
Abstract
Background
Duchenne muscular dystrophy (DMD) is a severe X-linked neuromuscular disorder causing progressive muscle loss and early death. Despite global evidence on its burden, data from Sweden remain limited.
Objective
This study described the natural history of DMD, treatment patterns, healthcare resource utilization, and direct medical and non-medical costs among patients with DMD and their caregivers in Sweden.
Methods
A retrospective, observational matched cohort study was conducted using data from the Swedish National Registry for Neuromuscular Disorders linked to national health and social registers. Patients diagnosed with DMD and their caregivers were compared to matched population controls. Disease progression was classified into four stages based on the HERCULES model.
Results
A total of 211 DMD patients (mean age at diagnosis: 4.9 years) and 877 comparators were included. Patients experienced progressive loss of function, spending on average 3.8, 4.8, 4.8, and 7.4 years in stages 1–4, respectively. Glucocorticoid use was high (84% on either prednisolone or deflazacort). Annual direct medical costs were significantly higher for DMD patients (€14,590 vs. €660). Direct non-medical costs, predominantly for personal assistance, increased substantially with disease stage, representing 89% of total DMD-related costs (€135,671 annually).
Conclusions
DMD is a severe disorder marked by prolonged time in the later stages of the disease and increasing need for support. DMD imposes a significant economic burden in Sweden, with direct non-medical costs far exceeding direct medical costs. These findings highlight the need for and value of early and effective interventions to delay disease progression and alleviate societal burden.
Introduction
Duchenne muscular dystrophy (DMD) is a rare progressive X-linked neuromuscular disorder caused by mutations in the dystrophin gene. These mutations lead to a lack of functional dystrophin which impairs myofiber structure and function, resulting in progressive muscle degeneration and weakness. 1 Patients experience loss of ambulation (typically by adolescence), scoliosis, and eventually death, generally in early to mid-adulthood, most commonly from respiratory failure, cardiac failure, or gastrointestinal complications.2–5 DMD is divided into stages of disease progression based on ambulatory level that generally correspond with age: stage 1: diagnosis and early ambulatory, stage 2: late ambulatory, stage 3: early non-ambulatory, and stage 4: late non ambulatory. 6 DMD affects males almost exclusively. Females are likely to be asymptomatic carriers. 1 The estimated global prevalence of DMD is less than 10 per 100,000 among males and it is very rare among females (less than 1 per 1,000,000). 7
Although there is still no cure for DMD, advances in care and management—particularly the use of ventilatory support—have, over recent decades, raised patient life expectancy from previously low levels.3,8 Treatment guidelines recommend a multidisciplinary, coordinated, patient-centered team-based medical, surgical, and rehabilitative approach to ensure comprehensive care for patients with DMD.4,6,9–11 The aim of direct physical therapy is to prevent decreased muscle function and joint contractures to ultimately prolong ambulatory ability. 6 Glucocorticoids (prednisone/prednisolone or deflazacort), which are the mainstay of DMD treatment, have also been shown to prolong time in the ambulatory stage and it is now recommended to start treatment in younger individuals, before the onset of physical decline. 12 Treatment with glucocorticoids has also been shown to reduce the likelihood of developing scoliosis. 10 Yet, for patients with scoliosis, surgical intervention may be required.
Coordinating and providing treatment according to treatment guidelines is associated with significant direct medical and direct non-medical costs. Evidence from both the US and Europe found that annual healthcare costs for patients with DMD were 10-times greater than for controls, with costs rising with age and disease progression.13,14 A study from UK that modeled costs associated with standard DMD care estimated lifetime costs between£624,240 and £713,840, most of which were attributable to direct non-medical care such as supportive aids, home modifications, and informal caregiving. 15
In the last 20 years, research has made considerable strides in developing therapeutic strategies for DMD aimed at restoring dystrophin production (e.g., gene therapy, exon skipping, cell-based treatments, and protein replacement therapies) or reducing the downstream effects of dystrophin deficiency (e.g., inflammation, fibrosis, muscle atrophy). 16 Considering the evolving treatment landscape for DMD, it is important to understand the present state of disease severity, disease progression, and the use of existing treatment options, to provide patients with optimal care. Moreover, healthcare resource use (HCRU) and costs associated with DMD have not been specifically assessed in Sweden. Therefore, this study used Swedish registry data spanning 2001–2022, a period during which glucocorticoids were the mainstay of treatment, to describe natural disease progression, comorbidity profile, treatment patterns and estimate HCRU and the associated direct medical and non-medical costs in patients and caregivers to patients with DMD in Sweden.
Methods
Study design and study population
This observational matched cohort study included all patients diagnosed with DMD in the Swedish National Registry for Neuromuscular Disorders (NMiS). The NMiS is a National Quality of Care registry that aims to improve the management of neuromuscular disorders such as DMD. 17 While reporting to NMiS is not mandatory, it includes 83% of DMD patients in Sweden according to the annual report from 2023. In addition, this study included also national administrative data on hospital care, deaths, pharmacy-dispensed drugs, and various social benefits programs (see Supplementary Table 1 for details on the data sources). Reporting to these registers is mandatory including the personal identification number given to all Swedish citizens which enable linkages across registries.
Patients in the NMiS were linked to national administrative registers via their personal identification number. The study period spanned from 1 January 2001 to 31 December 2022. The study included four cohorts, the DMD cohort was comprised of patients diagnosed with DMD and who had a registered visit in the NMiS registry from 1 January 2006 to 31 December 2021. Diagnosis was based on clinical signs and/or mutation in the dystrophin gene compatible with DMD. The date of the first visit was set as index date. A comparator cohort, compromised of age-, sex, and region-matched (1:5) individuals was drawn from the total population. Individuals who emigrated within one year of the index date were excluded from the study population. The DMD caregiver cohort included caregivers of patients with DMD, identified using the Multi-Generational Register. Similarly, the comparator caregiver cohort consisted of caregivers of comparators, also identified using the Multi-Generational Register. The caregiver’s index date corresponded to that of the cases and comparators. All individuals were followed from index date until death, emigration or end of the study period (31 December 2022), whichever came first (Supplementary Figure 1).
Study outcomes
Demographics and comorbidity profile of the study cohorts at index date
Age, sex, residency, and level of education were extracted from the Longitudinal Integration Database for Health Insurance and Labour Market Studies (LISA) for the calendar year prior to the index date. Comorbidities from start of the study period to index date were identified solely through the National Patient Register (NPR), as no observation time prior to registry inclusion was available in NMiS. As index dates varied across individuals, the length of pre-index observation differed between patients. Baseline comorbidity estimates should therefore be interpreted as the prevalence of recorded comorbidities within the available observation window rather than as lifetime prevalence. See Supplementary Table 2 for ICD-10 codes of comorbidities.
Disease progression and treatment patterns
At each visit registered in NMiS, DMD patients were classified according to their disease status using the HERCULES natural history model of disease progression in DMD.18,19 Information enabling classification according to all stages of the Hercules model was not available in the NMiS; therefore, the model was condensed into four stages. Specifically, observations on reduced walking ability was not available in NMiS and very few patients had no/partial need for ventilation at the same time as hand-to-mouth-function (or loss thereof), which motivated the use of a condensed model. Figure 1 outlines the disease model used in this study and stages were defined as follows: Stage 1 (ambulatory – patient can walk >300 meters in 6 minutes), Stage 2 (transitory/non-ambulatory – patient cannot walk >300 meters in 6 minutes), Stage 3 (non-ambulatory, partial need for ventilatory support or loss of hand-to-mouth function), and Stage 4 (non-ambulatory, full ventilatory support – patient requires full ventilation [>16 hours/day] or has a forced vital capacity <30%). Disease stage at each time point was determined based on clinical information recorded at each registered healthcare visit in NMiS. The start of a disease stage was defined as the first recorded visit at which the criteria for that stage were met. Some patients had a registered approximate date for loss of ambulation. When this was the case, this date was used to include patients in stage 3 or 4. As registry visits are intermittent, and the actual date of loss of ambulation was not recorded frequently, stage transitions reflect the timing of recorded observations rather than the exact onset of functional decline. Given the nature of the data, patients could therefore skip stages (e.g., transitions from stage 1 to stage 3). The condensed model employed in this study corresponds closely to clinically relevant functional milestones (ambulatory, transitory/non-ambulatory, partial ventilatory support, full ventilatory support). This approach, despite the degree of missing data, was deemed superior to an age-based disease-progression model as such model would miss the heterogeneity of disease progression between individuals of same age. Patients were classified into disease stage according to the available information. Patients with missing information on disease stage were included in the study population but omitted from the results based on disease stage. It was only possible to progress to a later disease stage which is in line with the natural course of the disease. Time spent (in years) in each disease stage was estimated, and progression to higher-level disease stages together with number of patients who died or were censored at end of study or migration was visualized. Age at treatment start, treatment type, and treatment duration were obtained from NMiS. Treatment duration was based on the cumulative duration of exposure recorded in the registry by the treating physician. For patients with treatment interruptions and subsequent re-starts, separate treatment episodes could be recorded, but the duration used in this study reflected the total treatment duration across all recorded episodes. Disease progression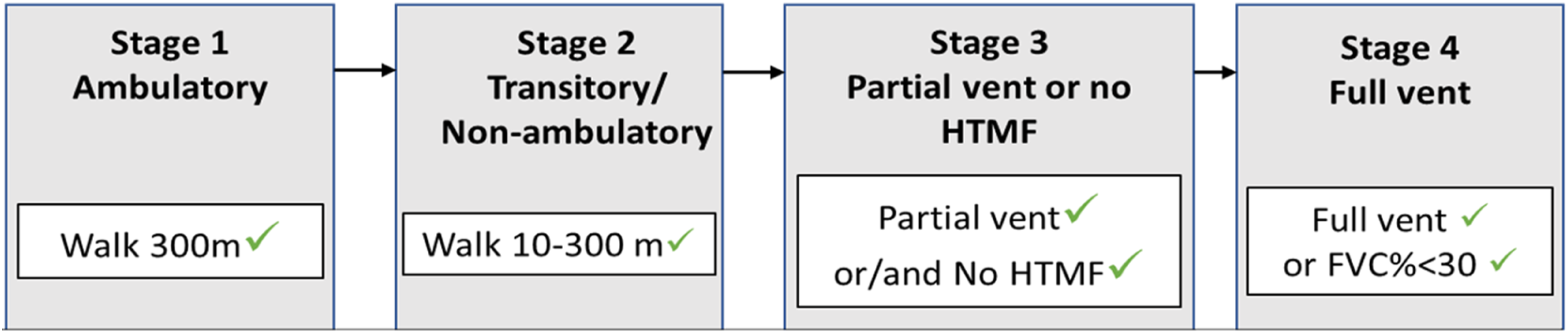
Comorbidities
The prevalence of selected comorbidities co-occurring and related to DMD (reduced respiratory function, pneumonia, cardiomyopathy, arrhythmia, scoliosis, kyphosis, lordosis, osteoporosis, Attention Deficit Hyperactivity Disorder [ADHD], anxiety, autism, depression, obsessive compulsory behavior, and cataract) was estimated at the time of each disease stage transition (i.e., at the time when patients transitioned from one stage into the next). Because follow-up time varied between individuals, these estimates are descriptive and should be interpreted as stage-specific recorded comorbidity burden rather than directly comparable point prevalences.
HCRU and associated direct medical costs
Outpatient specialty visits, hospital admissions and the duration of hospital adminssions (in days) were summed from the index date to end of follow-up using data from the NPR. Similarly, the number of pharmacy dispensations were also summed across all individuals using data from the Prescribed Drug Register (PDR). All HCRU was divided by the length of follow-up (in years) by subject and reported as the average annualized number of visits/dispensations. HCRU was also stratified by disease stage in the DMD cohort.
Direct medical costs of outpatient and inpatient visits were calculated by multiplying each healthcare visit by its corresponding diagnosis-related group-code (DRG) using the national tariff of 2023. If the DRG-code was missing in the tariff of 2023, prior year’s tariffs were used. 20 The cost of dispensed drug was extracted directly from the PDR and represents the public list price.
Non-medical resource use and direct non-medical costs
Definitions, data sources, measurement, and costing of non-medical resource use and related payments.
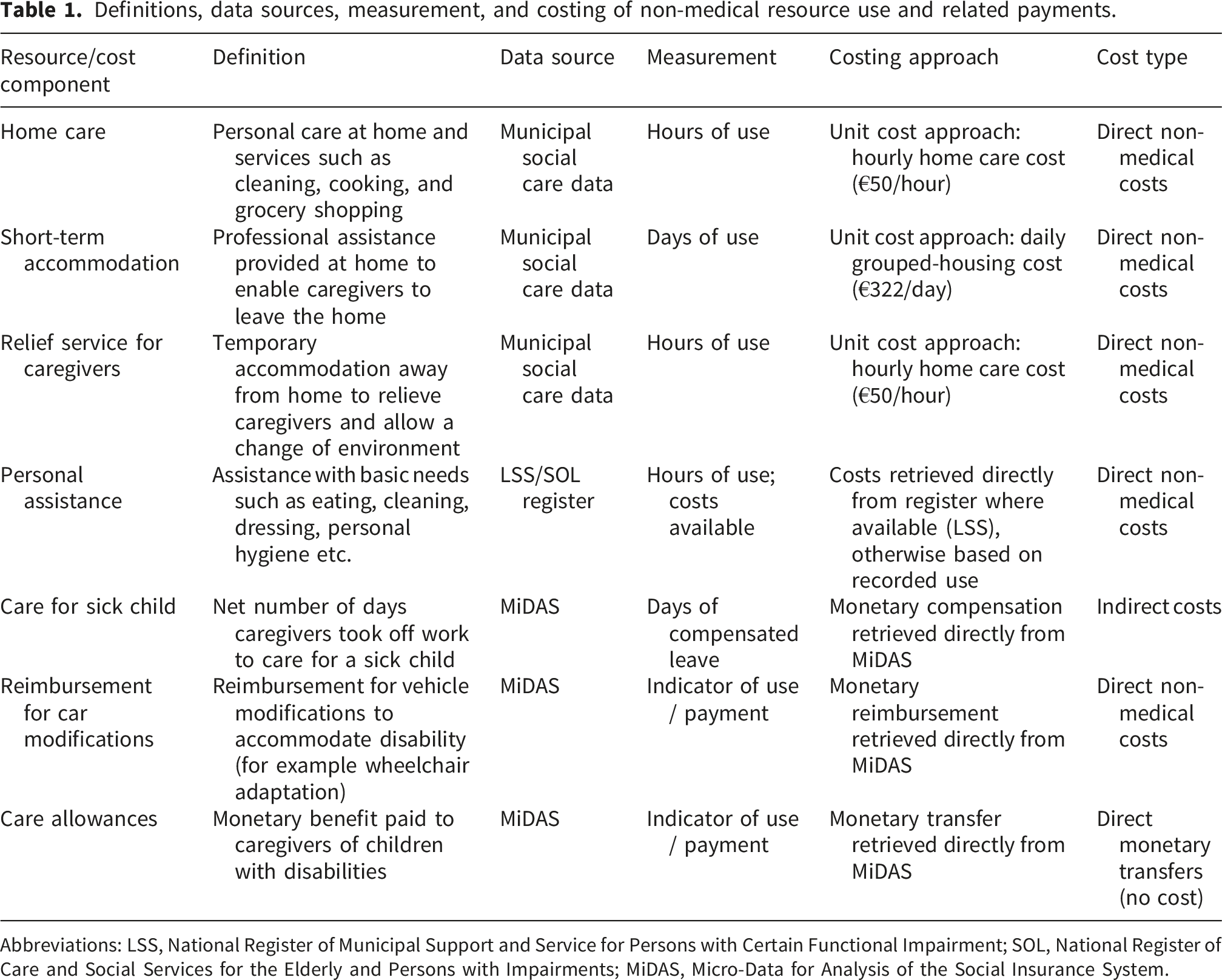
Abbreviations: LSS, National Register of Municipal Support and Service for Persons with Certain Functional Impairment; SOL, National Register of Care and Social Services for the Elderly and Persons with Impairments; MiDAS, Micro-Data for Analysis of the Social Insurance System.
Data on the resource use of home care, short term accommodation and relief service were only available for November each year. These resource useages were therefore annualized by multiplying the November value by 12. The cost of home care, short term accommodation and relief service were estimated by applying unit cost approach. Specifically, the average hourly cost of home care (€50) was derived from a study on 65 municipalities in Sweden (covering ∼20% of the Swedish population) and multiplied by the number of hours of home care and relief service. From the same report, the average daily cost (€322) of grouped housing (a type of accommodation with professional support that often offers common areas such as kitchen, living room as well as private spaces like dormitorio) was multiplied by the number of days on short term accommodation. 21
Personal assistance data was sourced from two registries, the National Register of Municipal Support and Service for Persons with Certain Functional Impairment (LSS) and the National Register of Care and Social Services for the Elderly and Persons with Impairments (SOL). LSS contains data on patients whose individual need exceeds 20 hours per week whereas SOL only include individuals whose need is below 20 hours per week. LSS contains data on resource usage (hours) and associated costs whereas SOL only includes data on resource usage.
Reimbursement for car modifications was estimated as the observed monetary amount reimbursed to the family for disability-related vehicle adaptations.
When resource use was recorded for the caregiver (car modifications and care allowances to parents with disabled children) in a family with more than one child with DMD (n=17), resource use was evenly split between the siblings.
All costs were inflated to 2023 price-levels using the Swedish Consumer Price Index and converted to € (from SEK) using an exchange rate of 10.6.
Statistical analysis
Categorical variables were summarized by the number of available observations, frequency, and percentage. Continuous variables were summarized by the number of available observations, mean and standard deviation (SD). Differences in resource use and costs between the DMD cohort and the comparator cohort was assessed using t-test. All statistical tests were interpreted at a significance level of 0.05.
Results
Study population
Patient characteristics at index date.
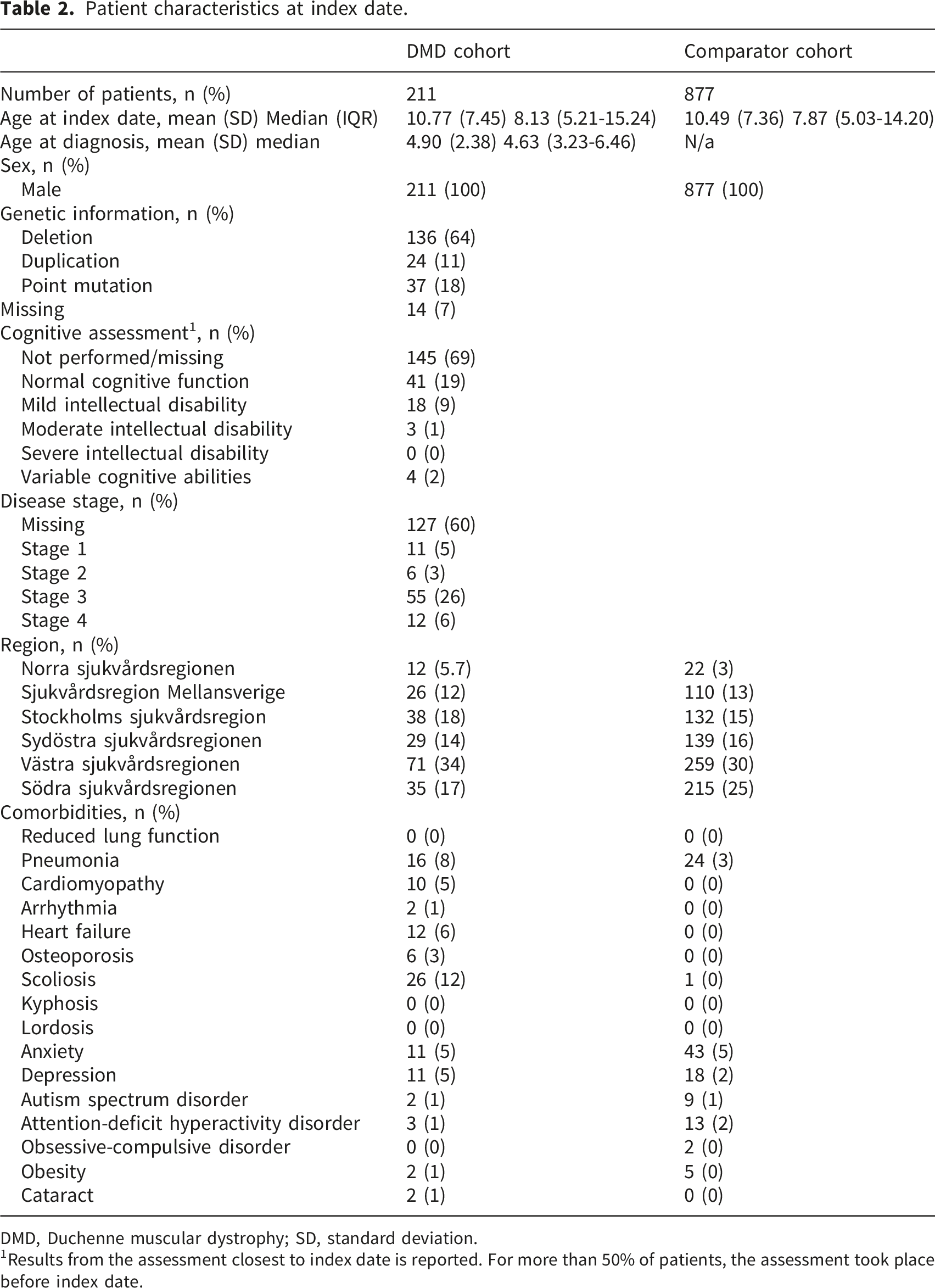
DMD, Duchenne muscular dystrophy; SD, standard deviation.
1Results from the assessment closest to index date is reported. For more than 50% of patients, the assessment took place before index date.
Comorbidity burden and time spent at each disease stage during DMD progression.
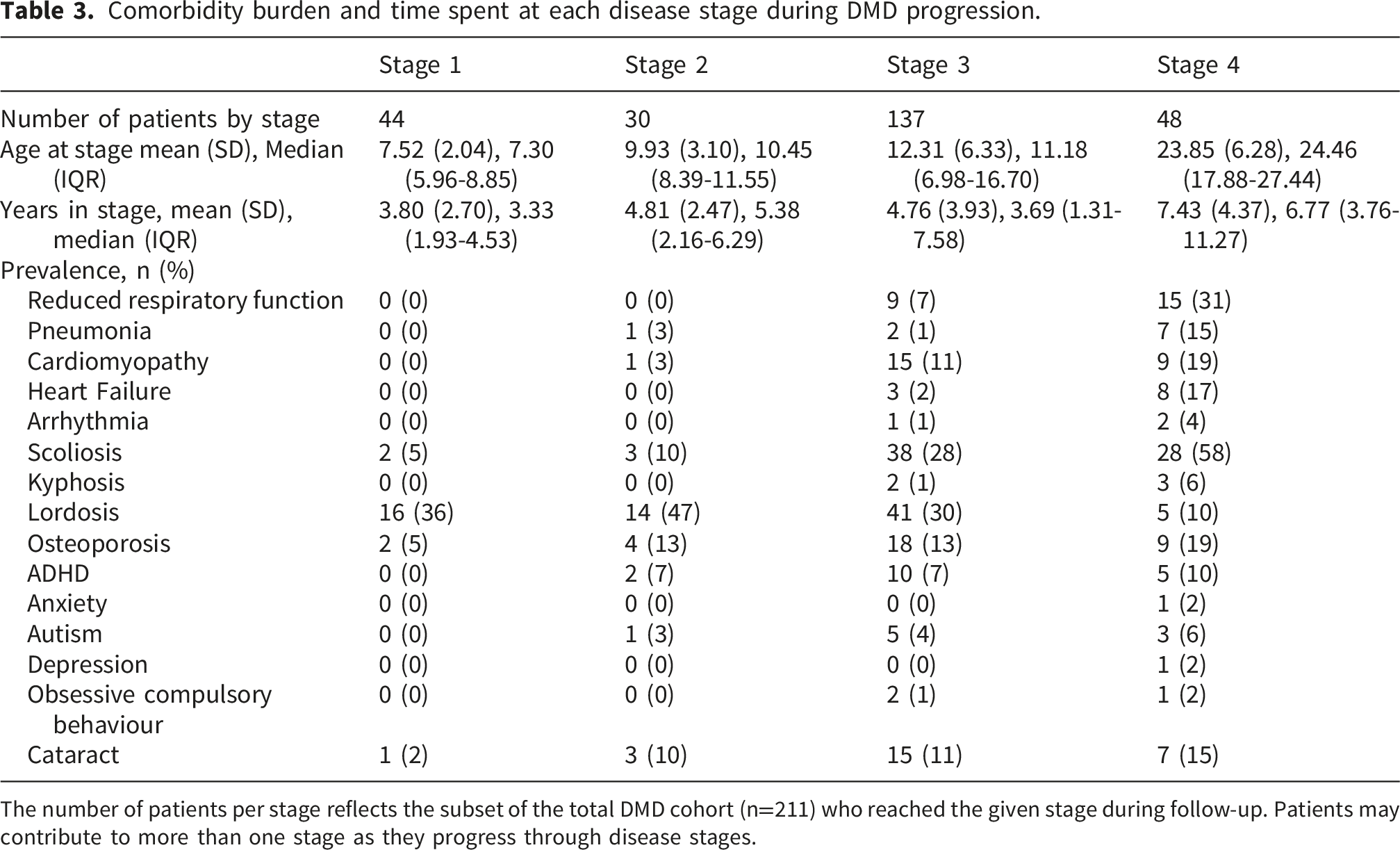
The number of patients per stage reflects the subset of the total DMD cohort (n=211) who reached the given stage during follow-up. Patients may contribute to more than one stage as they progress through disease stages.
Disease progression in the DMD cohort
Disease progression over follow-up is summarized in Figure 2, and patient characteristics and time spent in each disease stage are presented in Table 3. At index date, 11 (5%) patients were in stage1, 6 (3%) in stage 2, 55 (26%) in stage 3 and 12 (6%) in stage 4. The remaining 127 (60%) patients did not have sufficient information about their disease stage at index date to be classified. Time spent in each disease stage is presented in Table 3. A higher comorbidity burden was observed among patients with a higher disease stage. A total of 17 patients died during follow-up; deaths occurred predominantly among patients classified in advanced disease stages or among patients with missing stage information at the time of death. The average age at death was 26.3 years (SD: 9.6; IQR: 21.0-28.8 years). Disease progression over time in patients with Duchenne muscular dystrophy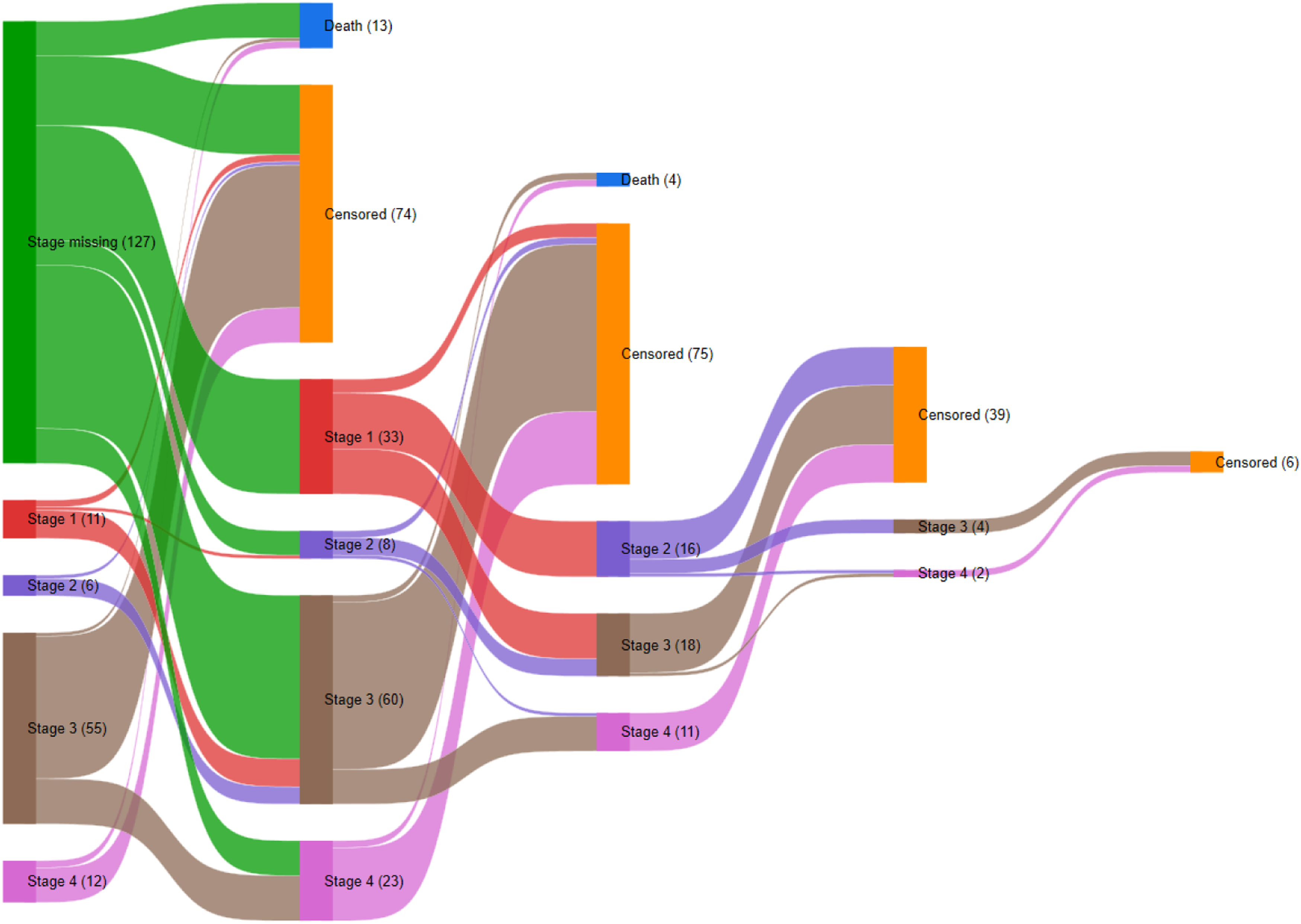
Treatment patterns in the DMD cohort
Treatment patterns.
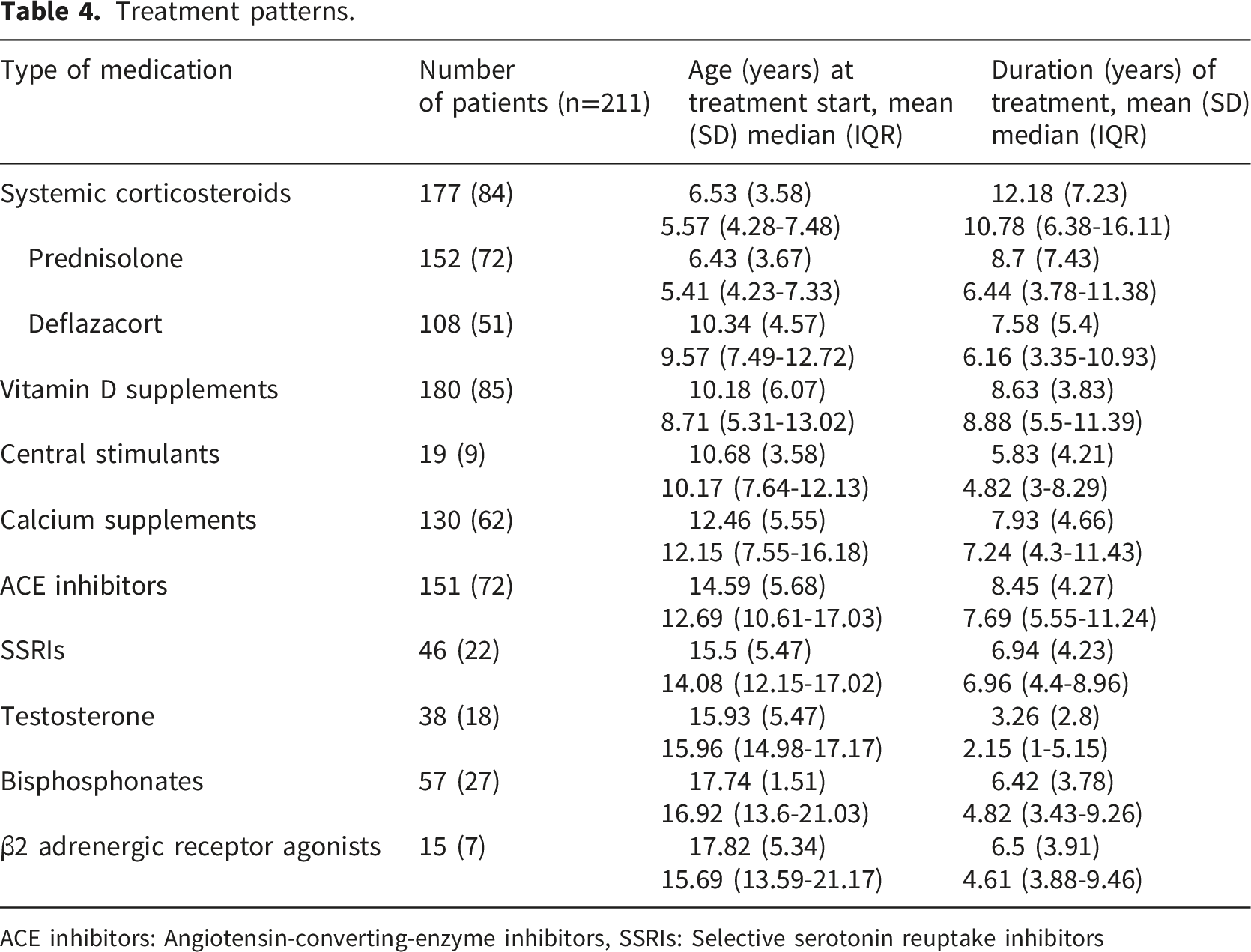
ACE inhibitors: Angiotensin-converting-enzyme inhibitors, SSRIs: Selective serotonin reuptake inhibitors
Prevalence of comorbidities during follow-up
Table 3 shows the prevalence of comorbidities across disease stages. The prevalence of selected comorbidities varied across disease stages. The prevalence of comorbidities increased with disease progression. In some cases (pneumonia and lordosis), the prevalence decreased with higher-level disease stage.
HCRU and costs
DMD associated direct medical costs
Annualized healthcare resource use and direct medical costs per patient-year.
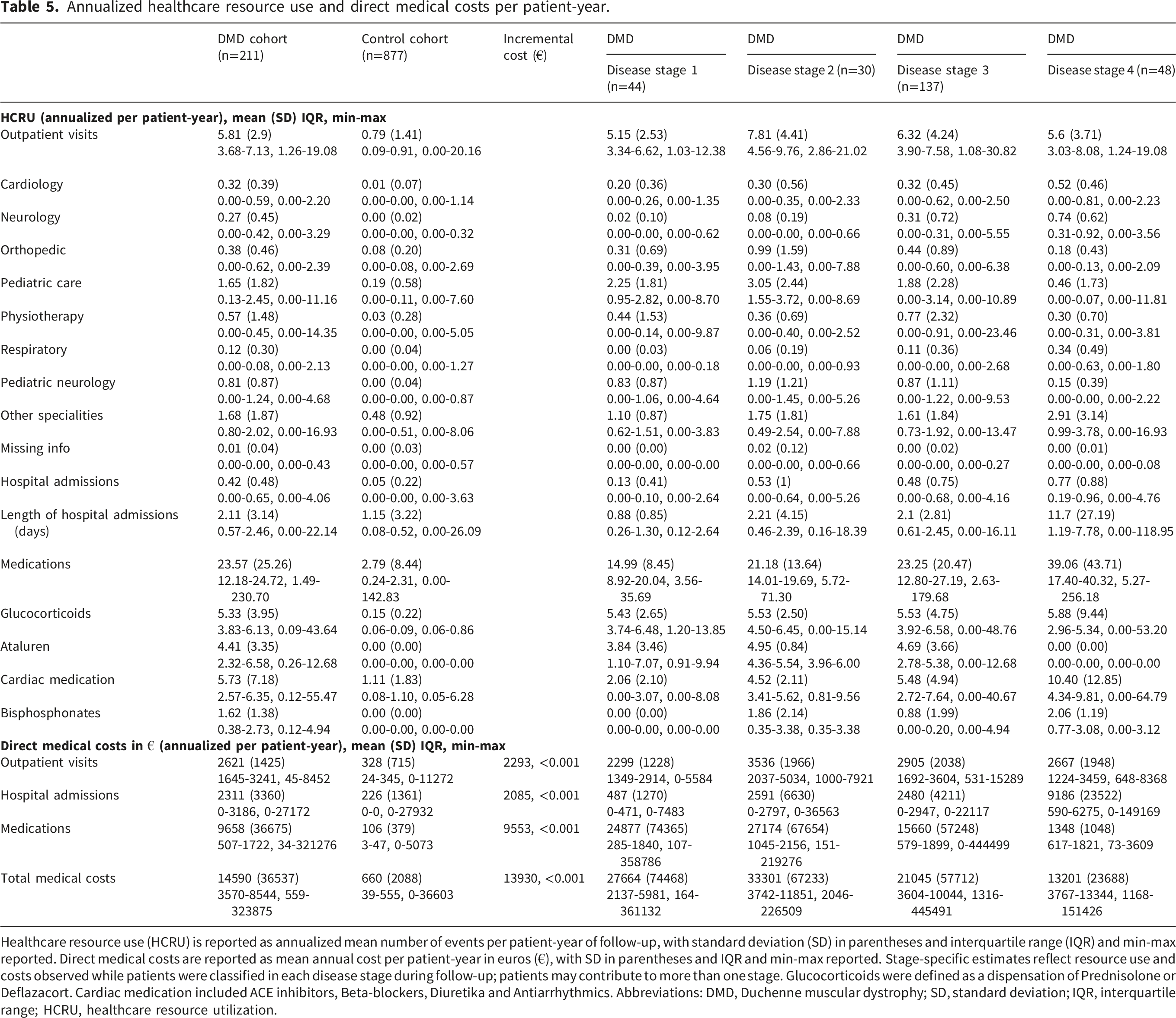
Healthcare resource use (HCRU) is reported as annualized mean number of events per patient-year of follow-up, with standard deviation (SD) in parentheses and interquartile range (IQR) and min-max reported. Direct medical costs are reported as mean annual cost per patient-year in euros (€), with SD in parentheses and IQR and min-max reported. Stage-specific estimates reflect resource use and costs observed while patients were classified in each disease stage during follow-up; patients may contribute to more than one stage. Glucocorticoids were defined as a dispensation of Prednisolone or Deflazacort. Cardiac medication included ACE inhibitors, Beta-blockers, Diuretika and Antiarrhythmics. Abbreviations: DMD, Duchenne muscular dystrophy; SD, standard deviation; IQR, interquartile range; HCRU, healthcare resource utilization.
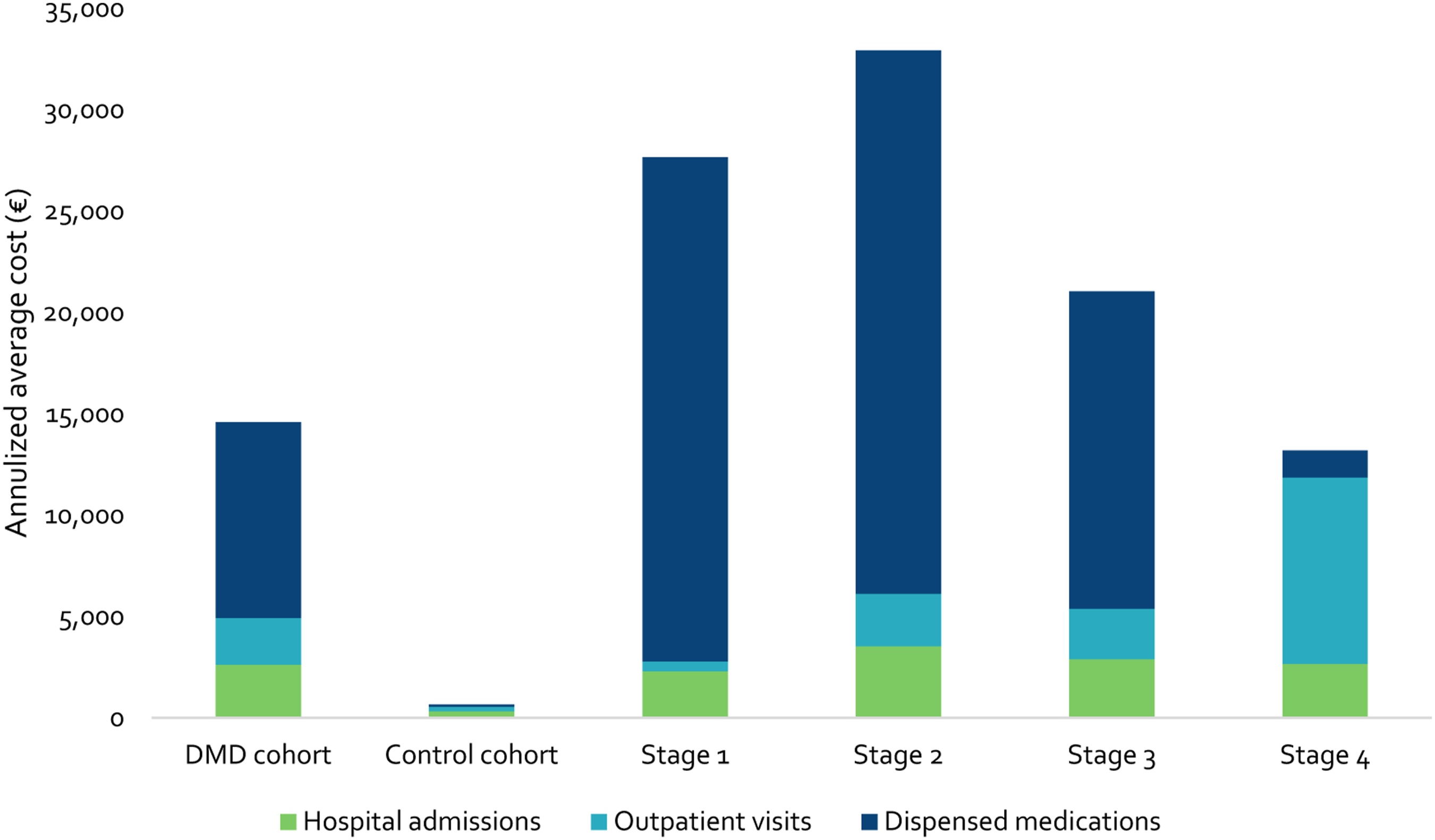
Average annualized direct medical cost for DMD cohort and control cohort. DMD, Duchenne muscular dystrophy.
Annualized direct medical costs were significantly higher in the DMD cohort than in the comparator cohort. The average annualized direct medical cost in DMD patients varied by disease stage. Direct medical costs decreased with disease progression. Costs for disease-modifying treatment (Ataluren), which was prescribed to 14 patients (13 patients with a nonsense mutation, 1 with missing information on type of mutation) was stage-dependent, accounting for 87% (€23,968), 78% (€25,778), 62% (€13,048), and 0% (€0) of direct medical costs at stages 1, 2, 3, and 4, respectively.
Non-medical resource use and direct non-medical costs
Direct non-medical resource utilization in the DMD and control cohort.
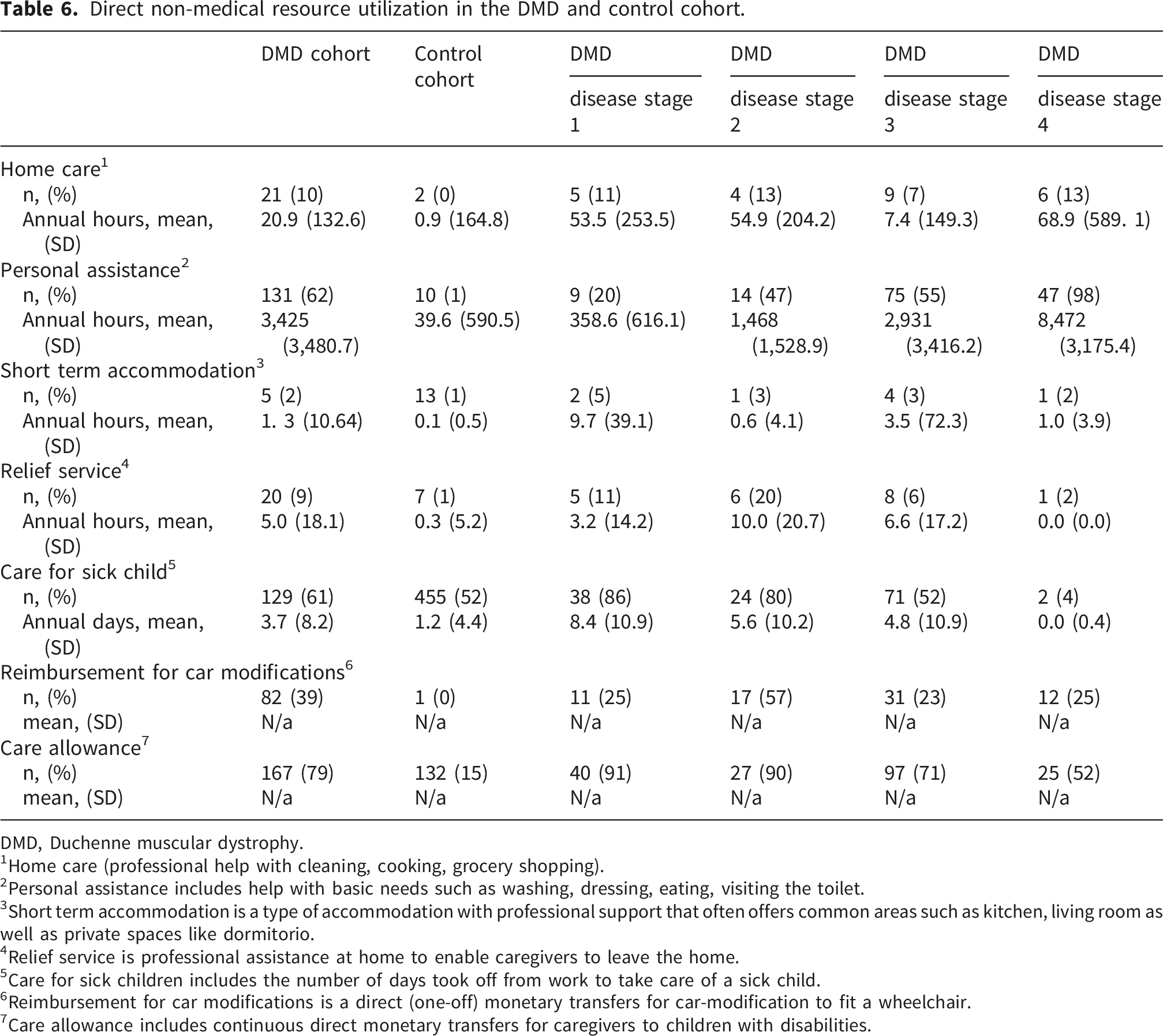
DMD, Duchenne muscular dystrophy.
1Home care (professional help with cleaning, cooking, grocery shopping).
2Personal assistance includes help with basic needs such as washing, dressing, eating, visiting the toilet.
3Short term accommodation is a type of accommodation with professional support that often offers common areas such as kitchen, living room as well as private spaces like dormitorio.
4Relief service is professional assistance at home to enable caregivers to leave the home.
5Care for sick children includes the number of days took off from work to take care of a sick child.
6Reimbursement for car modifications is a direct (one-off) monetary transfers for car-modification to fit a wheelchair.
7Care allowance includes continuous direct monetary transfers for caregivers to children with disabilities.
A comparable percentage of caregivers in the DMD cohort (39.3%; n=154) and control cohort (32.5%; n=547) took sick leave.
Annualized direct non-medical costs (Sup Table 5), reflecting the cost of non-medical support services, were higher in the DMD cohort than in the comparator cohort and increased across higher-level disease stages.
The cost of personal assistance increased by stage (Stage 1: €204; Stage 2: €13,601; Stage 3: €50,814; Stage 4: €198,334). In addition, monetary care allowance amounted for €30,538 in the DMD cohort compared to €4,448 in the control cohort.
When direct medical and direct non-medical costs were combined, the annualized total direct cost per patient-year was €44,370 in the DMD cohort, compared with €2,914 in the comparator cohort, corresponding to an incremental direct cost of €41,456. Direct non-medical costs accounted for the majority of total direct costs in the DMD cohort (67%).
Discussion
This population-based registry study provides a comprehensive description of disease progression in DMD in Sweden, using a functionally defined disease-stage model applied to longitudinal real-world data. Moreover, HCRU, non-medical resource use and associated costs in patients with DMD were compared to age-, sex-, and residency-matched comparators and their caregivers drawn from the total population.
Although phenotypic variability exists, DMD is a progressive disease that inevitably leads to loss of ambulation and wheelchair dependency with increasing age. However, glucocorticoid treatment, which is strongly recommended in DMD care guidelines, can delay loss of ambulation and decrease in pulmonary function.4,6 Indeed, a recent meta-analysis that identified several key predictors of loss of ambulation found that glucocorticoid therapy (deflazacort, prednisone, or prednisolone) was associated with a delayed loss of ambulation. 22 The current study showed that glucocorticoid therapy was used extensively, and started at an early age in the DMD cohort which likely contributed to delayed disease progression. Yet, patients spent a substantial proportion of their disease course in advanced stages, with the longest duration observed in the most severe stage, reflecting prolonged survival with substantial functional impairment. These findings were also described by Broomfield et al. 19 who reported the longest duration in stage 8 (which corresponds to our stage 4) of the original 8-stage HERCULES model. In addition to glucocorticoids, a substantial proportion of patients received supportive pharmacological treatments, including ACE inhibitors and supplements aimed at managing or preventing secondary complications. In Swedish clinical practice, and according to standard of care, ACE inhibitors are frequently prescribed prophylactically, which partly explains the observed medication use in the absence of formally recorded cardiac comorbidity diagnoses in some patients. The prolonged time in advanced stages reflect not only loss of function (e.g., loss of ambulation, HTMF etc.) but also emphasizes the increasing multisystemic burden of DMD, as illustrated by the accumulation of respiratory, musculoskeletal, and neurobehavioral comorbidities across stages. Our study therefore provides new evidence on disease trajectory in a Swedish population with high glucocorticoid use and comprehensive health care.
Beyond disease progression and treatment patterns, this study highlights the substantial healthcare utilization and economic burden associated with DMD in Sweden, consistent with previous studies.23,24 Reflecting the spectrum of comorbidities, patients with DMD received care in a wide range of specialties, including pediatrics, neurology, cardiology, physiotherapy, and orthopedics. This aligns with findings from an Australian study, where patients with DMD and their families’ reported visits to 21 different specialists. 25 However, our study also shows that the total economic burden of DMD is driven by the associated cost with non-medical resource use. In particular, non-medical resource use—including personal assistance, home care, and other support services—increased markedly with advancing disease stage and accounted for the majority of total costs. This pattern reflects the progressive nature of the disease and the resulting reliance on sustained, long-term support. A similar trend was observed in the study by Schreiber-Katz et al., which provided evidence that informal caregiver and social care costs are positively associated with severity, as measured by the stage of DMD. 26 The significant direct non-medical costs among patients with DMD highlight the disease burden on patients with DMD as well as their informal caregivers. The impact of a DMD diagnosis on caregivers has been well-documented, including feelings of isolation, depression, anxiety, and exhaustion, as well as stress from giving care, sleep deprivation, and financial difficulties. 27
Given the high direct non-medical costs of patients in stage 4, this evidence further highlights the need for more treatment options than presently available. Glucocorticoid treatment is also associated with an increased risk of complications across multiple organ systems, including cardiorespiratory complications, gastric ulcers, obesity, as well as growth and endocrine complications such as short stature and delayed puberty. 4 The direct medical costs were largely driven by prescription of disease-modifying treatments (Ataluren) to a small proportion of patients (those with a nonsense mutation). The recent EMA recommendation to withdraw marketing authorisation for ataluren ( 28 ), together with challenges related to glucocorticoid treatment, add to the unmet treatment and care needs of patients with DMD. 6 However, 29 recently, therapies targeting restoration of dystrophin production and the consequences of dystrophin deficiency have been developed and some have received regulatory approval in Europe, Japan, and the US.4,30 These developments are promising for reducing the burden of DMD on patients, families, and the healthcare system. Overall, our results show that most of the economic burden associated with DMD is attributable to costs accrued from support services (direct non-medical costs) and increases substantially in the latter stages of the disease. This suggests that targeted treatment in early disease stages aimed at slowing disease progression holds huge potential for attenuating economic burden of DMD.
The study had many strengths, including population-based patient and comparator cohorts and a longitudinal design, however, the results must also be viewed considering the study’s limitations. This study relied on Swedish register-based data, which are known for their high degree of completeness. However, registration to NMiS is not mandatory and while the NMiS captured 83% of patients with DMD in 2023, the lack of complete coverage in Sweden may introduce bias to our results. 17 For example, prescriptions registered in NMiS are not always accompanied by a diagnosis code which introduces discrepancies between frequency of treatments and comorbidities. Comorbidity estimates should also be interpreted with caution because both pre-index and post-index observation time varied across individuals. As a result, recorded comorbidity prevalence may underestimate true lifetime burden in patients with shorter observation windows, and higher prevalence in later disease stages may partly reflect longer cumulative observation time. Secondly, this study did not have sufficient information to fully replicate the Hercules disease progression model which included 8 stages. Nevertheless, the condensed model applied in the present study captures clinically meaningful functional milestones and was adapted to align with the information available in the NMiS. Importantly, this functional staging approach allows for heterogeneity in disease trajectories among patients of similar age, which would not be captured by age-based stratification alone. Although a substantial proportion of patients lacked information for disease-stage classification, the absolute number of patients contributing to the later stages in our condensed model remained relatively high for a rare disease and compares favourably with prior DMD natural-history work in advanced stages. 18 An additional limitation is that patients could contribute to more than one disease stage during follow-up. Consequently, stage-specific estimates are not statistically independent and should be interpreted as descriptive summaries of burden observed at different points in the disease course rather than as comparisons between mutually exclusive groups. Thirdly, although, many of the variables reported in the national healthcare registers used in this study are mandatory, ensuring nearly complete coverage of outpatient visits and inpatient admissions and prescriptions, some relevant cost components were not captured. Inpatient prescriptions are not reported, which may have impacted estimates of direct health care cost and the cost of dispensed medications used public listed prices which may over-estimate the actual costs as price-agreements are confidential information and not available in the prescribed drug registry. Direct medical cost estimates should also be interpreted in light of the influence of expensive pharmacological treatments. In particular, the use of ataluren among a small subset of eligible patients contributed substantially to direct medical costs in some stages, especially earlier stages, and may therefore have affected comparisons of stage-specific medical costs. In addition, selected direct non-medical and indirect costs such as informal caregiving time, productivity losses due to reduced working time, out-of-pocket expenditures, and transportation costs were not available in the data. The reported estimates should therefore be interpreted as a substantial, but incomplete, measure of the economic burden of DMD.
Conclusion
This study contributes important real-world evidence to the current knowledge base on DMD by providing a comprehensive, population-based assessment of disease progression, treatment patterns, healthcare utilization, and both direct medical and non-medical costs in Sweden. Patients with DMD represent a vulnerable patient population who often suffer from several comorbidities and whose need for support increases as the disease progresses. Our results emphasize that most of the economic burden associated with DMD arises from support services, particularly in higher-level disease stages. This suggests that timely, targeted treatment interventions in early stages of DMD could significantly reduce overall disease burden on patients, families, and the healthcare system.
Supplemental material
Supplemental material - Disease progression and economic burden of duchenne muscular dystrophy: A retrospective study using Swedish register data
Supplemental material for Disease progression and economic burden of duchenne muscular dystrophy: A retrospective study using Swedish register data by Thomas Sejersen, Anna-Karin Kroksmark, Aina Törnblom, Samira Toghanian, Gustaf Ortsäter, Anne-Berit Ekström in Journal of Neuromuscular Diseases.
Footnotes
Acknowledgments
Editorial and medical writing support under the guidance of authors was provided by Kripi Syal of Quantify Heor Private Limited, in accordance with Good Publication Practice (GPP3) guidelines (Ann Intern Med. 2015; 163:461-464). Karolinska and Sahlgrenska membership of EURO-NMD is gratefully acknowledged. TS was supported by a research fund to the Center for Neuromusculoskeletal Restorative Medicine from the Health@InnoHK programme launched by the Innovation and Technology Commission, the Government of the Hong Kong Special Administrative Region of the People’s Republic of China.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and approved by the Swedish Ethical Review Authority (reference number 2022-06220-01). As this was a retrospective register-based study using pseudonymized data, the requirement for informed consent was waived.
Consent to participate
As this was a retrospective register-based study using pseudonymized data, the requirement for informed consent was waived.
Author contributions
All authors participated in the conceptualization and the development of the methodology of the study. Gustaf Ortsäter performed the data curation, statistical analysis, and visualization of the results. All authors participated in the drafting, reviewing and editing of the manuscript and have approved the final content. Samira Toghanian led the supervision, project administration and acquired funding for the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Quantify Research AB received funding from Pfizer AB to conduct this study and for the development of this manuscript.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Thomas Sejersen is recipient of research grant from Pfizer, and honoraria received for lectures or consultancy from Biogen, Novartis, PTC Therapeutics, Sarepta Therapeutics, Pfizer, Roche, and Italfarmaco. Gustaf Ortsäter is an employee of Quantify Research and owns Quantify Research stocks and stock options. Quantify Research AB provides consulting and other research services to pharmaceutical, medical device, and related organizations. Samira Toghanian is an employee of Pfizer AB and owns Pfizer AB stocks and stock options. Aina Tornblom is an employee of Pfizer AB and owns Pfizer AB stocks and stock options. Pfizer is a research and development pharmaceutical company which provides medicines and vaccines to patients who need them. Anna-Karin Kroksmark is a physiotherapist and docent at the Department of Health and Rehabilitation, Institute of Neuroscience and Physiology, University of Gothenburg, Gothenburg, Sweden. She is also coordinator for the Neuromuscular Registry in Sweden (NMiS). Anna-Karin Kroksmark has no conflict of interest to declare. Anne-Berit Ekström is a child neurologist and senior consultant at the Neuromuscular Unit, Queen Silvia Children’s Hospital, Sahlgrenska University Hospital, Gothenburg, Sweden. She is also an associate professor at the Department of Pediatrics, Institute of Clinical Sciences, University of Gothenburg. In addition, she serves as the registry holder of the Swedish Neuromuscular Registry (NMiS). Anne-Berit Ekström is recipient of honoraria received for lectures or consultancy from Biogen, Novartis, PTC Therapeutics, Sarepta Therapeutics, Pfizer, Roche, and Italfarmaco.
Data Availability Statement
Data used in this study is protected under Swedish and European law and may only be accessed following relevant ethical approvals, data protection assessments, and compliance with GDPR and other legal frameworks.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.