
Abstract
Patient-oriented research is increasingly recognized as an important methodology in health sciences. Benefits of patient engagement include aligning research priorities to those living with health conditions, developing better recruitment strategies and protocols, and integrating findings more meaningfully. However, for research teams to work well with patient-partners, training for all stakeholders is needed. While training exists, none consider the uniqueness of the neuromuscular disease experience. To address this gap, our team of researchers, clinicians, and patient-partners collaborated to increase the capacity for patient-engagement in neuromuscular disease research. Our methods included: 1) conducting a landscape of available resources, and 2) using adult education principles and a backwards design process to develop unique training modules. The result is an online platform with three modules focusing on the neuromuscular disease context, addressing the inclusion, diversity, equity, and accessibility needs of those with neuromuscular diseases, and building teamwork skills. Early evaluation of the first two modules indicates high satisfaction and knowledge gain. Through this process, we have learned about the barriers of patient-oriented research, how to support the required system culture shift, and how to plan for long-term sustainability.
Keywords
Highlights
Patient-engagement is important to build relevant and purposeful research knowledge, especially in rare and neuromuscular diseases
Capacity building is needed for the whole team, including researchers, clinicians and patient-partners to create meaningful engagement
We present the co-development of an online, neuromuscular-specific patient engagement training
Uptake of patient engagement is enhanced by considering sustainability for training modules, providing funding to support consequential engagement at the start of projects, and requiring patient-partnerships in grant competitions
Introduction
Over the past decade, the participation of individuals with lived experience in research has undergone significant evolution. There is now a strong emphasis on patient-oriented research (POR), a collaborative approach that actively engages patients, family members, and caregivers as integral partners throughout the research process. Essentially, POR means conducting research with patients rather than for patients, 1 thus ensuring that health research stays relevant and focused on improving outcomes that matter most to patients. 2
Involving patient-partners is increasingly recognized as essential for high-quality health research. Benefits of this approach are highlighted in a 2019 review of studies conducted through the Patient-Centered Outcomes Research Institute (PCORI), which found an increased uptake in patient engagement, contributing to research that is more aligned with the needs of patients and clinicians. 3 The integration of patient-partners into health research lies at the convergence of two key ideas: 1) the concept that “research is care”, and 2) the “nothing about us without us” principle widely embraced by the Disability Rights Movement.4–6 This approach emphasizes the importance of including individuals with lived experience in the decision-making processes of research, ensuring that their perspectives are integral to shaping health outcomes and policies. 7 This represents a paradigm shift away from traditional research models, which treat patients as passive subjects, and instead emphasizes the inclusion of lived experiences and perspectives as essential to the research process. Unlike the term “patient,” which typically refers to an individual receiving medical care, the term “patient-partner,” describes someone with lived experience of a particular disease, either as a person directly affected, a family member or as a caregiver. A patient-partner collaborates and/or participates in decision-making roles within various health research contexts, from serving on grant review panels, advisory councils, to participating as an embedded member of a research team. This may involve prioritizing research ideas, and/or participating in study development, measurement selection, participant recruitment, data analysis, and dissemination of findings.8–10
Numerous components are needed to ensure meaningful patient-partner contributions throughout the research process. Careful planning is essential to maximize benefits, reduce risks, and ensure success. 5 Crucial elements include establishing trust and respect and fostering genuine relationships amongst all team members.11–14 Additional considerations range from practical aspects, such as scheduling team meetings, 15 to issues of justice, such as ensuring diverse voices are represented, 13 and philosophical questions about the nature and ownership of knowledge. 12 Importantly, for POR to be effective, patients and researchers need to develop the necessary skills and competencies for this type of partnership to work. 11
Capacity building needs to be considered and supported for effective patient engagement in research. 9 Training is recommended to cultivate successful collaboration, recognizing the diversity of experiences and needs within the research team.8,9 Specifically, training should strive to build a “collective competence” in POR, nurture relationships and team dynamics, and foster a culture of co-learning to enhance team readiness. 14 Researchers require skills to support patient-engagement and participatory approaches, group processes, and effective communication.11,16,17 Training programs for patient-partners should emphasize how to leverage lived experience in planning projects and disseminating findings, while deemphasizing the need to acquire specialized research skills. 11
There is a growing recognition and application of POR in the realm of rare diseases and neuromuscular diseases (NMD).18–20 Considering the broad spectrum of over 200 NMDs, 21 each individual brings a unique set of experiences, barriers, and challenges of their rare disease journey. Many NMDs are multisystemic disorders, affecting not only physical abilities but also mental health, cognition, endocrine, respiratory, cardiac, and bone health. As many are genetically inherited, multiple generations and other family members may also be affected by the same condition. This complexity can lead to immense economic burdens in affording treatments, medications, mobility equipment, and personal support care, resulting in social isolation.22–24 Engaging with patient-partners with NMDs is paramount to understanding this complexity. Well-intentioned researchers may not consider the day-to-day realities of those living with NMD, and this in turn may result in less meaningful research, or research procedures that are difficult to access and engage in. Those affected, along with their families and caregivers, have unique experiences which can guide research questions and clinical practice to maximally benefit patient outcomes. 25 Patient-partners provide depth and context to rare disease research, increase innovation, facilitate improved recruitment and research procedures, improve study completion rates, enhance the relevance, utility and application of research, and aid in the dissemination of information to medical and NMD communities. 3 26–28 However, despite the importance of patient engagement, few NMD research studies to date use POR methods.
Numerous POR training and capacity building supports exist for other populations and conditions.2,8,29,30 However, there are none that are specifically tailored with an NMD focus and designed to be accessible for and considerate of the unique challenges of living with an NMD. To effectively conduct POR within this population, it is imperative to develop capacity-building training that acknowledges the experiences of individuals with NMDs. This includes addressing the wide range of potential NMD related participation barriers, such as fatigue (almost all NMDs), cognitive and language understanding (e.g., myotonic dystrophy), dysarthria and respiratory illness vulnerability (e.g., spinal muscular atrophy), physical accessibility and equipment needs of many NMDs, and related caregiver assistance barriers (scheduling limitations and availability). All these challenges can limit attendance at research team meetings, reading and understanding of communications, ability to provide feedback, or attendance and participation in activities. The purpose of this project was to develop a set of online, self-directed training modules applicable to NMD research; from which patient and family partners, researchers, trainees, and others on research teams can learn about researcher-patient partnerships and discover ways to conduct research that is accessible and meaningful to individuals living with NMDs.
Methods
A dedicated multi-stakeholder team was formed to determine the learning objectives, training content and user interface. The ‘Expert Patient Capacity Building (EPCB) team’ consisted of four patient-partners (CK, CM, LN, MT), representatives from a national patient organization, Muscular Dystrophy Canada (MDC) (HO), the Neuromuscular Disease Network for Canada (NMD4C) (a pan-Canadian network connecting clinical, scientific, technical and patient experience to enhance care and research in NMD) (EB), one researcher, one clinician (KS), and one project coordinator/clinician (PM). POR principles and practices were integrated into all phases of the current project. Patient-partners on the team each had a different NMD condition with different related experiences and challenges. The full project occurred in two major phases and developed three unique modules (see Figure 1 for project flow chart and Supplemental Figure 1 for patient-partner visualization of the project). Patient-partners were involved in each phase and activity, including the identification of search terms for a landscape analysis, collection and analysis of data (i.e., resources), design of the capacity building online training modules, and implementation and dissemination of all the modules.
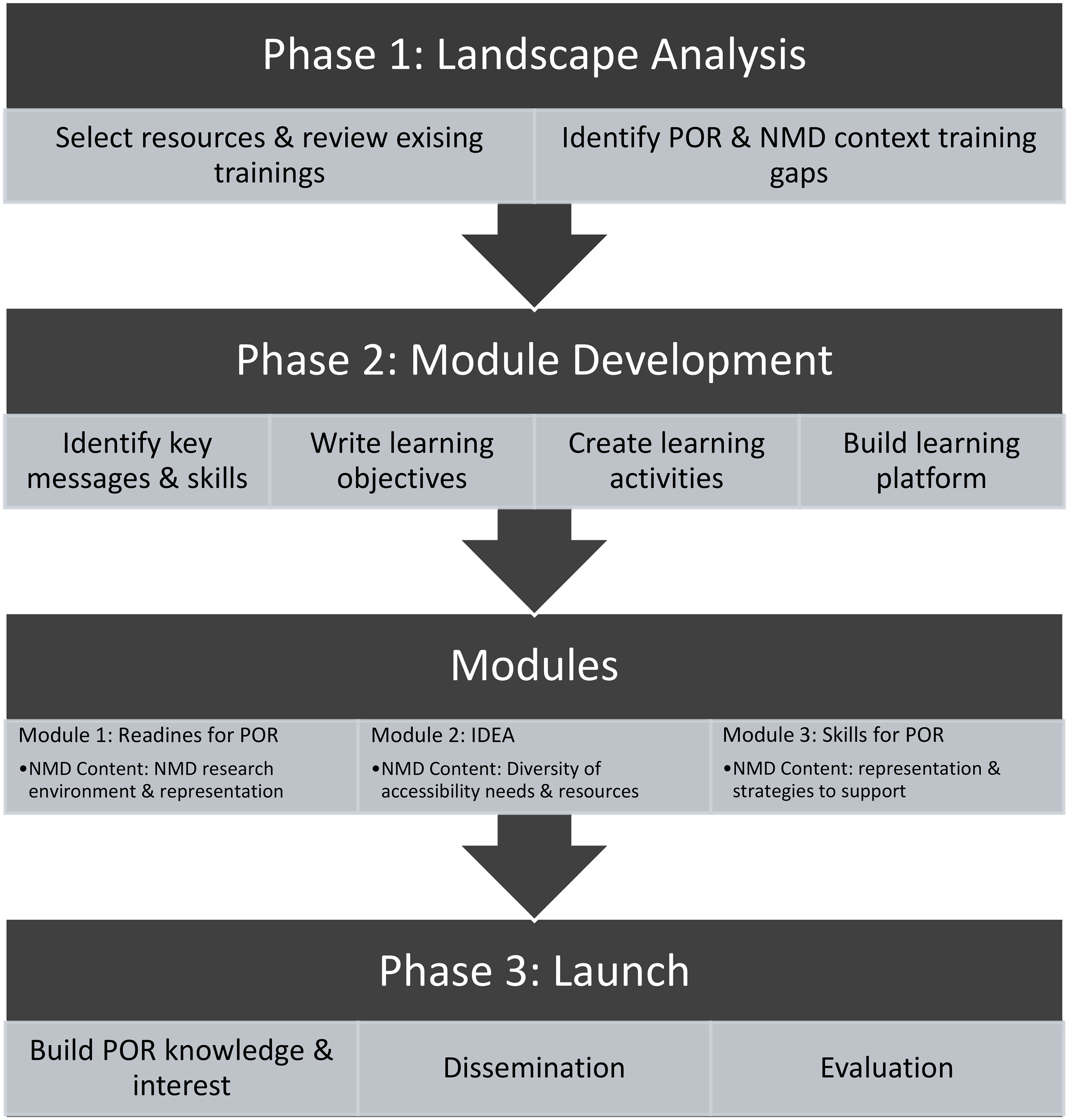
Project flow chart. Abbreviations. IDEA, Inclusion, diversity, equity, accessibility; NMD, neuromuscular disease; POR, patient-oriented research.
Phase one: landscape analysis
The goal of Phase 1 was to complete a landscape analysis of the available POR resources and best practices and to retrieve, screen, and categorize the evidence collected. The outcomes of the landscape analysis were: (a) to select relevant resources to be included in an online resources repository for POR in NMD research, and (b) to identify gaps in the existing resources that could guide the development of a new online POR capacity building training for NMD research. Search terms included: rare disease, neuromuscular diseases, capacity building, training, patient engagement, patient partner, patient participation, and/or patient-oriented research. Searched databases included: Google, Google scholar, OVID Medline, and EBSCO CINAHL, all with English language limits. The grey literature search was iterative to identify tools and resources for POR captured in workshops, conferences, websites, repositories, and other resource materials. Websites of known POR organizations (e.g., Canadian Institutes of Health Research Strategy for Patient-Oriented Research, Patient-Centered Outcomes Research Institute) were also scanned for linked resources. One author (PM) scanned, downloaded and categorized the published article citations onto a Microsoft Word document; online sources were collected and categorized on an Excel database, with two authors (CK, HO) confirming the resources and categories. This was then converted into an online resource repository on the NMD4C website.
The EPCB team discussed gaps in the existing resources in relation to rare disease and NMD research. Three team members (CK, HO, PM) used an inductive approach 31 to identify major gaps that emerged from the landscape analysis. These identified gaps were then used to inform the development of the POR capacity building training modules for patient-partners and researchers involved in NMD research (Phase 2). To build our collective skills and identify gaps in trainings, team members (CK, CM, PM, HO, MT) completed and evaluated engagement trainings available at the time, including the Patient-Oriented Research Curriculum in Child health modules 29 and the Maritime SPOR SUPPORT Unit Patient-Oriented Research Training Online Practicum. 32 Midway through our project, the Canadian Institutes of Health Research - Institute of Musculoskeletal Health and Arthritis (CIHR-IMHA) launched POR training modules which our team then reviewed.
Phase two: POR in NMD research online capacity building training development
We followed a ‘backward design process’ to develop the framework for the capacity building training. 33 Backward design begins with identifying learning needs and desired actions/skills, followed by specific learning objectives and competencies (the evidence of learning), and ends with planning learning activities to support the learning objectives. We developed our training, ‘Patient-Oriented Research Training in Neuromuscular Disease (imPORTND)’ 34 in four steps; we: (a) established the key messages and skills, (b) wrote the matching learning objectives, (c) created the learning activities, and (d) built the online platform. Adult learning principles, including offering learning choices, grounding in real life context and application, and incorporating social learning opportunities informed the development of the learning activities. 35 The EPCB team collaborated through online gatherings to discuss results of the landscape analysis, and the development, dissemination, evaluation and sustainability of the training modules. To facilitate sustainability, the evaluation process utilized the RE-AIM Framework, 36 which examines aspects of reach, effectiveness, adoption, implementation, and maintenance.
Phase three: launching the modules
As we built the modules, we embedded methods for the project launch, including knowledge translation activities, dissemination, and evaluation. This involved strategies to build awareness and interest in patient engagement prior to the launch and dissemination approaches once the modules were ready. Finally, we tracked learner participation, completion and evaluations using features of the Moodle platform.
Results
Phase one: landscape analysis
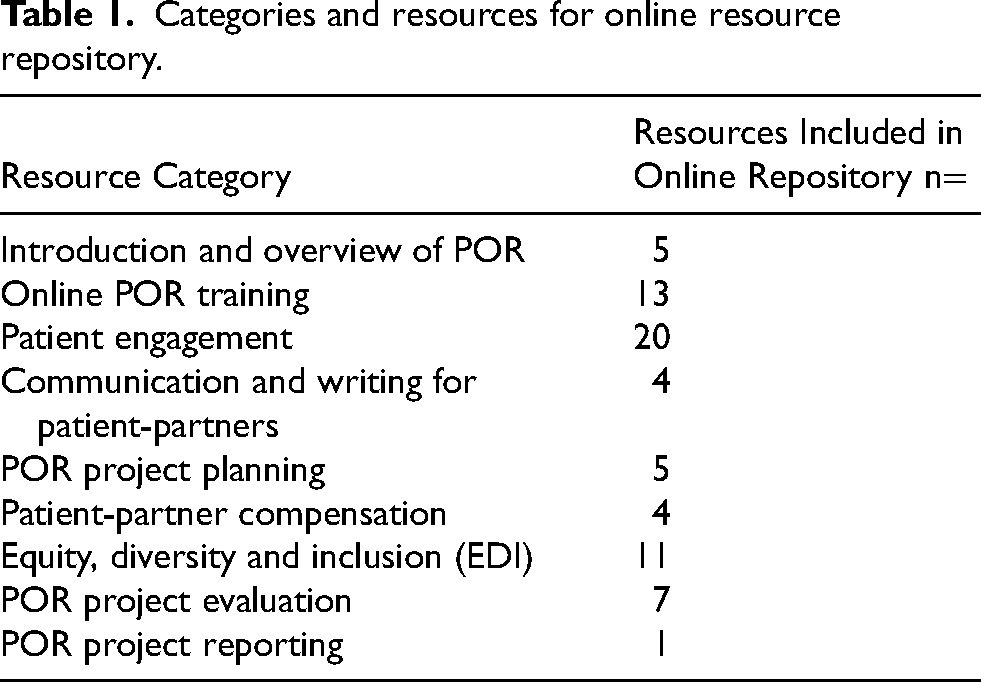
A total of 80 resources were included in the online repository (Table 1), sorted into nine major categories. The online repository serves as a library of mostly Canadian resources for stakeholders engaged in POR, including people affected by NMDs, researchers, and advocates. The repository is housed on the NMD4C website and is maintained by the NMD4C communications coordinator, together with MDC. 37
Categories and resources for online resource repository.
By consensus, we identified these gaps in the current trainings and resources: 1) NMD context and environment; 2) focus on inclusion, diversity, equity and accessibility needs (accessibility being particularly important to an NMD context); 3) consideration of motivations; 4) skills for building and working in, teams; 5) support for patients and researchers to exchange unexpected knowledge through patients sharing impactful stories and researchers listening; 6) considerations for engagement planning; and lastly7) representation and visibility, as existing POR training lacked examples featuring patient-partners with a range of disabilities, as are experienced with NMD.
The first gap specifically addressed the need to describe the complex NMD research environment. With over 200 rare conditions (some extremely rare), many different organizations and institutions involved in NMD research, creating a layered and confusing research environment. The second gap was also unique to patient engagement in the NMD context. Given the different health and disability complexities represented, supporting patient-partners to participate in research requires considering and addressing a wide range of different physical, health, and communication barriers. This extends to the importance of terminology and language-use and reflecting on unconscious biases and stigmas. The remaining gaps, while not necessarily unique to NMD, were not addressed by other resources. However, two principles made these gaps important to address, first, the need to consolidate training to make it accessible and doable, and second, the importance of representation. In a population that has had so little patient engagement in research to date and for whom many face disability discrimination, seeing oneself in a role and others appreciating the potential is critical. 38
Phase two: online capacity building training development
Step one: development of the learning objectives
The EPCB team determined the desired learning messages and key skills through discussion and consensus and incorporating the identified gaps. These were divided into three main themes that became one welcome module and three content modules (introduction to POR in NMD context; inclusion, diversity, equity, and accessibility (IDEA); and skills for POR) (see Figure 2). Key skills were developed into 22 learning objectives and competencies, some directed primarily for patient-partners, others for researchers/research teams, and some applicable to all, with the thought that certain skills, like team building, are best learned together (see Supplementary Tables 1, 2, 3). To limit duplication, the imPORTND modules were developed to complement the newly published CIHR-IMHA modules and to link to resources found through the landscaping phase.
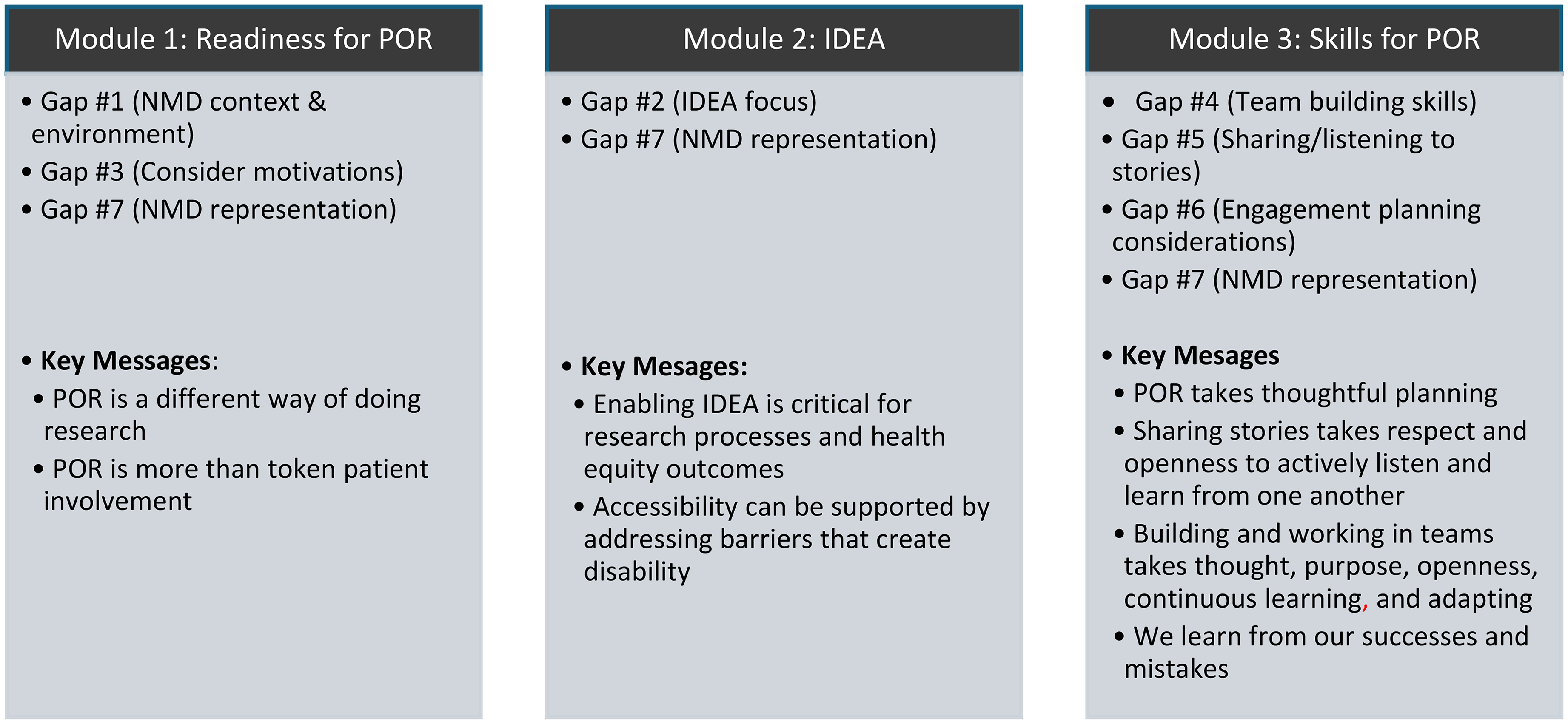
Identified gaps and key messages module themes. Abbreviations. IDEA, inclusion, diversity, equity and accessibility; NMD, neuromuscular disease; POR, patient-oriented research.
Step two: module content development
During the platform design and development of learning activities to meet the learning objectives, the team aimed to create content that was inclusive by design and responsive to the diversity of NMD accessibility needs. First, the content followed the Web Content Accessibility Guidelines 2.1, 39 an internationally recognized set of recommendations for improved web accessibility. This ensures that content is accessible to people with a variety of vision, hearing, mobility and cognitive needs. This included creating transcripts or closed captioning options for videos and adjusting font and colour usage. Second, plain language was used wherever possible to eliminate barriers to understanding, ensure optimal uptake, and to empower patient-partners. Third, representations of people living with NMD were used in examples, case scenarios and module knowledge tests. And fourth, it was determined that online training should track learning and completion of each module. Finally, we translated the full training, including video voice overs, into French to provide the training in both national languages (RE-AIM outcome: Reach).
In building our modules, we chose the Moodle platform, a free and open-source learning management system (https://moodle.org/), to host the training. Moodle's features, such as content pages, discussion boards, ability to link in external videos and content, quiz features, and ability to track participation and completion, met our need for a diversity of learning activities. Throughout content building, we used a shared Word document to track content ideas and appropriate resources, each matched to specific learning objectives, reflecting the backward-design process (see Supplementary Tables 1, 2, 3). Text, video scripts, visuals, and graphics were developed and reviewed by the team. This iterative process made best use of our different perspectives (patient, researcher, clinician) and allowed for our team to learn from each other and adjust the content to best meet the needs of mixed users. In addition, following adult learning principals, we built the modules with elements of choice and the ability to quickly revisit specific content and resources to provide ‘just-in-time’ follow-up learning opportunities. Finally, a small research group, engaging patient-partners in the creation of a core data set for Duchenne muscular dystrophy, pilot tested the first two imPORTND modules (RE-AIM outcome: Effectiveness). 40 Final adjustments were made based on feedback from this group.
ImPORTND training content and learning activities
Module 1: readiness for patient-oriented research
The first imPORTND module (see Supplementary Table 1) defines POR within a NMD context, including how lived experience can enhance NMD research. The complex NMD environment is introduced, including the key organizations that partner in health research, such as the numerous patient and research organizations, the Canadian NMD network and the Canadian NMD registry, hospitals and clinics, and universities. The different roles and responsibilities of research team members within these organizations is further explained. This module also explores the different motivations people may have in participating and engaging in research. The underlying message is that POR involves mutual trust and constant relationship building, and tips and resources are featured for how to effectively do this work. This includes a video example of a NMD researcher and a patient-partner with NMD related dysarthria in conversation about relationships in research, modelling communication and visibility. Researchers are provided practical tools to support patient-partners, including information on compensation, reimbursement and how to acknowledge and report the impact of POR in reports and papers. The module concludes with contact information for potential patient-partners and researchers to use to facilitate connections and coordination by the patient organization, MDC (RE-AIM outcome: Adoption).
Module 2: inclusion/diversity/equity/accessibility (IDEA)
Module 2 (Supplementary Table 2) presents learning to equip research teams and patient-partners with the skills and resources needed to support inclusive, diverse, equitable and accessible (IDEA) research. Rather than addressing NMD related research participation barriers by each NMD diagnosis, the team made two decisions. First, to equip users more broadly through the lens of IDEA and the social model of disability, 7 and second, to have all users complete this learning. Not all researchers and trainees understand the diversity of NMD needs, and those with lived experience of one NMD condition may not understand that of another. To start, learners are introduced to IDEA and complete an activity to prompt reflection on their biases by completing an online bias test. The module then links to teaching content about the social model of disability as a lens to consider all types of accessibility barriers. As many people with NMDs have mobility needs, learners are introduced to different types of mobility devices, and content is linked and provided to discuss how to communicate and share information with those with learning and communication needs. For researchers specifically, resources are provided to help describe the research cycle process in a plain language, accessible manner for those supporting participation of patient-partners with cognitive support needs, and an accessibility checklist of research environments and processes is available for download. 41
Module 3: skills for patient-oriented research
Module 3 (Supplementary Table 3) focuses on specific skills to help with POR. This includes how to develop an effective patient engagement plan, how to share and listen to patient stories, how to work effectively in groups, and how to evaluate the project engagement. Module 3 also provides practical information about the stages of team development along with identifying the needs for each stage and group activities to foster relationships and trust. This module also links to the CIHR-IMHA trainings. To address NMD visibility and representation in research processes, Module 3 includes a case study activity that asks participants to read a vignette about a person diagnosed with Charcot-Marie-Tooth disease and identify what matters most to them, along with the accommodations or considerations needed if they joined a research team.
Phase three: launching the modules
To build knowledge and interest for POR, the EPCB team delivered a network webinar, and presented the project ‘in progress’ at two national network meetings (RE-AIM outcome: Reach). Dissemination included email notifications to all individuals registered within MDC and NMD4C and advertising in e-blasts and newsletters using consistent graphics and messaging (RE-AIM outcome: Adoption).
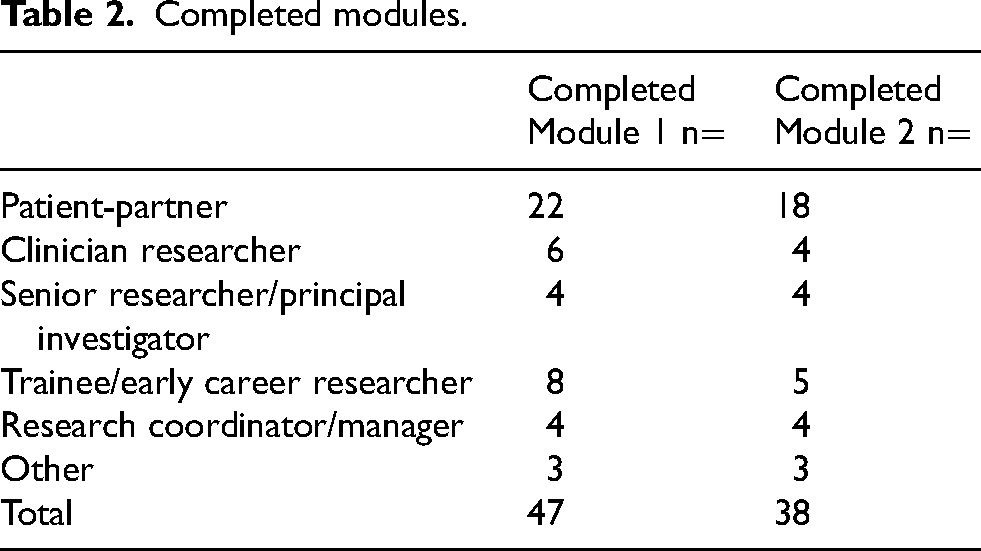
To date, 47 people have completed Module 1, and 38 have completed Module 2, with interested patient-partners the most involved, followed by trainees and early career researchers (see Table 2). Satisfaction with the training has been highly rated to date. For Module 1, 44 of 47 people (94%) agreed or strongly agreed that they knew more about POR following the module, and for 37 (79%), learning this from an NMD perspective and context, as presented in the module, was important (see Figure 3). For 42 people (89%), Module 1 took an appropriate length of time to complete and 44 (94%) would revisit the site to access the resources. For Module 2, 29 of 38 people (76%) agreed or strongly agreed that they learned more about IDEA principles through the module, and 36 (95%) reported that learning this through an NMD lens, as presented, was important (see Figure 4). The two that were either neutral or disagreed on this point were patient-partners, who may have gained this knowledge already through lived experience. For 33 people (87%), Module 2 took an appropriate length of time to complete, and 28 (74%) would revisit it in the future to access the resources.
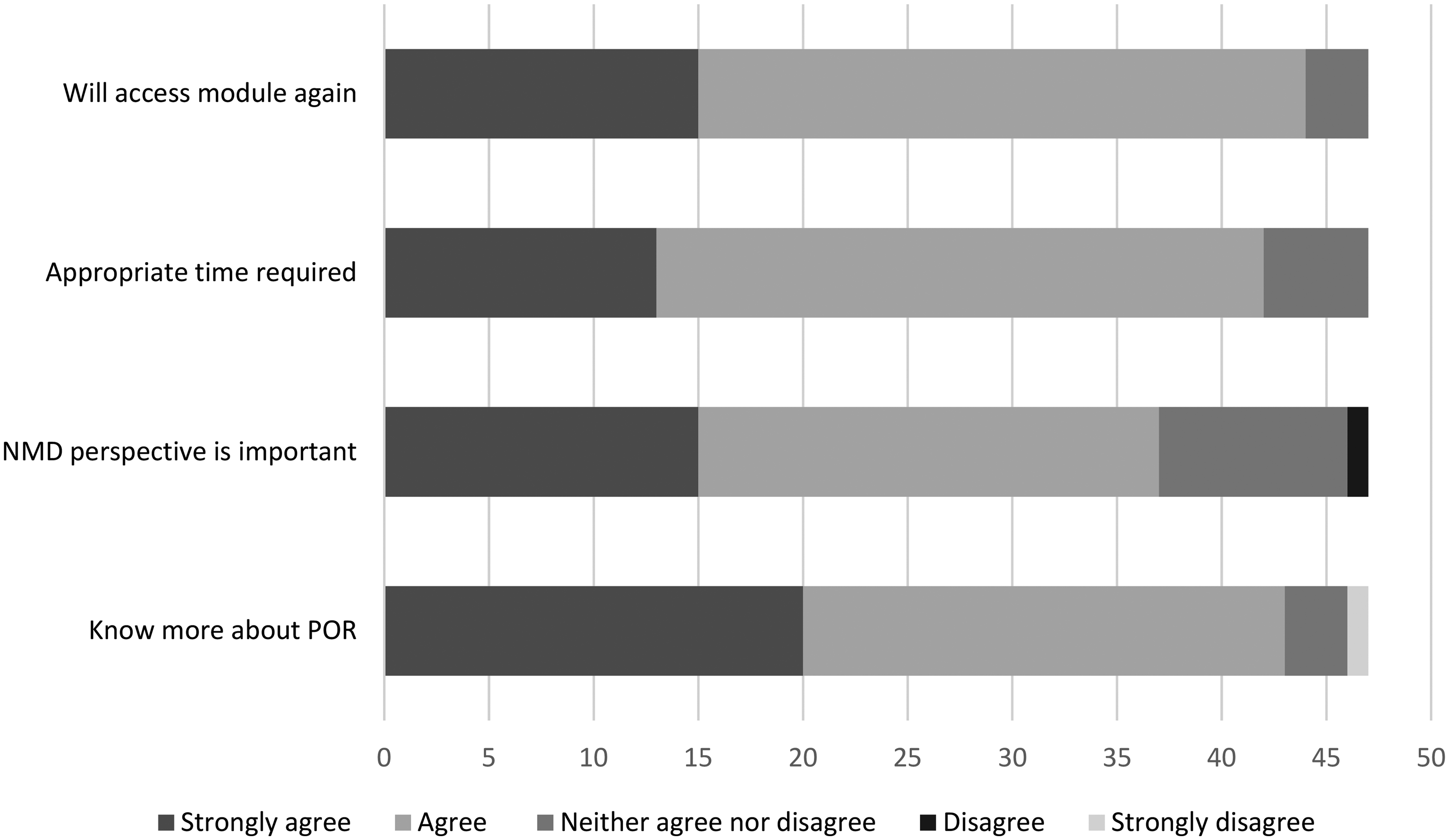
Module 1 program evaluation data.
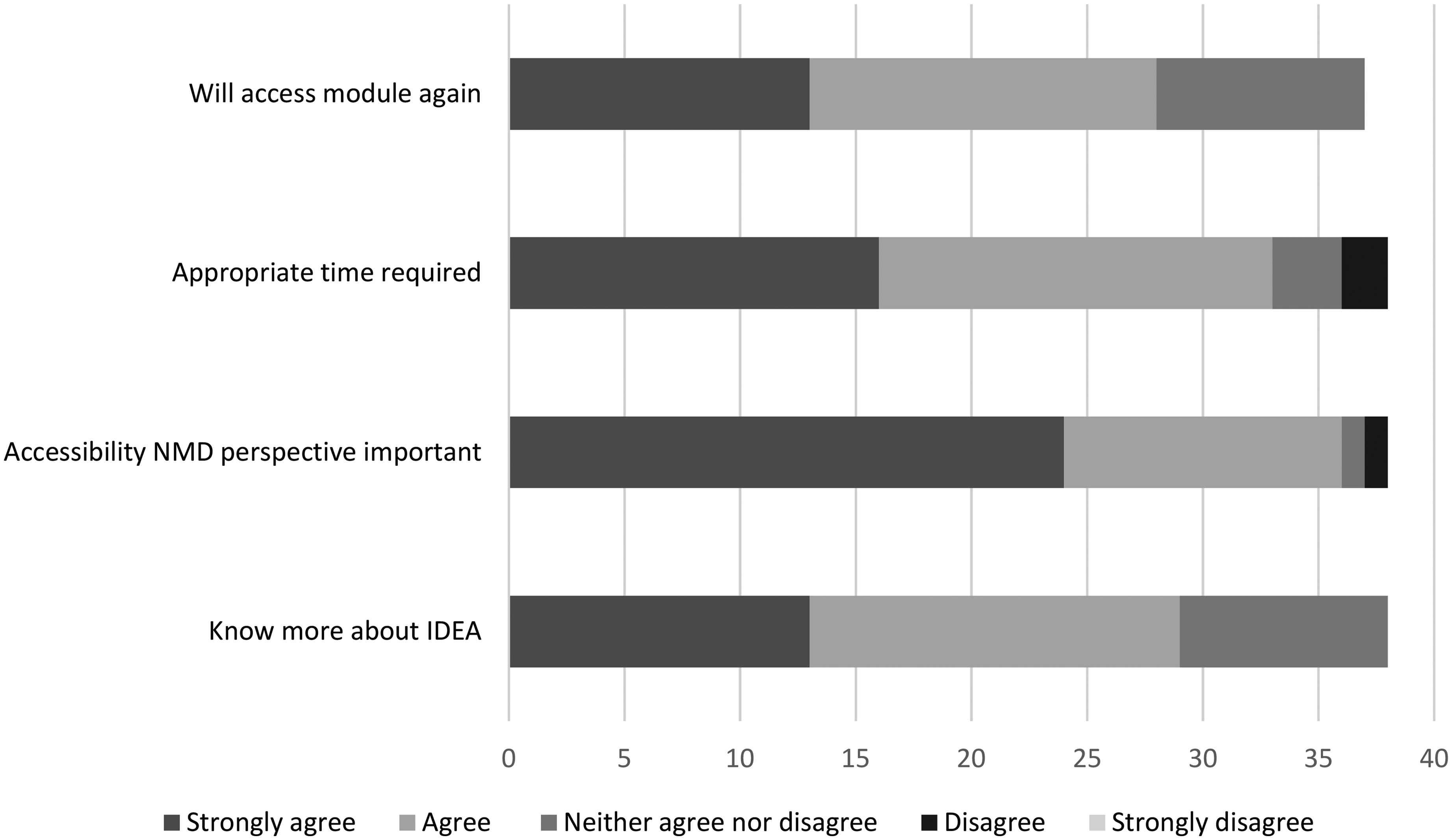
Module 2 program evaluation data.
Completed modules.
Evaluation included tracking user perceptions of the intent and meaning of the modules, and their ‘take home messages’. For patients, the learnings demonstrated a shift in research approach and opportunities. From one patient, “as a person with a neuromuscular disease, I am very happy learning how this subject is being taught, and that energy is going into being more understanding of us”. Another noted, “having a healthy relationship and communication between researchers and patients can lead to better outcomes for the research being done”. For researchers, comments focused on how including patient-partners can change research processes and outcomes. A senior researcher wrote, “we can learn so much more about research priority from the patients”, and a trainee/early career researcher noted to, “consider IDEA at the onset of research redesign, consider communication strategies to address any unique needs of your patient partners and community”. The few negative comments related to practicalities of online learning and internet connectivity, such as buffering speed to view videos. Online learning can present challenges, but one participant noted, “my attention span for online learning has decreased in the last few years but held out for this complete module”.
Discussion
Our imPORTND project addresses notable voids in patient-engagement knowledge and available resources. Initially we confirmed the lack of POR resources and optimal methodologies applicable to NMDs. We then addressed this gap by creating the first POR training modules unique to the needs of NMD patients and their research and clinical care teams. Through this work our EPCB team gained a deeper understanding of the barriers to this type of work, the research culture shift required, and how to build for sustainability.
Barriers to POR
We designed our imPORTND modules with the intention that patient-partners, and research and clinical teams build relationships and learn together through content that is reflective of all perspectives. However, there can be barriers to POR participation for both patients and professionals. Accessibility can be a challenge for patients, impacting the diversity and representation of patient-partner recruits.41,42 In addition, the complexities of living with a rare condition can limit patient involvement even further, 1 and for those living with progressive neuromuscular conditions, the impacts extend to family and caregivers. Patients and caregivers can spend considerable time advocating for research, funding, financial support, and access to treatments, leaving little time for research involvement. These sentiments are echoed in patient engagement in other rare disease research.1,16 The co-design of imPORTND mitigates some of these barriers and facilitates POR as it was developed in collaboration with patient-partners and NMD-organizations, which have diverse reach and can thus facilitate dissemination of the training program and uptake among patient-partner groups. For example, imPORTND has an entire module dedicated to supporting accessibility for patient-partners in research activities. Finally, imPORTND is self-paced and has flexible learning content, allowing all to move through modules on their own time and capacity.
Ensuring diversity of patient voices within research is important to expanding reach and applicability of research but is difficult to achieve.43,44 A survey examining the demographics of patient-partners in multiple Canadian jurisdictions and health organizations found that patient-partners are predominantly female, university-educated, white, and have a household income greater than $90,000 a year. 42 In the case of rare diseases, with small potential patient-partner pools, the same people tend to be repeatedly invited if they demonstrate interest and aptitude. In addition, founder effects seen in some NMDs create concentrated, regional distributions of specific conditions, sometimes in rural locations far from research ‘hubs’.45,46 This highlights the need to target patient engagement at regional and community levels to ensure representation of these rare conditions. Failing to include representative patient-partners can have a direct impact on the identification of research priorities and knowledge translation initiatives to reach the larger population. 16 imPORTND was developed to build the capacity and inclusion of more patient-partners so researchers are not continually involving the same patient-partners.
Barriers for researchers engaging with patient-partners include poor understanding of the purposes, meaning, and methodology of POR. Both veteran and early career researchers report having only basic knowledge of POR and only one third of researchers perceive POR as actively involving patient-partners in all phases of research.1,47 These findings imply that researchers may be unclear of the potential roles for patient-partners. In particular, patient-partner engagement in bench science remains difficult. 48 While grant competitions increasingly require patient-partner participation, few do so for basic science research. This type of research is vital for making advances in the treatment of genetically based or autoimmune NMDs. Potential patient-partner contributions in basic science research include informing priorities and proposals, developing effective recruitment strategies when needed, and/or participating in ‘lay’ knowledge translation messaging.
Partnering scientists early in their career with patient-partners may be a key strategy to increasing uptake and developing inclusive methods while infusing laboratory research with meaning. At a 2024 NMD4C basic science summer school, NMD research trainees met with patients to hear their stories. This experience helped trainees connect the meaning of their laboratory research and its impact on those living with an NMD. This resulted in a trainee-driven push for further engagement, including their completion of the imPORTND training modules, and the development of a ‘Building Bridges” learning series. This series focuses on collaboration between patient partners and researchers to ensure that scientific communication is accessible, empowering, and inclusive.
While training can increase knowledge and skills to improve POR uptake, it doesn’t address systemic barriers in research processes, funding and connecting with patients. While our imPORTND modules highlight the importance of early involvement, our team recognized a significant barrier to this ideal. Best practice includes compensating patient-partners for their time and reimbursing them for any costs incurred for their participation (e.g., caregiver support required, parking, childcare, etc.), 49 however projects rarely have funding available at these early stages, and not all developed proposals receive funding. For a true commitment to patient engagement, research funding models need to change to support patient-partners from the start. Until this happens, our partnering patient organization, MDC, has made funds available for researchers to compensate patient-partners for their time involvement in the initial phases of project development and grant application. This is supported by imPORTND, which incorporates a process to build a bank of trained patient-partners to be prospectively matched by our partnering patient organization with researchers early in grant development.
Shifting research culture
During our work on this project, we became increasingly aware of the culture shift required for integration of POR. When our EPCB team began this project, it was one of seven separate project streams within the NMD4C. In a systematic review of competencies required by researchers, development of community engagement skills was viewed as a low priority, with only one of 16 reports identifying this as a required research skill. 50 However, by involving patient-partners as co-presenters and co-developers in our knowledge translation activities, including a webinar, and at network meetings, the perceived importance of patient-engagement within the network evolved. Building capacity for patient engagement is no longer a separate project in NMD4C but is now a cross-cutting theme, and patient-partners are ‘embedded’ members in all the network's current work. As noted, however, the uptake of our modules has been higher with patients than with research teams, highlighting the need for future projects to focus on generating continuous buy-in amongst researchers.
Directing the utilization of research funds is another tangible mechanism to demonstrate commitment and a shift in practice. To further promote this behaviour our supporting patient organization, MDC, has made patient engagement a criterion for submitted applications in their research grant competitions. This has increased patient-partnered work by 50%. Additionally, patient-partners are involved as reviewers in the grant review process. Involvement at this level gives patient voice and representation in directing research funding and prioritization but also helps provide critical feedback to investigators when a project's ranking suffers for not including patient-partners.
While capacity building is just one piece of POR it is only through authentic partnerships between patients and researchers that research can advance for rare diseases. Fagan et al. 51 suggest that research institutions utilize existing structures, like patient organizations (e.g., Muscular Dystrophy Canada), to facilitate POR. imPORTND actively focuses on establishing and maintaining relationships through training and is a catalyst for matching patient-partners with appropriate research studies.
Future
The need for continuous maintenance and sustainability is a concern with online training and resources. We developed imPORTND with sustainability at the forefront to ensure that the training remains live, updated and continuously relevant. To ensure maintenance, quarterly reviews of the content take place to ensure that links and videos are operational. Survey evaluation is built into the end of each module, to track ‘roles’ of who completes the training and to seek feedback for learner experience, and suggestions for improvement and relevance. Future projects and initiatives should focus on ensuring researchers understand the value of POR and tracking practice shifts, including the diversity and numbers of patient-partners involved, the numbers of network associated projects that include patient-partners, and in what type of research, and how the patient community perceives the relevance of research outputs. We anticipate that the training may need updating every three years and have built in mechanisms to inform the next iteration.
Conclusion
The aim of this project was to develop a capacity-building training program focused on POR specifically tailored for researchers and patient-partners involved in NMD research. We achieved this goal but also discovered that the process was as important as the product. Engagement with patient-partners throughout the project helped the team consider the barriers and research culture from different perspectives. This enabled us to address some of these barriers directly in the design and content of the training. It also helped establish better processes for linking patients with researchers, and in working with our patient organization, we were able to address some of the financial and structural funding barriers to POR. Most importantly, it helped us communicate the importance of POR more effectively to the entire network and establish ‘buy-in’ from researchers and patients. This has extended to having patient-partners further embedded within the network and established respectful and beneficial connections. At a time when research is shifting towards treatment possibilities for rare neuromuscular diseases, having a fully engaged community is critical. Our training project has started to shift how that research activity and associated networking is being co-constructed in Canada. There is still much work to do, but this has been a meaningful start.
Statements and declarations
Dr K. Selby has been principal investigator in clinical trials with Biogen, Roche, Italfarmico and Reverogen. She received an honorarium for consultant advisory committee work for Roche and Novartis and received an honorarium for a presentation from Novartis. Dr Selby decares that she has no declarations of interest regarding this manuscript.
Supplemental Material
sj-zip-1-jnd-10.1177_22143602251405819 - Supplemental material for Building capacity for patient-engagement in neuromuscular disease research: A network project
Supplemental material, sj-zip-1-jnd-10.1177_22143602251405819 for Building capacity for patient-engagement in neuromuscular disease research: A network project by Patricia Mortenson, Homira Osman, Erin Beattie, Corinne Kagan, Victoria Larocca, Claudia Maltais, Linda Niksic, Margo Thompson and Kathryn Selby in Journal of Neuromuscular Diseases
Footnotes
Acknowledgements
The authors acknowledge James Davis, Communications and Administrative Coordinator for the Neuromuscular Disease Network for Canada, for his technology assistance and support in uploading our resource repository and developing the learning platform courses and uploading and managing learning materials. We also acknowledge Dr Cynthia Gagnon's contributions to the conceptualization, funding acquisition and methodology of the project and her French language video content.
Ethical considerations
Research ethics was not needed for this education project. Data collected was in keeping with quality improvement and course evaluation.
Author contributions
Patricia Mortenson: Conceptualization, Methodology, Formal Analysis, Investigation, Resources, Writing - original draft preparation, review and editing, Visualization, Project administration.
Homira Osman: Conceptualization, Methodology, Formal Analysis, Investigation, Resources, Writing - original draft preparation, review and editing, Supervision, Funding acquisition.
Erin Beattie: Conceptualization, Methodology, Writing - review and editing, Project administration, Supervision, Funding acquisition.
Corinne Kagan: Conceptualization, Methodology, Resources, Writing - review and editing.
Victoria Larocca: Writing - original draft preparation, review and editing
Claudia Maltais: Conceptualization, Methodology, Resources, Writing - review and editing.
Linda Niksic: Conceptualization, Methodology, Resources, Writing - review and editing.
Margo Thompson: Conceptualization, Methodology, Resources, Writing - review and editing.
Kathryn Selby: Conceptualization, Methodology, Writing - review and editing, Project administration, Supervision, Funding acquisition.
Funding
This project was supported by the Neuromuscular Disease Network for Canada (NMD4C) via Canadian Institutes of Health Research and Muscular Dystrophy Canada grants (Network Grant: OR2-189333; Network Catalyst Grant: NG2-170044); Patricia Mortenson is funded by a University of British Columbia Four Year Doctoral Fellowship.
Institute of Musculoskeletal Health and Arthritis, Muscular Dystrophy Canada, (grant number OR2-189333, Network Catalyst Grant: NG2-170044).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.