
Abstract
Aim
To evaluate the longitudinal performance of inertial measurement unit (IMU)-based workspace metrics as a complementary tool to standard clinical scales for monitoring upper limb function in Duchenne muscular dystrophy (DMD) and spinal muscular atrophy (SMA).
Methods
Eighteen children and adolescents (10 DMD, 8 SMA) previously assessed at baseline underwent a one-year follow-up evaluation. Functional status was measured using disease-specific clinical scales (Performance of Upper Limb [PUL] for DMD; Revised Upper Limb Module [RULM] for SMA) combined with IMU-based kinematic analysis. Longitudinal changes in IMU-derived variables were compared with the evolution of clinical scores.
Results
Overall, IMU-based metrics showed longitudinal trends broadly comparable to those observed with clinical scales, with most participants remaining stable over 12 months. Minor individual discrepancies occurred in a few cases, and only two individuals exhibited a clear divergence between IMU-derived measures and clinical scale scores.
Interpretation
IMU-based workspace analysis is feasible and showed meaningful associations with established functional assessments in pediatric neuromuscular disorders. These findings support its further evaluation as a complementary tool for longitudinal monitoring and highlight its potential future role in both clinical trials and routine follow-up.
Keywords
What this paper adds
• One-year IMU follow-up is feasible in individuals with DMD and SMA. • IMU-based workspace metrics showed longitudinal trends broadly comparable to those observed with clinical scales. • IMU measures may capture aspects of upper-limb performance not directly reflected in clinical scale scores. • IMU workspace analysis provides complementary real-world functional assessment • IMU metrics could help monitor neuromuscular progression in future clinical trials.
1. Introduction
Duchenne muscular dystrophy (DMD) and spinal muscular atrophy (SMA) are the two most clinically impactful childhood-onset neuromuscular diseases (NMDs).1,2 Both are characterized by progressive muscle weakness but differ in genetic cause, natural history, and therapeutic options. In DMD, most individuals lose ambulation around the age of 12 despite receiving the current standard of care, which includes corticosteroid therapy. 3 In untreated SMA, children with types 1 and 2 never acquire independent walking, and those with type 1 typically require ventilatory support early in life and have reduced life expectancy. In contrast, individuals with SMA type 3 usually achieve ambulation, although some may lose walking ability over time, even when treated.4,5
In DMD, several therapeutic approaches are currently under investigation or have recently received regulatory approval. 6 Therapeutic progress has been even more remarkable in SMA, where the prognosis has improved significantly with the advent of disease-modifying therapies and the implementation of newborn screening programs.1,5 These advances in both conditions have increased the need for accurate and sensitive tools to monitor motor function in clinical trials as well as in routine clinical practice.4,7
Traditionally, greater attention has been given to the assessment of lower-limb function, as the loss of ambulation represents a major clinical milestone in both disorders. However, with the advent of new therapeutic strategies, there is growing interest in evaluating upper-limb function, particularly in non-ambulant individuals who retain residual arm and hand abilities that are essential for independence.
In this context, wearable inertial measurement units (IMUs) have emerged as promising tools to objectively quantify motor function in children with NMDs, including the assessment of upper limb function.8–11 Baseline motor assessments of this cohort were previously reported, 12 showing that several kinematic metrics, such as workspace area and volume, and curve efficiency, correlated strongly with widely used clinical scales in DMD and SMA. In the present work, the analysis is extended to evaluate their longitudinal performance over a one-year follow-up.
Longitudinal studies using IMU-based metrics in pediatric NMDs remain relatively limited,13,14 particularly for upper-limb assessments. For instance, Ferrarin et al. examined gait in children with Charcot-Marie-Tooth disease, 14 and Rinaldi et al. analyzed lower-limb kinematics over two years in DMD. 13 While IMUs have also been applied to assess upper-limb function, these studies have mostly focused on adults with acquired neurological conditions such as stroke, typically in rehabilitation or inpatient settings.15,16 Some longitudinal IMU-derived metrics, such as SV95C, have been evaluated in DMD and other conditions like FSHD, and have even received EMA qualification.17,18 Building on this work, our study examines complementary kinematic metrics specifically in children with DMD and SMA over a one-year follow-up, addressing the need for longitudinal upper-limb assessments in this population.
The aim of this study is to determine whether kinematic metrics obtained through an IMU-based system can provide complementary information to standard clinical assessments in tracking disease progression in children with NMDs over a one-year period—a timeframe aligned with the duration of many clinical trials and of clear clinical relevance.
2. Methods
2.1. Participants
Ten children with DMD and eight with SMA were included in the study. Inclusion criteria for both groups were: (1) a confirmed genetic diagnosis of DMD or SMA, and (2) age between 6 and 18 years. The study protocol was approved by the Ethics Committee of Hospital Sant Joan de Déu, Barcelona (PS-28-22), and written informed consent was obtained from the parents or legal guardians of all participants.
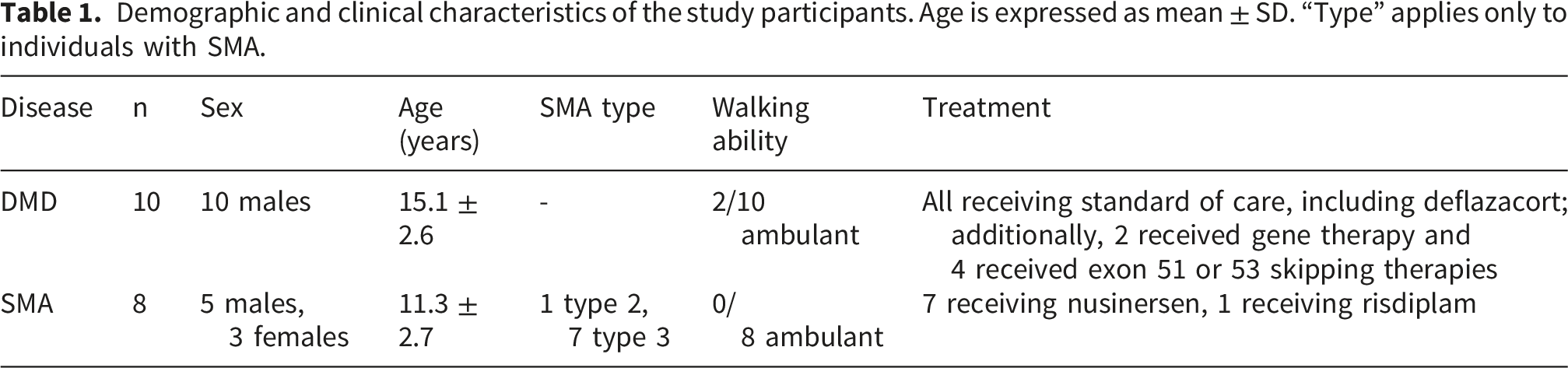
Demographic and clinical characteristics of the study participants. Age is expressed as mean ± SD. “Type” applies only to individuals with SMA.
2.2. Experimental setup and protocol
Upper limb function was assessed using a wearable IMU-based system consisting of seven Xsens DOT sensors (Xsens Technologies, Netherlands).
12
The sensors were placed on the torso at the sternum level, and bilaterally on the upper arms, forearms, and hands (Figure 1). Each sensor is a compact device (36.3 × 30.4 × 10.8 mm, 11.2 g) integrating a 3D accelerometer, gyroscope, and magnetometer, which measure linear acceleration, angular velocity, and the Earth’s magnetic field, respectively. Sensor fusion and 3D orientation were computed using the proprietary Xsens Kalman Filter core (XKFCore). Data were acquired at 60 Hz. Sensor placement from right lateral side. The same configuration is repeated for the left side.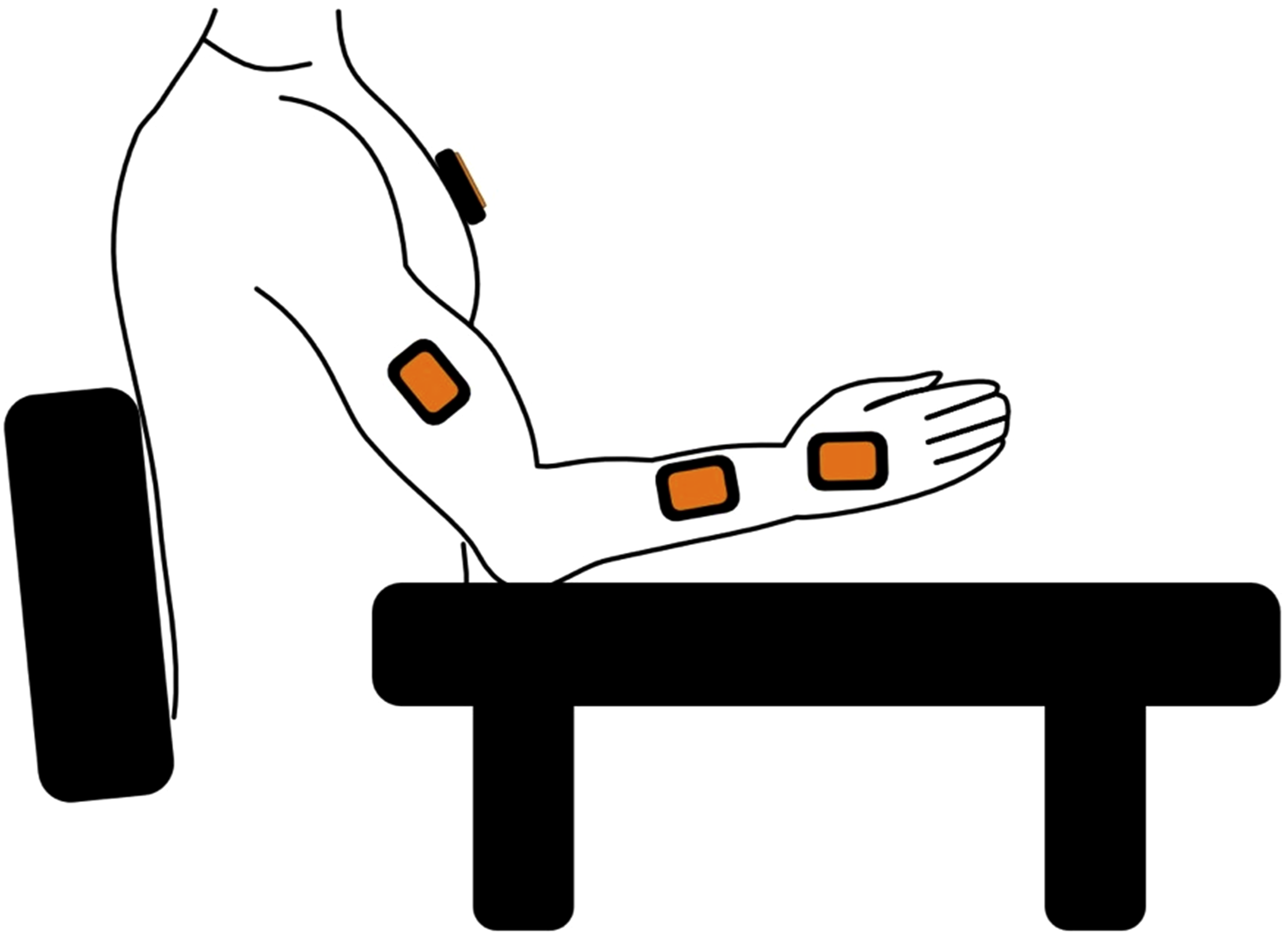
The IMU system and biomechanical model used here have been previously validated against a gold-standard optoelectronic motion capture system in an independent study. 19 That study demonstrated high agreement and acceptable accuracy in upper-limb kinematic reconstruction across multiple functional tasks, supporting the reliability of the spatial trajectories from which workspace metrics are derived.
For calibration, participants were asked to maintain a comfortable, still posture with the arm lying on a table and the torso resting against the back of the wheelchair. 12 A picture-based sensor-to-segment calibration procedure was then applied. Video recordings were also obtained during the assessments to support manual annotation of task execution. 19
Clinical upper limb function was evaluated using validated scales: the Performance of Upper Limb (PUL) 2.0 scale for children with DMD and the Revised Upper Limb Module (RULM) for children with SMA.20,21 IMU data were collected solely during the execution of the PUL or RULM scales, with no additional IMU-specific movement protocol. The PUL 2.0 consists of 22 items and yields a total score ranging from 0 to 42, 20 while the RULM includes 20 items with scores from 0 to 37. 21 Higher scores indicate better upper limb function. Each item was scored as 0 (unable to perform), 1 (performed independently with modification), or 2 (performed without compensation). Both scales share an initial entry item based on the Brooke Upper Extremity Scale, which ranges from 1 (normal arm abduction) to 6 (no useful hand function) 22 (Supplementary Table 1). This score guides the administration of subsequent PUL items, as some are skipped depending on functional capacity. In this study, assessments were performed bilaterally and repeated after one year.
2.3. Kinematic model and data analysis
Upper limb kinematics were computed using a segmental biomechanical model that assumes three rotational degrees of freedom at the shoulder, elbow, and wrist joints, without accounting for translational components. Scapular movement relative to the thorax and humerus was excluded from the model; instead, the humerus was assumed to articulate directly with the thorax.23,24 Seven body segments were represented: trunk, and right and left upper arms, forearms and hands. A right-handed coordinate system was defined with the Y-axis directed inferior–superior, the X-axis posterior–anterior, and the Z-axis medial–lateral, following biomechanical conventions. 24 The model was personalized for each participant using their anthropometric measurements.
Kinematic metrics analyzed included frontal and transverse normalized workspace areas, normalized workspace volume, and curve efficiency, selected based on prior literature.8,11,12,25 These metrics were first introduced and validated against clinical scales in a previous study, 12 and a detailed description of their mathematical derivation and underlying equations, as well as the full computational framework, is provided in Favata’s doctoral thesis. 26 Metrics were extracted during the execution of clinical scale items, which were manually annotated from video recordings. All video-based task annotations were performed by a single experienced investigator following a standardized and predefined segmentation protocol applied consistently across all participants and time points. This approach ensured methodological consistency and minimized inter- and intra-observer variability, thereby reducing potential sources of systematic bias in kinematic metric extraction. To identify the portions of IMU recordings corresponding to each PUL or RULM item, synchronized video recordings were reviewed offline and manually annotated by the same investigator. The start and end of each task were defined based on the observed movement execution, and these annotations were used to segment the IMU data and compute the kinematic metrics. Rest periods and transitions between tasks were excluded from the analysis. Median values and interquartile ranges (IQR) were reported.
Correlations between kinematic metrics and clinical scores (PUL/RULM) at follow-up were assessed using Spearman’s correlation coefficient (ρ), interpreted as low (<0.45), fair (0.45–0.75), or strong (>0.75). Normality was assessed using the Shapiro-Wilk test. Comparisons between baseline and one-year follow-up were performed using paired t-tests or Wilcoxon signed-rank tests, as appropriate. Statistical significance was set at p < 0.05, with correction for multiple comparisons where applicable. All analyses were conducted using IBM SPSS Statistics version 30.0.0 (IBM Corp., NY, USA).
3. Results
The results are presented in three sections. Section 3.1 describes the evolution of motor function scale scores over the one-year follow-up. Section 3.2 reports the kinematic findings in individuals with DMD, all of whom performed the PUL scale. Section 3.3 presents the kinematic analysis of individuals with SMA, all assessed using the RULM scale.
3.1. Assessment of individuals with SMA and DMD using motor function scales
Figure 2 shows the motor function scale scores at baseline and after one year of follow-up. Individuals with DMD were assessed using the PUL scale, while those with SMA were assessed using the RULM. Each marker represents a single individual, with color fill indicating the corresponding Brooke score. Changes in the clinical score after one year from the first assessment for children with DMD (left panel) and children with SMA (right panel). Each marker represents an individual. The fill is colored according to the Brooke score.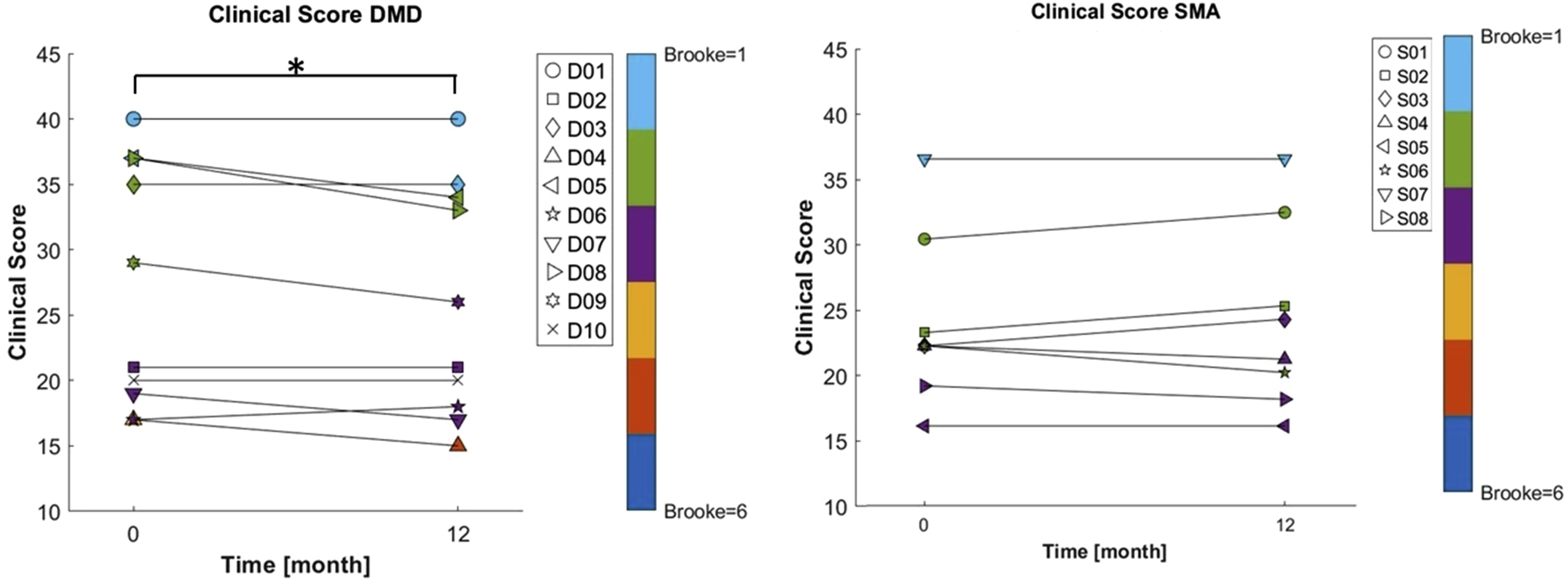
In DMD, the median PUL score decreased slightly but significantly from 25 points (IQR: 18.5) at baseline to 23.5 points (IQR: 16.5) at follow-up (p = 0.03). In contrast, in the SMA group, in which all individuals received disease-modifying therapies for SMA during the follow-up year, the median RULM score showed a small increase from 22 (IQR: 8.5) to 22.5 (IQR: 11.75), although this tendency did not reach statistical significance. At the individual level, only one participant with DMD (individual D08) showed a change greater than 3 points; no SMA participant exceeded this threshold. This cutoff was chosen to approximate the minimum detectable change previously reported for the PUL and RULM scales (4 points).27,28
The Brooke score also remained stable, with no significant differences over the follow-up period in either DMD or SMA. Individual Brooke scores varied by no more than one point in both groups, reflecting overall clinical stability.
Cross-sectional correlations between motor function scales and the Brooke score were strong. Specifically, PUL correlated strongly with Brooke (ρ = −0.93, p < 0.001), and RULM also showed a significant correlation (ρ = −0.73, p = 0.040). However, in the longitudinal analysis, only the PUL score exhibited a statistically significant decline, while RULM and Brooke scores remained unchanged.
3.2. Kinematic analysis of individuals with DMD
Overall, kinematic metrics remained stable between baseline and follow-up. As shown in Supplementary Table 2, frontal workspace area changed from 21.5% to 23.8%, transverse workspace area from 16.1% to 16.5%, workspace volume from 13.1% to 12.3%, and mean curve efficiency from 0.37 deg/s to 0.36 deg/s. None of these changes reached statistical significance, consistent with the modest decline observed in the PUL scores.
At follow-up, most kinematic metrics showed strong correlations with the PUL scale: frontal workspace area (ρ = 0.78, p = 0.0075), transverse workspace area (ρ = 0.84, p = 0.002), and workspace volume (ρ = 0.93, p < 0.001) (Supplementary Figure 1). Curve efficiency also correlated significantly, though more moderately (ρ = 0.71, p = 0.0217). Figure 3 illustrates the longitudinal evolution of these kinematic metrics - workspace areas, workspace volume, and curve efficiency-showing the results obtained at baseline and after one year of follow-up. Changes in the workspace areas (frontal and transverse), workspace volume and curve efficiency after one year from the first assessment for DMD group. Each marker represents one subject and the fill is assigned according to the Brooke score.
Overall, both PUL scores and kinematic metrics showed limited changes over the follow-up period, as illustrated in Figures 2 and 3. At the individual level, correspondence was more variable, with only a few notable exceptions, which are shown in Figure 4. Individual D03 exhibited an increase of 7.6 percentage points in frontal workspace area, which was accompanied by a 1-point improvement in the Brooke score, while the PUL score remained unchanged. Similarly, individual D05 showed improvements across all kinematic parameters, including a 13.3-percentage-point increase in frontal workspace area, despite a 3-point decline in the PUL score. Frontal workspace area of individuals D03 and D05 at baseline and follow-up. Different colors represent the items of the PUL scale.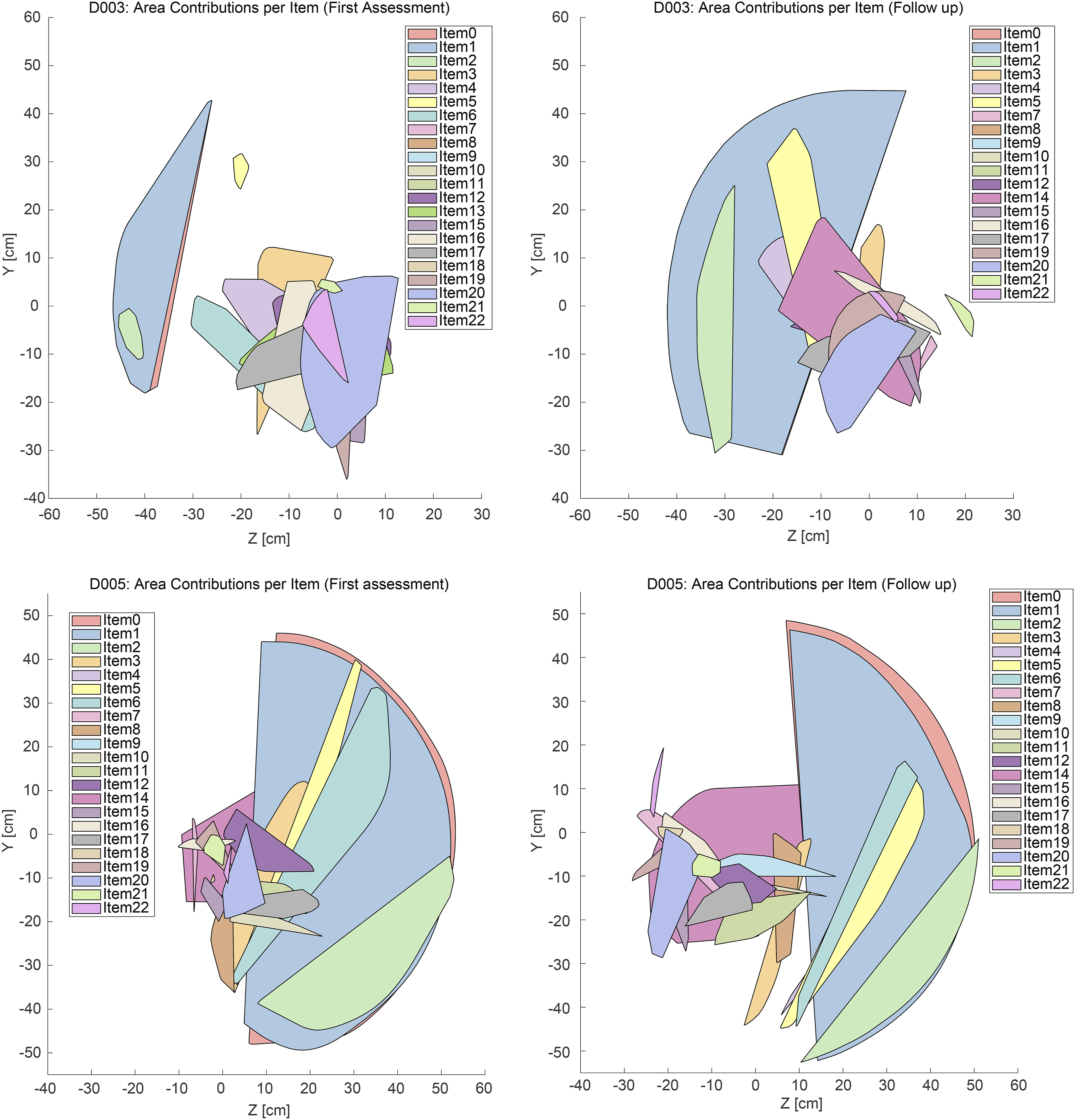
3.3. Kinematic analysis of individuals with SMA
Changes in kinematic metrics between baseline and follow-up were generally small, supporting the overall stability of upper limb function over one year. As shown in Supplementary Table 3, frontal workspace area decreased slightly from 37.3% to 35.4%, transverse workspace area from 19.0% to 18.6%, and workspace volume from 21.7% to 20.5%, while curve efficiency increased modestly from 0.38 deg/s to 0.44 deg/s. RULM scores also showed a small increase from 22 to 22.5 points. Overall, these results indicate that both kinematic metrics and clinical scores remained stable at the group level, with only non-significant trends observed.
Strong cross-sectional correlations were observed between kinematic metrics and RULM scores at follow-up, particularly for frontal workspace area (ρ = 0.81, p = 0.015) and curve efficiency (ρ = 0.90, p = 0.002). Correlations with transverse workspace area and workspace volume were weaker but still statistically significant (ρ = 0.74, p = 0.036 for both cases) (Supplementary Figure 2). These results indicate meaningful associations between kinematic measures and clinical function at each time point.
Figure 5 shows the progression of the kinematic metrics between baseline and follow-up assessments. Changes in the workspace areas (frontal and transverse), workspace volume and curve efficiency after one year from the first assessment for SMA group. Each marker represents one subject and the fill is assigned according to the Brooke score.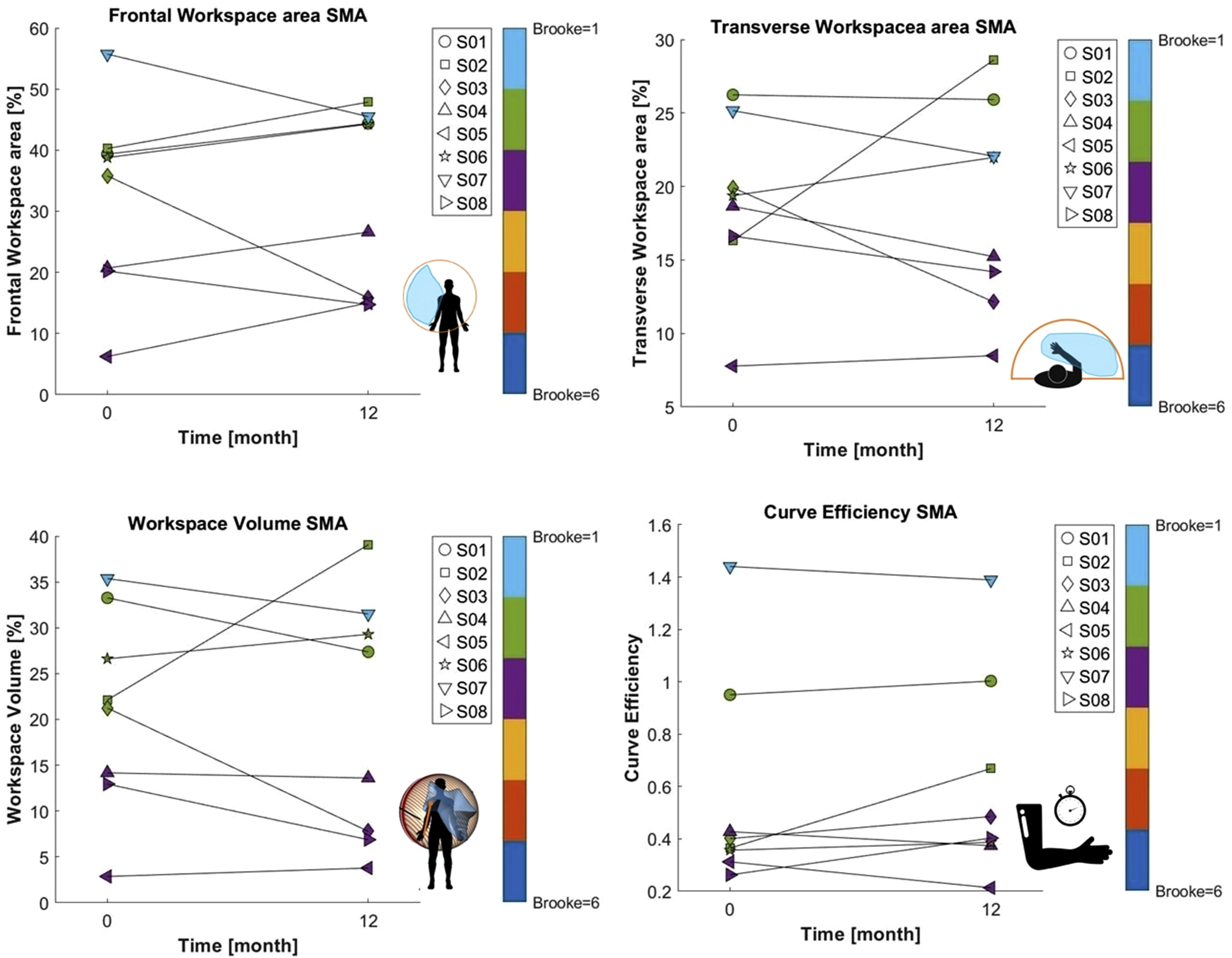
At the individual level, changes in RULM scores were ≤3 points for all eight participants, reflecting clinical stability. Five individuals (S01, S02, S04, S05, S08) also showed small changes in frontal workspace area (≤10 percentage points) (Figure 6). Only one participant (S03) exhibited a larger change in workspace area despite minimal variation in RULM, while another (S07) showed a stable RULM but a workspace area change slightly above 10 percentage points. Overall, these results confirm that most individuals with SMA remained clinically stable over the one-year follow-up. Transverse workspace area of individual S02 at baseline and follow-up. Different colors represent the items of the RULM scale.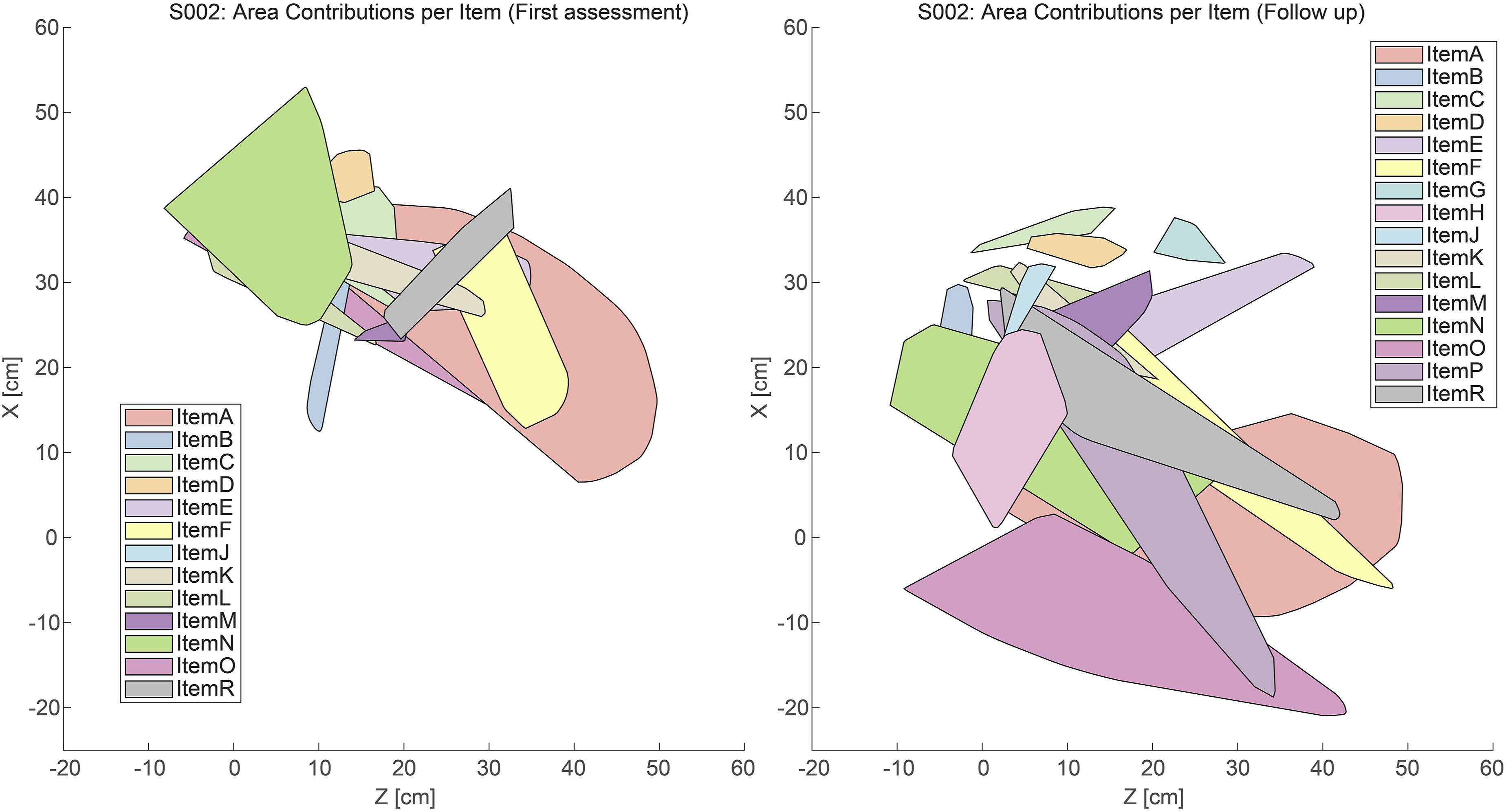
4. Discussion
This study complements the few existing longitudinal reports using IMU-based metrics to assess upper limb motor function in children and adolescents with neuromuscular diseases.25,29 By extracting and analyzing IMU-derived kinematic metrics (frontal and transverse workspace area, workspace volume, and curve efficiency), we aimed to evaluate their trends over time and their relationship with conventional motor function assessment through clinical scales (PUL and RULM), using the following terminology: “consistency” refers to general trends at the group level, “concordance” to cross-sectional correlations at single time points, and “alignment” to visual agreement of individual trajectories over time.
Strong cross-sectional correlations were found between most of the IMU-derived kinematic metrics and the corresponding clinical scales, supporting their potential as complementary tools to assess upper limb function. 12 This finding supports the potential of kinematic metrics, such as workspace area, workspace volume, and curve efficiency, to objectively quantify upper limb motor function in children with neuromuscular diseases and to complement traditional clinical assessments.
Changes in clinical scores over the one-year follow-up were generally minimal, reflecting stability in upper limb function. This observation aligns with previous reports showing that fluctuations below approximately 4 points in PUL or RULM likely fall within the range of measurement variability rather than true clinical change.27,28 The lack of larger changes suggests either true clinical stability or limited sensitivity of conventional scales to detect subtle functional variation over this time frame.
At the individual level, visual inspection suggested broadly similar patterns between clinical scores and IMU-derived metrics in most of individuals, with only a few notable exceptions highlighted in Figure 4. Among the kinematic measures, frontal workspace area appeared as one of the metrics most likely to capture small longitudinal changes, though these were often subtle and did not always align perfectly with changes in clinical scores.
Notably, some participants exhibited interesting discrepancies. Individual D03 showed an increase in frontal workspace area despite no change in PUL score; this improvement was supported by an increase in Brooke score, suggesting a discrepancy between kinematic and clinical assessments that warrants further investigation (Figure 4). Individual D05 also demonstrated an improvement in frontal workspace area, whereas their PUL score indicated a functional decline. These examples illustrate that kinematic metrics and clinical scales may provide partially different information regarding upper-limb performance.
Transverse workspace area and workspace volume also provided useful information but required cautious interpretation. For instance, individual S02 showed an apparent increase in transverse workspace area, initially suggesting improvement. Further evaluation of the kinematic data and corresponding video analysis revealed that this change was due to a compensatory movement during item O rather than true functional gain (Figure 6). This finding underscores the importance of contextualizing kinematic data with qualitative movement patterns rather than relying solely on numerical trends. Similar considerations apply to workspace volume, which reflects overall upper limb motor capacity but may be affected by analogous interpretative limitations.
Curve efficiency correlated with functional status at single time points but showed less consistent longitudinal trends, potentially influenced by inter-individual differences in movement speed and task execution. It is worth noting that the absence of statistically significant differences between baseline and follow-up assessments in kinematic metrics does not necessarily indicate a lack of clinically meaningful change. These measures may reflect individual variations in upper-limb performance over time, although their clinical relevance requires further study.
Several limitations should be noted. The sensitivity of workspace-based metrics can be influenced by small variations in experimental setup, such as arm positioning or table distance, for example, if an individual is seated farther from the table, a larger reaching area is required, potentially affecting comparability across sessions. Moreover, IMU recordings were performed while participants completed the PUL or RULM scales. Therefore, the derived kinematic metrics do not represent an unrestricted assessment of maximal upper-limb workspace, but rather the movement repertoire elicited by the specific tasks included in these clinical scales. In addition, these scales do not prescribe specific speed or amplitude for task execution, as their scoring can be achieved independently of such parameters. This lack of standardization may reduce the ability of certain kinematic measures to consistently capture disease progression. Manual segmentation of movement tasks from video footage may also introduce subjectivity. Finally, the sample size was small, highlighting the need for larger, multicenter studies with standardized protocols and quantitative indices (e.g., effect size, minimal detectable change) to more rigorously evaluate the potential of IMU metrics to capture subtle variations in upper-limb function.
While this study demonstrates the technical feasibility of a multi-sensor IMU system for longitudinal upper-limb assessment, the current setup including seven sensors, calibration, and manual video-based segmentation is resource-intensive. This may limit its use in routine clinical practice. Future work should explore simplifications such as fewer sensors, streamlined calibration, and automated analysis to improve scalability and integration into clinical workflows.
In summary, traditional clinical scales remain essential but may miss subtle changes in upper limb function. IMU-based assessments provide a complementary approach, offering objective, quantitative data that aligns broadly with conventional measures while capturing minor functional variations. These findings support the potential integration of wearable motion tracking into longitudinal monitoring in both research and clinical practice.
5. Conclusions
This study demonstrates the feasibility of using an IMU-based system to assess upper limb motor function progression in children with neuromuscular diseases. Kinematic metrics, particularly frontal workspace area, showed strong cross-sectional correlation with standard clinical scales and provided complementary quantitative information during longitudinal follow-up. While most participants exhibited patterns broadly aligned with clinical assessments, minor discrepancies highlight the importance of standardized task execution and careful interpretation of sensor-based data. The exploratory nature of these longitudinal findings suggests that further studies in larger cohorts are needed to confirm the utility of IMU-based metrics as a complementary tool in clinical practice. Future work should aim to refine task protocols, ensure technical reproducibility, and validate these metrics across diverse neuromuscular conditions, supporting a more sensitive and objective evaluation of therapeutic efficacy.
Supplemental material
Supplemental material -IMU-based workspace area as a promising complementary tool to assess upper limb function in Neuromuscular Diseases: A one-year follow-up
Supplemental material for IMU-based workspace area as a promising complementary tool to assess upper limb function in Neuromuscular Diseases: A one-year follow-up by Alessandra Favata, Jesica Expósito-Escudero, Roger Gallart-Agut, Julita Medina-Cantillo, Carme Torras, Josep M. Font-Llagunes, Rosa Pàmies-Vilà, Daniel Natera-de Benito in Journal of Neuromuscular Diseases.
Appendix
Abbreviations
Duchenne muscular dystrophy
Inertial measurement units
Interquartile range
Neuromuscular diseases
Performance of Upper Limb
Revised Upper Limb Module
Spinal muscular atrophy.
Footnotes
Acknowledgements
JEE and DNdB are members of the European Reference Network for Neuromuscular Diseases ERN-NMD - Project ID N° 870177.
Ethical considerations
The study received approval from the Ethical Committee of the Hospital Sant Joan de Déu (Esplugues de Llobregat, Barcelona, Spain; approval number: PS-28-22).
Consent to participate
Informed written consent was obtained from all participants and, in the cases where the participants were under 16 years of age, from their parents as well.
Consent for publication
Written informed consent for publication of their clinical details was obtained from the patient/parent/guardian/relative of the patient. We confirm that consent has been obtained to publish images or descriptions of individuals and documentation can be produced if required.
Author contributions
Alessandra Favata contributed to data acquisition, analysis and interpretation and manuscript writing; Jesica Expósito-Escudero contributed to patient recruitment, data interpretation and manuscript revision; Roger Gallart-Agut contributed to data analysis and interpretation and manuscript revision; Julita Medina-Cantillo contributed to patient recruitment, data interpretation and manuscript revision; Carme Torras contributed to data interpretation and manuscript revision; Josep M. Font-Llagunes contributed to the study design, data interpretation and manuscript revision; Rosa Pàmies-Vilà contributed to the study design, data interpretation and manuscript revision. Daniel Natera-de Benito contributed to the study design, data interpretation and manuscript writing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Fundació La Marató de TV3 under Grants No.202023-30, 202023-31 and 202023-32. This study has been funded by Instituto de Salud Carlos III (ISCIII) through the project “CP22/00141” and co-funded by the European Union.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during the current study are available from the corresponding author upon reasonable request.
AI statement
The authors used an artificial intelligence tool (ChatGPT, OpenAI) solely for language proofreading. No artificial intelligence tools were used for scientific content generation, data analysis, or interpretation of results. The authors reviewed and take full responsibility for the final content of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.