
Abstract
Polypharmacy, defined as the concurrent use of five or more drugs, can lead to drug duplication (DD), which is considered a medication error that increases costs to the health systems. The key objectives of this study are to characterize DD in a population receiving care at a Health Services Provider Institution and identify factors associated with DD. This study was a retrospective case-control study. Controls were selected using 1:4 propensity-score matching based on age, sex, geographic location, and socioeconomic status. This study revealed a 1.67% prevalence of DD over 6 months. The most prescribed drugs were: Levothyroxine, Acetaminophen and Losartan. A logistic regression was used to calculate the odds ratio (OR), which showed a relationship between DD and the number of medications (OR: 1.355, 95% CI: 1.324–1.386), number of pathologies (OR: 1.314, 95% CI: 1.272–1.357), number of emergency cases (OR: 3.470, 95% CI: 1.679–7.170), number of hospitalizations (OR: 1.130, 95% CI: 1.019–1.253), inconsistent drug claim (OR: 2.131, 95% CI: 1.937–2.344), and laboratory test off target (OR: 1.399, 95% CI: 1.228–1.593). The study showed DD prevalence in a health services provider from a low-to-middle income country. The main findings indicated that polypharmacy, suffering from several pathologies, hospitalizations, and visits to emergency departments, increases the risk of DD.
Keywords
Introduction
Pharmacovigilance encompasses activities focused on identifying, evaluating, comprehending, and mitigating adverse effects or potential drug-related issues, 1 drug interactions occurring when two or more substances, including other drugs, nutraceuticals, or foods, are co-administered.2,3 These interactions can modify a drug’s therapeutic or toxic effects by influencing its pharmacokinetic or pharmacodynamic properties through various mechanisms, such as synergism, antagonism, and alterations in metabolic pathways.4,5
Polypharmacy is defined as the concurrent use of five or more drugs. This definition was selected as it represents the most commonly used threshold in the literature, with 138 different definitions identified by Masnoon et al., where greater than or equal to five medications was the most frequent criterion, 6 therefore, it becomes a risk factor by increasing the possibilities of drug interactions. Predominantly observed among elderly patients contending with multimorbidity, polypharmacy is increasingly prevalent 7 ; nevertheless, there is a growing trend of younger patients consuming multiple medications. 8
Overall, statistics showed that, during 2010, polypharmacy affected approximately 10% of American patients. 9
Another problem in pharmacotherapy is drug duplication (DD), which refers to the prescription or administration of two or more medications of the same pharmacological group, or with similar pharmacological effects, therapeutic uses, or active molecules within a clinically relevant timeframe. It is important to distinguish that legitimate therapeutic duplications may occur in specific clinical scenarios (e.g., combination levothyroxine doses to achieve non-standard dosing, or combination products containing acetaminophen where the total daily dose is appropriately managed). However, unintended duplications represent medication errors that increase patient safety risks. The main causes of this issue are fragmentation of health care attention, lack of communication among health care providers, inadequate medication reconciliation, and polypharmacy, among others.10–13 DD increases the risk and presence of adverse drug reactions, drug interactions, and unnecessary healthcare costs.11,14 Therefore, identifying and addressing instances of DD is important in optimizing patient safety and healthcare quality.
A report from the Institute of Medicine of the United States, published in the early 2000s, suggests that within healthcare, errors in medical practice should be considered an inherent aspect of the human condition and a risk to patient safety; 15 DD is considered one of them. In addition, this report brought attention to a global issue, revealing that approximately 4% of hospitalized patients were at risk of suffering harm due to factors associated with healthcare, with 70% leading to temporary disability and 14% resulting in fatal events, causing an estimated 44,000 to 98,000 deaths. 15 Moreover, the Institute of Medicine publication prompted further research and publications on patient safety and mortality associated with Errors in Healthcare (EH). Approximately 37% of adverse events in hospitalized patients have been reported to be associated with medications, 16 and medication errors can occur at various stages of medication use, from prescription and administration to therapy monitoring.17,18 Therefore, this study aimed to characterize DD in a population receiving care at a Health Services Provider Institution (IPS), and identify the associated factors with the presence of DD.
Method
Study Design
This investigation was structured as a retrospective case-control study, examining medication orders processed by an outpatient pharmacy network of an IPS based in Medellín, Colombia, over a 6-month period (May–October 2023). The timeframe was selected to capture seasonal variations in prescribing patterns while providing sufficient sample size for robust statistical analysis. This duration was considered appropriate for detecting DD patterns without extending to periods where clinical contexts might significantly change. The primary focus was on identifying instances of DD among outpatient adult patients, who constituted the case group.
Cases were defined as adults who experienced DD incidents within the medication orders dispensed during the study’s timeframe. Identifying control subjects involved selecting individuals from the same healthcare setting who did not exhibit any instances of DD during the same period, and who were selected using 1:4 propensity-score matching based on age, sex, geographic location, and socioeconomic status. Primary diagnosis was defined as the main condition driving the patient’s current treatment plan, as documented in the electronic health record by the prescribing physician.
To identify duplications, a validated automated clinical decision support system (CDSS) was employed. The system was developed and validated by a multidisciplinary team of clinical pharmacists and medical toxicologists. It compared the active pharmaceutical ingredients, pharmacological classifications, and mechanisms of action of all medications dispensed to each patient within 30-day periods. Duplications were defined as the concurrent dispensing of two or more medications from the same therapeutic class with overlapping mechanisms of action, excluding clinically justified combinations. The system flagged potential duplications when medications with similar pharmacological effects were dispensed within overlapping time periods, accounting for medication half-lives and dosing intervals. When matches are found, the process marks the record as a duplication. A propensity-score matching technique was employed using logistic regression to estimate the probability of experiencing DD based on demographic and clinical covariates. Propensity-score matching was performed using age, sex, geographic location, and socioeconomic status. Each case was matched to four controls using nearest-neighbor matching with a caliper of 0.2 standard deviations of the logit of the propensity score to ensure adequate matches while maintaining sample size. By employing this matching approach, the study aimed to reduce potential confounding influences, thereby enhancing the reliability and validity of the comparisons drawn between the case and control.
Data Collection
The data were collected from the comprehensive electronic pharmacy database of the IPS, which captures all outpatient prescriptions dispensed through the institution’s pharmacy network. The database includes detailed information on drug name, drug concentration, quantity dispensed, prescribing physician, and dispensing date.
Sample Size and Selection
From the population of patients who experienced DD during the study period (n = 15,847), a representative sample of 7,015 cases was selected using systematic random sampling. This approach was adopted to ensure computational feasibility, as the 1:4 propensity-score matching design required processing 28,060 control subjects alongside the cases. Under the assumptions of a minimum detectable odds ratio (OR) of 1.2, 80% power, a two-sided significance level of 0.05, and an expected exposure prevalence of approximately 4% among controls, this sample size was considered sufficient for the planned analyses. To assess potential selection bias, the main demographic and clinical characteristics of the sampled cases were compared with those of the remaining eligible cases; no statistically significant differences were observed, supporting the representativeness of the analytic sample.
Inclusion Criteria
All outpatient medication orders dispensed during the study period were included. There were no restrictions on the type of medication, dosage, or associated diagnosis.
Identification of Drugs and DD
To identify the most prescribed medications, medication orders were classified and counted according to their international nonproprietary name. For the detection of duplications, we employed a validated automated CDSS that analyzed prescriptions based on active pharmaceutical ingredients, pharmacological class, and mechanism of action. The system was programmed with clinical rules developed by our multidisciplinary team, considering factors such as: (a) medications within the same therapeutic class, (b) overlapping mechanisms of action, (c) concurrent administration timeframes, and (d) clinically inappropriate dose escalations. A duplication was flagged when a patient received prescriptions for medications with overlapping therapeutic effects within a 30-day window, excluding clinically justified combinations as determined by established therapeutic protocols.
Variable Definitions
Number of pathologies: Total count of distinct active diagnoses documented in the patient’s electronic health record during the study period, coded according to the International Classification of Diseases, 10th edition (ICD-10).
Laboratory off target: Patients classified as having any laboratory parameter outside the established reference ranges during the study period, assessed at the patient level rather than the individual test level.
Inconsistent drug claim: Irregular patterns in medication retrieval by patients, including failure to claim prescribed medications within expected timeframes, incomplete medication pickups, or erratic patterns of medication collection that deviate from prescribed regimens. This was assessed as a patient-level binary variable indicating whether the patient demonstrated inconsistent medication claiming behavior during the study period.
Data Analysis
A quantitative analysis was performed using Python 3.11. The results were presented as frequencies and percentages, focusing on the descriptive analysis of monthly frequencies of dispensed medications and identifying patterns in prescription DD. To delve deeper, we also applied logistic regression models to evaluate the association between factors and the likelihood of DD.
Ethical Approval Statement
This study was reviewed and approved by the Ethics Committee of the Faculty of Nursing at the University of Antioquia, under approval number 246, Act 61 of 2023. The committee operates primarily in accordance with Resolution 8430 of 1993 issued by the Colombian Ministry of Health, as well as Resolution 2378 of 2008 issued by the former Ministry of Social Protection, including Requirement 2.2, which establishes the proper preservation of all documentation related to the projects submitted for its review. The research was conducted in compliance with national and international ethical standards. Informed consent was waived by the Ethics Committee due to the retrospective nature of the study, which did not involve direct patient contact or the use of identifiable personal information.
Results
Drug Duplications
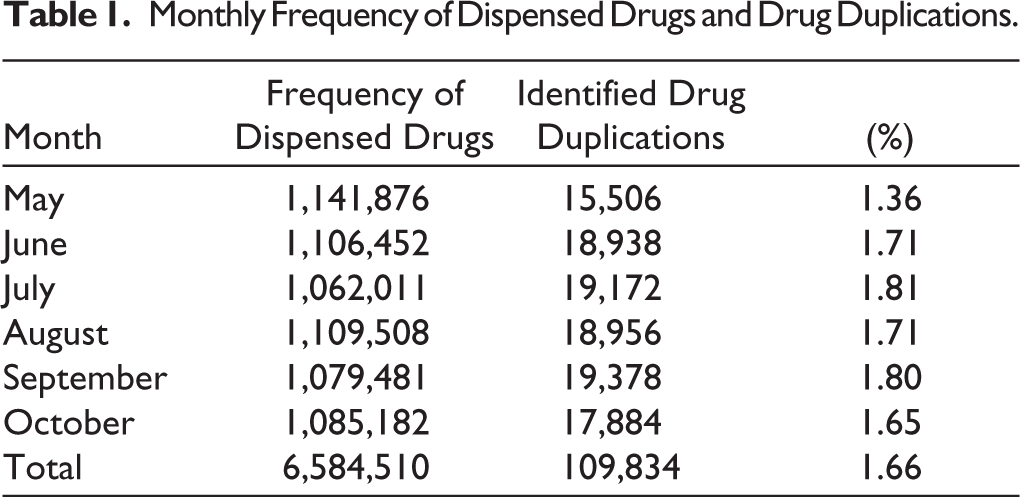
A critical aspect of this study was the detection of duplications in outpatient prescriptions. July showed the highest monthly prevalence of duplications (1.81%; 19,172/1,062,011), followed by September (1.80%; 19,378/1,079,481) and June and August (both 1.71%). In absolute terms, however, September recorded the highest number of duplications (19,378), followed by July (19,172) and August (18,956); these differences in ranking reflect variations in the monthly volume of dispensed medications. These findings suggest a possible lack of coordination in prescription management or a deficit in pharmaceutical review systems. Table 1 provides a monthly analysis of the identified duplications, which is fundamental to informing strategies for improving prescription and medication dispensing. In addition, Table 1 also shows the frequency of identified DDs by month.
Monthly Frequency of Dispensed Drugs and Drug Duplications.
Main Prescribed Medications
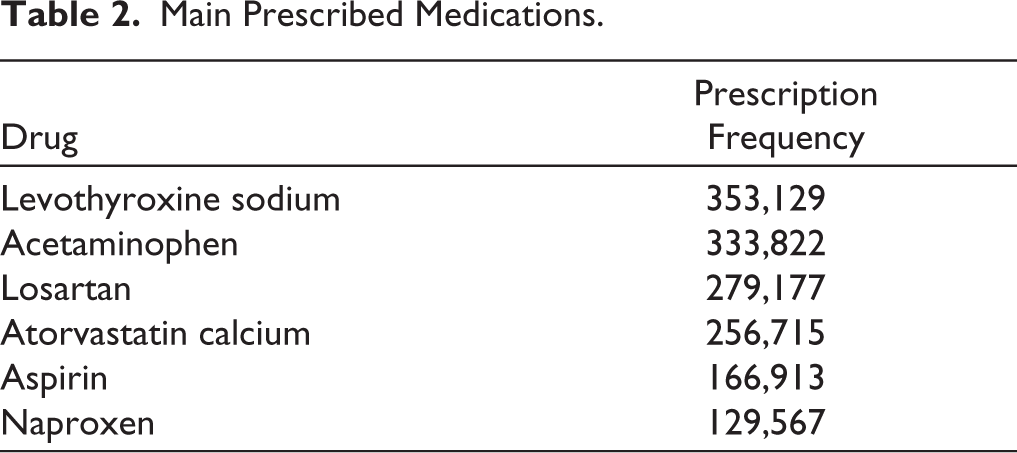
The study identified a list of the most frequently prescr-ibed medications during the analysis period. Notably, Levothyroxine Sodium was prescribed on 353,129 occasions, reflecting its high demand in treating thyroid conditions. This was followed by Acetaminophen and Losartan, with 333,822 and 279,177 prescriptions, respectively, indicating widespread use for pain management and hypertension. This information is crucial to understanding prescription trends and the needs of the served population. The details of the six most prescribed medications are presented in Table 2, including their frequency.
Main Prescribed Medications.
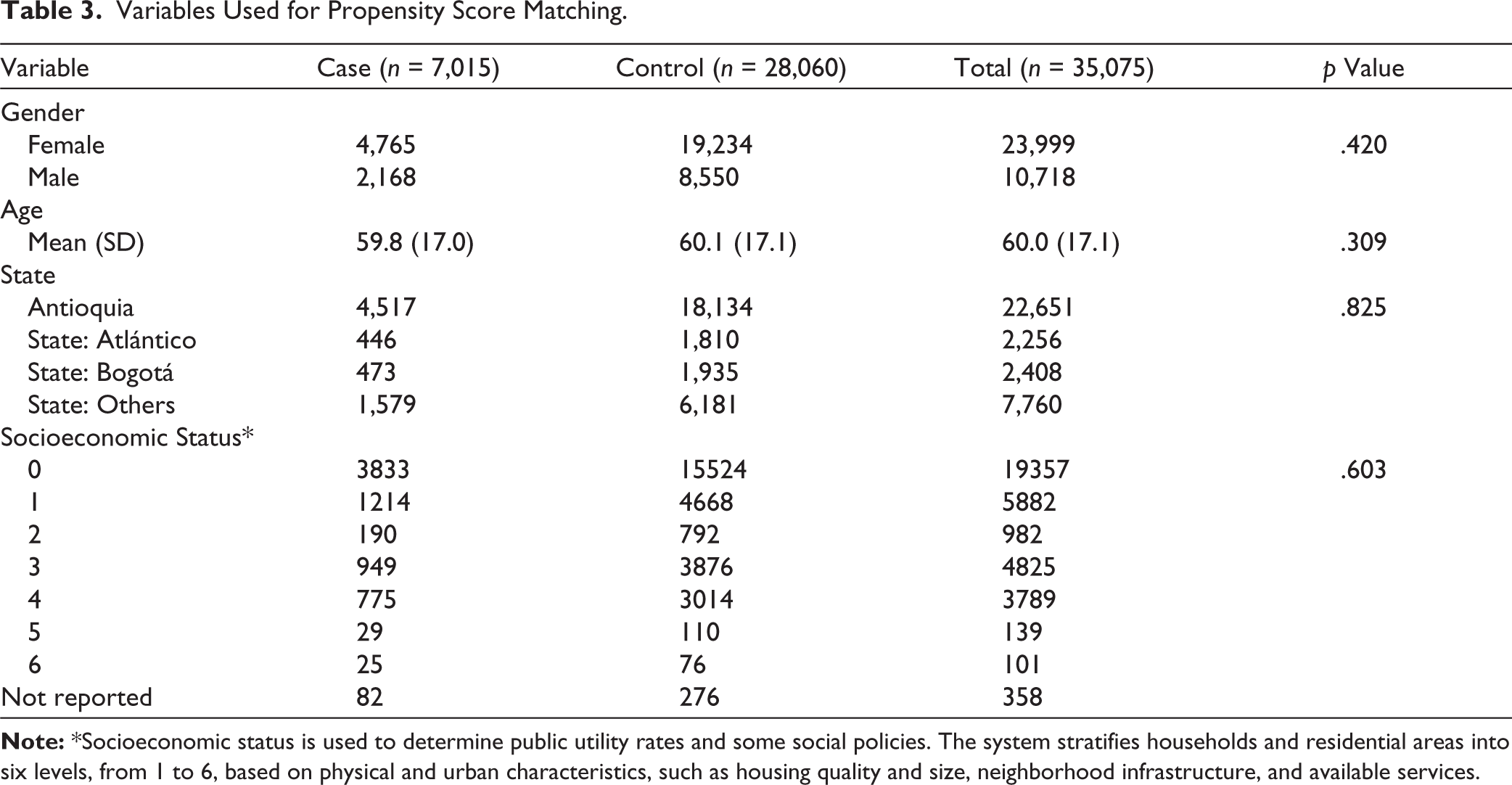
We selected a sample of 7,015 cases to analyze associated factors, employing a 1:4 ratio with the controls. Complete data were available for all matching variables with the exception of gender which was unrecorded for 358 patients, corresponding to 82 cases and 276 controls. The proportion of unrecorded gender was low and similar between groups. These records were retained in the descriptive analysis under a “Not reported” category.
Table 3 shows the variables used for propensity-score matching. The table confirms no significant differences between the groups in these variables. To ensure comparability of the groups, chi-square tests were conducted for qualitative variables, and Student’s t-tests and Mann–Whitney U tests were conducted for quantitative variables.
Variables Used for Propensity Score Matching.
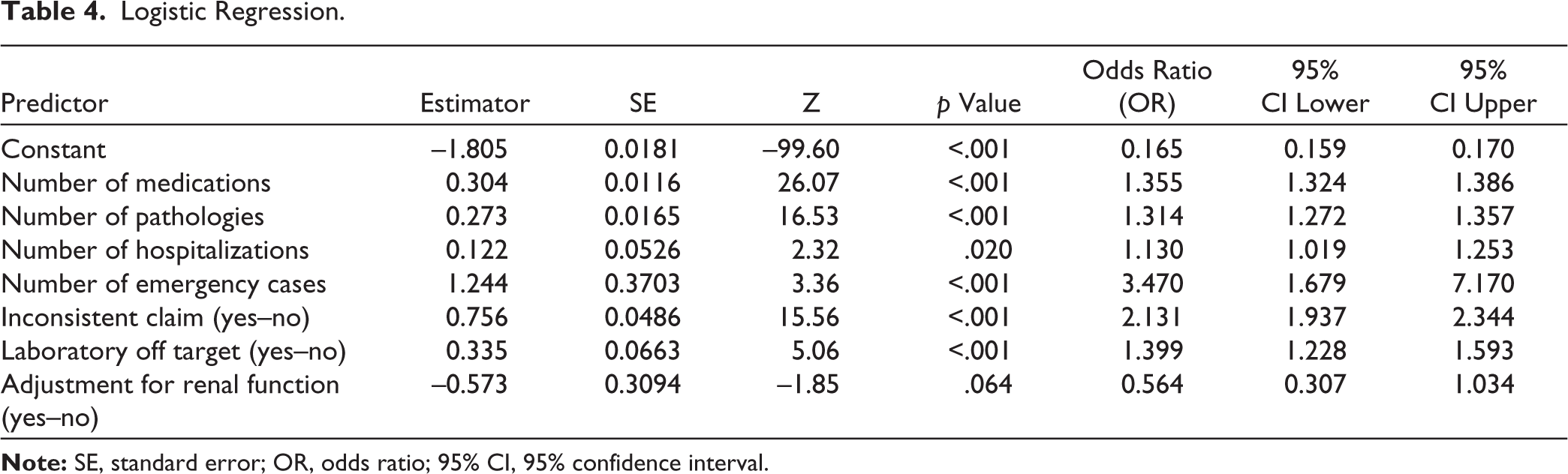
It can be observed that as the number of medications, the number of pathologies, the number of hospitalizations, and the frequency of emergency room visits increase, there is a corresponding rise in the likelihood of DD occurrences. This relationship is shown in Table 4. Additionally, inconsistent medication claims and laboratory results that deviate from established targets have been identified as significant risk factors contributing to the probability of DD. Finally, there was no statistical association for the adjustment of medications for the renal function variable.
Logistic Regression.
Discussion
DD refers to the prescription or administration of two or more medications of the same pharmacological group with similar pharmacological effects, therapeutic uses, or active molecules. In addition, in some cases, there is no clear distinction in this practice of when one agent should be administered over another. This study detected a prevalence of 1.67% of DDs in a 6-month period. DD prevalence may vary depending on several factors, such as the type of patients (hospitalized, outpatient), healthcare service (internal medicine, pediatric, internal care unit, etc.), and type of drugs, etc. Therefore, other studies have quantified the prevalence of DD in different services and conditions in the healthcare system. For instance, Pasina et al., 19 performed a cross-sectional study on internal and geriatric wards, with patients admitted and discharged from these services. DD of admitted and discharged patients was 2.52% and 3.41%, respectively, higher than in this report. Nevertheless, there are differences between this research and that of Pasina et al. 19 ; this includes outpatient people, and they are considered hospitalized patients. Indeed, their investigation considered hospitalization as an important risk factor for increasing DD. Similar findings to the present study were reported by Trenaman et al., 11 who informed 1.7% of duplications in nonsteroidal anti-inflammatory drugs (NSAIDs) and 1.0% of selective serotonin reuptake inhibitors (SSRIs) for 30 days. In contrast, Huynh and Rajendran 19 implemented a Quality Improvement Project (QIP) to reduce DD in the general surgical wards. The baseline of DD was 9% of all prescriptions in a week, a similar value to this study. Nevertheless, after personnel education, DDs were reduced to 5.29% and 3.12% in the second and third measurement rounds, respectively. 20
Health deterioration is the main cause of elderly patients suffering from several pathologies (multimorbidity) and, therefore, also presents polypharmacy.21,22 The present study cases were 59.8 ± 17.0 years old; for example, the proportion of participants aged 65 years or older was not formally quantified, so this cohort should be regarded as middle-aged to older adults rather than as a strictly elderly population. The results showed that the number of medications (polypharmacy) and the number of pathologies increase the risk of undergoing DD by 35.5% and 13.0%, respectively. These findings agree with those of Trenaman et al., 11 who also reported DDs in a cohort of older adults with dementia. In the same way, Pasina et al. 19 also informed DDs in hospitalized elderly patients. All of these results suggest that polypharmacy and multimorbidity may be considered as a potential risk factor for DD.
Medication errors are common in emergency departments; previous observational studies have reported prevalences ranging from approximately 30.5% to 59.4%.23–25 The present study showed that visiting the emergency department increases the risk of presenting DD by 247%, the most significant associated risk factor described in this study. The consequences of these errors may be mortal, or they can trigger health problems and additional costs to the healthcare system. For instance, Shao et al. 26 reported hypocalcemia in a patient who received a double dose of bisphosphonates, the first in an ambulatory department and the second on the next day in the emergency department. Some studies have attributed medication errors in emergency departments to multitasking, fatigue, interruptions, lack of medical records, stress, and sleep quality, among others.27,28 Therefore, there is a need to continue investigating the causes and improve the conditions of the healthcare professionals in emergency departments.
Additionally, the number of hospitalizations was significantly associated with DD (OR: 1.130, p = .020). Although the effect size was modest compared with emergency cases, this finding suggests that patients with repeated hospital admissions may be exposed to medication changes across care transitions, increasing the opportunity for unintended DD. This result is consistent with the findings of Pasina et al., 19 who identified hospitalization as a risk factor for DD among elderly patients.
The high number of levothyroxine prescriptions identified in this study may also be explained by the local burden of thyroid dysfunction. In Medellín, a cross-sectional study conducted in a healthcare institution reported that 19% of evaluated individuals had elevated TSH levels, while 5.1% were classified as having subclinical hypothyroidism, suggesting a considerable demand for thyroid hormone replacement therapy in this setting. Therefore, the local epidemiological profile may partially explain the frequent prescription of levothyroxine observed in our analysis. 29
A logistic regression was performed as described above to improve the relationship between DD and the variables available in the data set. Nevertheless, the model was not predictive because it showed an R2 of 7%, indicating that it was purely explicative. The analysis performed in this study included exploring a data set after the drug was prescribed, with further notification of healthcare providers. With this approach, future DDs can be avoided. However, the most suitable strategy must be to implement a systematic search in prescriptions before patients receive the medications, using other methods, such as CDSS, as recently developed by Dahmke et al., to avoid anticoagulant DD. 30
Strengths and Limitations
One of the strengths of this study is its focus on a specific healthcare context, which provides detailed insights into the prevalence and associated factors of DD within that setting. The use of logistic regression allowed for an explanatory analysis of the relationships between DD and various risk factors.
However, the study has several limitations. As a retrospective case-control study, it cannot establish causality, only correlations. There is a potential for selection bias since the data were sourced from a single Health Services Provider Institution, limiting the generalizability of the findings to other healthcare settings or geographical areas with differing prescription practices and management systems. Although propensity-score matching was employed to minimize confounding, unmeasured or poorly recorded variables such as medication adherence, personal beliefs about medications, and access to healthcare may have influenced the results. These limitations suggest that the findings should be interpreted with caution.
A further limitation is that clinical outcomes were not evaluated in this study. Therefore, although the study identified factors associated with DD, it was not possible to determine its direct impact on patient health, adverse events, or healthcare utilization.
Despite these limitations, the study provides valuable insights into the prevalence and factors associated with DDs within a specific healthcare context. By highlighting critical areas such as polypharmacy and emergency department visits, the research offers actionable data to guide healthcare providers and policymakers in designing and implementing strategies to enhance medication safety and reduce unnecessary healthcare expenditures. The findings serve as a foundation for further research, encouraging more comprehensive studies that can build on this work to develop targeted interventions to improve patient safety across different healthcare settings.
Interpretation Within the Context of the Wider Literature
The 1.67% prevalence of DD found in this study aligns with similar research, such as Trenaman et al., 11 who reported 1.7% duplication for NSAIDs and 1.0% for SSRIs over 30 days. However, higher rates were observed by Pasina et al. 19 in internal and geriatric wards (2.52% and 3.41%, respectively), likely due to their focus on hospitalized patients, a known risk factor for duplication. Additionally, Huynh and Rajendran 20 demonstrated that targeted interventions like personnel education could significantly reduce duplication rates from 9% to below 5%. These comparisons highlight the influence of patient population and intervention strategies on duplication rates, emphasizing the need for tailored approaches to manage polypharmacy and multimorbidity effectively.
Implications for Policy, Practice, and Research
The study’s findings suggest that healthcare policies should include regular medication reviews, especially for patients with polypharmacy and multiple chronic conditions. Integrating CDSS can further prevent duplications by providing real-time alerts to prescribers. In clinical practice, enhancing coordination during patient transitions, particularly in emergency departments, is crucial to minimize errors. Educational programs aimed at healthcare professionals can improve prescribing accuracy and awareness of duplication risks. For future research, exploring the underlying causes of DD across diverse settings and evaluating the effectiveness of various intervention strategies will be essential. Additionally, studies should consider factors like medication adherence and patient beliefs to develop comprehensive solutions for reducing duplication.
Conclusions
This study highlights the prevalence of DD and its associated factors within a specific healthcare context, revealing a 1.67% prevalence over 6 months. The findings indicate that polypharmacy, multiple pathologies, hospitalizations, and emergency department visits increase the risk of DD. Strategies to address this issue include improved prescription coordination, the use of CDSS, and ongoing education for healthcare personnel. Despite the study’s limitations, such as its retrospective design and reliance on records from a single institution, the results provide a basis for enhancing patient safety and guiding future research in various healthcare settings.
Footnotes
Acknowledgements
The authors would like to acknowledge Cielum Health and the Research Group on Pharmaceutical Promotion and Prevention for their support in the development of this study.
Authors’ Contribution
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work. All the authors are eligible to be authors as per the International Committee of Medical Journal Editors (ICMJE) requirements/guidelines.
Consent to Participate
Not applicable. This was a retrospective study based on anonymized records and did not involve direct patient contact.
Consent for Publication
Not applicable. The manuscript does not include identifiable individual patient data, images, or personal information.
Data Availability Statement
All the data are available with the authors and shall be provided upon request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Although one of the authors, Newar Giraldo, is affiliated with Cielum Health, Medellín, Antioquia, Colombia, this affiliation had no direct or indirect influence on the study design, experimental work, results or manuscript preparation.
Ethical Approval
This study was conducted in accordance with national and international ethical standards, including Colombian Resolution 008430 of October 4, 1993, which establishes the scientific, technical, and administrative regulations for health research, as well as the principles of the Declaration of Helsinki and the Council for International Organizations of Medical Sciences. The research protocol was independently reviewed and approved by the Ethics Committee for Research of the Faculty of Nursing at the University of Antioquia (CEI-FE), as recorded in approval no. 246, Act No. 61 CEI-FE 2023, dated September 22, 2023. The committee assessed the study with regard to its scientific validity, social value, equitable participant selection, risk–benefit balance, and safeguards to protect participants’ rights and welfare.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Universidad de Antioquia (CIFAL-363).
Informed Consent
Not applicable. Informed consent was waived by the Ethics Committee due to the retrospective nature of the study and because no identifiable personal information was used.
Use of Artificial Intelligence-assisted Tools:
The authors declare that they have not used artificial intelligence (AI) tools for writing and editing of the manuscript, and no images were manipulated using AI.