
Abstract
Diabetic patients exhibit delayed skin wound healing due to chronic hyperglycemia, which results in prolonged tissue recovery. In this work, a skin dressing was synthesized using three natural composites: chitosan, gelatin, and Zingiber officinale herb, commonly known as ginger (CH+GE+ZO). The dressing was applied to albino Wistar rats, which then received an intraperitoneal injection of Alloxan at a dose of 150 mg/kg. Incision caused skin wounds. The antioxidant markers were quantified. A histological study was conducted to evaluate the effectiveness of the skin healing process. Analysis of the oxidative balance revealed a significant (p < .001) increase in enzymatic antioxidant activities in the CH+GE+ZO-treated group compared to the diabetic group. A considerable increase in non-enzymatic markers was observed compared to the diabetic group (p < .001). Histologically, the application of a composite synthesized by CH+GE+ZO dressing showed an improvement in the healing process, compared to controls, and a total recovery of wounds was observed around Day 13. This was characterized by a progressive reepithelialization, a structured organization of the layers of the epidermis, as well as a partial restoration of the cutaneous appendages. Overall, the synthesized biological dressing actively contributes to tissue repair and skin healing.
Introduction
The skin, an organ of communication and exchange, serves as the body’s primary defense against external damage. Its vital functions include mediating the physiological process of wound healing, which facilitates tissue renewal through distinct catabolic and anabolic phases, including inflammation, the eradication of damaged cells, cellular proliferation, and tissue remodeling. 1 The integrity of the skin can be compromised by various factors, including trauma, infections, vascular conditions, or tumors. Such damage often results in wounds, which initiate the physiological process of healing. In healthy individuals, wound closure typically occurs spontaneously through local care methods (secondary intention healing) or via surgical intervention (primary intention healing), therefore proceeding without complications. However, in individuals with systemic conditions such as diabetes mellitus, the healing process is frequently impaired, leading to various complications. 2 Health professionals are confronted with these complications and then aim to implement innovative therapeutics to fight against the infection. Vegetable-based dressings composed of natural polymers and plant-derived biomaterials provide a favorable wound healing environment by promoting tissue regeneration and offering antimicrobial, anti-inflammatory, and antioxidant activities. Such formulations, including gelatin/chitosan–based systems and plant mucilage–derived dressings, have shown improved wound closure and biocompatibility, particularly in infected wounds.3,4 Today, the high cost of care and the ineffectiveness of certain medications, which, in most cases, do not provide rapid and satisfactory healing in diabetics, are limiting factors for their use. Faced with this situation and in order to have effective results that meet the expectations of patients, extensive research around the world has been undertaken on the physiological effects of certain natural compounds that may be beneficial in wound healing in diabetic patients. 5 Chitosan (CH) is a cationic hydrocolloid with film-forming properties. 6 It has a great potential for a wide range of medical applications due to its biocompatibility, non-toxicity, and cost-effectiveness.7–9 Moreover, numerous studies have shown various biological effects10–12 such as antioxidant, antimicrobial, and healing properties since CH allows the reconstruction of all skin layers as well as the vascular network.13,14 At present, various dressings containing chitin or CH, such as Chitodine→, Chitodine, Tegasorb, and others, are already marketed. 15 On the other hand, gelatin (GE) is a natural polymer derived through the partial hydrolysis of collagen. Its relevance primarily derives from its excellent biocompatibility and inherent biodegradability. 16 Thanks to its acidic charge, this polymer can create polycationic complexes, making it an effective material for molecular release. 17 GE is commonly used as a primary material for dressings due to its biological activity, making it an effective hemostatic agent for temporary wound protection. 18 Various GE-based dressings are commercially available. Moreover, the combination of CH with other compounds, such as GE, can induce rapid coagulation, even under conditions of severe hemorrhage. 19
In order to increase the biological properties of CH+GE, other natural components can be added to enhance these therapeutic efficacies. For this purpose, the plant Zingiber officinale (ZO), commonly known as ginger, was utilized in the synthesis of the skin dressing. Its medicinal properties are due to its wealth of natural substances, including anti-inflammatory and antimicrobial activities. 20 The current study consists of the formulation and evaluation of a CH+GE+ZO-derived biologic wound dressing for diabetic rats.
Materials and Methods
Plant Material
The plant species used was Z. officinale L. (ZO), recognized as ginger. Dry Rhizomes were purchased from a local herbalist from Sfax (Tunisia). They were washed under running water. After drying at room temperature (25°C ± 2°C) for 7 days, the rhizomes were cut into small pieces and then crushed using an electric grinder. The powder was stored in glass boxes and labeled, then kept in the shade until use.
Dressing CH+GE+ZO Preparation
A solution of 1% w/v was prepared by dissolving 1 g of beef skin gel (powder, gel strength ~225 g, Bloom, Sigma-Aldrich, USA) in 100 mL of distilled water (purity 99%, conductivity <5 μS/cm) for 30 minutes. The solution was then heated at 50°C for 30 minutes under continuous agitation. CH (DDA ~90%, Sigma-Aldrich viscosity, USA). 1% w/v CH solutions were prepared by dissolving in 1% acetic acid (99.8%, Sigma-Aldrich, Darmstadt, Germany) and stirring overnight at room temperature. A 4% solution of ZO was added to the mixture. All components of the solutions were filtered through 0.55 μm PTFE filter membranes to remove impurities. 3
Total Polyphenols (PPT) Determination
The determination of polyphenols was carried out using the Folin-Ciocalteu reagent according to the method of Dewanto et al. 21 The reagent, of yellow color, consists of a mixture of phosphotungstic acid (H3PW12O40) and phosphomolybdic acid H₃PMo₁₂O₄₀, which, upon reduction by the action of polyphenols, leads to the formation of a new complex of tungsten oxide (W8O23) and molybdenum oxide (Mo8O23) of blue color. The procedure consisted of adding 2 mL of 7.5% sodium carbonate solution to 0.5 mL of each sample solution in a test tube. After shaking and incubation for 5 minutes, 2.5 mL of 1 N Folin-Ciocalteu reagent was added. The mixture was immediately kept in darkness for 30 minutes at room temperature. The absorbance of each solution was directly measured at 655 nm. A calibration curve was performed in parallel under the same experimental conditions using gallic acid as a positive control. Thus, 500 mg of gallic acid was diluted in 10 mL of ethanol, and then the volume was adjusted to 100 mL with distilled water (stock solution). Dilute solutions of known gallic acid concentrations were prepared (0, 50, 100, 150, 250, and 500 mg/L). The quantification of polyphenols was done by comparing the absorbance of the studied solution to that of the calibration curve. The results were expressed as mg equivalent of gallic acid per gram of dry vegetable matter (GAE/g DM). The quantification was repeated three times for the studied extract.
Total Flavonoids (FVT) Determination
The method used was the colorimetric method using aluminum trichloride (AlCl3), developed by Luaces et al. 22 This method is based on the formation of a yellow complex between aluminum trichloride and flavonoids. Thus, in test tubes, 250 μL of the tested extract and 1 mL of distilled water were placed successively. At an initial time (0 minutes), 75 μL of a NaNO2 solution (5%) was added. Five minutes later, 75 μL of AlCl3 (10%) was incorporated. After 6 minutes, 1 mL of NaOH (1N) and 2.5 mL of distilled water were added. The absorbance of each mixture obtained was directly measured at 430 nm using a UV-visible spectrophotometer.
Animals
Our study was conducted on adult male rats of the Wistar strain bred at the Pasteur Institute in Tunis, each weighing approximately 180 g. The animals were placed in a pet store where the temperature was maintained at 25°C (2 degrees), humidity at 60% (5%), and the light/dark cycle at 12/12 h. The animals have free access to water and food. They received a normal diet: concentrated, energetically balanced, and coming from SICO, Sfax. This study followed the guidelines for the care and use of laboratory animals of the Faculty of Sciences of Sfax (Tunisia), which refer to the Guide for the care and use of laboratory animals, and was approved by the local ethics committee (Approval No.: G/A/SV/2016/001).
Induction of Diabetes
Experimental diabetes was induced in animals by intraperitoneal injections of Alloxan at a dose of 150 mg/kg. The onset of diabetes was confirmed by classic symptoms (polyuria, polydipsia, and polyphagia) and hyperglycemia, then detected by test strips. Diabetic animals were divided into four groups Table 1:
Summary of Experimental Groups, Treatments, Wound Induction, and Sample Size.

Group I: Normal control group
Group II: Diabetes control group (Al-DM) (150 mg/kg Alloxan in i.p).
Group III: Diabetic rats with excision wounds (Al-DM/wound)
Group IV: Diabetic rats treated with the dressing CH+GE+ZO on excision wounds (Al-DM/CH+GE+ZO).
Incision Wound Model
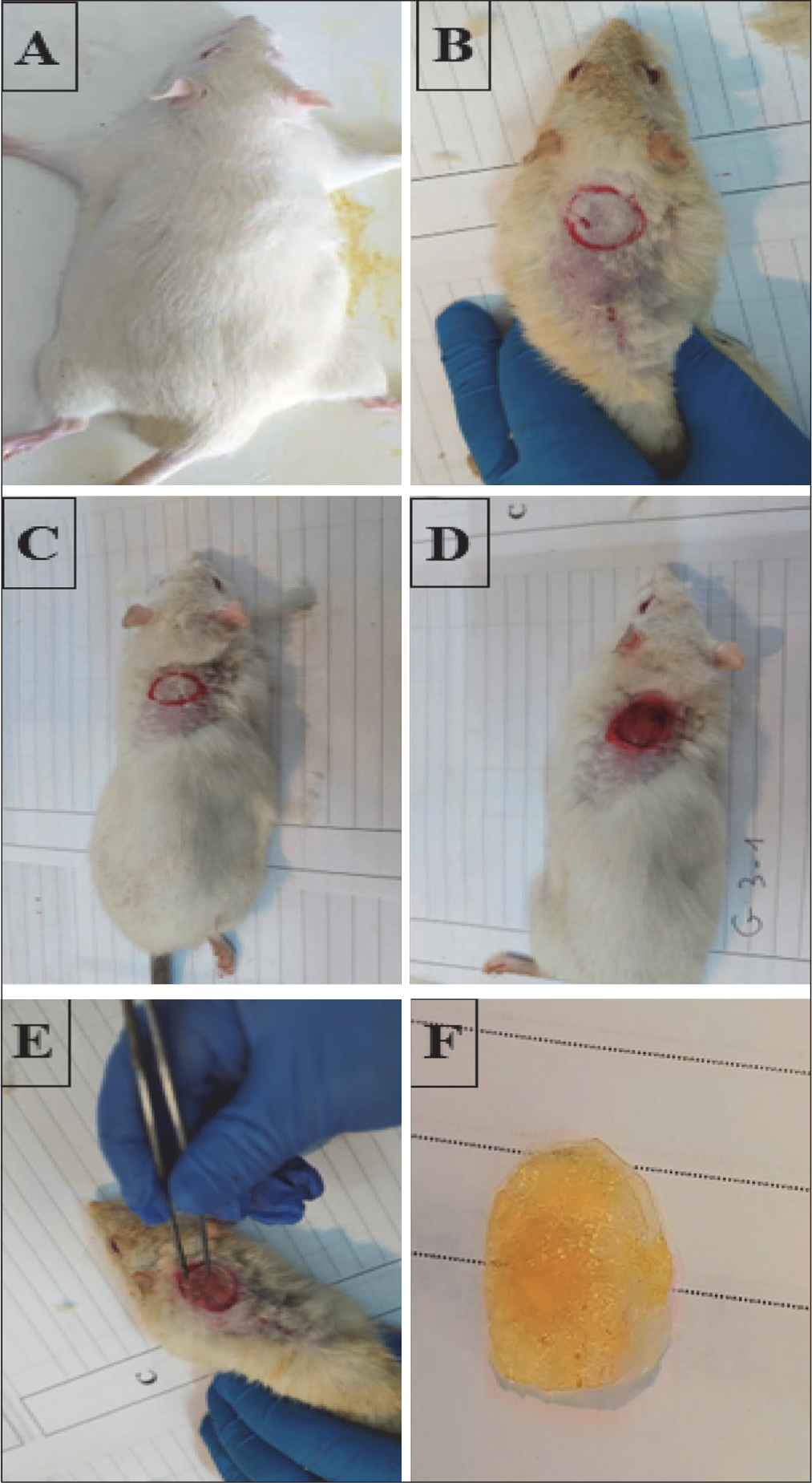
Once the rats were anesthetized by inhalation of diethyl ether, the dorsal neck area was shaved using a razor blade, pliers, and scissors. The depilated part was then disinfected using surgical alcohol 70°. A circular wound of 2 cm in diameter (drawn using a circular device) was created on the spine using a sterile scalpel blade (Figure 1). After wound provocation, today is designated Day 0, and treatment with the ZO-based dressing was carried out daily. The animals were treated at 1, 3, 5, 7, 9, 11, 13, and 15 days after the injury.
Wound Induction in Diabetic Rats and Application of the Dressing CH+GE+ZO. A: Anesthetized Rat; B, C: Shaving; D, E: Causing Wounds: A Circular Part With a Diameter of 2 cm Was Created on the Spine Using a Circular Vertebral Device, Then Wounds Were Created Using a Sterile Scalpel Blade; F: the Dressing CH+GE+ZO.
Determination of Blood Sugar
During the handling period (from Day 1 to 15), blood glucose values were measured. The first measurement was performed in order to check the onset of diabetes in Alloxan-treated rats, using batches I and IV (before starting treatment). It was measured in the fasting state, 72 h after administration of the diabetogenic product. If the test was positive (onset of disease), then the manipulation would start on the same day (time t = 0 of the manipulation); otherwise, Alloxan is reinjected until diabetes symptoms develop. After blood glucose measurement, three others were measured every 3 days and at fixed times using ACCU-CHEK Active strip glucose. Blood was taken from the rat’s caudal vein by means of a small incision in the distal part of the tail. After each established operation, the tail of the animal had to be disinfected using cotton soaked in Betadine. No mortality occurred during the experiment.
Dissection and Removal of Organs
After decapitation, rats were dissected to remove skin. This organ was first cleared of hair, rinsed with NaCl at 0.9%, and weighed. The skin was placed in 30% formalin (fixation) for the purpose of performing histological cuts.
Determination of Plasma Parameters
All the plasma parameters, Serum levels of aspartate aminotransferase (AST), alanine aminotransferase (ALT), and creatinine were measured in frozen aliquots of serum by standardized enzymatic procedures using commercial kits (Biolabo, France) on an automatic biochemistry analyzer (Vitalab Flexor E, USA).
Determination of Antioxidant Enzyme and Non-enzymatic Activities
The catalase activity (CAT) was estimated according to the Aebi method, 23 based on the hydrolysis of H2O2 and the resulting decrease in absorbance at 240 nm. The CAT activity was calculated in terms of μmol H2O2 consumed/min/mg of protein. Superoxide dismutase (SOD) activity was determined by monitoring the photochemical reduction of nitro blue tetrazolium (NBT) as described by Beauchamp and Fridovich. 24 One unit (U) of SOD activity was the amount of enzyme required to cause 50% of inhibition of NBT reduction at 560 nm. The activity of SOD was expressed as protein U/mg. Glutathione peroxidase (GPx) activity was measured according to Flohe and Gunzler’s study. 25 The enzymatic activity was expressed as nmol of GSH oxidized/min/mg protein. Glutathione (GSH) levels were measured using Ellman’s method, 26 as modified by Jollow et al., 27 and total GSH values were expressed as nanomoles per milligram of protein. The non-protein thiols (NPSH) were performed according to the method of Ellman, 26 and the results were expressed as nanomoles per milligram of protein.
Histological Study
All skin samples were fixed with 10% formalin and used for histological examination by light microscopy. They were then integrated into paraffin, dissected in series at 5 μm, and colored with modified trichrome and hematoxylin and eosin staining.
Statistical Analysis
Statistics were performed on GraphPad Prism 10.0 for Windows (GraphPad Software, San Diego, CA). The one-way ANOVA was applied to assess significant differences between treatment groups, followed by Tukey’s post hoc correction at p < .05.
Results
Polyphenol and Flavonoid Content
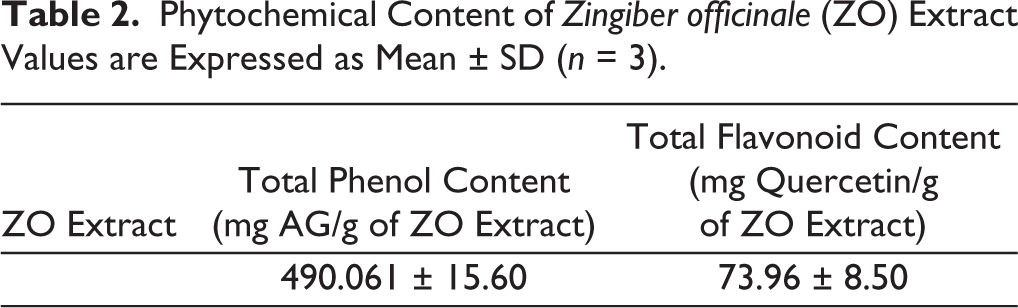
The total phenolic content, determined using gallic acid as a standard, was found to be 490.061 ± 15.60 mg of gallic acid equivalents per gram of extract (mg GAE/g). Regarding the flavonoid content, quercetin was used as the standard. The analysis showed that the ethanolic extract from the Z. officinale rhizomes contained a total flavonoid content of 73.96 ± 8.50 mg of quercetin equivalents per gram of extract (mg QE/g) (Table 2).
Phytochemical Content of Zingiber officinale (ZO) Extract Values are Expressed as Mean ± SD (n = 3).
Evaluation of Pre-sacrifice Parameters in Controls and Diabetic Rats
1. Determination of blood glucose levels
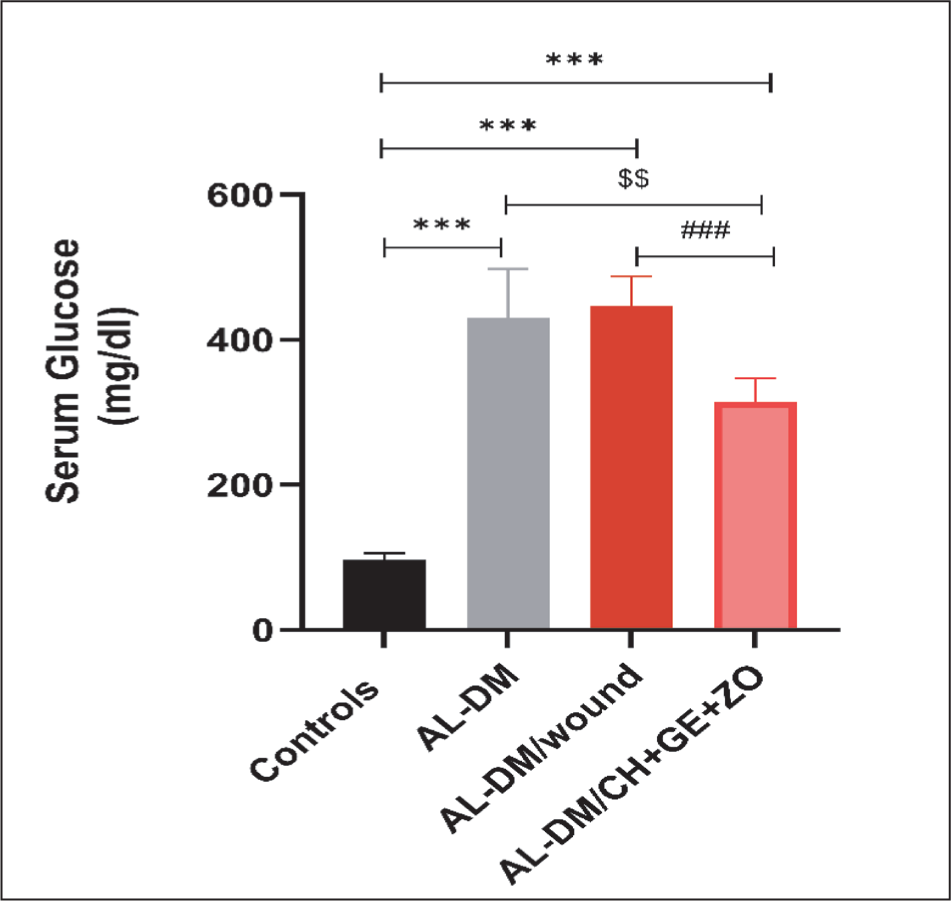
During the experimental period, the initial blood glucose measurement was performed to confirm diabetes induction in Alloxan-treated rats. The baseline reference for normal blood glucose was established using measurements from the G I group (Controls), and obtained after an overnight fast, at 72 hours post-administration of Alloxan. As shown in Figure 2, diabetic rats (GII, GIII, and GIV) exhibited a significant increase in blood glucose levels, as compared to the normal controls. These findings were consistent with a previous study. 28 The observed hyperglycemia reflects a disruption of carbohydrate metabolism due to pancreatic dysfunction, resulting in impaired glucose uptake by target cells and reduced hepatic glucose storage. No significant differences in blood glucose levels were detected among the diabetic groups throughout the study period, thus indicating that topical application of the dressing in diabetic rats did not influence systemic blood glucose levels (local, external application).
Fasting Blood Glucose Levels in Rats Before Sacrifice. Values Are Means ± SEM (n = 6). Al-DM, Al-DM/Wound and Al-DM/CH+GE+ZO Versus Control Group: *p < .05; **p < .01; *p < .001; Al-DM/Wound and Al-DM/CH+GE+ZO Versus Al-DM: $$p < .01; Al-DM/CH+GE+ZO Versus Al-DM/Wound: ###p < .001.
Transaminase (AST and ALT) Activities in Plasma of Control, Diabetic Rats, Diabetic Wounded Rats, and Diabetic Rats Treated Topically with CH+GE+ZO
The effect of CH+GE+ZO on the plasma activities of transaminases (AST and ALT) in all rats was illustrated in Figure 3. These results revealed a significant increase in ALT activity in diabetic Groups (II, III, and IV) as compared to the controls. Furthermore, treatment with the topical dressing CH+GE+ZO application resulted in a significant reduction (p < .01) in ALT when compared to the untreated diabetic control group (Al-DM) (Figure 3A). The ALT activity in wounded diabetic rats receiving a topical CH+GE+ZO treatment was significantly lower (p < .005) than that measured in the untreated wounded diabetic group. This suggests that the topical CH+GE+ZO treatment provided a significant therapeutic effect, probably by mitigating the systemic inflammatory response and/or reducing stress associated with the non-healing diabetic wound state.
Plasma Transaminases (ALT and AST) Activities of Controls, Al-DM, Al-DM/Wounds, and Al-DM/CH+GE+ZO. Values Are Means ± SEM (n = 6). Al-DM, Al-DM/Wound and Al-DM/CH+GE+ZO Versus Control Group: **p < .01; *p < .001; Al-DM/Wound and Al-DM/CH+GE+ZO Versus Al-DM: $p < .05; $$p < .01; Al-DM/CH+GE+ZO Versus Al-DM/Wound: #p < .05; ##p < .01.
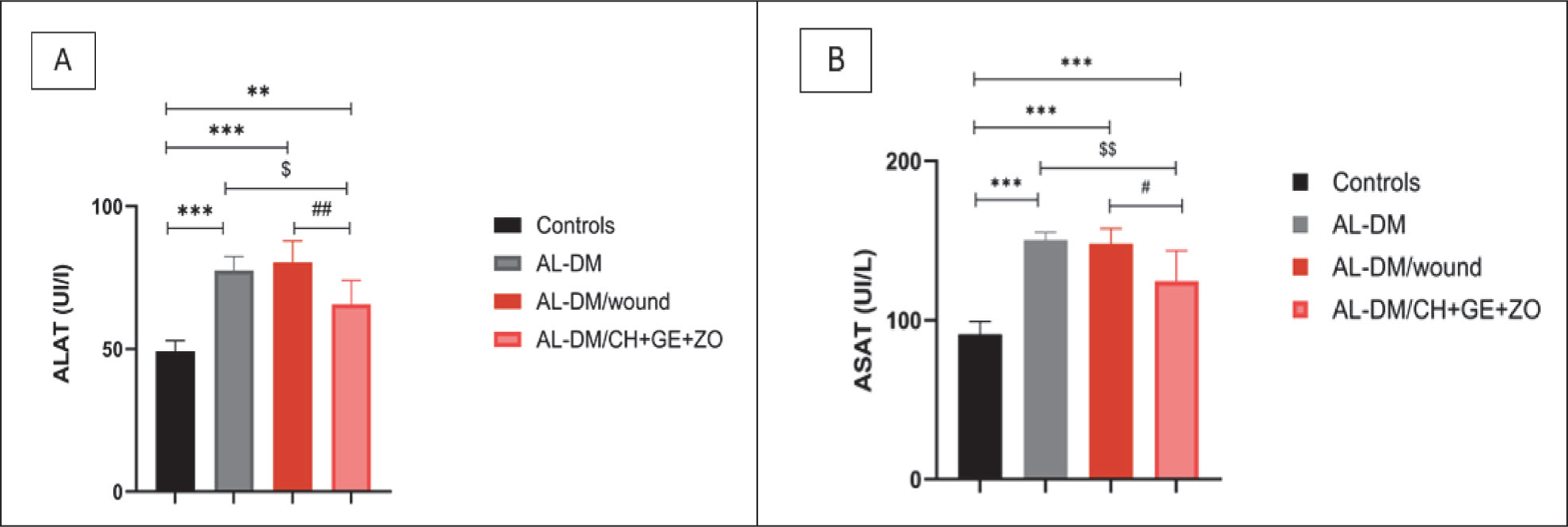
As for AST, the results were reported in Figure 3B. The results revealed that the activity of this enzyme increased with diabetes in rats. The statistical analysis indicated significant differences (p < .001) between Group I and the diabetic Groups II, III, and IV.
C-reactive Protein
The results related to the determination of the C-Reactive Protein (CRP) were presented in Figure 4.
CRP Levels in Plasma of Controls, Al-DM, Al-DM/Wounds, and Al-DM/CH+GE+ZO. Values Are Means ± SEM (n = 6). Al-DM, Al-DM/Wound, and Al-DM/CH+GE+ZO Versus Control Group: **p < .01; *p < .001; Al-DM/CH+GE+ZO Versus Al-DM/Wound: #p < .05.
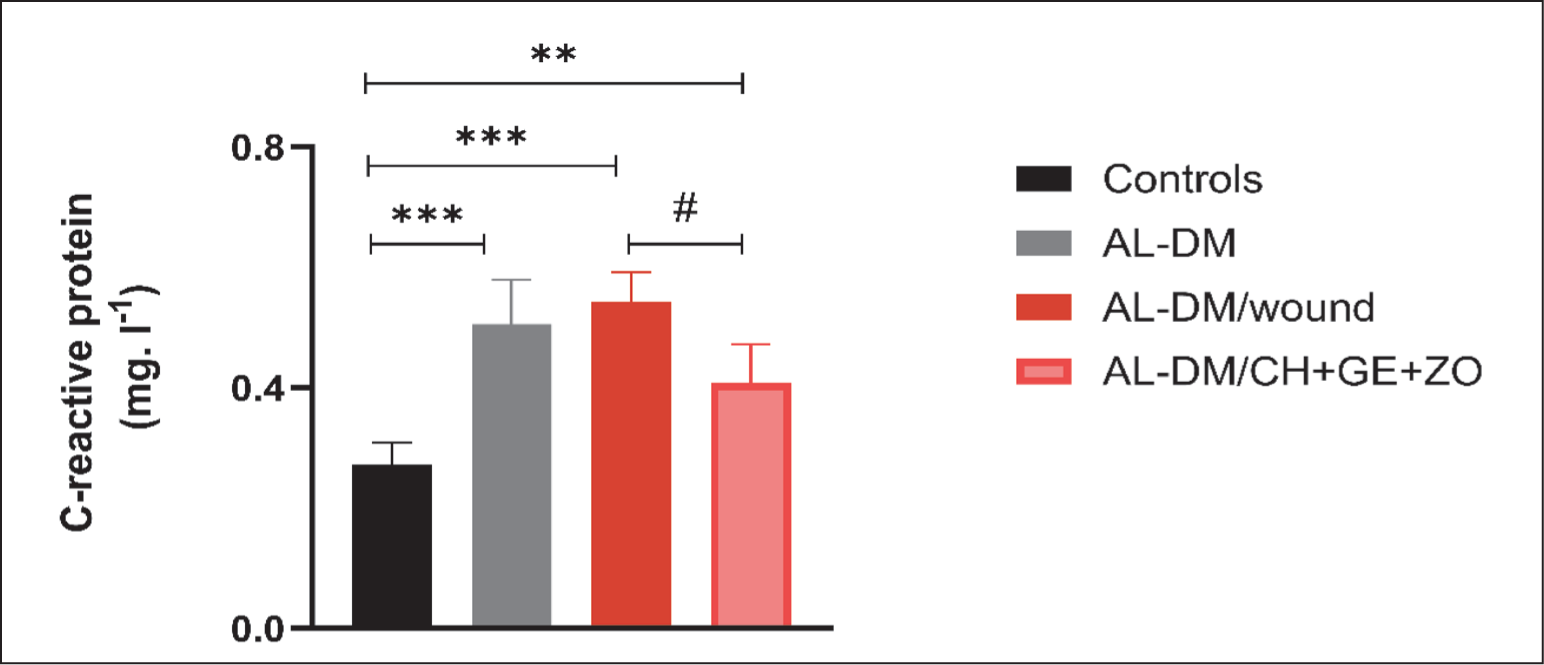
Assessment of CRP levels revealed a significant elevation across all treated groups compared to the control. Mean CRP values increased from 0.272 in Group I to 0.506, 0.54, and 0.408 in Groups II, III, and IV, respectively. Statistical analysis confirmed that while Groups II, III, and IV differed significantly from Group I (p < .01), no significant variations in CRP levels were observed between Groups II and III (p > .05).
Urea and Creatinine
Table 3 presents the results of urea and creatinine dosing in the different groups of rats. Our results showed that serum urea concentration varied between different groups. Statistical analyses revealed the presence of significant differences between diabetic rats II, III, and IV compared to the controls (Group I) (p < .001). However, no significant difference was observed between Group IV treated with the dressing and Groups II and III.
Plasma Levels of Creatinine and Urea of Controls, Al-DM, Al-DM/Wounded, and Diabetic Rats Treated Topically with CH+GE+ZO.

Study of Antioxidant Activity
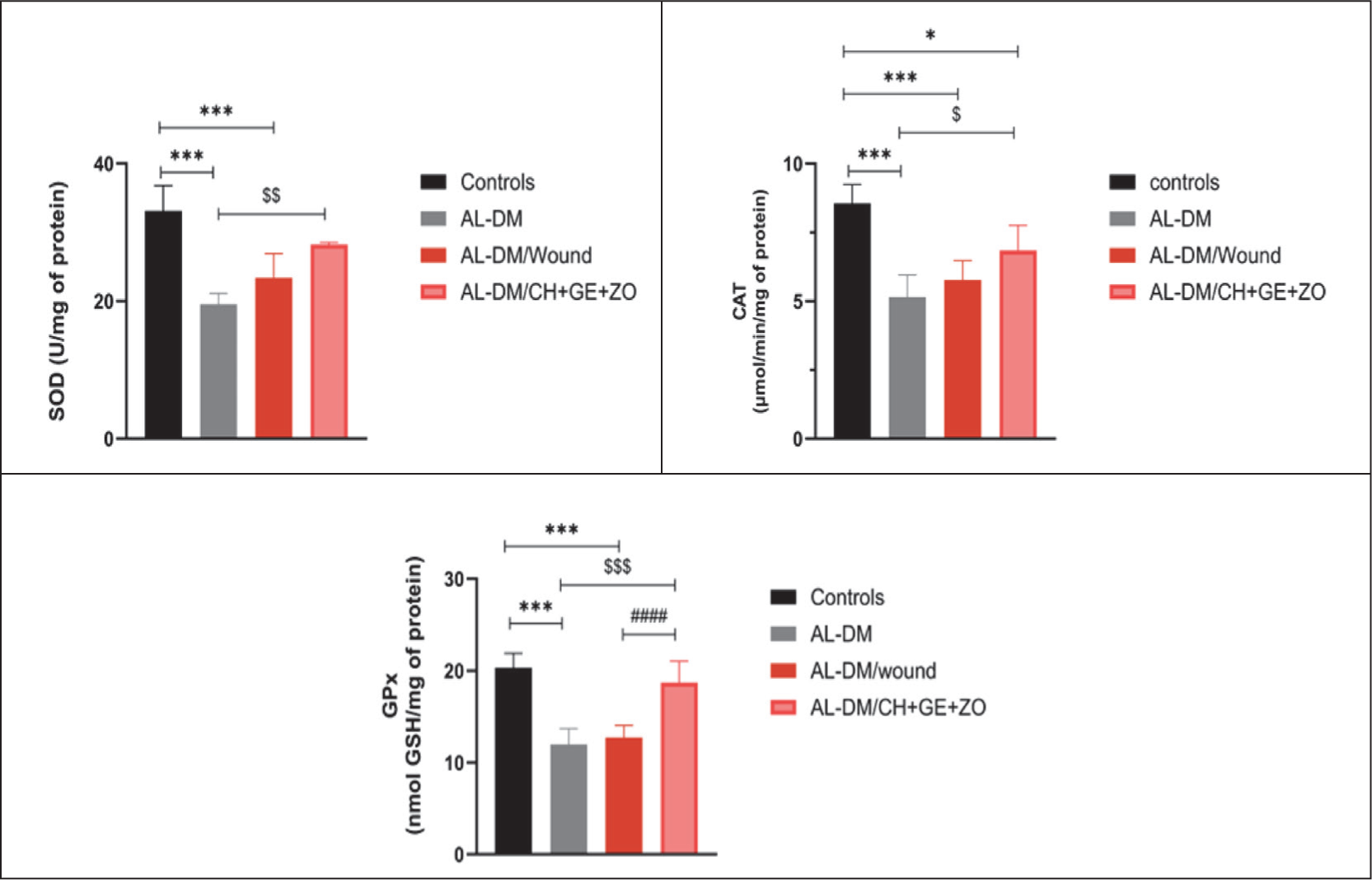
Determination of superoxide dismutase (SOD) activity
SOD activity results were displayed in Figure 5. An examination of this graph showed that the control group exhibited the highest SOD, approximately 33 U/mg protein, followed by Group IV treated with the biologic dressing (25 U/mg protein), then Group III (22 U/mg protein), and finally Group II (19 U/mg protein). The statistical analysis demonstrated the existence of highly significant differences (p < .001) between control Group I, as compared to diabetic Groups II and III, and no significant differences (p > .05) between control Group I and Group IV. Significant differences between Groups IV and Group II were also recorded (p < .001).
Determination of catalase (CAT) activity
The results of the CAT activity measured at the skin level are presented in the Figure 5. The results showed that the state of diabetes seemed to have a significant impact on the CAT rate (p < .001). The lowest amount of CAT, 5.156 μmol H2O2/min/mg protein, was observed in the diabetic Group II compared to the control group. Statistical analysis revealed significant differences in Groups II (p < .001), III (p < .001), and IV (p = .01) compared to the controls (Group I).
Determination of glutathione peroxidases (GPx) activity
Figure 5 illustrates the amounts of this parameter in the four groups of rats. Group I showed the highest GPx level of about 20 μmol GSH/min/mg protein. Statistical analysis revealed highly significant differences (p < .001) between Groups II, III, and IV in comparison with Group I.
Antioxidant Enzyme Activities (SOD, CAT, and GPx) in the Skin of Controls, Al-DM, Al-DM/Wounds, and Al-DM/CH+GE+ZO. Values Are Means ± SEM (n = 6). Al-DM, Al-DM/Wound and Al-DM/CH+GE+ZO Versus Control Group: *p < .05; *p < .001; Al-DM/Wound and Al-DM/CH+GE+ZO Versus Al-DM: $p < .05, $$p < .01, $$$p < .001; Al-DM/CH+GE+ZO Versus Al-DM/Wound: ###p < .001.
Determination of the GSH Level
Figure 6A illustrates the evolution of the GSH rate among the studied groups. Statistical analyses revealed the presence of significant differences between the four groups (p < .001). The results showed a very significant decrease (p < .001) in GSH concentration in Groups II, III, and IV as compared to Group I. However, this decrease was lower in Group IV compared to Groups II and III. The treatment of wounds with a dressing prepared from CH+GE+ZO dressings contributed to the normalization of this parameter.
Non-enzymatic Antioxidant Levels (GSH and NPSH) in the Skin of Control and Al-DM, Al-DM/Wounds, and Al-DM/CH+GE+ZO. Values Are Means ± SEM (n = 6). Al-DM, Al-DM/Wound and Al-DM/CH+GE+ZO Versus Control Group: *p < .05; **p < .01, *p < .001. Al-DM/Wound and Al-DM/CH+GE+ZO Versus Al-DM: $$p < .01, $$$p < .001. Al-DM/CH+GE+ZO Versus Al-DM/Wounds: #p < .05, ###p < .001.
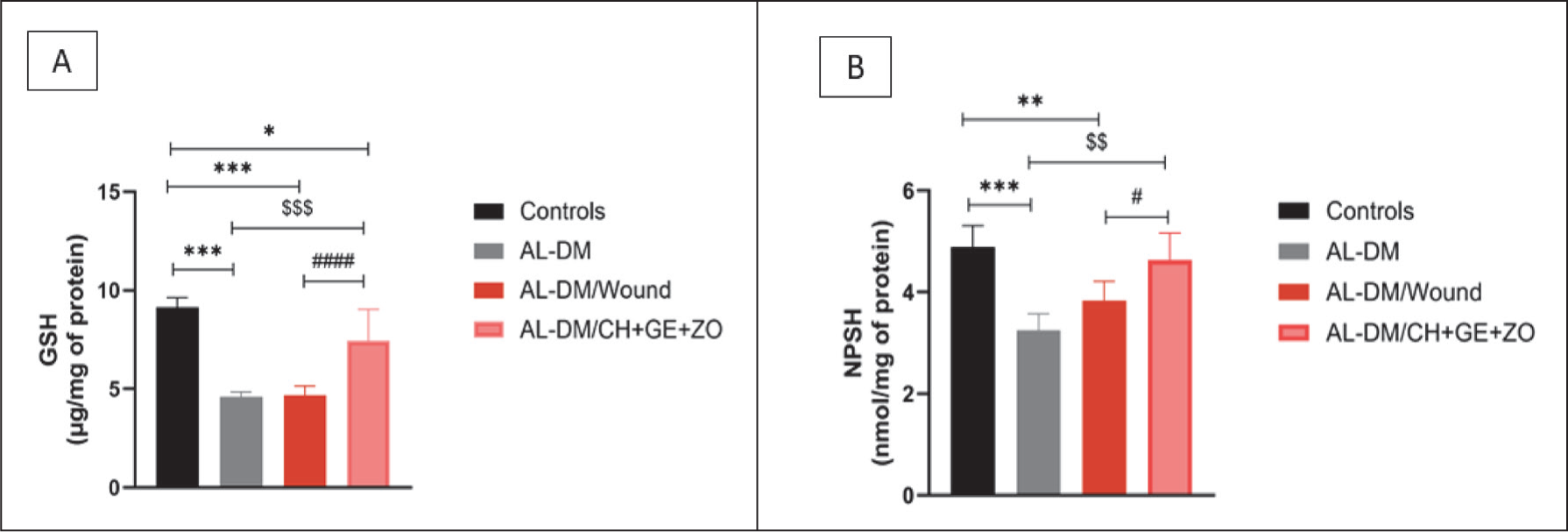
Determination of NPSH Levels
The results depicted in Figure 6B demonstrate that NPSH levels fluctuated according to the different experimental groups. The statistical analyses revealed the presence of significant differences between the four groups of rats. Indeed, a highly significant decrease (p < .001) was observed in the diabetic II group and Group III (p = .007) compared to Group I.
Evaluation of Wound Healing Evolution
The wound healing kinetics for Groups I, III, and IV are illustrated in Figure 7. Macroscopic observations revealed that the rate of wound contraction significantly accelerated starting from Day 3 post-induction, particularly in Groups I and III. This could be attributed to the mechanism of angiogenesis and the migration of fibroblasts, part of which differentiates into myofibroblasts responsible for the contraction of the wound, thus marking the beginning of the tissue phase.
Photographic Illustrations of the Wound Healing Process in the Different Experimental Groups on 0, 3, 6-, 9-, 12- and 15-days Post-wounding; and Area of Wounds (cm 2 ) at Different Time Points Following the Application of Preparations to the Surface of the Wounds.
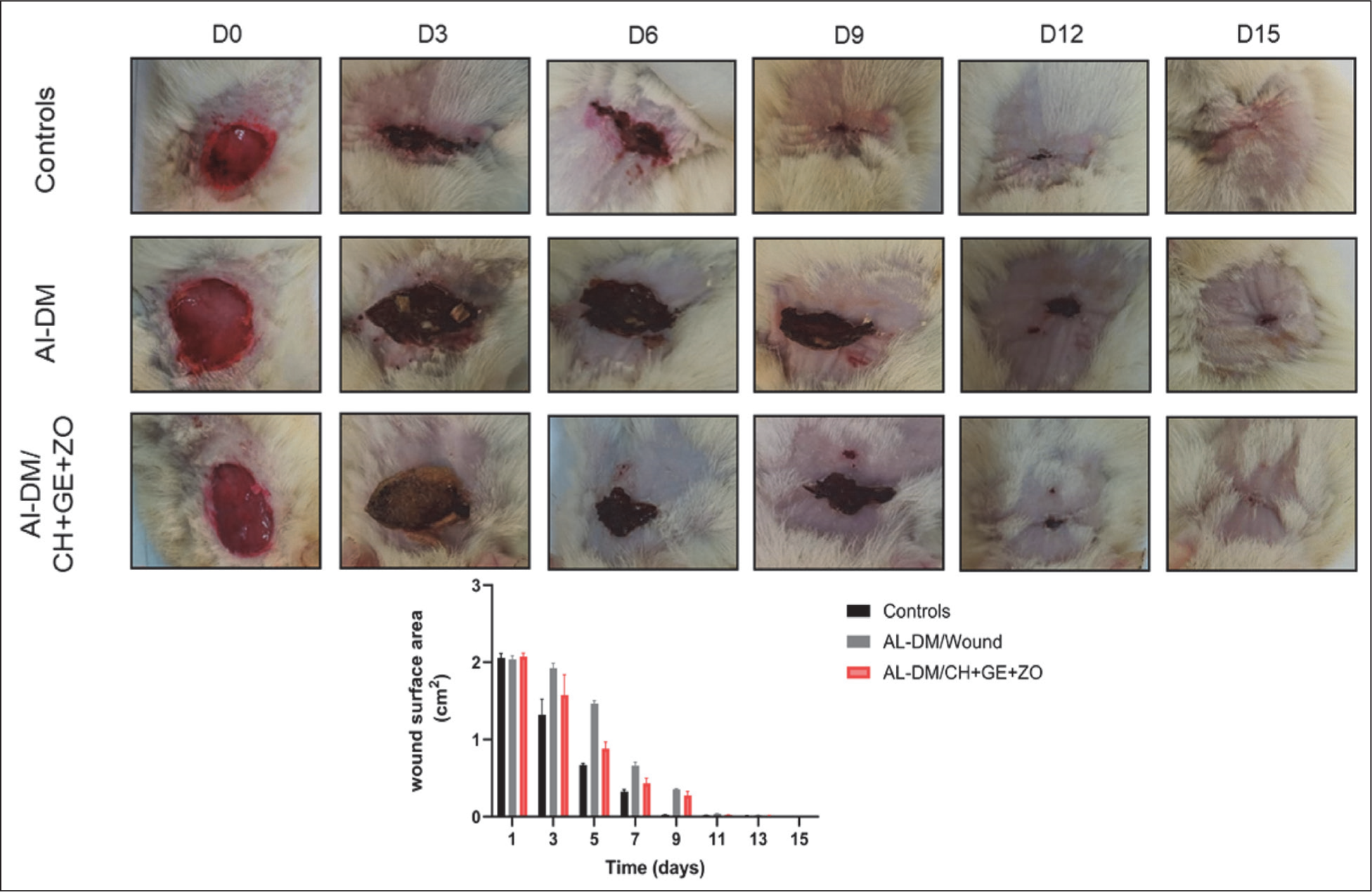
A reduction in average wound areas was observed in rats from different groups (Figure 7). The speed of healing is significant in Group I, as compared to diabetic Groups III and IV from Day 3. The initial wound surface area was standardized at 2.1 cm 2 for Groups II, III, and IV, ensuring a uniform baseline for evaluating healing efficacy. Following treatment, a progressive and significant reduction in wound area was observed across all experimental cohorts from Day 3 to 9. In the control group (Group I), the mean wound area decreased to 1.3 cm 2 by Day 3, reflecting an initial contraction rate of 38.13%, and further reduced to 0.08 cm 2 by the end of the observation period. Notably, the groups treated with the experimental dressing achieved complete wound closure (100%) by Day 13 post-wounding, indicating an accelerated recovery compared to the control. At the final observation on Day 15, prior to animal sacrifice, complete closure was maintained, confirming sustained tissue integrity and successful re-epithelialization.
The comparison of wound surface evolution between the two groups, I, II, III, and IV, showed that:
From Day 0 to 3: the healing profiles were similar across all groups. D3 to D5: A significant delay in wound closure was observed in Groups II, III, and IV compared with the control group (Group I). D7: The gap between the two groups increased further with a highly significant difference. D13: Groups II, III, and IV exhibited accelerated healing, resulting in markedly improved wound closure. D15: By Day 15, complete wound healing (100%) was achieved in all groups.
Under normal conditions, inflammatory, proliferative, and remodeling phases generally evolved linearly and synchronized at the wound level. However, the results obtained could be explained by the alteration of this synchronization due to diabetes. Similarly, the results showed that the application of CH+GE+ZO resulted in a significant improvement, as compared to Group III.
Wounds treated with the dressing prepared from the plant healed faster. The average surface area of the wounds, which was 1.5 cm 2 corresponding to a contraction percentage of 28.58% on the 3rd day of treatment, decreased to 0.09 mm 2 and that is, a contraction of 95.71% on the 9th day. In untreated diabetic rats (Group III), the wound surface decreased from the 3rd day, with an average that went from 1.9 mm 2 to 0.21 mm 2 at the 9th day, giving 80.95% of the wound surface contraction. The healing time was about 13 days for Group I, Group III rats, and Group IV rats.
Histological Study
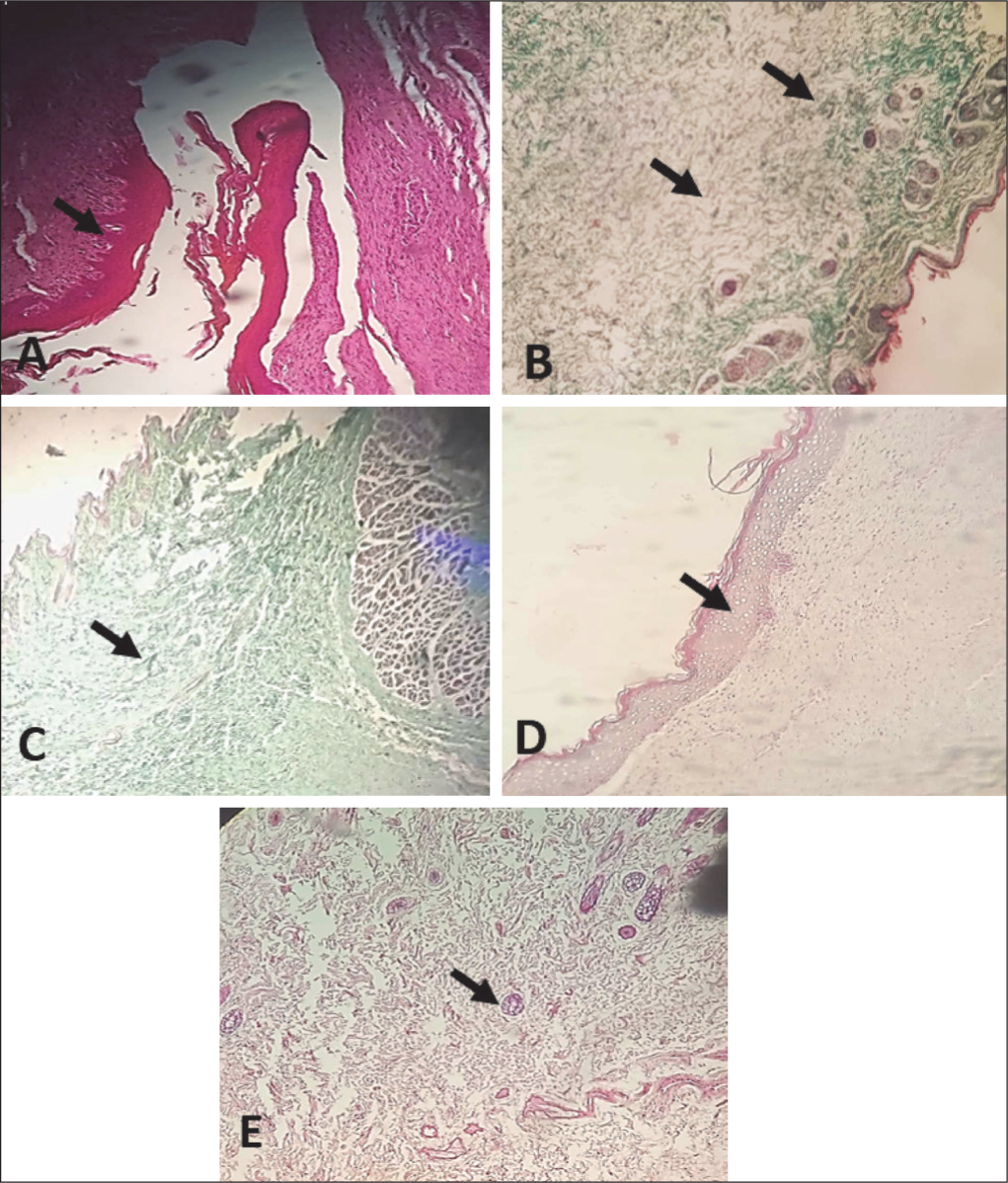
A staining based on modified trichrome, hematoxylin, and eosin was performed on the scar tissue. The study allowed for highlighting the cellular architecture and collagen fibers. The Group I tissue (control) showed a good stratification of the epidermal layers (Figure 8A). The induction of diabetes (Group II) caused skin atrophy (Figure 8B) with a disorganized collagen network architecture. Regarding Group III (diabetes + wound healing), the neo-tissue developed was less dense than that of the control Group. Collagen fibers were randomly dispersed in the tissue (Figure 8C). Concerning Group IV, a complete reconstruction of skin tissue was noted. The treated tissues exhibited collagen deposits more rapidly, forming at a later stage, large fibrous areas, and a more compact structure than those of Group II and III rats. Neovascularization was also more pronounced than in the untreated tissues. The CH+GE+ZO-induced wound healing produced a healthy appearance of tissue, which was evidenced by the normal appearance of the cutaneous layer (epidermis, dermis, and hypodermis), complete epithelialization, tissue granulation of the well-constructed epidermis, and a remarkable neovascularization (Figure 8D and 8E).
Histological Effect of Topical Application of a Chitosan-Gelatin-Zingiber officinale Dressing on Wound Healing and Scar Remodeling in Alloxan-induced Diabetic Rats. A: Control Group: Arrow a Complete Epithelialization. B: Diabetic Group: a Disorganized Architecture of the Collagen Network. C: Diabetic Group + Healing: Epithelialization Not Complete. D and E: Diabetic Treated With the CH+GE+ZO Dressing: Arrow Shows Significant Vascularization. Intense Cellular Activity for Skin Regeneration.
Discussion
Developing biological dressings that increase wound healing is a key therapeutic objective in diabetes management. 29 In this work, the innovative CH+GE+ZO dressing was formulated using ZO rhizome, which was selected for its richness in bioactive compounds, serving as a natural alternative to synthetic dressings. The quantitative analysis revealed significant levels of polyphenols (490.061 ± 15.60 mg GAE/g) and flavonoids (73.96 ± 8.50 mg/g) in the ethanolic extract of ZO. These compounds are the primary causative agents responsible for the dressing’s therapeutic potential, as polyphenols and flavonoids act as potent antioxidants that can neutralize reactive oxygen species (ROS) at the wound site. In the present study, the combination of ZO with CH and GE was used in diabetic rats to evaluate its systemic and local impact. The in vivo study evaluated the level of CRP to reflect the systemic inflammatory response. The results showed an increase in CRP in diabetic rats (Groups II, III, and IV) compared to Group I. The high rate observed in Group IV treated with the CH+GE+ZO dressing did not show a decrease as compared to other diabetic Groups (II, III). This indicates that the dressing’s influence is primarily localized to the wound environment rather than systemic. This can be attributed to the topical application mode, which limits the systemic absorption of bioactive compounds required to alter circulating CRP levels, yet remains effective for local tissue repair. Our work also demonstrates the dressing’s capacity to modulate the oxidative balance, a critical factor in diabetic healing where chronic oxidative stress impairs tissue regeneration. The antioxidant enzyme activities (SOD, CAT) significantly decreased in diabetic rats, reflecting a state of oxidative exhaustion. Furthermore, an alteration of the GSH redox cycle was noticed. GSH, which is the major NPSH quantified in the NPSH assay, is also considered a marker for oxidative damage. 30 The inclusion of the polyphenol-rich ZO extract in the dressing aims to supplement these depleted endogenous antioxidants, thereby restoring the redox balance and creating a more favorable biochemical environment for cellular proliferation and wound closure.
Our results revealed that Alloxan reduced GSH levels in skin tissue. GSH depletion has been shown to cause irreversible damage to cells, as it acts directly or indirectly in many biological processes, including protein synthesis, metabolism, and cell protection. 31 Our study demonstrated that the components of the CH+GE+ZO dressings significantly enhanced the activities of GSH, SOD, and CAT and the levels of non-enzymatic antioxidants such as NPSH and GSH in the skin. Indeed, following the application of the dressing, dermal fibroblasts showed the ability to increase the activity of antioxidant enzymes. This can be attributed to the synergistic effect of bioactive compounds such as polyphenols, gingerols, and shogaols,32,33 which possess powerful antioxidant 34 and anti-inflammatory properties, allowing the reduction of local oxidative stress, the decline of excessive inflammatory response, and the enhancement of cell proliferation. In parallel, ginger contains flavonoids such as quercetin, kaempferol, and luteolin that contribute to wound healing by modulating the signaling pathways involved in tissue repair, stimulating collagen synthesis, and improving vascularization.34,35 Phyto bioactive compounds acted as powerful ROS scavengers and could stimulate fibroblasts’ function by reducing ROS production and increasing collagen synthesis via activation of pathways like Nrf2 and inhibition of MAPK. 37 To follow up on the study on the evaluation of oxidative stress observed after healing, a histological study was conducted to estimate the quality of dermal regeneration. The difference between the wound retraction surfaces and the percentages of wound contractions was very marked in animals between diabetic rats (II, III), as compared to Group I and the diabetic group treated with the CH+GE+ZO dressing (IV).
Throughout the experimental period (D0–D15), a reduction in wound surface area was observed from the initial to the final day of the trial. Thus, after 15 days, complete wound closure was achieved. Indeed, the period that extended between Day 0 and 6 corresponded to the vascular-inflammatory phase of the healing process, which lasts from 2 to 4 days. 38 During this phase, a hemostatic clot was formed, and the inflammatory process was initiated. The reduction in wound surface area seems to be mediated by contraction driven by myofibroblasts. 39 During the period between D5 and D9, a significant acceleration of wound contraction was noticed in the group treated with CH+GE+ZO. Our results revealed that the time needed to cover half of the wound (T50%) corresponds, in our case, to D6. Schilrreff and Alexiev 40 identified this period as the stage of proliferation. During this period, activated fibroblasts and endothelial cells that have already migrated to the wound site actively proliferated. According to Kolanthai et al., 41 the vascular-inflammatory phase of the healing process began from 2 to 6 days after the initiation of healing. This study has proven a variability of this latency period, which corresponds to the time required for activation, migration, and proliferation of fibroblasts. Its duration can range from 10 to 15 days, or even more, 21–42 days. During this phase, the formation of granulation tissue and reepithelialization seems to be triggered. 42 Thus, the contraction of the wound, leading to the approximation of the banks, was closely linked to the formation of the granulation tissue. 43 During the period from D9 to D15, a slowdown in wound contraction was observed. By Day 15, the wounds had achieved full closure, marking the end of the repair phase and the initiation of the maturation phase. This helped to explain the slowdown in the contraction speed recorded during the last few days. The results of the examined histological study showed a more elaborate epithelialization in the rats of Group (IV) treated with the dressing compared to the control Group I and the untreated diabetic group (Group III). Indeed, in diabetes, He et al. 44 revealed that chronic blood glucose elevation leads to the formation of final glycosylation substrates. In the same context, Jadach et al. 45 reported that essential structural modifications consisted of a glycosylation of Type 1 collagen placed at the level of the basement membrane of the vascular wall, thereby leading to the amplification of blood vessel rigidity. This consequently led to the alteration of the passage of leukocytes, oxygen distribution, and metabolic damage.
In this context, the quantity of fibroblasts within the wounds of the treated group with CH+GE+ZO was significantly more abundant, as compared to the other two diabetic groups. The increase in fibroblasts, producers of collagen within wounds, also proved that the plant promoted fibroblast proliferation, which would be the cause of good-quality healing. In addition, previous studies have demonstrated that CH stimulates skin repair and formation. 46 The possible interactions between CH with proteoglycans (PG) and glycosaminoglycans (GAG) and other negatively charged molecules within the skin level were associated with the fact that the material belongs to the category of cationic polymers. Indeed, the study proved that this property allowed the retention and concentration of certain biomolecules, namely, a very large number of cytokines and growth factors, having the power to bind to GAGs. 47 On the other hand, the dressing, also composed of GE, exhibiting various biological activities, 46 demonstrated a role for this polymer during the healing process. Indeed, GE not only absorbs exudates from the wound but also prevents infections by forming a physical barrier against pathogens. 48 It provides a favorable environment for the proliferation and migration of fibroblasts and keratinocytes.
In the present study, GE was used as a reservoir of active molecules produced by ZO, which subsequently allowed a progressive delivery to the site of injury. The synergistic effect of CH and GE, as well as Phyto bioactive compounds derived from ZO, such as polyphenols and flavonoids, applied locally to the skin tissue, contributed to a significant acceleration of the healing process, stimulating cell proliferation, reducing oxidative stress, and promoting tissue regeneration.
Conclusion
The biologic dressing synthesized from bioactive compounds from ZO has proven its marked effectiveness in restoring the skin’s oxidative stress balance and accelerating the healing process. Rich in polyphenols and flavonoids, this treatment contributed to the restoration of oxidative–antioxidant balance. This was demonstrated by the normalization of SOD and CAT activities, levels of GSH and NPSH, as well as the histological improvement of skin tissue. The CH+GE+ZO dressing highlighted the effective therapeutic role of ZO in the creation of innovative and biocompatible biomaterials for wound treatment in diabetic rats.
Footnotes
Acknowledgements
The authors gratefully acknowledge the Tunisian Ministry of Higher Education and Scientific Research for supporting this work through the Young Researcher project (22PEJC-D5PI).
Authors’ Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work. All the authors are eligible to be authors as per the International Committee of Medical Journal Editors (ICMJE) requirements/guidelines.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Data Availability Statement
All data are available from the authors and will be provided upon request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval details are given in the “Materials and Methods” section.
Funding
The authors disclosed receipt financial support from the Tunisian Ministry of Higher Education and Scientific Research (Young Researcher project 22PEJC-D5PI).
Informed Consent
Not applicable.
Publisher’s Note:
All claims expressed in this article are solely those of the authors and do not necessarily represent those of the publisher, the editors, or the reviewers. This journal remains neutral about jurisdictional claims in published institutional affiliation.
Use of Artificial Intelligence-assisted Tools:
The authors declare that they have not used artificial intelligence (AI) tools for the manuscript’s writing or editing, and that no images were manipulated using AI.