer from illness, including poor balance and reduced postural stability via peripheral mechanisms. 7
An intraarticular corticosteroid injection at the zygapophyseal joint is noted to provide no significant advantage; chemical neurolysis is forbidden because of the dissemination of neurolytic agents and potential severe adverse effects, including paralysis and deafferentation pain, thus necessitating the execution of percutaneous radiofrequency (RF) neurotomy for the management of chronic cervical zygapophyseal joint pain. 8 Trigger points are regions inside a muscle that have entered a state of spasm or cramp, resulting in a palpable lump. This condition constricts the muscle, impeding blood circulation and leading to an accumulation of metabolic waste and a deficiency of oxygen, rendering the area poisonous and exacerbating muscle spasms and tightness, thereby causing a “lock on” phenomenon. 9
Recent therapeutic approaches have explored the effectiveness of targeting pressure points, particularly in the SCM muscle, as a non-invasive treatment strategy for CGH. This technique involves the application of manual pressure to specific points within the SCM muscle to alleviate muscle tension, reduce referred pain, and improve overall function. The rationale behind this approach is based on the concept that pressure on these points can deactivate trigger points, leading to an interruption of nociceptive input and a subsequent reduction in headache symptoms. 10
The author’s hypotheses are that (a) there is no effect of pressure point release of SCM on CGH patient’s VAS scores, (b) there is no effect of pressure point release of SCM on neck disability index scores in CGH patients, (c) there is no effect of pressure point release of SCM on overall stability scores in CGH patients.
This paper aims to explore the current evidence supporting this treatment modality, examining its physiological basis, clinical efficacy, and potential as a therapeutic option for individuals suffering from cervicogenic headache, to relieve CGH pain, neck disability index, overall stability, and cervical ROM.
Methods
This research was a double-masked, randomized controlled experiment that adheres to all CONSORT standards and presents the requisite information properly. The Faculty of Applied Medical Science Ethics Committee sanctioned the research at Umm Al Qura University, KSA (HAPO-02-K-012-2025-01-2463), and registered it as a clinical trial (NCT06733896). The study was completed in the Department of Physical Therapy at the Faculty of Applied Medical Sciences from December 2024 to January 2025. All individuals executed a permission form before their registration in the study.
Participants
A neurologist referred 52 female patients, aged 20 to 45, from the outpatient clinic of the Umm Al Qura University Department of Medical Rehabilitation Sciences, who were diagnosed with chronic cervicogenic headache (CGH) according to (IHS) criteria. The inclusion criteria were as follows: office worker, permanently employed or enrolled in studies, motivated to keep employment, motivated for rehabilitation, and suffering from persistent or recurring neck pain and balance abnormalities for at least 6 months. Specific cervical spine disorders such as post-operative cases, a history of trauma, spasmodic torticollis, frequent migraines (occurring more than two times/month), nerve entrapment, fibromyalgia, shoulder diseases, rheumatic diseases, severe psychiatric disorders, and conditions that impede physical exertion, temporomandibular disorder (TMD)/orthodontic before enrolling in the study, the states were screened based on their medical histories and clinical examinations.
Randomization
Before the study, all participants reviewed and signed a consent form with assurances of anonymity and confidentiality, and all procedures adhered to relevant laws and institutional standards. A computer-based randomization program randomly assigned all participants into two groups: Experimental Group A (26 participants): All participants in Control Group B (26 patients) underwent manual pressure on the sternocleidomastoid (SCM) and manual exercise. A researcher, blinded to participant recruitment and care, conducted the allocation, and patients were unaware of their assigned group (Figure 1). Flow chart diagram.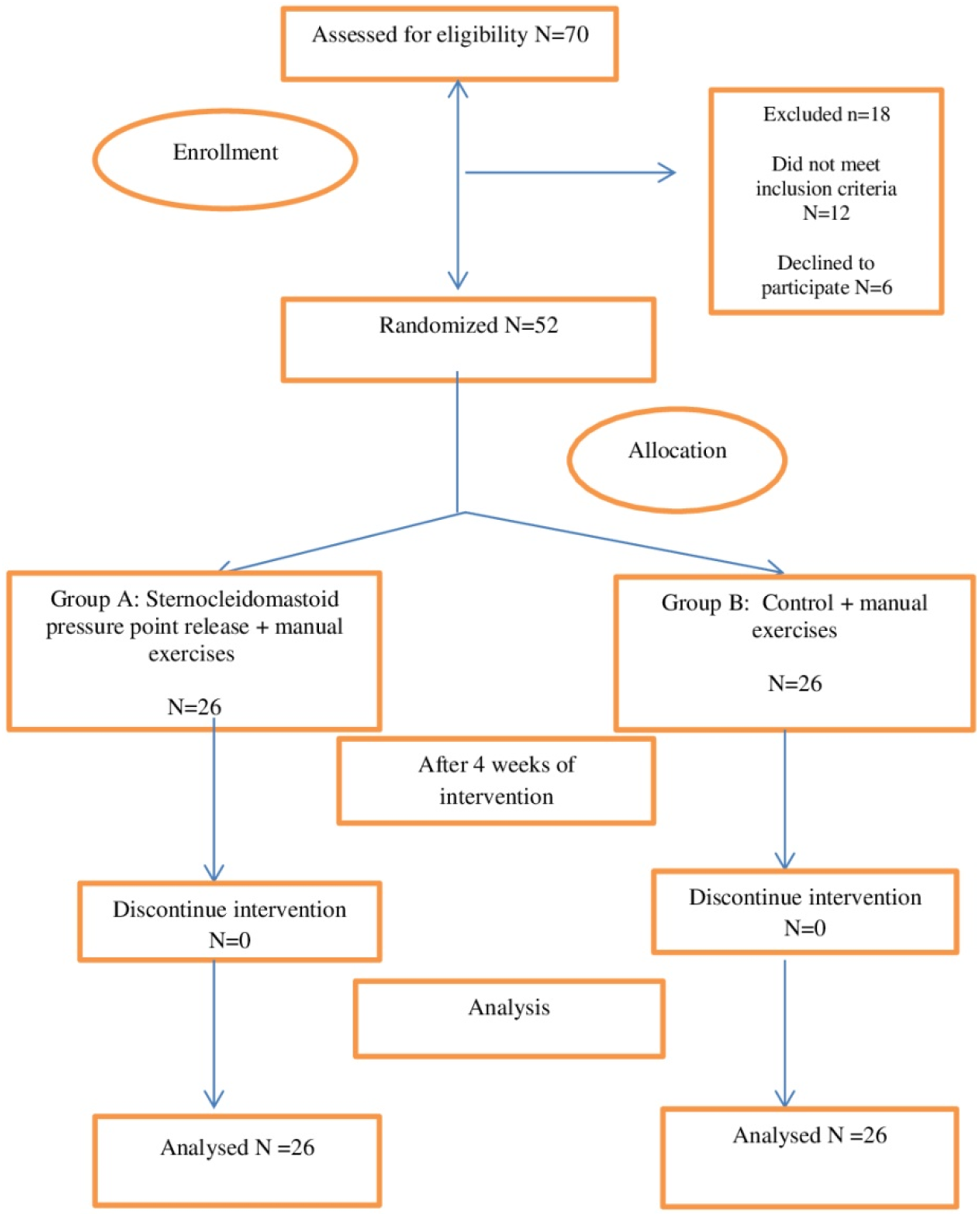
To eliminate type II error, the sample size was calculated using G*POWER statistical software (version 3.1.9.2; Franz Faul, Universitat Kiel, Germany). 11 It was determined that 26 participants per group was the appropriate sample size for this study. Calculations were performed with allocation ratio N2/N1 = 1 with α = 0.05, β = 0.2, and effect size (Cohen’s d values) = 0.8.
Outcome measures
All measures were performed at the baseline and after 4 weeks. • Primary outcome: Pain is a subjective psychological and physiological phenomenon, necessitating precise assessment and the appropriate execution of interventions essential for successful pain management.
12
- The visual analog scale (VAS) is a proven Arabic tool for measuring pain. It is used to inscribe a mark on a 10-cm line that signifies a continuum from “no pain” to “worst pain.”
13
• Secondary outcome: posture stability and neck function: (1) Biodex Balance System: An evaluation of postural stability was conducted, selecting level eight (the most stable level), followed by choosing the dynamic (LOS) testing mode, after which the results for each were input into the device. The patient was directed to attain a centered posture on the platform by adjusting their feet after the platform. Visual feedback was displayed on the screen, with the patient’s movements moving the cursor. After centering the cursor, the platform was maintained in a level position beneath the patient’s feet while the patient stood comfortably erect.
14
(2) The neck disability index (NDI): This is a patient-completed, valid Arabic version of a self-reported functional questionnaire having 10 items: pain, personal care, lifting, reading, headaches, concentration, work, driving, sleeping, and recreation. Each item is scored on a scale of 0–5, with higher scores indicating greater self-reported disability status. The score on this questionnaire may vary from 0 to 50. To compute a percentage, multiply the final result by two.
15
Interventions
Sternocleidomastoid (SCM) pressure point release techniques
The SCM can form taut, non-contractile bands known as trigger points that may radiate discomfort to other areas. The trigger point referral locations for the SCM include the eye, forehead, occiput, anterior neck, cheek, and lateral head. Trigger points were addressed via various manual procedures such as. • Deep stroking massage and ischemic compression technique. A deep stroking massage lasting 10 minutes and ischemic compression entails applying sustained pressure for 2 minutes every application, repeated five times. These procedures were implemented in the middle of the sternocleidomastoid muscle, a prevalent site for trigger points and soreness. The acupoints utilized for alleviating localized muscle spasms and enhancing nerve nutrition are approximately located at the level of the thyroid cartilage (Adam’s apple) in the neck and at the endpoints of the sternocleidomastoid muscle
16
(Figure 2) • Positional Release Therapy (PRT) is applied to the sensitive areas of the sternocleidomastoid (SCM) muscles. It suppresses sensitive sites that cause local discomfort (tender points) by applying pressure to these spots and passively maintaining the muscle in question in a relaxed position for 90 seconds four times, for around 8 minutes.
Four minutes of relaxation between deep stroking, ischemia compression, and PRT. Each therapy session lasts around 40 minutes thrice weekly for 4 weeks. The technique of pressure point release of SCM muscle.
Manual exercises
All patients were evaluated by a clinically qualified physical therapist specializing in manual therapy and treated by another physical therapist with comparable qualifications. The same physical therapist who did the original evaluation reassessed the patient after completing treatment. The suggested procedure included the following techniques: Hot packs were applied to the patient’s neck for 4 minutes before beginning the workouts. The sternocleidomastoid (SCM) muscles were then stretched individually, followed by 4 minutes of isometric strengthening exercises for neck flexion, lateral bending, and rotation.
Statistical analysis
An unpaired t-test was implemented to evaluate the subject characteristics of the two groups. The Shapiro-Wilk test was employed to verify the normal distribution of the data. Levene’s test was implemented to assess the homogeneity of variances between groups. The effects of pain, NDI, and overall stability were compared within and between groups using a mixed-design MANOVA. Post-hoc tests were conducted for successive multiple comparisons using the Bonferroni correction. The significance level for all statistical tests was established at p < 0.05. The statistical application for social studies (SPSS) version 25 for Windows (IBM SPSS, Chicago, IL, USA) was employed to conduct all statistical analyses.
Results
Subject characteristics
Basic characteristic of participants.
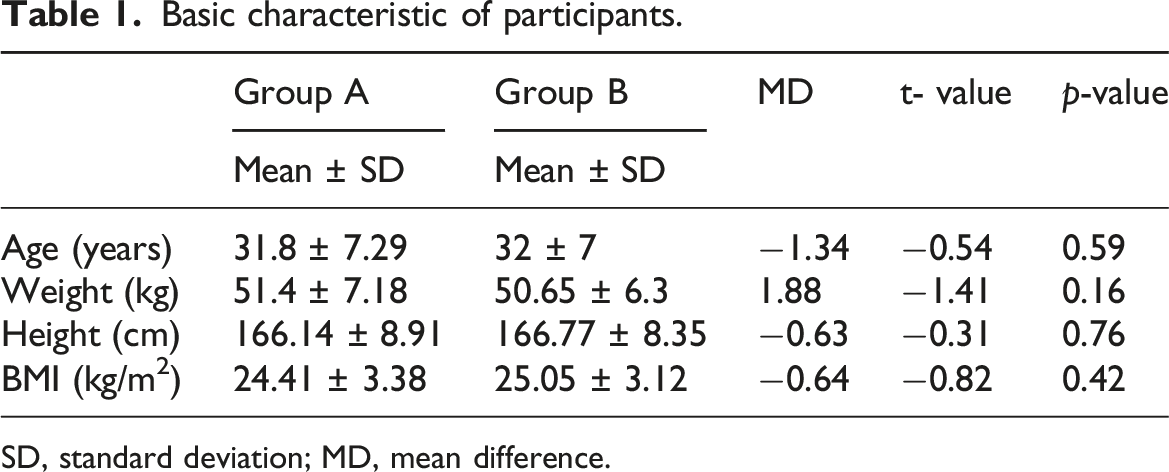
SD, standard deviation; MD, mean difference.
Effect of treatment pain, neck disability index, and overall stability
There was a significant interaction of treatment and time (F = 31.23, p = 0.001,
Within-group comparison
Mean values of VAS, NDI, and overall stability pre and post-treatment of groups A and B.
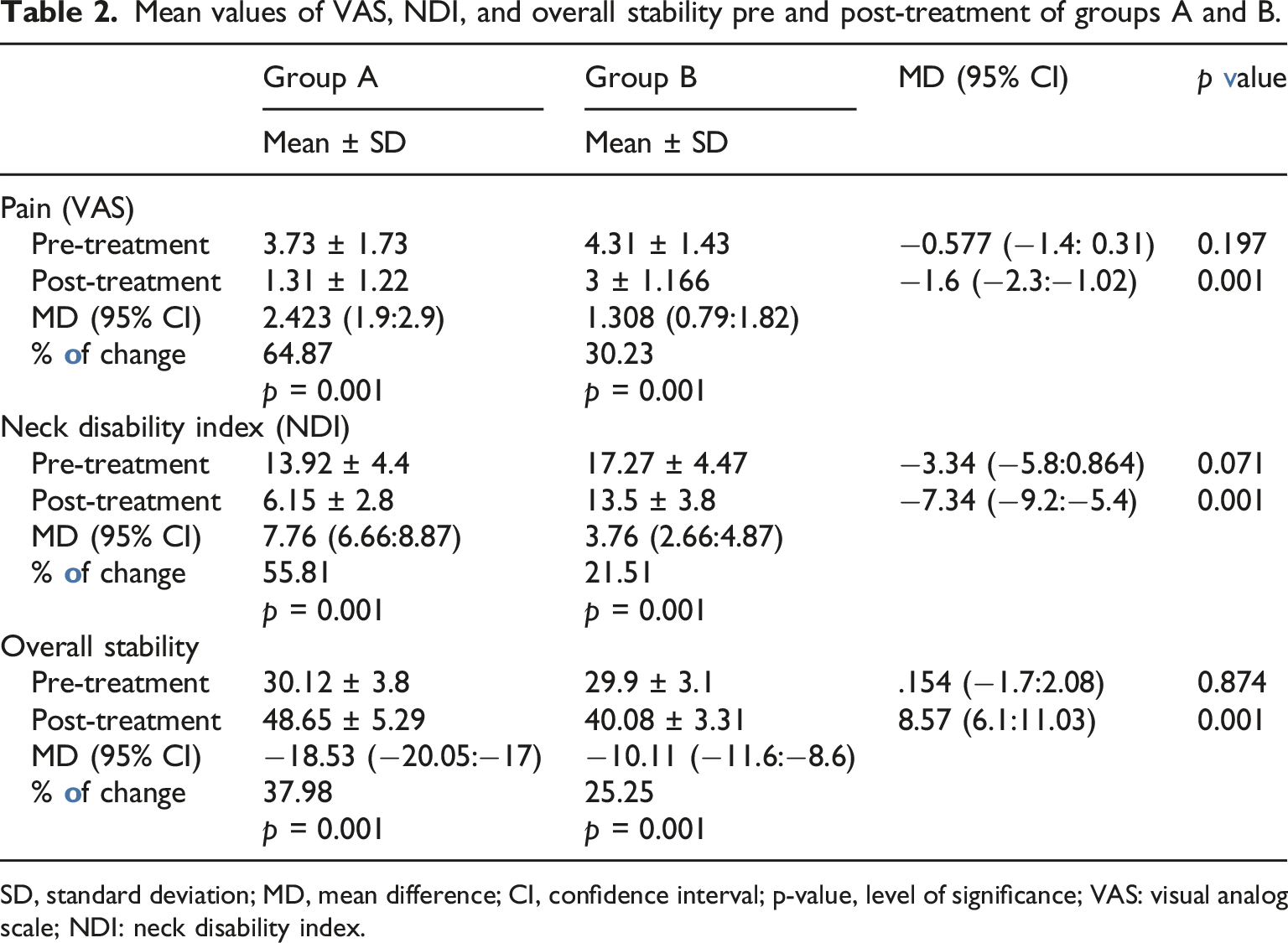
SD, standard deviation; MD, mean difference; CI, confidence interval; p-value, level of significance; VAS: visual analog scale; NDI: neck disability index.
Between-group comparison
Shows effect size of the outcome measures.
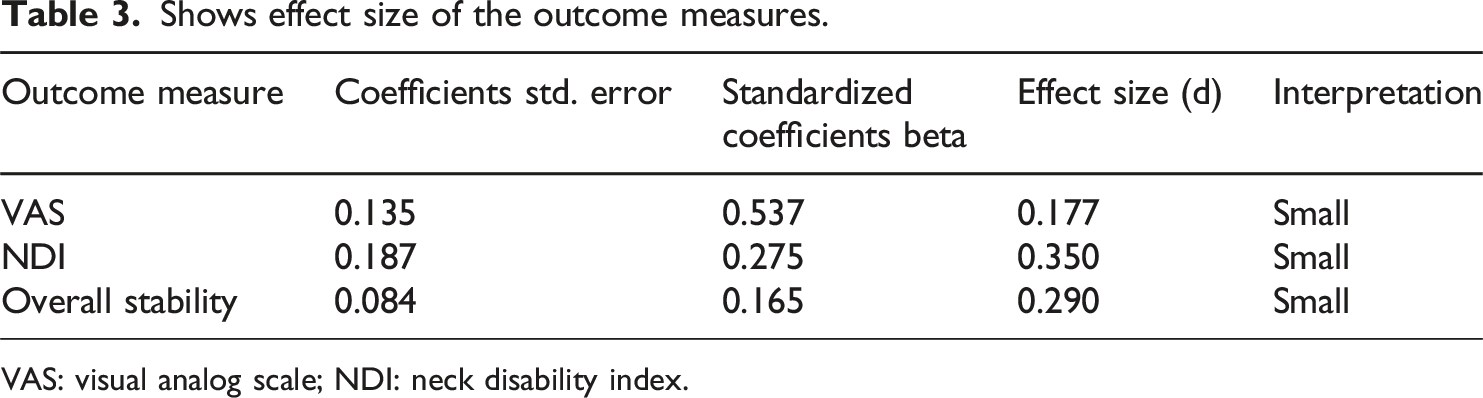
VAS: visual analog scale; NDI: neck disability index.
The authors note the significant differences between groups in the grouped bar chart to visualize the pre and post-differences in Figure 3. Shows pre- and post-differences between both groups.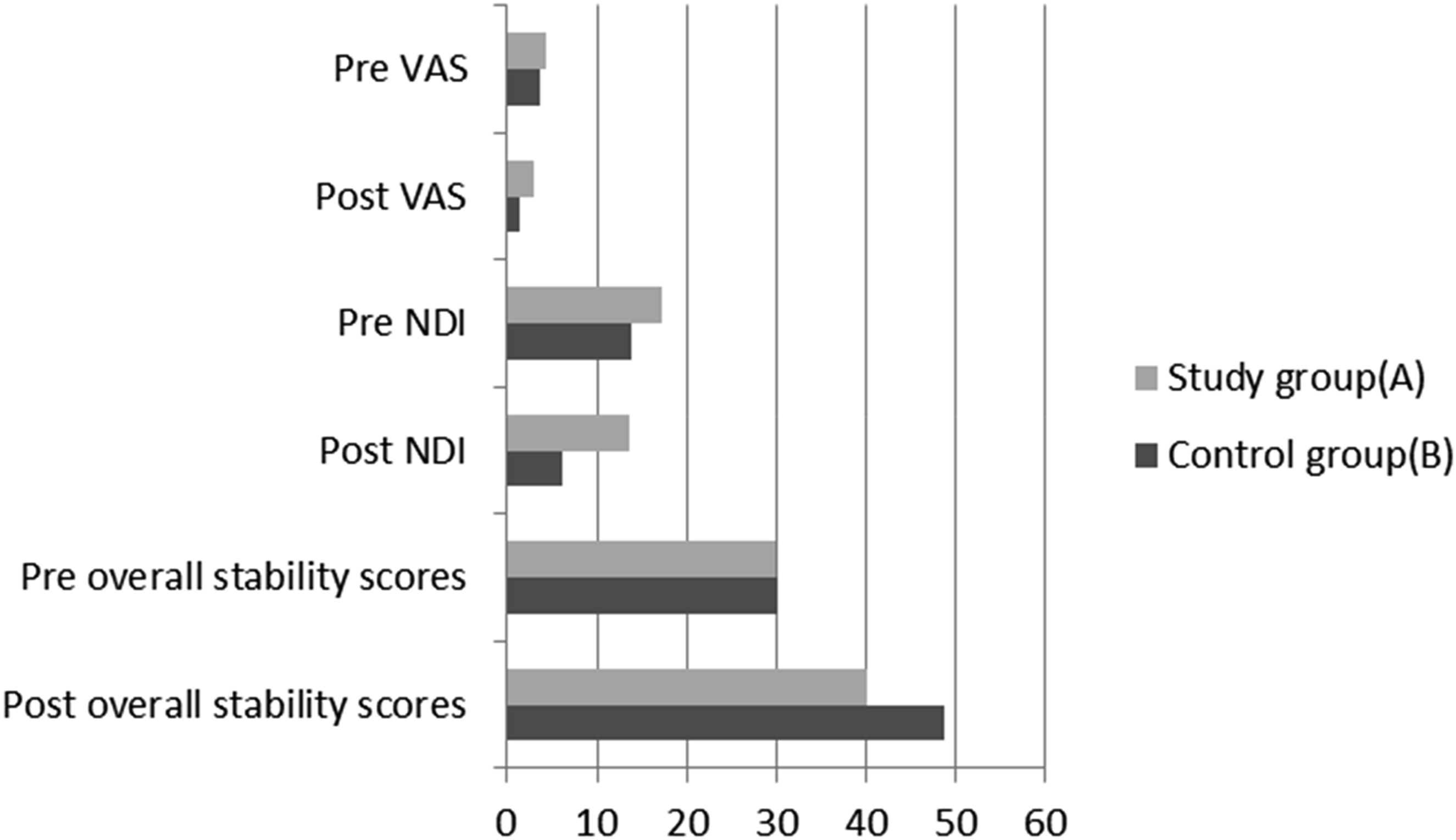
Discussion
The present study aimed to evaluate pain, cervical function, and stability limits following SCM manual pressure in patients with CGH. The within-group comparisons revealed statistically significant reductions in discomfort (p < 0.001 across all measures); these results align with previous studies demonstrating a statistically considerable enhancement in postural stability and neck function.
In a previous study, stretching with muscle endurance and strength reduced headaches and upper extremity discomfort by 58% in the strength group, 70% in the endurance group, and 21% in the control group. 17
Our findings corroborate those of Büyükturan et al., who discovered that stretching and massage administered to the SCM muscle, in conjunction with traditional physiotherapy, can alleviate pain and impairment while enhancing range of motion and endurance. 18
A parallel investigation revealed that applying pressure to the trigger points of the upper trapezius muscle and the sternocleidomastoid muscle, both innervated by the same nerve, effectively enhanced the neck range of motion and alleviated discomfort. 19
Additionally, Sbardella et al. 20 published a comprehensive review in 2021 that assessed the clinical efficacy of manual pressure release (MPR) of neck muscles combined with (MET) for neck discomfort. The outcome measures were tested 15 times after the intervention, including neck pain using the VAS scale, functional disability using the (NDI) Questionnaire, and neck rotation range, which showed that MPR and MET were equally effective in relieving pain, increasing neck disability, and improving range of rotation in people with non-specific neck pain.
In addition, the observed increase in postural stability may be attributed to a comprehensive improvement in balance and proprioception as a result of long-term MET application to the suboccipital muscles, indicating that manual therapy combined with a behavioral approach is recommended for achieving superior balance and proprioception outcomes. 21
Moreover, Peolsson et al. 22 demonstrated that postural stability, a component of static balance, refers to the capacity to sustain erect in the horizontal plane around the (COM) while standing. Various factors influence it, including spatial orientation, movement strategies, and sensorimotor processes. Neck-specific exercises enhance cervical intramuscular coordination and sensorimotor function, affecting postural sway and improving general stability.
Simultaneously, the discharge of trigger points in the sternocleidomastoid muscle results in an enhancement of postural stability. Peng et al. 23 investigated the physiology of motor coordination and balance, which are indispensable activities in daily life that require precise perception of the head’s position in 3D space. The cervical spine is equipped with a highly sensitive proprioceptive system that coordinates the vestibular and visual systems, conveys the head’s position relative to the trunk, and is essential for regulating balance and posture. Proprioceptive information from cervical muscle spindles and mechanoreceptors in cervical discs and facet joints is integrated and transmitted to the central nervous system to regulate the head position and overall body posture. The alignment between sensory information and motor performance can be facilitated by enhancing neck musculature through manual treatment.
Besides, Xia et al. 24 indicated that (ESWT) and manual therapy (MT) on trigger points of the sternocleidomastoid muscle were equally beneficial in alleviating pain, enhancing functional neck capacity, and diminishing muscular stiffness in patients with cardiogenic headache (CGH).
On the other hand, some studies do not agree with these results. Bodes-Pardo et al. (2013) indicated no significant difference in headache relief between patients who received sternocleidomastoid muscle pressure point therapy and those who did not. The authors suggest that while manual therapy might offer temporary relief, it does not address the underlying causes of cervicogenic headaches. 25
Moreover, Martín-Rodríguez et al. (2019) highlighted the lack of robust clinical trials supporting the exclusive use of sternocleidomastoid pressure point techniques. They argue that more comprehensive studies are needed to establish the efficacy and safety of this method. The review suggests that focusing solely on this technique might lead to overlooking other effective treatment options, thus questioning its standalone effectiveness. 26
Furthermore, a systematic review by Núñez-Cabaleiro et al. (2022) analyzed various manual therapy techniques, including SCM pressure point therapy, to treat cervicogenic headaches. The review indicated insufficient high-quality evidence to support the effectiveness of SCM pressure point therapy. The authors emphasized the need for more rigorous randomized controlled trials to substantiate efficacy claims and better understand the mechanisms through which SCM pressure points might exert their effects. 27 Another pertinent study by Olesiejuk M. et al. (2025) examined the potential adverse impact of SCM pressure point therapy. The study highlighted that patients often reported increased sensitivity and discomfort in the neck region following treatment, which sometimes exacerbated headache symptoms instead of alleviating them. The authors concluded that the pain associated with the pressure points could outweigh the potential benefits, questioning the overall utility of this approach in managing cervicogenic headaches. 28
The authors explain their results that the SCM muscle is a prominent neck muscle that plays a key role in the movement and stabilization of the head and neck and is involved in both flexion and lateral rotation of the neck. Dysfunction or tension in this muscle can lead to restricted neck movement and increased strain on cervical vertebrae, potentially triggering headaches; pressure points in the SCM muscle can effectively reduce muscle tension, which is often a contributing factor to cervicogenic headaches. Releasing this tension can result in decreased headache frequency and intensity.
The present study possesses certain limitations. The limited sample size must be acknowledged since it may affect the repeatability and representativeness of the research findings. Second, given that our follow-up duration was 4 weeks, we cannot ascertain the long-term effects of the intervention. The patients’ subjective influence must be considered, as they were aware of their therapies. Additional research with extended follow-up and bigger sample size, focusing on active release trigger points of the SCM muscle in cervicogenic headache, is necessary to enhance clinical practice guidance.
Conclusion
SCM pressure points might effectively reduce pain, increase neck function, and improve posture stability in patients with CGH.
Footnotes
Author contributions
All authors confirm their authorship according to the international ICMJE criteria (all authors contributed significantly to the conception, study design, and preparation of the article read and approved the final version before publication). Special contributions:
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Details of previous presentation of the research
This research is original, has not been published or reviewed for publication before and is not currently being considered for publication elsewhere.
Data Availability Statement
The datasets generated during and/ or analyzed during the current study are available from the corresponding author on reasonable request.
Implication for physical therapy practice
The findings of the randomized controlled trial on the effectiveness of sternocleidomastoid muscle pressure points in patients with cervicogenic headache have significant implications for physical therapy practice. These results suggest that targeted pressure point therapy on the sternocleidomastoid muscle can be an effective non-pharmacological intervention for alleviating cervicogenic headaches. Physical therapists can incorporate this technique into their treatment plans to provide relief for patients suffering from this condition. By integrating pressure point therapy, therapists can offer a holistic approach that may reduce dependency on medication, thereby minimizing potential side effects and promoting overall patient well-being. This approach can enhance the treatment repertoire of physical therapists, leading to improved patient outcomes and satisfaction.