
Abstract
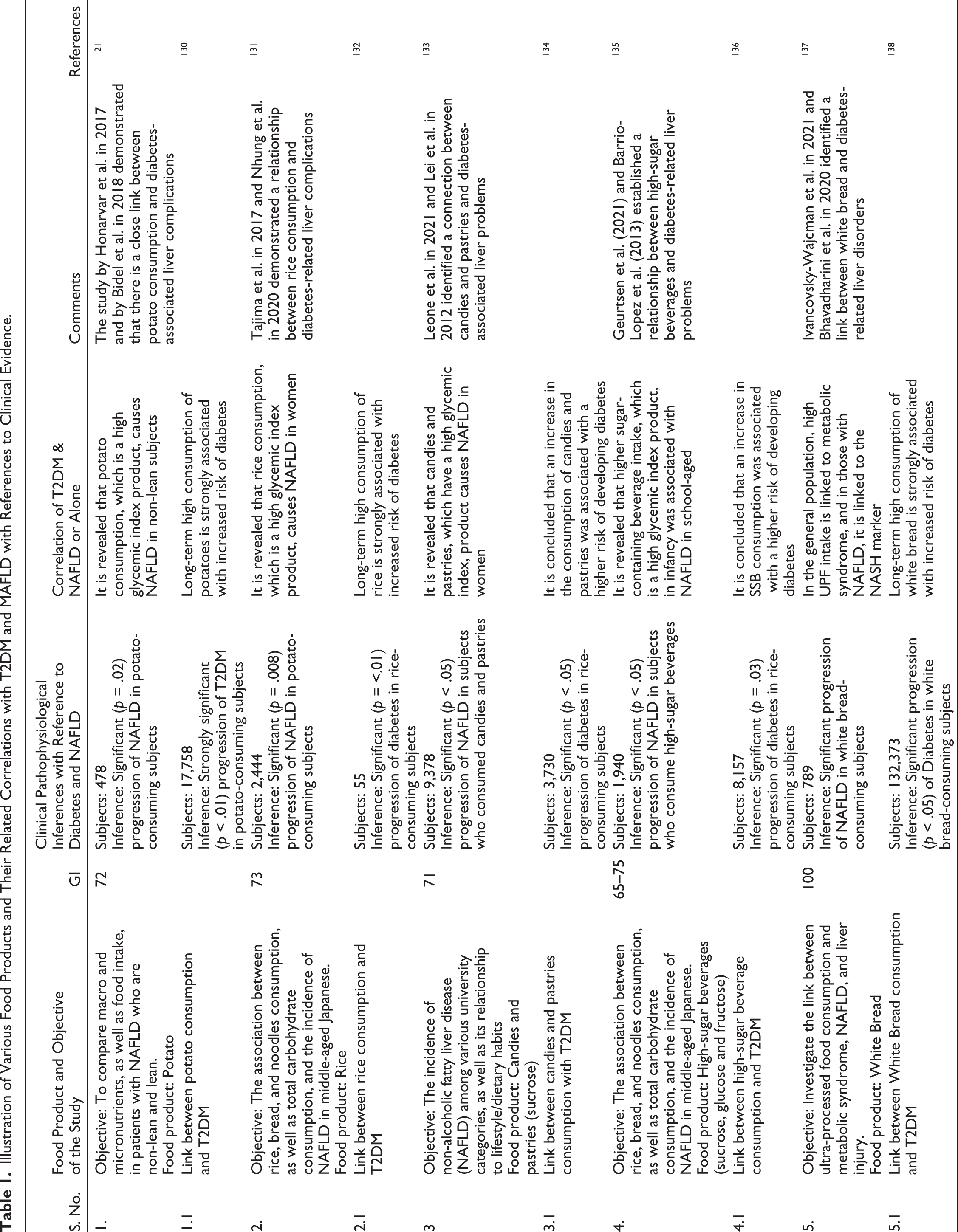
The progression of various devastating metabolic syndromes like diabetes, metabolic dysfunction-associated fatty liver disease (MAFLD), obesity, etc., is due to the inappropriate lifestyle with respect to the consumption of high-fat and high glycemic index (GI) products. The epidemiological data revealed that the prevalence of metabolic disorders is increasing gradually and will create a global burden. According to reports, the global prevalence of MAFLD in people with Type 2 diabetes mellitus (T2DM) is between 50% and 75%, with 12.5%–87.5% in India. The culprit dietary components, which have a high GI (potatoes, rice, high-sugar beverages, candies and pastries, white bread, etc.), and high-fat diet products (trans fatty acids, sucrose, fructose, high cholesterol, etc.), act significantly in the pathogenesis underlying liver-related complications and further trigger the other secondary metabolic complications. These inappropriate dietary interventions lead to alteration of different pathways like fibroblast growth factor 10 (FGF10), AMP-activated protein kinase (AMPK), c-Jun N-terminal kinase (JNK) pathways, etc., which directly trigger the other secondary pathways leading to diabetes-associated MAFLD and liver-related complications. There are numerous dietary interventions (Vitamin D-rich diet, soy isoflavones, ketogenic diet, unsaturated fatty acid diet, low-carbohydrate diet, green leafy vegetables, etc.), which may improve the various molecular pathways and help in normalizing the pathological state of liver-compromised subjects. In the present review, the new dietary interventions are discussed, which help in managing the diabetes-associated metabolic disorders.
Keywords
Introduction
The burden of obesity and other devastating metabolic disorders has increased since 1975, making it a global epidemic. According to the World Health Organization (WHO), adult obesity is connected to more fatalities worldwide than underweight. In 2016, overweight adults were 1.9 billion (39%), while obese adults were 650 million (13%). 1 Obesity raises the risk of chronic disease morbidity and death, including disability, Type 2 diabetes mellitus (T2DM), liver disorders, cardiovascular disease, and other related malignancies.2–4 Obesity has been strongly linked with insulin resistance (IR) and metabolic dysfunction-associated fatty liver disease (MAFLD), which has become a prominent risk factor in the progression of diabetes and related MAFLD.5–7 As per the epidemiological data of 2016, approximately 13% of the world’s adult population, out of which 11% of men and 15% of women, were considered to be obese. 1 As per the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), MAFLD is prevalent in up to 75% of overweight adults and more than 90% of people with serious obesity. According to reports, the predominance on a global scale of MAFLD in patients with T2DM lies between 50% and 75%, and in India, it was found to be 12.5%–87.5%.8,9 The above epidemiological evidence demonstrated that there is a close relationship between obesity and other metabolic complications like MAFLD, T2DM, etc. Diabetes-related metabolic abnormalities frequently lead to altered liver metabolism, culminating in hepatic injury and induction of cell death.10–12 The major etiological reason for the metabolic complication is directly associated with the use of bad dietary approaches that include the consumption of dietary components such as saturated fatty acids (SFA), steroids, simple sugars, and trans fats, which produce a dangerous effect on vital organs, leading to acting as a major culprit in causing obesity and associated metabolic disorders.13–15 The present scenario inculcating the various secondary dietary sources like high-fat, high-fructose (HFHF), and high glycemic index (GI) food products like potatoes, rice, pastries, candies, high-sugar beverages, white bread, etc., leads to slow progression of metabolic complications (Table 1).16,17 It is revealed that all the abnormal dietary products trigger the production of oxidative stress. hepatic inflammation, IR, etc. via different molecular pathways like fibroblast growth factor 10 (FGF10), AMP-activated protein kinase (AMPK), etc., which are associated with the progression of metabolic-related complications.18,19 The primary consideration for the management of the above-mentioned problems should be managed by dietary interventions like the ketogenic diet, soy isoflavones, low-carbohydrate diets, calorie restriction, etc.20,21 In lieu of the same, the present review emphasizes the clinical and preclinical studies for highlighting the beneficial effects of different dietary interventions in ameliorating the diabetes-associated MAFLD.
Illustration of Various Food Products and Their Related Correlations with T2DM and MAFLD with References to Clinical Evidence.
Inappropriate Dietary Habits in the Progression of Diabetes-associated MAFLD
Increased dietary volume, high-energy-dense meals, imbalance in meal times and bad eating habits, and excessive consumption of carbohydrate-rich food products are directly linked to the progression of various metabolic disorders, and these key culprits need to be explored for the build-out of interventions for the management of metabolic disorders. These factors serve as significant indicators or checkpoints to manage diabetes-related liver disorders such as MAFLD, metabolic dysfunction-associated steatotic liver disease (MASLD), etc.22,23
HFD and Other Fat-rich Food Products
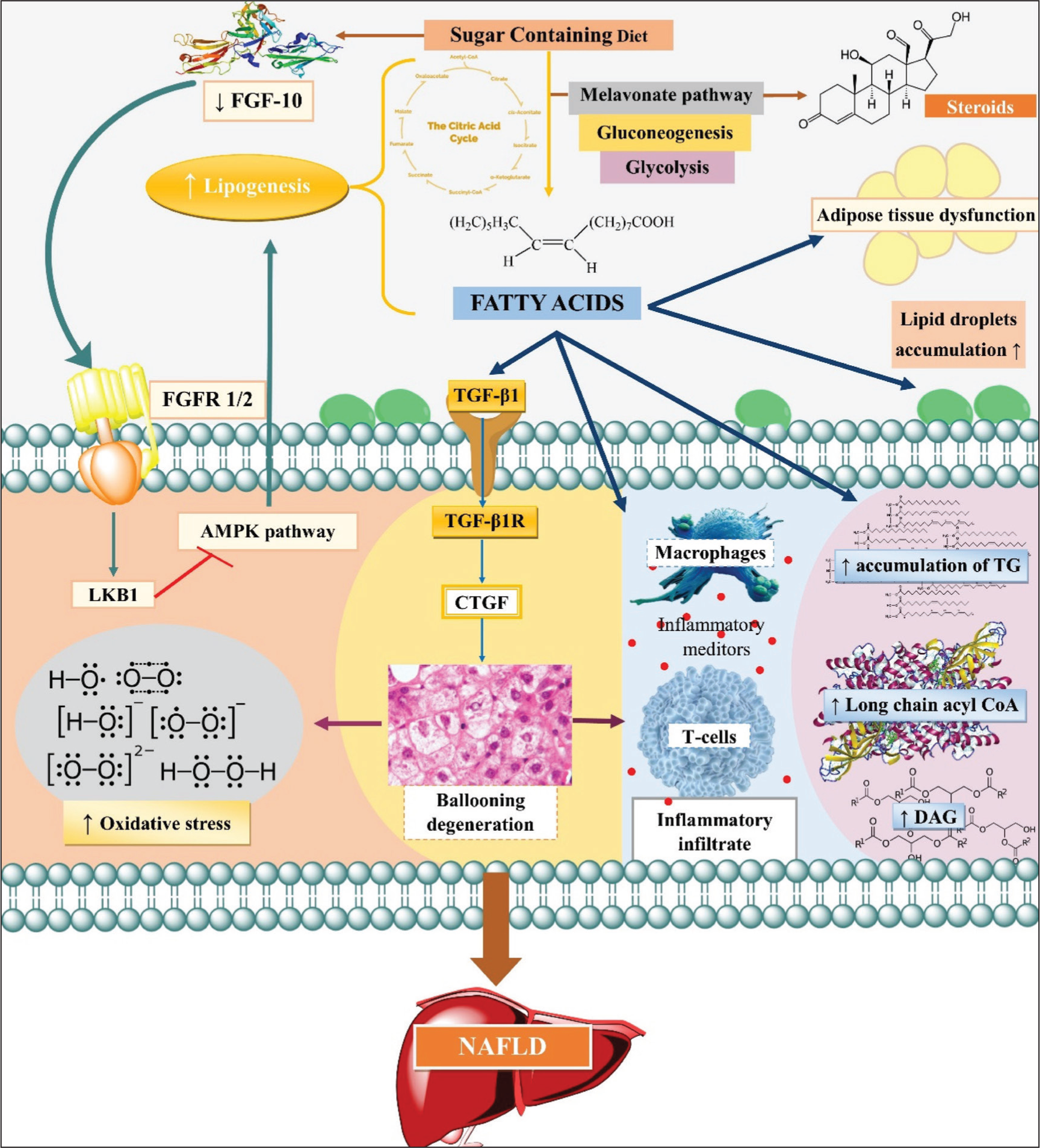
A high-fat diet (HFD), which includes both unsaturated and saturated fat, accounts for at least 35% of total calories. Many other foods, in addition to popular processed foods, have a high-fat content, such as animal fat, cocoa butter, and fatty fish, of which some are hazardous, and others are macrophage-full for maintaining body homeostasis within a specified range. The scientific evidence revealed that sugar-containing diets are converted to fatty acids in a steady state with the help of different enzymes corresponding to the Krebs cycle, malonate pathway, glycolysis, and gluconeogenesis. 24 The above-mentioned high-carbohydrate diet can also convert to steroids in the body via the acetate-mevalonate pathway. 25 In a nutshell, all types of diets work as a connecting link, allowing all these pathways to work in synchronization to overcome the condition of IR and associated MAFLD. Due to the overstimulation of metabolic pathways, an HFHF diet increases the accumulation of free fatty acids (FFA), which results in the accumulation of triglycerides (TG), long-chain acyl-coenzyme A, and diacylglycerol (DAG) in hepatocytes, causing a diabetic-like condition26,27 and the progression of MAFLD. 28 The mechanism by which HFD and high-fructose diet lead to diabetes-associated MAFLD via increased de novo lipogenesis, adipose tissue dysfunction, and lipid droplet accumulation is illustrated in Figure 1.7,29 Prolonged consumption of either a high-carbohydrate diet or an HFD causes the same liver injury, increase in the inflammatory infiltrate, and fibrosis marker. Transforming growth factor 1 (TGF-1) and its downstream effectors, connective tissue growth factor (CTGF), lead to ballooning degeneration and severe fibrosis, all of which cause a significant progression of MAFLD/MASLD. 16 Rats on an HFD (containing 15% fat) cause diabetes-associated MAFLD by deregulating FGF10 and AMPK signaling pathway, which causes increased blood glucose levels and leads to abnormal de novo synthesis and causes enhanced lipid accumulation with increased TG levels in the liver. 19 In lieu of the above evidence, our lab has recently also evidently proved that in rodents, the HFD is a major factor in the development of diabetes-related liver problems. 30 Trans fatty acid (TFA)-rich diet (margarine diet) induces lipid peroxidation, increases blood glucose level, and oxidative stress, ultimately demonstrating the direct effect of TFA in the progression of diabetes and associated MAFLD. 31 The addition of 0.75% cholesterol to an HFD raises blood glucose and TG levels as well as hepatocyte ballooning, tumor necrosis factor α (TNF-α) levels, and the MAFLD activity score (NAS), all of which contribute to the advancement of diabetes-related MAFLD in WT C57BL/6J mice. 32 A high-cholesterol-containing diet enhanced the expression of chemotactic and pro-inflammatory cytokines, which together cause a pro-inflammatory response and rendered hepatocytes more susceptible to proapoptotic stimuli in wild-type B6 mice, ultimately causing IR and associated metabolic syndromes like MAFLD, MASLD, etc. 33 Based on the scientific evidence presented above, high-fat food products are thought to be the primary cause of a variety of catastrophic metabolic problems.
Illustration of Sugar-containing Diets Leads to Diabetes-associated MAFLD via Converting to Fatty Acids and Steroids with the Help of Different Enzymes Corresponding to the Krebs Cycle, Malonate Pathway, Glycolysis, and Gluconeogenesis. This Leads to Deregulating FGF10 and AMPK Signaling Pathway, Which Causes Increased Blood Glucose Levels and Leads to Abnormal De Novo Synthesis and Causes Enhanced Lipid Accumulation with Increased TG Levels in Liver; Increase in the Inflammatory Infiltrate and Fibrosis Marker Transforming Growth Factor 1 (TGF-1) and Its Downstream Effector Connective Tissue Growth Factor (CTGF), Leading to Ballooning Degeneration and Severe Fibrosis; Increase in Inflammatory Mediators, that is, Macrophages, T-Cells, etc., Causing Inflammatory Infiltrate; Increase Accumulation of TG Leading to Increase Long Chain of Acyl-CoA Ultimately Leading to Increase in DAG in Hepatocyte; Other Mechanisms Like Increase Lipid Accumulation and Adipose Tissue Dysfunction. Acyl-CoA, Acetyl Coenzyme A; AMPK, AMP-Activated Protein Kinase; DAG, Diacylglycerol; FGF-10, Fibroblast Growth Factor; FGFR½, Fibroblast Growth Factor Receptor; LKB1, Liver Kinase B1; MAFLD, Metabolic Dysfunction-associated Fatty Liver Disease; TG, Triglycerides; TGF-β, Transforming Growth Factor-beta.
High GI Food Products
High GI foods are products that are rich in refined carbohydrates and are quickly digested and absorbed, causing a rapid rise in blood sugar and associated complications and disorders. 17 When compared to goods with a lower GI, which give a more stable diurnal blood glucose profile, these products normalize postprandial blood glucose levels and hyperinsulinemia while minimizing late postprandial rebounds in circulating FFAs. 20 Subjects on a high GI diet show levels along with elevation in aspartate aminotransferase (AST), TG, homeostatic model assessment-IR (HOMA-IR) score, total cholesterol (TC), and various inflammatory mediators in the liver, which are cumulatively responsible for diabetes-associated metabolic disorders. 34 Mice on a high GI diet led to a change in substrate oxidation, leading to IR along with an elevation in AST and inflammatory biomarkers in the liver, which ultimately leads to metabolic syndrome-like MAFLD, MASLD, etc. 35 Consumption of a low GI diet benefited the diabetes-associated MAFLD patients, as there was a significant decrease in glycated hemoglobin (HbA1c) and TG levels, along with an elevation in high-density lipoprotein (HDL) levels, hence establishing a strong positive correlation between a high GI and the prevalence of having diabetes-associated MAFLD. 36 Probiotic supplementation may improve the condition of diabetes-associated MAFLD by reducing the glycemic condition in patients, hence demonstrating the importance of diet GI as one of the most significant factors in diabetes-associated MAFLD. 37
Mechanistic Approaches for Dietary Supplementation and Interventions in the Management of Diabetes-associated MAFLD
The management of metabolic complications with the help of dietary intervention and change in diet style via controlling the intake of high GI index, high-fat, and high-fructose-rich food products is widely accepted by health professionals. These scientific approaches target the overall change in energy consumption or dietary macronutrient composition, as well as adding dietary supplements to their regular diets. There will be an utmost need to check the comprehensive assessments of excess energy intake with adequate nutritional therapy to produce better results for the management of various metabolic disorders.19–21
The dietary interventions discussed in this review are systematically classified into three broad categories to enhance clarity and applicability. These include: (a) Single nutrient components, such as vitamin D, PUFA and isoflavones; (b) dietary patterns, including ketogenic and low-carbohydrate diets; and (c) whole or natural food-based approaches, such as leafy greens and calorie-deficient strategies.
Single Nutrient Components
Vitamin D-rich Diet
Vitamin D is a fat-soluble secosteroid used in the absorption and retention of calcium (Ca2+), magnesium (Mg), and phosphate (PO43-) in the body for building bones. It has long been known for its association with obesity and the onset of T2DM and its complications. The linkage between vitamin D deficiency and IR is the key player in the progression of T2DM into MAFLD. It has been reported that vitamin D controls the expression of genes, which can control the physiological levels of Ca2+ and reactive oxygen species (ROS). 38 Moreover, vitamin D has a protective role in mediating inflammation as well as maintaining the normal mitochondrial control of cellular bioenergetics. Therefore, its deficiency can lead to altering the homeostasis of Ca2+ levels, production of ROS, mediation of inflammation, and mitochondrial functioning, which can result in the onset of diabetes and further progress it to MAFLD. 39 The mechanistic pathways by which vitamin D may protect against MAFLD are not clearly understood; however, various putative mechanisms have been postulated:
Modulation of Insulin Secretion and Resistance
Vitamin D has been proven to increase insulin sensitivity and improve IR, both of which are important factors in the development of MAFLD. By regulating the expression of genes involved in glucose and fat metabolism, vitamin D may alleviate IR. Therefore, it has been postulated that a Vitamin D-rich diet can reduce glycemia and increase insulin secretion in T2DM patients and associated metabolic disorders like MAFLD, MASLD, etc., with known hypovitaminosis related to vitamin D, implying a role of vitamin D in the pathophysiology of T2DM. 40 Vitamin D regulates insulin production and secretion by acting directly on pancreatic β-cells’ activity and plasma Ca2+ levels. The presence of vitamin D receptors (VDR) and vitamin D–binding proteins (DBP) in pancreatic tissue, as well as a link between certain allelic variants in the VDR and DBP genes and glucose tolerance and insulin secretion, all lend support to this notion. 41 Numerous in vitro and in vivo data have revealed that vitamin D can modulate insulin production and secretion in β-cells through multiple pathways, 42 which can help in glucose homeostasis. Many suggest it may be due to the reduction in JNK activation, 43 and restoration of Ca2+ homeostasis. 44 Additionally, in a recent systematic review and meta-analysis, 45 Vitamin D supplementation has revealed that it can improve IR in MAFLD patients, marked by reduced HOMA-IR, with a pooled mean difference of –1.06 (p = .0006; 95% CI = –1.66 to –0.45). Also, the supplementation of vitamin D increases the serum levels of vitamin D and decreases ALT levels, but no change has been seen in AST levels. Similarly, there is a large amount of evidence based on clinical studies, systematic reviews, and meta-analyses46–48 suggesting the supplementation of vitamin D might have a beneficial effect on glucose homeostasis and IR in MAFLD patients. Similarly, another clinical study was performed where it was demonstrated that vitamin D supplementation may improve diabetes-associated MAFLD, and the related evidence is summarized in Table S1 (Supplementary data).
Via Reduction of Inflammation
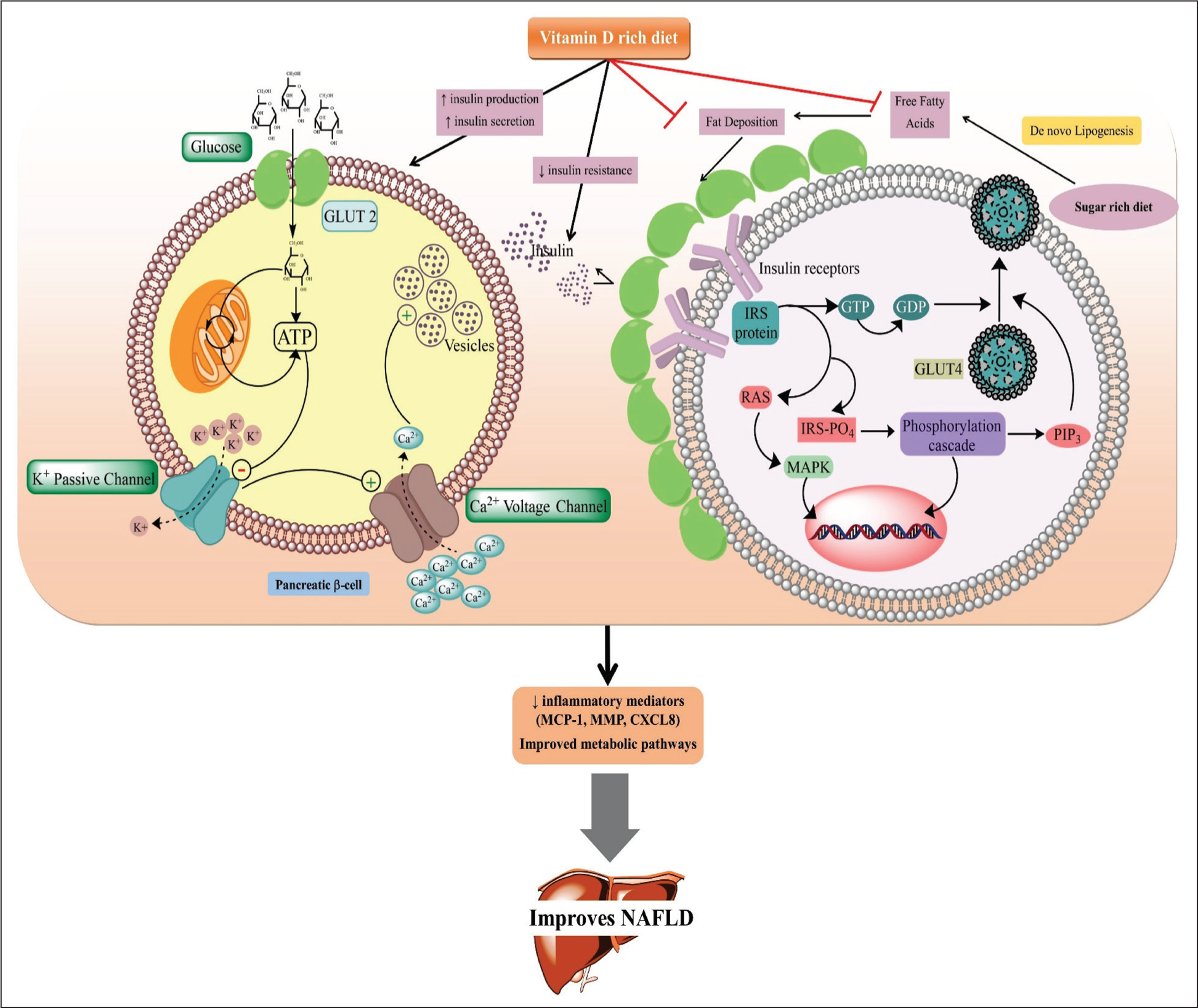
Evidence suggests that a lack of vitamin D may lead to inflammation and the development of non-alcoholic fatty liver disease (NAFLD). Inflammation is a common feature of MAFLD, and studies have shown that vitamin D has anti-inflammatory effects. Vitamin D deficiency has been linked to higher levels of pro-inflammatory cytokines like interleukin-6 (IL-6), IL-1β and TNF-α, both of which are involved in the pathophysiology of MAFLD. Furthermore, research has revealed that vitamin D insufficiency is prevalent in people with MAFLD and that low vitamin D levels are linked to an increased risk of MAFLD progression. Vitamin D supplementation has recently been demonstrated in trials to enhance circulating vitamin D, and decrease TC, HbA1c, low density lipoproteins (LDL), HOMA-IR, and TG levels, all of which contribute to significantly decreasing the inflammatory mediators (such as membrane cofactor protein [MCP-1], MMP, CXCL8, etc.), and IR help in the management of liver diseases as depicted in Figure 2. 49 Also, in a 12-week randomized controlled trial, the vitamin D-fortified drink-taking group showed an increase in the serum levels of vitamin D as well as a reduction in the expressions of TNF-α, C-reactive protein (CRP), amyloid A (AA), IL-6, and IL-10 compared to the control group (unfortified drink). 50 In conclusion, there is evidence to suggest that vitamin D deficiency may contribute to inflammation and the development of MAFLD. Adequate vitamin D levels may have protective effects against MAFLD, although further research is needed to fully understand the mechanisms involved.
Highlighting the Ameliorative Mechanism of Vitamin D Supplementation in Diabetes-associated MAFLD. A Vitamin D-containing Diet, upon Interaction with Vitamin D Receptors (VDR) and Vitamin D–Binding Proteins (DBP) in Pancreatic Tissue, Leads to Stimulation of Insulin Release via Exogenous Glucose, Which Is Taken up by GLUT2 and Undergoes Glycolysis Inside the Cell. This Leads to Elevated ATP Levels, Which Alter the ATP/ADP Ratio, Which in Turn Leads to the Closure of ATP-sensitive K+ Channels and Opens Voltage-dependent Ca2+ Channels in Response to Increasing Intracellular Calcium Levels, Which Eventually Trigger Insulin Secretion Following Vesicle Fusion with Membrane Along with via Decreasing Fat Deposition From Insulin Receptors Leading to Activation of Mitogen-activated Protein Kinase Which Leads to IRS1 Protein Phosphorylation Causing Cell Proliferation. The Phosphorylated IRS1 Promotes GLUT4 Translocation to the Plasma Membrane and Further Glucose Uptake. This Together Leads to a Decrease in Inflammatory Mediators (MCP-1, MMP, CXCL9, etc.), Ultimately Benefiting Subjects with Diabetes-associated MAFLD. ATP, Adenosine Triphosphate; CXCL8, C-X-C Motif Chemokine Ligand 8; GLUT2, Glucose Transporter 2; GLUT4, Glucose Transporter 4; IRS, Insulin Receptor Substrate; IRS PO4, Insulin Receptor Substrate Phosphorus; MAPK, Mitogen-activated Protein Kinase; MCP-1, Monocyte Chemoattractant Protein-1; MMP, Matrix Metalloproteinases; PIP3, Phosphatidylinositol-3,4,5-triphosphate; RAS, Activator of Raf.
Reduction in Oxidative Stress by Antioxidant Enzymes
Oxidative stress is a significant factor in the emergence and advancement of MAFLD, and the antioxidant properties of vitamin D have been shown to be advantageous in decreasing oxidative stress in the liver. MAFLD is marked by a disturbance in the equilibrium between the ROS generation and hepatic cellular antioxidant defense mechanisms. The Overproduction of ROS can cause oxidative damage to cellular macromolecules such as proteins, lipids, and DNA, which will further contribute to hepatocellular injury and inflammation. 51
The neutralization of excessively generated ROS by the antioxidants can serve as an essential role in maintaining the redox balance that ultimately helps in reducing oxidative stress. Among various cell types, including hepatocytes, vitamin D is expressed in all the cells, which has been reported to have a significant antioxidant property. 52 Vitamin D has the potential to downregulate the enzymes that are responsible for ROS production, like NADPH oxidase, and upregulate the expression of antioxidant enzymes like catalase and superoxide dismutase (SOD), which are very crucial for the detoxification of ROS and ultimately provide a protective effect to the liver cells from ROS-induced hepatic cell injury and inflammation. Vitamin D’s antioxidant property highlights its therapeutic potential in diseases associated with oxidative stress, such as MAFLD. More studies indicated that MAFLD patients with low vitamin D experience high oxidative stress. 53 In contrast, vitamin D supplementation aids in alleviating the oxidative stress in animal models with MAFLD.
Suppression in Nrf2/HO-1 Mediated Oxidative Stress Pathway
In the hepatic cellular defense system for the mitigation of oxidative stress, inflammation, and tissue injury, the Nrf2/HO-1 signaling pathway plays a crucial role. A recent finding suggests that vitamin D has the capability to stimulate this pathway and thereby promote the up-modulation of antioxidant enzymes, which further assist in liver protection in MASLD. In vivo studies on MAFLD have demonstrated that vitamin D supplementation enhances the expression of Nrf2 and HO-1, which further results in the reduction of oxidative stress and improvement of hepatic activity.
An investigation done by Zhu et al. 54 showed that in mice-fed a HFD-induced model in mice, if vitamin D supplementation is given, it shows promising outcomes by alleviating hepatic injury and oxidative stress through induction of the Nrf2/HO-1 signaling pathway. Moreover, supplements of vitamin D, if given to patients with MAFLD, it up regulates expression of genes which are associated with the Nrf2/HO-1 pathway by inhibiting the redox biomarkers. 55 Hence, an in-depth investigation is necessary for a better understanding of the underlying mechanism, which can reveal the molecular crosstalk between the Nrf2/HO-1 pathway and vitamin D in MAFLD.
Reduction in Oxidative Stress Via the NADPH Oxidase Pathway
Numerous studies highlighted that NADPH oxidase plays a crucial role in the pathogenesis of MAFLD. It is also documented in the studies that vitamin D can also emerge as an important molecule that can help in alleviating the NADPH oxidase pathway. During the in vivo studies done by the researcher, it was observed that supplementation with vitamin D can reduce the up-regulation of NADPH oxidase expression and activity in hepatocytes. 56 Likewise, research done by Dong et al. (2019) investigates that during exposure to high glucose conditions in hepatic cells, vitamin D supplementation helps in the suppression of NADPH oxidase activation. These research findings make it clear that vitamin D has the potential to attenuate oxidative stress and hepatocellular injury through diminishing the NADPH oxidase pathway. On the other hand, during the clinical investigation in patients with MAFLD, it has been observed that the serum vitamin D level is low, and they have elevated NADPH oxidase levels in their bodies that contribute to the ROS accumulation and hepatic cell injury. 57 These research findings collectively suggest that vitamin D deficiency can lead to increased oxidative stress, which can further lead to enhanced activation of NADPH oxidase to generate more ROS, which can result in liver cell injury. Hence, it is evident that vitamin D plays a pivotal modulatory role in regulating NADPH oxidase activity, and its supplementation can reduce the oxidative pathway of NADPH, which can ultimately affect the development of MAFLD. 58
Reduction in Oxidative Stress Via Mitochondrial Dysfunction
Recent research suggests that mitochondrial dysfunction can contribute to MAFLD due to the enhanced oxidative damage, inflammation, and liver cell death. The mitochondria play a pivotal role in cellular energy metabolism, a primary site for ATP production, and any type of impairment in mitochondrial activity can lead to hepatocellular damage. Evolving studies suggest that vitamin D can serve a defensive role in protecting mitochondria from oxidative damage in relation to MAFLD. Manna et al. 58 research studies suggest that in an in vivo model of HFD-induced MAFLD, vitamin D supplementation shows a promising role in protecting mitochondrial damage. During the research, it is also demonstrated that vitamin D can elevate the performance of mitochondria and upregulate its electron transport chain-related enzymes activity and help to reduce oxidative stress. Correspondingly, recent evidence investigated the correlation between vitamin D and mitochondrial dysfunction in patients with MAFLD, and its results reveal that vitamin D deficiency was associated with elevated oxidative damage and mitochondrial impairment. 59 In addition to those studies, it has also been examined in a murine model that vitamin D supplementation can augment the impaired mitochondrial activity and diminish oxidative stress markers in hepatic cells. 54 Moreover, ex vivo assays show that vitamin D modulates the regulation of genes of electron transport chain enzymes and their activity, including PGC-1α and SIRT,60,61 which emphasize its role in maintaining mitochondrial homeostasis in MAFLD patients.
In summary, vitamin D possesses antioxidant properties that can play a significant role in the mitigation of oxidative stress in hepatocytes and provide a protective effect in MAFLD progression. Moreover, additional research studies are required to fully unveil the underlying mechanism of the antioxidant effect of vitamin D in reference to MAFLD.
Regulation of Fatty Acid Uptake and Beta-oxidation
Emerging research findings suggest that vitamin D can modulate β-oxidation and fatty acid infiltration and therefore possesses potential in benefiting the patients who exhibit hepatic steatosis in MAFLD. Vitamin D down-modulates the gene expression of enzymes that are involved in lipid influx, including CD36 and FABP4 in liver cells.62,63 This suppression minimizes the infiltration of fat molecules, which can result in a decrease in the retention of lipids within hepatic cells. Second, it has been demonstrated that vitamin D increases the expression of genes related to beta-oxidation, including CPT1A and ACOX1. 64 The method by which fatty acids are broken down in the liver to create energy is known as beta-oxidation. Vitamin D supplementation helps decrease hepatic steatosis by speeding up the rate of fatty acid breakdown in the liver by raising the expression of these genes. Additionally, in a study by Du et al., 65 in vitro by the use of HepG2 cells in oleic acid and in vivo by HFD-induced MAFLD, evidence has been given that vitamin D treatment may improve the hepatic steatosis in MAFLD through the modulation of uptake of fatty acids and β-oxidation by modulating the PPAR-α signaling pathway. This has been confirmed by the administration of MK886 (PPAR-α antagonist), which inhibits the steatosis activity of vitamin D both in vitro and in vivo via the PPAR-α pathway.
Genetic and Epigenetic Mechanisms
Since alteration of gene expression is involved in the pathogenesis of MAFLD and facilitates its progression, vitamin D may play a role in modulating gene expression and potentially preventing or ameliorating the development of MAFLD. Currently, there is no clear evidence to support the role of genetic or epigenetic mechanisms in mediating the effects of vitamin D on MAFLD. However, a study by Barchetta et al. 48 demonstrated altered expression of vitamin D-related genes, including VDR, CYP2R1, and CYP27A1, in the liver tissues of patients with MASLD and HCV, compared to healthy controls. The expressions of VDR and CYP2R1 were found to be decreased in both patients, whereas CYP27A1 expressions were found to be decreased in MASLD patients only.
Moreover, the genetic regulation of VDR and CYP2R1 has shown a concurrent relationship with serum vitamin D3 concentrations, and conversely, with CYP2R1, it shows an inverse relationship. Such findings reveal that any dysfunction in the vitamin D biotransformation can result in the HCV-related hepatic disorders and MASLD. Such insights emphasize the need for more in-depth research for the development of underlying mechanisms that are involved in hepatic disorders and MASLD in relation to vitamin D. Hence, vitamin D deficiency within the hepatocytes plays a pivotal role in the initiation and development of MASLD, and elevating serum vitamin D3 via supplementation can help in surging the level of vitamin D in hepatic cells and potentially attenuate the MASLD-related hepatocellular damage.
Soy Isoflavones
The soy isoflavones are a group of phytoestrogens that are present in soybeans and soy-based food products and have shown a beneficial role in mitigating MAFLD. Though the underlying mechanism of soy isoflavones for influencing MAFLD is still constrained, various hypotheses have been proposed for unveiling its activity, which are as follows:
Fatty Acid Metabolism Regulation
The crucial factor in the development and exacerbation of MASLD is lipid metabolism, and various studies show that soy isoflavones have therapeutic potential in reducing the oxidation of fatty acids. Research evidence suggests that this emerging role is due to the fact that isoflavones reduce the genetic expression of the enzymes that are involved in the oxidation of lipids and lipid synthesis, for instance, PPAR-α (proliferator-activated receptor alpha) and SREBP-1c (sterol regulatory element-binding protein-1c). PPAR-α serves as a transcriptional regulator that facilitates the gene expression of the enzymes that are involved in lipid metabolic pathways; on the other hand, SREBP-1c modulates the gene regulation of enzymes in the de novo lipogenesis pathway.
Soy isoflavones aid in reducing the accumulation of lipid by activating PPAR-α and inhibiting SREBP-1c. In recent research, it has been demonstrated that soy isoflavones show a similar effect in rats with MASLD (metabolic-associated steatosis liver disease) by enhancing the activity of PPAR-α and mitigating the fat buildup in the liver. 66 Moreover, research studies state that in rats with MASLD, investigations also down-modulate SREBP-1c, which is a key regulator of lipid synthesis in the liver. 67 Hence, it is clearly indicated that isoflavone has the potential to manage MAFLD by reducing the generation of lipids in the liver.
Anti-inflammatory Effects Via Reduction of Pro-inflammatory Cytokines
Soy isoflavones are also known for their anti-inflammatory properties that reduce the inflammation of the liver, which is the hallmark of MASLD. Soy isoflavone mitigates the pro-inflammatory mediators such as TNF-α and IL-6. Then rodent studies also showed that genistein, which is a soy isoflavone, lowers the retention of lipids in the liver. Also, it helps in the improvement of insulin sensitivity, lipid profile, and hepatic activity. It decreases pro-inflammatory cytokines and oxidative stress levels, which helps in the protection of high-fructose-induced insulin-resistant rats. 68
Also, during a double-blind randomized controlled trial, 82 patients with MAFLD were given a daily supplement of either 250 mg of genistein (n = 41) or a placebo (n = 41) for 8 weeks. The group that received genistein had significantly lower levels of serum insulin, MDA, TNF-α, and IL-6, as well as improved IR. Moreover, they had reduced waist-to-hip ratios, body fat percentages, and triglycerides as compared to the placebo group. However, there was no significant difference in BMI, fasting blood glucose, ALT, and AST between the two groups. 69 Hence, this indicates that soy isoflavones exhibit anti-inflammatory properties that help in beneficial effects against MASLD.
Anti-inflammatory Effects Through the COX/NF-κ B/MAPK Pathway
Genistein is a very good example of soy isoflavonoids that contains the ability to modulate the COX/NF-κB/MAPK pathways, which are directly linked to inflammation and oxidative stress. 70 In in vivo studies, genistein also demonstrates that it decreases the levels of inflammatory markers like TNF-α and IL-6. It also down-regulates the NF-ĸB p65 nuclear translocation, JNK activation, and Iĸβ-α phosphorylation. 71 These findings suggest that genistein has potential in reducing liver inflammation with special reference to MASLD.
The research findings emphasize the potential of genistein in COX/NF-κB/MAPK pathways, which further helps in the reduction of inflammation in HFD-induced MASLD in rats. 72 Soy isoflavanoids exert anti-inflammatory effects by altering these pathways. Soy isoflavones suppress inflammation that is linked with the MAFLD. As a result, it targets NF-ĸB/MAPK pathways that show its potential as an anti-inflammatory agent and help in managing MAFLD and its progression.
Antioxidant Effects
Soy isoflavonoids exhibit a very strong antioxidant effect, which helps in mitigating the oxidative stress in the liver, which is a key factor in the progression of MAFLD. They can detoxify free oxidative radicals and boost the antioxidant enzymes like glutathione and SOD, and as a consequence, they decrease lipid peroxidation. The research findings also show that genistein has the capacity to lower and reduce the level of MDA (malondialdehyde), which is a central player in oxidative damage in an HFD-induced mouse model. 73 Correspondingly, in MAFLD-induced rodent models, soy isoflavones increase the SOD level and minimize lipid peroxidation. 74 These demonstrations suggest that isoflavones aid in restoring the antioxidant equilibrium and protecting the oxidative damage of the liver by MAFLD.
Regulation of IR Via IRS-1 and GLUT
Soy isoflavones may improve insulin sensitivity and reduce IR (a crucial factor in the progression of MAFLD) by modulating the expression of genes involved in glucose and lipid metabolism. Insulin receptor substrate-1 (IRS-1) and glucose transporter (GLUT) are the significant genes which are involved in glucose and lipid metabolism. IRS-1 has a function in insulin signaling, whereas GLUT has a function in glucose transport. Biochanin A (soy isoflavone) has been seen to improve insulin sensitivity and reduce IR by modulating the PI3K/AKT pathway, which increases the expression of IRS-1 and GLUT4 in HFD-induced insulin-resistant mice. 75 Similarly, in STZ and HFD-fed BALB/c mice, administration of aglycin (a bioactive peptide from soybean) has been reported to increase the gene expressions of IRS-1, GLUT-4 and AKT, which improves insulin sensitivity as well as decreases IR. 76 Hence, through the regulation of gene expressions related to insulin signaling, such as IRS-1 and GLUT, soy isoflavones have the potential to alleviate IR and enhance insulin sensitivity.
Regulation of IR Via AMPK
Another mechanism of improving lipid and glucose metabolism in order to mitigate IR is through the activation of the AMPK pathway. In CD-1 male mice, administration of a soy-rich diet increased the expression of AMPK phosphorylation and acetyl-CoA carboxylase (ACC), along with up-regulation of genes implicated in peroxisomal fatty acid oxidation and mitochondrial biogenesis. 77 This leads to the improvement of IR due to increased glucose uptake into skeletal muscles. This beneficial effect of a soy isoflavonoid-rich diet can have significant implications for patients with NAFLD. By improving insulin sensitivity, soy isoflavones may help restore proper glucose metabolism and promote better control of blood sugar levels, which is crucial in managing MAFLD.
Regulation of IR Via cAMP
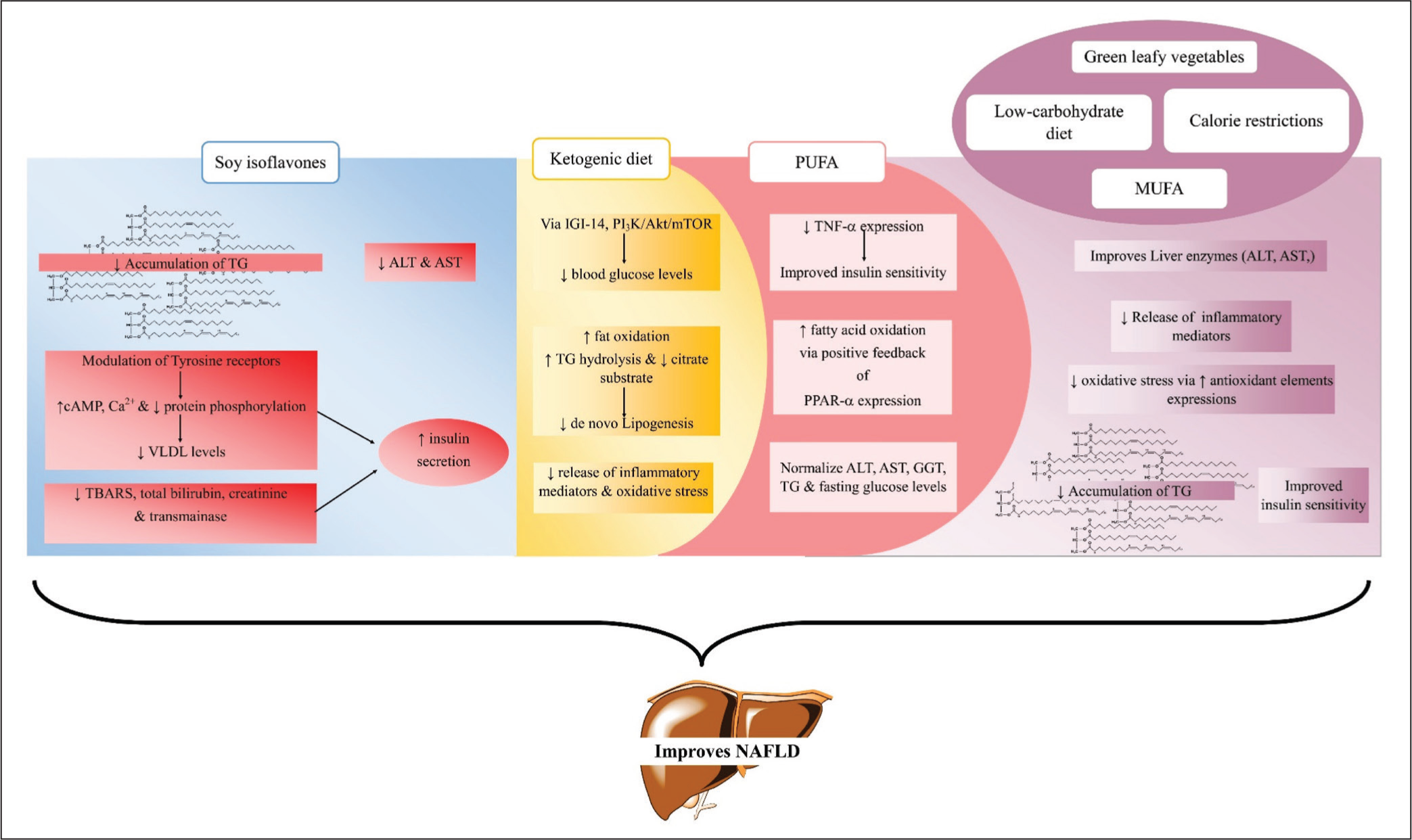
Soy isoflavones increase insulin secretion via tyrosine receptor modulating increased cyclic adenosine monophosphate (cAMP) and Ca2+ and downregulating protein phosphorylation, causing an effect on SREBP-2 and oxysterols, ultimately decreasing VLDL levels, which contributes to the suppression of diabetes-associated MAFLD as shown in Figure 3. 78 The cAMP pathway is a signaling pathway that plays an important role in several cellular processes, including lipid metabolism and inflammation, which are involved in the pathogenesis of MAFLD. Dysregulation of the cAMP pathway has been implicated in the development and progression of MAFLD.
Highlighting the Ameliorative Mechanisms of Various Dietary Interventions in Diabetes-associated MAFLD Where Soy Isoflavones Enriched Diet Increases Insulin Secretion via Tyrosine Receptor Modulating Increase Cyclic Adenosine Monophosphate (cAMP), Ca2+ and Down Regulating Protein Phosphorylation, Ultimately Decreasing VLDL, TBARS, Creatinine and Transaminases Content Along With Decrease in Accumulation of TG, ALT and AST Levels; Ketogenic Diet Significantly Decrease in Glucose Levels via IGI-14, P13K, AKT and mTOR Along With Increase in Fat Oxidation and Decreased de Novo Lipogenesis via Increase TG Hydrolysis and Decreased Citrate Substrate Leading to Subsequent Inflammatory and Oxidative Stress Limitation; PUFA Enriched Diet Decrease Hepatic TNF-α Expression, Suppresses Fatty Acid Synthesis via Negatively Controlling SREBP-1c, and Increases Fatty Acid Oxidation via Positive Feedback of PPARα Expression Resulting in Increased Insulin Secretion and Normal Levels of ALT, AST, GGT and TG Levels; Other Dietary Interventions—MUFA, Low-carbohydrate Diet, Calorie Restrictions and Green Leafy Vegetables Normalizes Liver Enzymes (ALT, AST, etc.), Decreasing Accumulation of TG and Increasing Insulin Release via Decrease in Inflammatory Mediators and Oxidative Stress. AKT, Ak Strain Transforming; ALT, Alanine Aminotransferase; AST, Aspartate Aminotransferase; cAMP, Cyclic Adenosine Monophosphate; GGT, Gamma-glutamyl Transferase; IGI-14, Insulin Secretion Capacity-14; MUFA, Monounsaturated Fatty Acids; mTOR, Mammalian Target of Rapamycin; P13K, Phosphoinositide 3-kinases; PPARα, Peroxisome Proliferator-activated Receptor Alpha; PUFA, Polyunsaturated Fatty Acids; SREBP-1c, Sterol Regulatory Element-binding Protein 1; TBARS, Thiobarbituric Acid Reactive Substances; TNF-α, Tumor Necrosis Factor Alpha; TG, Triglycerides; VLDL, Very-low-density Lipoprotein.
Modulation of Gut Microbiota
The gut microbiota has been implicated in the onset and progression of MAFLD. Studies Chen et al. 79 suggest that the administration of soy isoflavones has the potential to alter the composition of the gut microbiota by promoting the growth of beneficial bacteria while decreasing the prevalence of harmful bacteria. Soybean isoflavone-fed old Kunming mice showed an increase in food intake but lower body weight gain compared to normal-fed mice. The abundance of lumen-associated bacteria (LAB) and mucosa-associated bacteria (MAB) was found to be increased in soybean isoflavone-fed mice. 80 Also, in HFD-induced MAFLD rats, the fermented soy paste increased the abundance of Prevotellaceae NK3B31 and Desulfovibrio as well as reduced the levels of serum triglyceride, alanine aminotransferase (ALT), and lipid accumulation through activation of the AMPK pathway. 81 Consequently, through its ability to influence the gut microbiota, soy isoflavones have the potential to mitigate the advancement and occurrence of MAFLD, making them a potential therapeutic option for its treatment.
Hepatoprotective Effects Via ChREBP & Wnt/GSK3β Pathway
MAFLD is associated with multiple pathological conditions such as hepatic fibrosis, liver tumorigenesis, liver damage, and so on. Studies (refer to Xin et al.) 82 have reported that soy isoflavones exhibit hepatoprotective properties, which can be advantageous in mitigating the harmful progression of MAFLD and promoting liver health. Extensive research has established the ability of soy isoflavones to effectively modulate the expression of genes in the liver, making them a promising therapeutic approach for the treatment of MAFLD. For instance, by targeting carbohydrate-responsive element-binding protein (ChREBP), a transcription factor that initiates the transcription of lipogenic genes within the liver in response to an excessive dietary intake of carbohydrates. 83 By inducing the phosphorylation of AMPK, soy isoflavones effectively inhibit the signaling pathway of ChREBP. This inhibition impedes the binding of ChREBP to the promoter region of lipogenic enzymes. 84 As a result, the downstream effects of ChREBP-mediated lipogenesis are suppressed, thereby potentially reducing lipid accumulation and promoting a more favorable metabolic profile. Furthermore, isoflavones also exhibit an influence on the Wnt signaling pathway, specifically targeting hepatic genes. In MAFLD, key regulators of canonical Wnt signaling, such as β-catenin, GSK-3β, and so on, are abnormally regulated, which leads to the progression of MAFLD and MASLD to hepatic fibrosis and hepatocellular carcinoma. 85 Therefore, any abrupt signaling can be proven to be detrimental to MAFLD. However, soy isoflavones have some positive modulation on the Wnt pathway 84 activated through the estrogen receptor-dependent pathway, which leads to the inhibition of GSK-3β, which results in the activation of transactivating T-cell factor/lymphoid-enhancer factor (TCF/LEF), 86 an effector of Wnt signaling which promotes gene transcription. Moreover, soy isoflavone is also implicated in the degradation of PPAR-γ (adipogenic) 87 and enhances the activity of p300/CBP (transcriptional co-activators of TCF/LEF), 88 which further regulates the gene expressions and transcriptional activity related to adipogenesis. 84 By targeting this pathway, isoflavones can exert regulatory effects on the cellular processes and signaling cascades that are governed by Wnt signaling in hepatic cells.
Hepatoprotective Effects Via Reduction of Liver Enzymes
Diabetic rats, when fed with soy isoflavones, show that it protects hepatic functions as evidenced by reduction in thiobarbituric acid reactive substances, total bilirubin, creatinine, and transaminase content, which helps in increased insulin secretion and is ultimately beneficial for liver diseases like MAFLD, MASLD, etc. 89 Obese female Zucker rats on a short-term (8-week) soy isoflavone diet had lower serum AST and ALT levels than rats on a casein diet, acting beneficially in diabetes and their associated liver diseases like MAFLD. 90 Soy isoflavones had favorable effects on ALT by normalizing their levels and high sensitivity of CRP (hs-CRP) in overweight and obese patients with MAFLD.91,92 The other related clinical evidence of isoflavones acting as an intervention in diabetes-associated MAFLD is shown in Table S2 (Supplementary data). In conclusion, soy isoflavones may protect against MAFLD by regulating lipid metabolism, reducing inflammation and oxidative stress, improving IR, modulating the gut microbiota, and exerting hepatoprotective effects through multiple pathways affecting hepatic gene expressions. Soy isoflavones have been linked to cellular and molecular regulatory processes in animals and humans and have been shown to be useful in metabolic illnesses such as IR, dyslipidemia, and various metabolic disorders like MAFLD and MASLD. Soy isoflavone consumption lowers the risk of lipotoxicity by preventing TG accumulation in the liver. However, further research is needed to fully understand the underlying mechanisms involved and to determine the optimal dose and duration of soy isoflavone supplementation for MAFLD prevention and treatment.
Unsaturated Fatty Acid Diet
It contains monounsaturated and polyunsaturated fatty acids (PUFA), which help people manage MAFLD, lose weight, reduce hepatic TG accumulation and IR, and minimize steatosis-like devastating problems. which leads to liver complications. 93
Polyunsaturated Fatty Acids
By influencing the transcription of genes involved in lipid metabolism, omega-3 and omega-6 fatty acids normalize insulin sensitivity by decreasing hepatic TNF-α expression, suppressing fatty acid synthesis (FAS) via negatively controlling SREBP-1c, and increasing fatty acid oxidation via positive feedback of PPARα expression.94–96 Omega-3 fatty acids were found to normalize various biochemical parameters of MAFLD patients, like ALT, AST, gamma-glutamyl transferase (GGT), TG, and fasting glucose concentrations in several investigations, as represented in Figure 3.97–100 A live multi-strain probiotic mixture with omega-3 fatty acids once a day for 8 weeks can reduce liver fat, normalize blood lipids and metabolic profiles, and reduce chronic systemic inflammatory states in patients with insulin sensitivity and other liver diseases like MAFLD. 101 In lieu of the above evidence, the other possible research outcome was summarized in Table S3 (Supplementary data) with reference to various clinical evidence of PUFA-related intervention in diabetes-related MAFLD subjects.
Monounsaturated Fatty Acids
It is depicted that monounsaturated fatty acids (MUFA) aid in the reduction of oxidation and blood concentrations of LDL, TC, and triacylglycerols, as well as the modulation of insulin-sensitizing gene expression. MUFA aids in the prevention of diabetes and associated metabolic disorders, such as MAFLD, which is summarized in Figure 3. 102 Phenol-rich extra virgin olive oil, which contains MUFA, can repair HFD-induced diabetes and liver disorders such as MAFLD, possibly through an anti-inflammatory effect in adipose tissue and changes in liver lipid composition and signaling pathways in high-fat “Western-type” fed mice. 103 Dietary supplementation with FLINAX, a novel combination of nutraceuticals (i.e., vitamin E, vitamin D3, olive dry extract, cinnamon dry extract, and fish oil), reprogrammed cellular energy homeostasis by restoring mitochondrial function efficiency, with a consequent improvement in diabetes and associated fibrosis in male Wistar rats. 104 Co-supplementing Camelina sativa oil, which contains MUFA and resistant dextrin, with a low-calorie diet reduces HOMA-IR, hs-CRP, endotoxin, cortisol, general health questionnaire (GHQ), DASS, malondialdehyde (MDA), and increases levels of tacrolimus (TAC) and SOD, which decreased IR and associated metabolic disorders like MAFLD. 105 The related clinical evidence of MUFA acting as an intervention in diabetes-associated MAFLD is discussed in Table S6 (Supplementary data).
Dietary Patterns
Ketogenic Diet
Ketogenic diets are a fresh form of diabetes treatment that has been associated with a significant decrease in MAFLD and other metabolic disorders. 11 It causes a significant decrease in glucose levels via insulin secretion capacity-14 (IGI-14), phosphoinositide 3-kinases (PI3K), Ak strain transforming (AKT), and mammalian target of rapamycin (mTOR) as well as an increase in fat oxidation and decreased de novo lipogenesis via increased TG hydrolysis and decreased citrate substrate, as well as a microbiome shift with increased folate production and subsequent inflammatory and oxidative stress limitation, all of which contribute to liver fat reduction and aid in the treatment of diabetes-related MAFLD as illustrated in Figure 3. 106
Males benefit more from the low-carbohydrate ketogenic diet than females, as evidenced by a clinical trial conducted. Males lost significantly more excess body weight (EBWL) and had a bigger drop in glutamyl transferase (GT) than females. 107 When compared to patients on a standard low-calorie diet, patients on a very low-calorie ketogenic diet plan achieved superior weight loss, along with significant visceral adipose tissue and liver fat fraction reductions, benefiting diabetes and associated metabolic disorders like MAFLD. 108 There are not enough scientific papers to fully comprehend the mechanism, so more research into pharmacological intervention for the treatment of diabetes and associated disorders is needed, and the clinical evidence of the ketogenic diet acting as an intervention in diabetes-associated MAFLD is summarized in Table S4 (Supplementary data).
Low-carbohydrate Diet
Long-term hyperglycemia, insulin sensitivity, and liver damage are all caused by a high-carbohydrate diet, which leads to steatosis, a severe deterioration marked by inflammation, Kupffer cell (KC) activation, and fibrosis (MASLD). TGF-β, CTGF, leptin, and stimulation of hepatic stellate cells (HSC) all contribute to the fibrotic process. 16 A low-carbohydrate diet normalizes the ALT levels and reduces blood glucose, LDL cholesterol, and blood pressure levels in patients suffering from diabetes-associated MAFLD, which is illustrated in Figure 3. 109 A three-fold low-carbohydrate diet leads to the normalization of the ALT, AST, and HOMA-IR index levels in patients suffering from metabolic complications related to MAFLD. 110 Table S5 (Supplementary data) summarizes related clinical evidence of a low-carbohydrate diet acting as an intervention in diabetes-associated MAFLD.
Whole or Natural Food-based Approaches
Green Leafy Vegetables
Green leafy vegetable consumption leads to a decrease in the severity of diabetes and associated metabolic syndromes like MAFLD, MASLD, etc., by normalizing the levels of AST, LDL, IR, and TC levels as compared to the diseased subjects, also summarized in Figure 3. 110 Supplementation with spinach reduced the effects of a high-fat meal by boosting Lactobacillus counts, lowering fasting glucose and total and LDL cholesterol, and avoiding the formation of extra liver cholesterol, ultimately benefiting diabetes-associated MAFLD. 111 There is a strong association between the consumption of green leafy vegetables and a decrease in the severity of diabetes and related liver diseases like MAFLD, as there is a significant lowering of TG, fasting blood glucose, and LDL levels in patients consuming green leafy vegetables. 112 Consumption of spinach and Korean cabbage leads to a decrease in the severity of diabetes-associated MAFLD by targeting TC, TG, and IR. 113 Green tea supplementation decreases ALT, AST, LDL, TG, etc., ultimately benefiting patients with diabetes and associated metabolic syndromes like MAFLD, MASLD, etc. 114 The related clinical evidence of green leafy vegetables consumption acting as a preventive as well as protective measure in diabetes-associated MAFLD is discussed in Table S7 (Supplementary data).
Calorie Restriction (Fasting)
A decrease in the chylomicron remnants leads to a decrease in acetyl-CoA levels, leading to a decrease in glycogenolysis and glucose production via downregulating dihydroxyacetone phosphate acyltransferase as well as acetyl-CoA and also upregulating the AMPK pathway, leading to a decrease in inflammatory mediators via peroxisome proliferator-activated receptor gamma activator-alpha (PGC-1α), forkhead box transcription factor (FOXO), and nuclear factor kappa B (NF-kβ) gene stimulation, ultimately benefiting patients with diabetes-associated MAFLD.115,116 A substantial reduction in anthropometric parameters, fasting glucose, plasma insulin, and IR, as well as inflammatory mediators (IL-6 and hs-CRP), all of which are beneficial to diabetes-related MAFLD, as depicted in Figure 3. 117 Within the same context, calorie restriction is beneficial in the management of diabetes-associated MAFLD by reducing LDL levels as compared to standard care of treatment, that is, via medicines. 118 Following an 8-week intermittent fasting regimen lowers ALT and blood glucose levels; this is beneficial for diabetes-related MAFLD. 119 There is still a gap between calorie restriction and its therapeutic usage in the therapy of diabetes-related MAFLD that has to be bridged.
Genetic Modification with Respect to Appropriate and Inappropriate Food Products in Diabetes-associated MAFLD Patients
Inappropriate Food Products and Genetic Modification
A sucrose-rich diet had higher Cd36 mRNA expression, which was linked with diabetes and metabolic diseases such as MAFLD, MASLD, etc., in Wistar rats. According to the physiological evidence, rats with higher Cd36 mRNA expression had higher belly fat, TG, FFAs, AST (Alanine transaminase), ALT, uric acid, and HOMA index, as well as IR, which are proven to be key parameters in the management of liver-related complications. 120 An HFHF diet fed Wistar rats leads to a decrease in the expression of miR-122, leading to altered expression of FAS and ACC, ultimately leading to IR and liver-related complications. 121 Participants with the minor allele of the haplotype at the 22q13 locus had a higher risk of diabetes and associated metabolic disorders like MAFLD, as serum AST and ALT activities were elevated, along with high serum glucose levels, which was exacerbated by high-carbohydrate intake and a dietary pattern that included a lot of junk food like noodles and pork. 122 Consumption of lard with coconut oil leads to increased expression of fatty acid binding proteins and acyl-CoA synthetase (ACS), ultimately worsening diabetes-associated MAFLD in HFHF Iberian pigs. 123 Within the same context, it was also stated that long-term SFA-rich diet consumption promoted activation of lipogenesis, NF-k light chain enhancer of activated B cells (NFB), and c-Jun N-terminal kinase (JNK)/activator protein-1 (AP-1) signaling and ensured overexpression of cyclin D1 and p62, leading to IR and associated metabolic disorders like MAFLD, MASLD, and others in rodents. 124 C57BL/6J male mice on a HFD showed increased peroxisome proliferator-activated receptor alpha (PPARα) and SREBP-1 expression and decreased PPARα expression were found in gelatinized wheat starch and high salt diet rats, resulting in accelerated adipogenesis and inducing toll like receptor 4 (TLR-4) activation via the gut–liver axis, resulting in a pro-inflammatory response by TNF-α and IL in the absence of improper dietary habits, dysregulation of FAS, FABPs, ACC, SREBP-1c, and ACS gene expression leads to the development of diabetes and associated metabolic disorders such as diabetes, MAFLD, and MASLD, according to the above-mentioned scientific publication. 125
Appropriate Food Products and Genetic Modification
In an HFD male C57Bl/6 mouse model, green tea prevents diabetes-associated MAFLD through modulating miR-34a and miR-194 expression. 126 In male Sprague Dawley rats, up-regulation of nuclear factor erythroid 2-related factor 2 (Nrf2), glutamate cysteine ligase catalytic subunit (Gclc), NAD(P)H, quinone dehydrogenase 1 (Nqo1), SOD2, and catalase (Cat) genes protects against HFD-induced diabetes-associated MAFLD. 54 Mulberry fruit treatment decreased cholesterol homeostasis-related genes, including FAS cell surface death receptor (FAS), SCD-1, and carnitine palmitoyl transferase I (CPT-1), SREBP1c, ameliorating diabetes and associated metabolic syndromes like MAFLD, MASLD, etc., in HFD-fed male Sprague Dawley rats. 127 Ginger extract reduces the carbohydrate response element-binding protein (ChREBP) lipogenic gene expression and endoplasmic reticulum (ER) stress genes like C/EBP homologous protein (CHOP), X-box binding protein (XBP1), and GRP78 levels in HFD-induced diabetes-associated MAFLD in Wistar male rats. 128 A high-protein diet decreased the FGF21 levels in subjects suffering from diabetes and associated metabolic syndrome-like MAFLD, MASLD, etc. 129 Further studies are warranted to systematically elucidate the epigenetic regulatory mechanisms underlying dietary interventions such as folate- mediated DNA methylation and soy isoflavones-induced modulation of microRNAs (e.g., MiR-34a) while also clarifying the influence of genetic background on therapeutic efficacy to enable more precise and personalized nutritional strategies. The above scientific evidence depicts that food interventions play a pivotal role in the management of diabetes-associated liver complications. There are still certain gaps that should be explored with reference to various gene expression which directly involved in the pathogenesis of diabetic liver injury.
Conclusions and Future Perspective
The dietary interventions exhibit dual roles encompassing both harmful and beneficial aspects, which are directly and indirectly associated with metabolic homeostasis. The above-discussed preclinical and clinical evidence, along with genetic and epigenetic insights, demonstrate that consumption of food products enriched with high-fat and high GI foods (e.g., refined carbohydrates and sugar-sweetened products) contributes significantly to the progression of diabetes-associated MAFLD. In contrast, targeted dietary strategies have been proven to be a better option during the early progressive phases of diabetes and liver-related problems. The interventions like soy isoflavones, ketogenic and low-carbohydrate diets have shown promising therapeutic potential by modulating key inflammatory, oxidative stress and metabolic pathways like AMPK activation, SREBP-1c/FAS inhibition and Nrf2 signaling.
Furthermore, emerging evidence highlights the involvement of genetic and epigenetic regulators, including microRNA (miR)-34a, miR-194, Nrf2, Gclc, Nqo1, Sod2, Cat, ChREBP, CHOP, XBP1, and GRP78, ultimately improving the condition of diabetes-associated MAFLD. Despite these advances, several critical gaps remain. Notably, long-term adherence to dietary interventions, variability in response across special populations (such as elderly, pediatric and comorbid patients) and limited personalization based on genetic background pose significant challenges.
The dietary changes for the patients set new trends for shifting the dietary interventions from bench to bedside of the patient. Moreover, the fewer side effects of this approach attract gastroenterological experts to think twice for the benefit of their patients while shifting them toward the pharmacological approaches. In addition, further exploration should elucidate the dietary intervention-gut microbiota-metabolic products-liver-gut-axis to better understand the underlying mechanistic pathways through which nutritional strategies modulate MAFLD progression and therapeutic outcomes. Addressing these challenges through well-designed clinical trials and integrative, multidisciplinary approaches will facilitate the effective translation of dietary strategies from bench to bedside, ultimately improving the management of diabetes-associated MAFLD.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
We would like to express our gratitude to the Chitkara University administration for their continued support in the successful completion of this manuscript.
Authors’ Contribution
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work. All the authors are eligible to be authors as per the International Committee of Medical Journal Editors (ICMJE) requirements/guidelines.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Data Availability Statement
Not applicable, as this is a review article and no new experimental datasets were generated. Supplementary materials supporting this review are provided with the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study does not involve experiments on animals or human subjects.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not Applicable.
Use of Artificial Intelligence-assisted Tools
The authors declare that they have not used artificial intelligence (AI)-tools for writing and editing of the manuscript, and no images were manipulated using AI.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.