
Abstract
Introduction
Knowledge about facilitators and barriers to exercise among individuals with MG is limited.
Objective
The aim of this study was to identify factors that influence exercise participation for adults with MG and to explore beliefs and perceptions with respect to exercise.
Methods
This was a cross-sectional observational study via an online questionnaire. Adults with MG residing in France were eligible.
Results
Responses from 455 participants were analysed. The majority were between 50 and 69 years, 71% were female, 80% had generalised MG, and half had early-onset MG. Participants reported reduced MG-specific QoL (MGQOL-15F-r), a moderate-to-high impact of MG on activities of daily living (MG-ADL), and mild-to-moderate fatigue levels (NeuroQoL fatigue). Overall, 54% of respondents reported engaging in exercise (“exercisers”), while 47% did not (“non-exercisers”). Exercisers had a lower BMI, reported less fatigue, better HRQoL and a lower impact of MG on ADLs compared to non-exercisers. Fear of exercising was reported by one-third of participants, including half of non-exercisers versus 19% of exercisers (p < 0.001). Non-exercisers reported significantly more barriers to exercise (mean 3.5 (1.8)) than exercisers (mean 2.6 (1.9), p < 0.001). Health/symptoms was the most frequently reported barrier in both groups (59% of non-exercisers, 39% of exercisers). Non-exercisers also reported fewer facilitators (mean 2.1 (1.4)) than for exercisers (mean 2.5 (1.3), p=0.004). The most frequently cited facilitator for non-exercisers was specialised supervision/coaching (59%), while exercisers most frequently cited health/symptom improvement (57%).
Conclusion
Several barriers and facilitators influencing exercise participation for individuals with MG could be addressed with tailored programmes.
Introduction
Myasthenia Gravis (MG) is a rare, chronic autoimmune disease that causes dysfunction of neuromuscular transmission, resulting in varying degrees of fatigability or skeletal muscle weakness. Symptoms can differ in intensity, duration and onset. There is currently no cure, and management is primarily pharmacological. The consequences of MG often extend beyond its primary pathophysiology. Its symptoms, treatment-related side effects, and the fluctuating, unpredictable nature of the disease, are burdensome for individuals.1,2 These factors limit daily activities (ADLs), contribute to secondary deconditioning, and negatively impact psychological well-being, social participation, and professional integration.3,4
A growing body of evidence demonstrates that exercise in stabilised autoimmune MG is safe and effective in improving certain health components, such as strength, walking capacity, and reducing disease impact on ADLs.5–9 However, recent studies show that many individuals with MG are sedentary and may not engage in regular exercise.10–13 The reasons for this remain unclear due to a lack of data and mixed results in the literature. For example, two recent studies found that MG disease severity did not correlate with physical activity (PA) levels, as measured using trunk accelerometry.12,13 Other factors, such as increased age, were associated with reduced moderate-vigorous PA, while an increased body mass index was linked to reduced daily PA.11,12
Barriers to exercise can exist at the intrapersonal, interpersonal, or institutional/community levels. 14 In a recently published qualitative study of 10 adults with MG living in Queensland, Alsop and colleagues identified fatigue and pain as potential barriers to physical activity. 15 They also found that experiences with healthcare professionals were insufficient, failing to provide disease-specific advice regarding MG and physical activity. 15 The key enablers in their study were medical management and social support.
To implement exercise programmes that address the specific needs of individuals with MG, it is essential to understand the factors that may limit or facilitate exercise participation. 16 Access to exercise is crucial for individuals with MG, as physical inactivity and sedentary behaviour have detrimental effects on health and well-being, increasing both morbidity and mortality. 17 Therefore, the primary aim of this study was to identify key extrinsic and intrinsic factors that influence exercise participation in a large cohort of adults living with MG. Secondary aims were to explore beliefs and perceptions regarding exercise. The study also sought to compare individuals who exercise with those who do not in terms of clinical characteristics, symptoms, fatigue, and health-related quality of life, in order to identify potential levers to promote exercise. Identifying the facilitators and barriers to engaging in exercise is a critical step in developing targeted interventions that could improve the health and quality of life of individuals living with MG.
Methods
This was a cross-sectional observational study. Approval was obtained from a local ethics committee (Nord Ouest IV, 210519.71034) and the study was registered on ClinicalTrials.gov (NCT05408702). A purpose-built questionnaire was created and remained online and open to recruitment between November 2021 and May 2022. The survey was accessible via a secure online platform (Sanoïa e-Health services Digital CRO), which assured data confidentiality. No identifying information was collected. Information about the questionnaire was diffused through MG patient associations (AFM-Téléthon and A.M.I.S) via their websites, newsletters, private groups as well as via the French neuromuscular network Filnemus, specialist centres and via the AFM-Téléthon Regional Services.
Study cohort
To be eligible to participate, individuals were required to self-report a diagnosis of MG, be at least 18 years old, reside in France, and provide informed consent by confirming that they had read the information notice, had no further questions, and agreed to have their data analysed.
The information notice outlined the purpose of the study and the measures in place to ensure anonymity. It also stated that the questionnaire should be completed only once. Respondents could complete the survey on a computer, tablet, or smartphone. Access to the full questionnaire was granted once the participant answered ‘yes’ to informed consent and two subsequent eligibility questions: age and having a confirmed diagnosis of a neuromuscular junction disorder (NMJ), such as MG, Congenital myasthenic syndrome (CMS), or Lambert-Eaton myasthenic syndrome (LEMS). Data from any non-eligible participants, e.g., those not residing in France, were excluded from the analyses. Due to the exploratory nature of the study and the absence of reference studies on this topic with this patient population at the time, no specific sample size calculations were performed. As this was a patient-partnered study, it was available to all three myasthenic syndromes; however, only data from participants with MG are presented in this manuscript. Data from the CMS and LEMS cohorts will be analysed and presented in future publications.
Survey content
The questionnaire contained four sections, consisting predominantly of closed questions and several open-ended questions about sociodemographic information and mobility, MG and comorbidities, exercise and MG, as well as validated questionnaires including MG-ADL, MGQOL-15F-r, NeuroQoL fatigue. The MG-ADL is an MG-specific 8-item patient-reported scale that measures MG symptoms and their impact on daily activities (ADLs) based on the preceding 7 days.18,19 The score ranges from 0-24 with higher scores representing a greater impact of MG on ADLs. A score ≤ 1 has been used to express minimal symptom expression (MSE). 20 The MGQOL-15 is an MG-specific patient-reported 15-item measure evaluating physical, psychological, and social domains commonly impacted by MG over the preceding few weeks. The French version (MGQOL-15F) was validated, and the revised version has a total score of 30 with higher scores representing worse HRQoL (MGQOL-15F-r).21,22 The patient acceptable symptom satisfaction (PASS) is a single yes/no response question, where participants are asked whether they are satisfied if they had to remain in their current state. 23 PASS-positive and negative states have been evaluated in MG.24,25 The NeuroQoL fatigue consists of 19 questions, with responses based on a 5-level Likert scale with higher scores indicating more fatigue. Responses are based on a 7-day recall period. 26 A validated French version was provided by David Cella on behalf of the National Institute for Neurological Disorders and Stroke, used with permission of the PROMIS Health Organization. NeuroQoL recommends using T-scores for analysis so raw scores of the short form bank (8 items) were transformed to their respective T-scores using a free scoring service from Neuro-QoL. 27 T-scores were interpreted as: < 45 = no fatigue; 45–55 = mild fatigue; 56–65 = moderate fatigue; and > 65 = severe fatigue.28,29
A draft of the questionnaire was developed and underwent multiple rounds of revision. Initially, it was reviewed by several external researchers and clinicians. After incorporating their feedback, a focus group and cognitive interviews were conducted with six individuals with MG to further evaluate the questionnaire. Based on their suggestions, further amendments were made. The revised version was then pilot tested with ten individuals diagnosed with an NMJ disorder (MG or CMS or LEMS). Based on this testing, additional amendments were made to enhance the questionnaire’s relevance, clarity, and usability before its wider distribution. Final modifications were completed, and the estimated time to complete the questionnaire was determined to be 30 minutes.
All questions required a response to proceed to the next, except the NeuroQoL fatigue score which was optional. Some questions were conditional, meaning follow-up questions were only presented to respondents whose previous answers made them applicable. Respondents were allowed to go back and edit their prior responses; however, once the entire questionnaire was validated and submitted, changes could no longer be made. The questionnaire had to be completed in a single session (within 45 minutes), as there was no option to save responses and return later. Exercise was defined as an activity that is structured, planned, repetitive, voluntary and active, with the aim of improving or maintaining one’s health/fitness. 30 Respondents were classified as exercisers if they answered “yes” to the question: “Do you practice physical exercise?” (with the above definition provided), and as non-exercisers if they answered “no” (see Supplementary information S4).
The reporting of data followed the Checklist for Reporting Results of Internet E-Surveys and the Strengthening the Reporting of Observational Studies in Epidemiology statement.31,32 Following the closure of the questionnaire platform, the data were screened, and participants were excluded if they did not meet eligibility criteria.
Data analysis
Continuous variables are reported as mean and standard deviation, while qualitative data are reported as counts and percentages. Categorical variables were compared using the Chi-square test or Fisher’s exact test. To compare the distributions of continuous variables, either a Student’s t-test or a pairwise Wilcoxon test was used, depending on the distribution of the data. Based on responses, participants were classified as “exercisers” or “non-exercisers”. To evaluate the primary objective, univariate analyses were conducted to compare exercisers and non-exercisers to identify factors that may limit or facilitate exercise. To control for multiple comparisons, p-values were adjusted using the Benjamini-Hochberg method. Associations between limiting and facilitating factors and exercise were investigated through univariate analyses. Given the descriptive and exploratory nature of this study, analyses were limited to univariate comparisons to provide transparent group-level descriptions. Multivariable modeling was not performed due to the interrelated nature of key variables, the risk of multicollinearity and overadjustment, and limited sample sizes in some subgroups. All tests were two-sided, with p-values of 0.05 or less considered statistically significant. All analyses were carried out using SAS 9.4 (SAS Inc, Cary, NC). No data imputation was necessary, as responses to each question were required.
Results
Figure 1 represents the study flow chart. Responses from 455 participants with MG were analysed, covering all 13 regions of France as well as the French overseas territories (Figure S1). Respondents were from urban, intermediate and rural areas. Table 1 presents the characteristics of the respondents. One quarter were in the 50-59 years age range, one quarter were in the 60-69 years age range and 18% were in the 70-79 years age range. More than half (57%) of respondents were overweight or obese. The body parts most frequently affected by MG were the eyes, followed by the lower limbs and then the upper limbs (Figure S2). Overall, respondents reported an altered MG-specific QoL (MGQOL-15F-r), a moderate-to-high impact of MG on activities of daily living (MG-ADL) and mild-to-moderate fatigue (NeuroQoL fatigue) (Table 1). Three-quarters of participants (n=349) reported fluctuations in their walking ability, and half (n=233) reported difficulty walking. Walking duration varied from not being able to walk 15 minutes, to being able to walk more than one hour (Figure S3). Forty-six percent of respondents reported exercising (exercisers), while 54% did not exercise (non-exercisers). Study flow chart. Demographic and clinical characteristics of respondents. Data are presented as mean (SD), or number (n) and proportion (%). Sex: Non-binary, n=1 (0.2%), not included in sex analysis. MSE: Minimal symptom expression. ^based on MG-ADL score. #T scores NeuroQoL fatigue short form, n = 435 (232 Exercisers, 203 Non-Exercisers).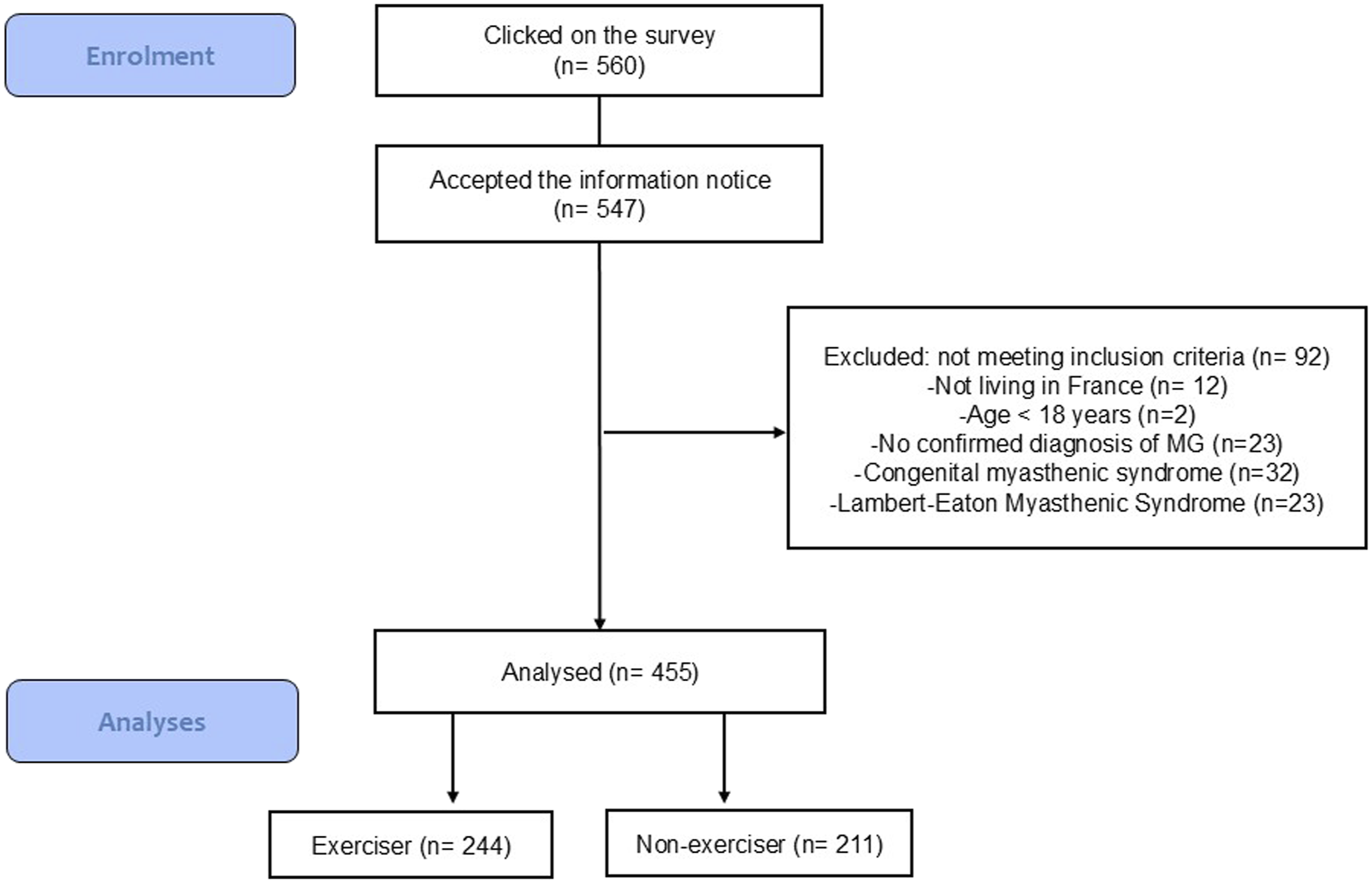
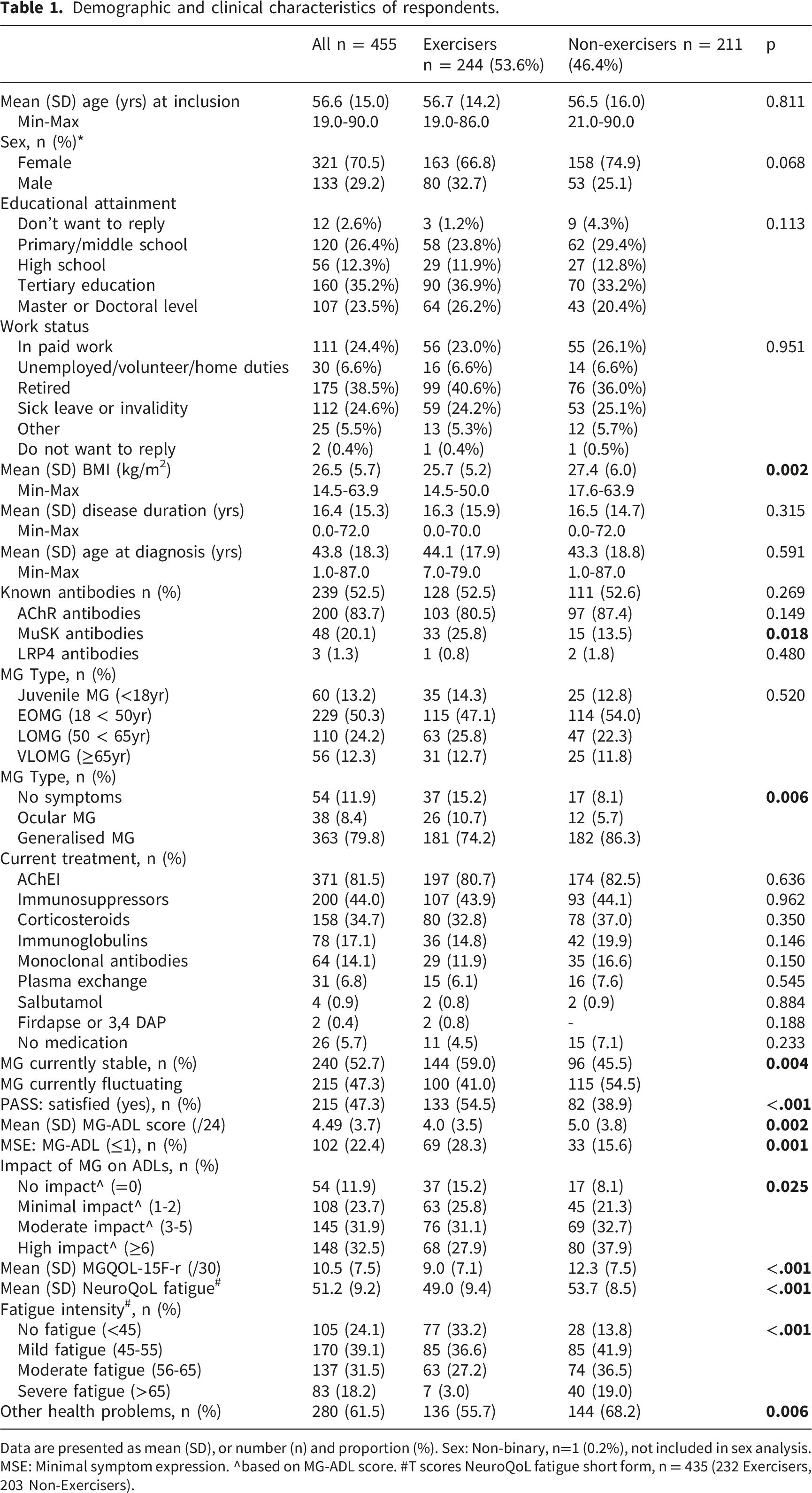
When comparing exercisers and non-exercisers, exercisers had a lower BMI, reported less fatigue, had better HRQoL, reported less impact of MG on ADLs and more exercisers were satisfied with their current state (PASS) (Table 1). For respondents who were not in paid employment, 54% (n=145) reported this being due to their MG, with a marked difference between exercisers (n=71, 47%) and non-exercisers (n=74, 62%), p=0.019. A greater proportion of non-exercisers (n=144, 68%) reported being mostly sedentary during the day compared to exercisers (n=94, 39%), while fewer non-exercisers (n=49, 23%) reported being active versus 53% (n=129) of exercisers p<0.001. The ability to walk fluctuated more for non-exercisers (85%) than exercisers (70%), p<0.001 and walking duration (p<0.001) and capacity (p<0.001) was reduced in non-exercisers compared to exercisers (Figure S3). Individuals without MG symptoms or with purely ocular MG were more frequently exercisers than non-exercisers (Table 1).
Healthcare professionals and family attitudes to exercise
The treating MG physician (neurologist for 80%, n=364) recommended fewer than half (46%, n=201) of respondents to exercise. For 47% (n=207), exercise was not mentioned at all, for 7% (n=30) exercise was discouraged and exercise was forbidden for 1% (n=4) of respondents. Exercisers reported receiving more support from their treating physician, including more recommendations to exercise and more frequent discussions about exercise, compared to non-exercisers (p<0.001). Exercisers were also more likely to receive support from family and friends to exercise, compared to non-exercisers (p<0.001).
Exercise and MG
Exercisers reported not exercising as much as they would like to; 53% reported less exercise since their MG diagnosis, 22% fraction their exercise, 5% exercise more, 9% started exercising after their MG diagnosis, and 11% did not change their exercise routine. The majority reported positive effects of exercise on morale (85%), desire to move (82%), well-being (82%), self-esteem/confidence (72%), energy (62%), muscle fatigability (63%), sleep quality (56%), general fatigue (54%), body control (54%), muscle weakness (53%), and that exercise reduced their feelings of withdrawal/sadness (57%). One-third of exercisers reported experiencing no bothersome MG symptoms during exercise. In contrast, the remaining two-thirds most frequently reported lower limb, upper limb and respiratory symptoms as bothersome. For nearly half of the exercisers (48%), these symptoms were present during and after exercise.
The majority of non-exercisers (77%) reported wanting to exercise, with two-thirds stating they had completely stopped exercising since being diagnosed with MG. The majority feared that exercise could increase their muscle fatigability (72%), general fatigue (61%) and muscle weakness (56%). They also anticipated that exercise could improve their morale (68%), desire to move (68%), well-being (65%), self-esteem/self-confidence (63%), sleep quality (57%), and energy (50%). Eighty-five percent of non-exercisers reported various MG symptoms as a barrier to exercise, with lower and upper limb symptoms, as well as respiratory symptoms, being the most frequently reported.
Beliefs/attitudes towards exercise
The majority of respondents (77%) believe that exercise is not contraindicated; however, exercisers and non-exercisers differ in their beliefs about exercise. Almost one-quarter of non-exercisers are unsure whether exercise is contraindicated; 17% believe it is compared to exercisers, of whom only 2% believe exercise is contra-indicated and 7% are uncertain (p<0.001). One-third of all respondents fear exercising, including almost half (48%) of non-exercisers, compared to 19% of exercisers (p<0.001). Like exercisers, nearly all non-exercisers (98%) believe that exercise is generally good for health. However, only two-thirds of non-exercisers think it is beneficial for them, with one-quarter unsure and 9% believe it is not. In contrast, almost all exercisers (93%) view exercise as personally beneficial.
Reported barriers to exercise
Overall, the mean number of barriers reported was 3.0 (1.9), with a minimum of 0 and a maximum of 9. The most reported barriers were health/symptoms (48%), lack of MG-specialised supervision (37%), fear of the consequences on disease/symptoms (33%), and weather conditions (33%). Non-exercisers reported more barriers (mean 3.5 (1.8)) than exercisers (mean 2.6 (1.9)) (p<0.001). Health/symptoms was the most frequently reported barrier for both exercisers (39%) and non-exercisers (59%) (Figure 2(b)). When comparing significant differences between the two groups, seven barriers (health/symptoms, lack of specialist supervision, fear of consequences on disease/symptoms, lack of exercise knowledge, lack of motivation, lack of time, lack of company) were more frequently reported by non-exercisers than exercisers. Only weather conditions were reported as a barrier more often for exercisers (39%) than for non-exercisers (28%). Prevalence of barriers (A) and facilitators (B) to exercise.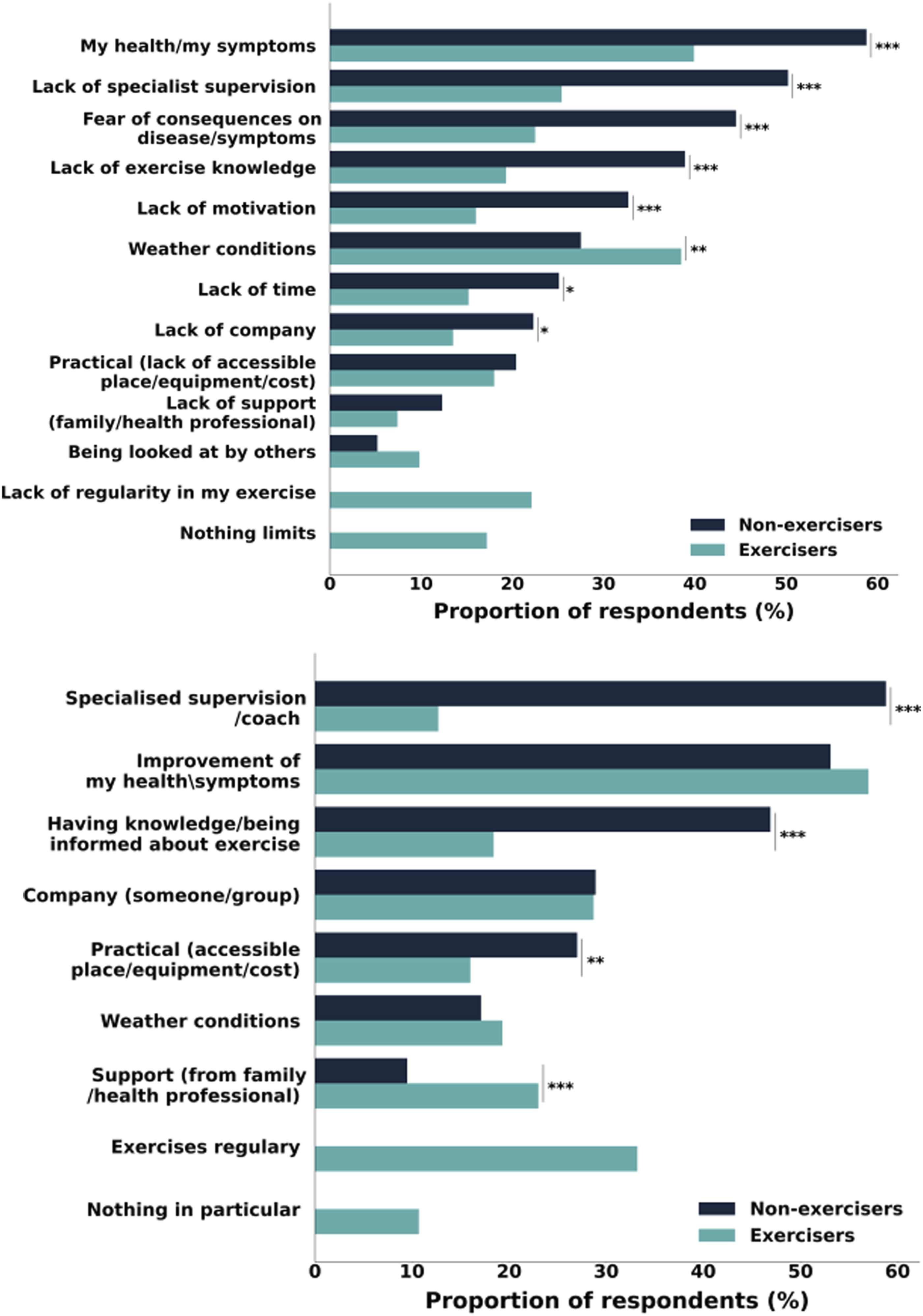
Reported facilitators to exercise
Overall, the mean number of facilitators reported was 2.3 (1.4), with a minimum of 0 and a maximum of 8. The most frequently reported facilitators were exercise improving health (55%), a specialist trainer/coach (34%), and having knowledge/information about engaging in exercise (32%). Fewer facilitators were reported by non-exercisers (2.1 [1.4]) compared to exercisers (2.5 [1.3]), p=0.004. Specialised supervision/coaching was the most frequently reported facilitator for non-exercisers (59%), while improvement in health/symptoms was the most frequently cited facilitator for exercisers (57%) (Figure 2(a)). When comparing significant differences in facilitators, non-exercisers reported three facilitators more frequently than exercisers: having specialised supervision/coaching, having exercise knowledge, and practical aspects such as cost and access. Exercisers (23%) more frequently reported having support from family or healthcare professionals as a facilitator to exercise, compared to non-exercisers (10%).
Discussion
This is the first national study including participants from across France to investigate the perceived barriers and facilitators to exercise participation among individuals with MG. The primary aim of this cross-sectional study was to identify factors that could hinder or support exercise engagement. The findings are intended to inform the development of future initiatives aimed at enhancing exercise participation and improving overall health outcomes for people living with MG and could be useful for other NMDs.
A comparable response rate was obtained from exercisers and non-exercisers. While most indicators were more favourable among exercisers, the cross-sectional design of this study limits the ability to infer causality. It remains uncertain whether exercise contributed to the observed differences in walking capacity, quality of life, and BMI, or whether individuals with more stable disease or reduced fatigue were simply better able to engage in exercise, or whether a combination of these factors played a role. While exercise in MG has been shown to improve walking capacity, strength, and reduce the impact of MG, improvements in quality of life have yet to be definitively demonstrated. 5
Unsurprisingly, the most commonly reported barrier for both exercisers and non-exercisers was health-related issues and symptoms. This highlights the central role of MG and any comorbidities in limiting exercise participation. While these challenges do not prevent exercisers from remaining active, they represent a significant deterrent for non-exercisers. Notably, in this cohort, two-thirds of non-exercisers had ceased all exercise following their diagnosis. Previous research demonstrates that for individuals with disabilities or chronic conditions, health status plays a significant role in shaping physical activity behaviour.33,34 Given the fluctuating nature of MG, efficient pharmacological management is essential. However, despite treatment, many individuals continue to experience suboptimal functioning, even when the disease appears clinically stable. 35 In this cohort, over half reported stable disease, yet, fewer than one-quarter exhibited minimum symptom expression. Common MG-related symptoms that hinder physical activity include fatigability, muscle weakness, general fatigue, dyspnoea, and pain 15. One of the major challenges for individuals with MG is the unpredictable nature of these symptoms. 2 Fluctuations, exacerbations and remissions contribute to a sense of vulnerability and reduced confidence in one’s physical abilities, a phenomenon referred to as “body uncertainty”. 36 In our study, lower limb symptoms were reported as the most bothersome by both exercisers and non-exercisers, followed by upper limb and respiratory symptoms.
Specialist supervision emerged as a key facilitator for non-exercisers. Previous research has highlighted a lack of specialised knowledge and appropriate guidance regarding the optimal type and dosage of exercise for individuals with specific health conditions. 37 The need for personalised exercise recommendations has been consistently emphasised, largely due to limited understanding of what constitutes safe and effective physical activity for those with chronic conditions. 38 Additionally, a shortage of trained exercise professionals has been identified as a barrier across various patient populations.14,39 This is consistent with findings from our study, where lack of exercise knowledge was reported as a key barrier among non-exercisers. The lack of knowledge about how or where to exercise is also a commonly reported barrier in other chronic conditions. 40 For example, in a study of 215 individuals with Parkinson’s disease, having a significant other or personal trainer, as well as receiving encouragement from their neurologist, facilitated exercise participation. 41 Interestingly, in this cohort, high exercisers (≥3h/week) increased their activity after diagnosis while low exercisers (<3h/week) reduced their activity. 41 This contrasts with our cohort, where 53% of exercisers reported exercising less since their MG diagnosis, and only 5% reported exercising more. Additionally, two-thirds of non-exercisers ceased exercising following their diagnosis. The rarity of MG presents an additional challenge in educating and training healthcare professionals, many of whom may rarely encounter individuals with the condition or see only a small number. As a result, there is often a lack of tailored advice. Specialist supervision may help address the fears around exercise expressed by participants in this cohort, as has also been reported in previous studies. 15
Education could be provided by healthcare professionals, patient associations, or through online seminars. Evidence suggests that advice from healthcare professionals can significantly influence the adoption of healthy lifestyle behaviours in sedentary adults in primary care, at least in the medium term (up to 12 months). 42 This underscores the need to educate and inform individuals about how to exercise and which types of exercise to engage in. Individuals may also require guidance on how to modify exercises based on their physical abilities and symptoms. Lack of motivation and lack of time are additional barriers for non-exercisers. Lack of motivation has previously been reported as barrier for people with neuromuscular diseases. 43 Education regarding the positive effects of exercise and potential benefits for them seems to be necessary based on the results of this cohort. Being aware of the benefits of exercise could potentially serve as a motivator. However, it has been suggested that experiencing the positive effects of exercise may be a stronger motivator than just awareness of the possible benefits. 34 Dependence on planning due to the unpredictable nature of MG may also contribute to reduced motivation as it is an added burden/constraint.
Support from family and healthcare professionals was identified as a key facilitator for exercisers and has previously been highlighted as providing a source of enjoyment, motivation and a sense of belonging. 15
To address the lack of time, while research specifically focused on MG and exercise is limited, insights from studies in the general population can help individuals reduce sedentary behaviour. Initiatives such as “snacktivity” or “exercise snacks”, which are defined as short, planned, and structured bouts of vigorous activity could be relevant and beneficial in promoting physical activity in MG. 44 It has previously been shown that, when the intensity is higher, individuals with MG engage in shorter bouts of activity than their peers. 12 These shorter bouts can provide an attainable, time-efficient way to accumulate sufficient activity throughout the day without causing excess fatigue.
In recent years, it has become increasingly evident how detrimental a physically inactive lifestyle is to health and how even a small amount of physical activity can mitigate the risks associated with sedentary behaviour. 17 Individuals with MG and other chronic conditions are generally less active than their peers.12,45 Exercise promotion in MG is still in its early stages, with no specific recommendations currently available. Our results highlight that not all healthcare professionals involved in patient care discuss exercise as part of their treatment plan. However, this finding is based on patient-reported perceptions and may reflect not only whether exercise was discussed, but also how it was communicated, understood, recalled, or perceived by patients. Nonetheless, it is essential that individuals with chronic, lifelong diseases are not excluded from the “exercise is medicine” movement. 46 Exercise should be integrated into the management of IwMG and, further research is needed to support the prescription of exercise based on FITT (frequency, intensity, time and type) principles.
This information is crucial for guiding future research and management strategies for this population. The current lack of research and implementation results in limited access, knowledge, and awareness for these individuals. This study, along with a recent qualitative study, represents the first steps toward addressing this gap in understanding current attitudes toward exercise participation. 15 Both studies are person-centred and directly reflect the perspective of individuals living with MG. 47
The strengths of this study include the large number of participants, encompassing both exercisers and non-exercisers, with a broad demographic range and diverse clinical characteristics, such as disease duration and clinical presentation. Additionally, the study was piloted by individuals with MG to ensure that the perspective of living with MG remained central, thereby confirming the feasibility, clarity, and relevance of the questionnaire. Several limitations should be acknowledged. The study relied on self-reported exercise data and categorisation. Although the dataset was reviewed and participants were instructed to respond only once, this cannot be guaranteed. We acknowledge that the absence of diagnostic verification represents a limitation inherent to anonymous survey methodology. Cultural background was not explored, despite its potential impact on exercise participation. Self-efficacy, defined as a person’s belief in their ability to successfully perform a task, 48 was not specifically examined but is relevant to exercise participation. 49 This was not evaluated as, to the best of our knowledge, no validated questionnaire is currently available in French. Although all regions of France were represented, a selection bias may exist, as individuals not affiliated with an MG patient association or not followed in a specialist centre may be underrepresented. Consequently, the current cohort may reflect a population with greater disease awareness and engagement and therefore may not be fully representative of the broader MG population in France. Response bias could also be present, as individuals with a particular interest in exercise may have been more likely to participate, potentially further limiting the representativeness of the sample. Additionally, a specific barrier-to-exercise questionnaire was not used, as, to the best of our knowledge, no relevant questionnaire is available in French.
Due to the cross-sectional nature of this study, it is not possible to determine whether exercise contributed to the observed differences in fatigue, quality of life, or BMI, or whether individuals with more stable disease or lower fatigue were more likely to engage in exercise, or whether a combination of these factors is involved. While exercise in MG has been shown to improve walking capacity, strength, and reduce disease impact, improvements in quality of life have yet to be definitively demonstrated. 5
Conclusion
This is the first national study which focused on exploring barriers and facilitators to exercise in a large cohort of individuals with MG. These results contribute to understanding the factors that are important to people living with MG and their engagement or lack of engagement, in exercise. Identifying these barriers can inform the development of tailored exercise programme initiatives. Further education and upskilling of healthcare professionals and providing access to specialised healthcare professionals may be an important tool to increasing exercise participation in this population and in other NMD populations.
Supplemental material
Supplemental material - Facilitators and barriers to exercise in autoimmune myasthenia gravis: A cross-sectional survey study
Supplemental material for Facilitators and barriers to exercise in autoimmune myasthenia gravis: A cross-sectional survey study by Birnbaum Simone, Archer Annie, Lejeune Julie, Hogrel Jean-Yves and Stalens Caroline in Journal of Neuromuscular Diseases.
Footnotes
Acknowledgements
We sincerely thank all participants. We thank our colleagues C. Devaux and Jean for their precious input. Thank you the Groupe d’intérêt MG (AFM), the Association A.M.I.S, Filnemus, D. Olivier, A. Bertrand, Societe Francaise Physiothérapie, Societe Sanoia, medical and and support staff at the French neuromuscular reference centres, services regionaux and delegations AFM. Special thank you to D. Valleteau, L. Blacas, to F. Fer, M. Jacoupy from MyoData and J. Audren for their assistance.
Author contribution
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the AFM-Téléthon.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Use of open AI
ChatGPT was used only to improve the wording of selected passages in this manuscript. No other AI tools were used. The authors take full responsibility for the scientific content presented in this work.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.