
Abstract
This study aimed to develop the population pharmacokinetics (PopPK) model of isoniazid (INH) and its metabolite acetylisoniazid (AcINH) in Vietnamese tuberculosis (TB) patients. Using a nonlinear mixed-effects modeling approach with Monolix, the pharmacokinetics of INH and AcINH were characterized, while covariates were selected via the Conditional Sampling for Stepwise Approach based on Correlation tests (COSSAC). The analysis included 132 TB patients aged 16 years or older who were treated under Vietnam’s National Tuberculosis Program. INH was best described by a two-compartment model with first-order absorption (including lag time) and elimination, while AcINH followed a one-compartment model with first-order elimination. The inclusion of covariates significantly improved the model fit, as evidenced by a reduction in the Akaike information criterion (AIC) from 1,308 to 1,115.3 (∆AIC = 192.7). Significant covariates included N-acetyltransferase 2 (NAT2) acetylator phenotype, body weight, dose-to-weight ratio, and sex, all of which were found to influence key pharmacokinetic parameters. Final parameter estimates exhibited acceptable precision, with relative standard errors of ≤35.2% for fixed effects and ≤14.7% for interindividual variability. Model validation through goodness-of-fit plots, prediction error plots, visual predictive checks, and normalized prediction distribution error plots confirmed good predictive performance and agreement with observed data. Overall, this robust PopPK model of INH and AcINH, incorporating NAT2 acetylator phenotype and clinical covariates, supports the application of model-informed precision dosing to optimize INH therapy and reduce toxicity in genetically diverse populations.
Introduction
In 2024, the World Health Organization declared that tuberculosis (TB) had returned as the leading cause of death from a single infectious agent, surpassing COVID-19 after 2 years of this pandemic (2020–2021). Vietnam is among the top 20 high-burden countries for TB and multidrug-resistant or rifampicin-resistant TB (MDR/RR-TB). 1 In terms of TB treatment, barriers to successful outcomes include suboptimal regimen efficacy, adverse drug reactions, prolonged treatment duration, and high costs. 2 INH, a first-line anti-TB drug, frequently encounters inadequate plasma levels, which contribute to treatment failure. 3 The maximum concentration/minimum inhibitory concentration (Cmax/MIC) and area under the concentration–time curve/minimum inhibitory concentration (AUC/MIC) have been identified as INH pharmacokinetic parameters predicting the therapeutic response.3,4,5 However, the emergence of INH resistance has led to a wide range of MIC values in clinical isolates from TB patients. 6
Additionally, treatment with INH is further challenged by significant interindividual variability in its pharmacokinetics, making the achievement of optimal PK/PD targets difficult with a one-size-fits-all dose. A key contributor to this variability is N-acetyltransferase 2 (NAT2), the primary enzyme responsible for INH acetylation. 7 NAT2 polymorphisms define three acetylator phenotypes—rapid, intermediate, and slow—each associated with distinct pharmacokinetic profiles. 8 The slow acetylator (SA) phenotype is associated with an increased risk of hepatotoxicity due to higher INH concentrations, whereas the rapid acetylator (RA) phenotype exhibits significantly lower INH exposure, potentially leading to poor treatment outcomes.9–12 These polymorphisms have been reported in Asian populations, and previous studies have shown their impact on INH concentrations.10,13,14 In addition to the NAT2 acetylator phenotype, other covariates such as body weight, sex and HIV status also influence INH pharmacokinetics and, consequently, its clinical efficacy.11,15
Given these sources of variability, population pharmacokinetic (PopPK) modeling offers a valuable approach for quantifying drug disposition and identifying individual predictors of variability. When integrated with pharmacogenetic data, PopPK models can inform model-informed precision dosing (MIPD), enabling the optimization of INH therapy by tailoring regimens to patient-specific characteristics. 16
This study aims, therefore, to develop and validate a PopPK model of INH and its major metabolite acetylisoniazid (AcINH), in Vietnamese TB patients, incorporating both clinical covariates and NAT2 acetylator phenotype to support individualized dosing strategies.
Materials and Methods
Study Population
This study included patients aged 16 years or older who had newly diagnosed pulmonary TB or retreatment pulmonary TB with a positive acid-fast bacillus culture. Patients with MDR-TB were excluded from the study. Participants received treatment according to the National Tuberculosis Control Program of Vietnam using either:
Regimen IA rifampicin, isoniazid, pyrazinamide, and ethambutol (RHZE)/rifampicin, isoniazid, and ethambutol (RHE). A 2-month intensive phase with four daily drugs, followed by a 4-month continuation phase with three daily drugs. This regimen was prescribed for newly diagnosed adult TB cases. Regimen II (2SRHZE/1RHZE/5RHE): A 3-month intensive phase, including five daily drugs for the first 2 months and four daily drugs (RHZE) in the 3rd month, followed by a 5-month continuation phase with three daily drugs. This regimen was indicated for cases of relapse, treatment failure, or retreatment after loss to follow-up.
Blood Sampling Strategy
Blood samples (4 mL each) were collected on treatment days 10–14 to ensure stable INH concentrations. Patients had breakfast before sampling and took their medication for at least 2 hours after eating. Each patient provided four blood samples at predefined time points following two alternating schedules: (a) 1, 4, 6, and 24 hours or (b) 2, 5, 8, and 24 hours post-dose. The alternating schedules improved the accuracy of PopPK estimations.
Blood samples were collected in heparinized tubes and maintained on ice at approximately 4 °C until plasma separation, which was performed within 30 minutes of blood collection. The separated plasma was labeled and stored at −70 °C under light-protected conditions until analysis.
Quantification of Plasma INH and AcINH 17
Plasma concentrations of INH and its metabolite AcINH were determined using a validated high-performance liquid chromatography–tandem mass spectrometry (HPLC-MS/MS) method. The analysis was performed on a triple quadrupole LC-MS/MS system (Waters, USA) equipped with a Surveyor MS pump (Acquity H-class Quaternary Solvent Manager [QSM]) and an autosampler (Acquity H-class Flow-Through Needle [FTN]). The mass spectrometer used was a triple stage quadrupole (TSQ) Quantum Access Max. The autosampler tray temperature was maintained at 10 °C. The HPLC system was coupled to a quadrupole mass spectrometer for detection.
The lower limit of quantification (LLOQ) for INH and AcINH was 0.1 μg/mL. At the LLOQ level, the precision coefficient of variation (CV) for both INH and AcINH remained below 15.5%, while the accuracy was within 99.9%–100.6%, satisfying the requirements for bioanalytical method validation.
NAT2 Genotyping and Acetylator Phenotype Determination 18
NAT2 genotyping was performed using PCR-RFLP and Sanger sequencing, as previously reported in Vietnamese tuberculosis patients. Sequence data were analyzed by BLAST search in the GenBank database and BioEdit version 7.1.9 software. NAT2 alleles, including common wild-type and variant haplotypes, were assigned based on the observed sequence variants; diplotypes were then determined and translated into acetylator phenotypes according to allele combinations. Individuals carrying two rapid alleles were classified as rapid acetylators, those carrying one rapid and one slow allele as intermediate acetylators, and those carrying two slow alleles as slow acetylators. The genotyping approach and phenotype classification followed methods previously reported in Vietnamese tuberculosis patients.
Population Pharmacokinetic Modeling
PopPK analysis of INH and AcINH was performed using nonlinear mixed-effects modeling in Monolix 2021R1 (Lixoft, France). A simultaneous parent–metabolite approach was used. For INH, one- and two-compartment models with first-order absorption and elimination were evaluated, whereas AcINH was described by a one-compartment model with first-order elimination. AcINH formation was modeled using two distinct apparent first-order pathways: Kam, representing model-defined pre-systemic AcINH formation before parent INH reached the systemic circulation, combining intestinal-wall formation during absorption and hepatic first-pass formation during portal–hepatic passage; and Kpm, representing systemic parent-to-metabolite formation from central INH after systemic availability. Because only peripheral plasma INH and AcINH concentrations were available, the intestinal and hepatic components of pre-systemic formation could not be separately estimated. In the final model, V_AcINH/F was fixed equal to V1/F and was not estimated separately. Delayed absorption was explored using lag time, sequential zero-/first-order absorption, and transit-compartment models. IIV was assumed log-normal and included on key PK parameters.
Model selection and evaluation were guided by changes in the objective function value (OFV), information criteria (Akaike information criterion [AIC], Bayesian information criterion [BIC]), goodness-of-fit (GOF) plots, and simulation-based diagnostics, including visual predictive checks (VPCs) and normalized prediction distribution errors (NPDEs).
Residual Error Modeling
Several residual error models were explored during model development, including additive, proportional, combined additive–proportional, and exponential error structures. Additionally, the “log-transform both sides” (LTBS) approach with an exponential error model was evaluated to stabilize variance and improve model fit.
The general LTBS model structure is defined as:

Taking the natural logarithm of both sides yields:

Where:
Y: The observed dependent variable f (θ, η,Time): The model prediction θ: Fixed effects (population-level parameters) η: Random effects (IIV) ε: The residual error, assumed to be normally distributed.
For INH concentrations, a transformation involving the normal logit distribution and exponential error was applied to account for the bounded nature of concentration data. The residual error model was specified as:

For AcINH, a proportional error model was used, assuming the residuals followed a normal distribution:

Where:
Cobsp is the observed INH concentration (μg/mL); Cobsm is the observed AcINH concentration; Cpredp is the predicted INH concentration; Cpredm is the predicted AcINH concentration; a and b are the additive error coefficient and the proportional error coefficient, respectively.
This dual-model residual approach was selected based on model stability, residual diagnostics, and improvement in OFVs.
Covariates Modeling
After establishing the base model, potential covariates were selected based on published literature and patient data collection. A total of 12 covariates were included in the analysis: NAT2 acetylator phenotype (rapid, intermediate, or slow), TB type (new or retreatment), sex (male or female), INH formulation (single, dual, or triple component), smoking status, alcohol consumption, mining work experience and comorbidity (diabetes) as categorical variables, while age, Body mass index (BMI), body weight, and dose per body weight (all log-transformed) were considered continuous variables. A covariate-structured pharmacokinetic model was developed using the Conditional Sampling used for the stepwise approach based on the correlation (COSSAC) method, with covariate selection based on their correlation with model parameters at each step. COSSAC iterations alternate between forward selection and backward elimination of covariates, depending on the results of correlation tests. A covariate that reduced the OFV by more than 3.84 was considered statistically significant (p < .05; df = 1).
Model Evaluation
The selection of the base and full models was based on several validation criteria. Statistical indicators, including OFV, AIC, BIC, and BICc, were evaluated, with the model showing the lowest values being preferred. Visual checks included GOF plots to compare observed and predicted concentrations, prediction error (WRES) versus time, and predicted concentrations, VPC, and NPDE plots based on 1,000 simulated datasets.
Results
Patient Characteristics
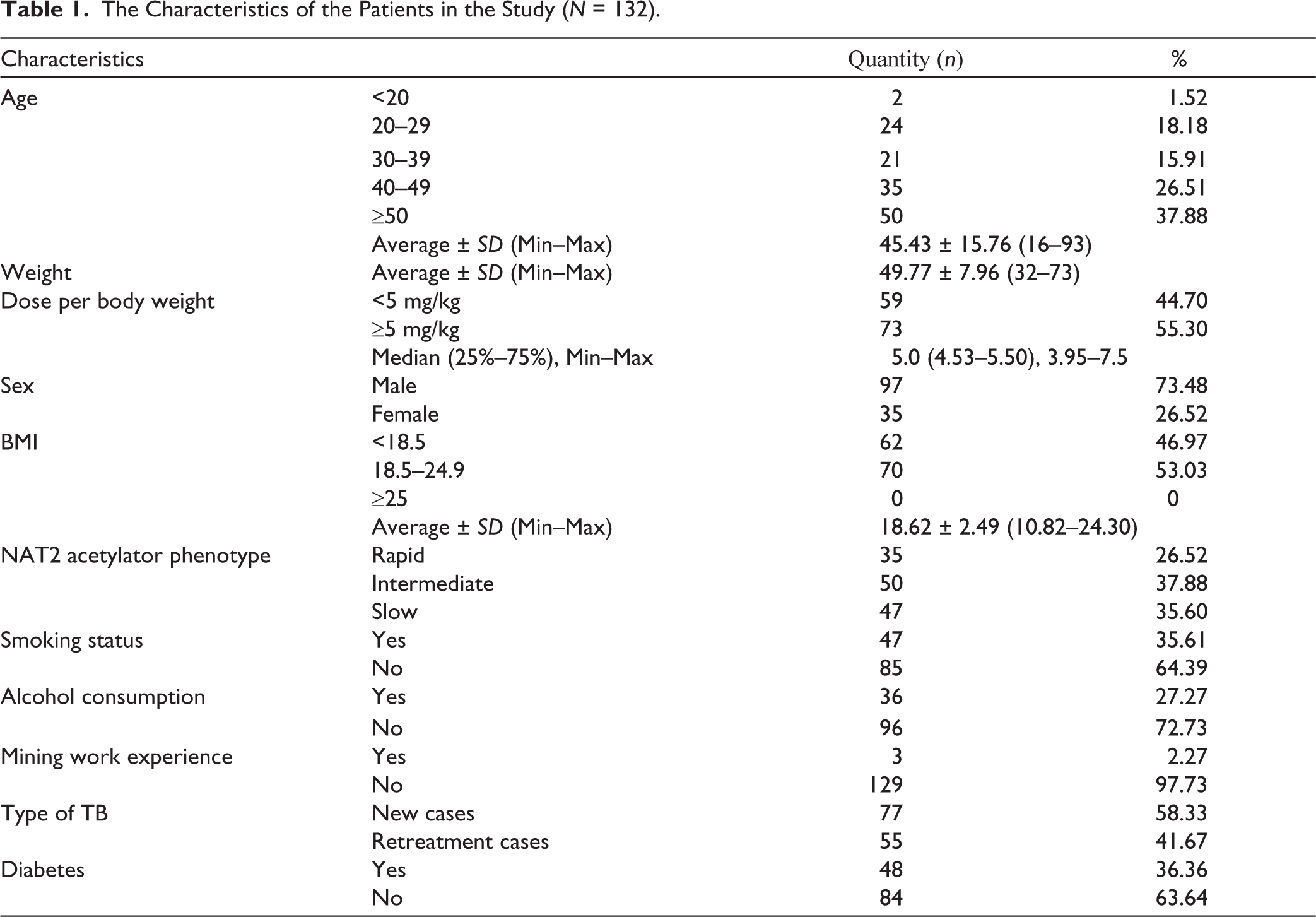
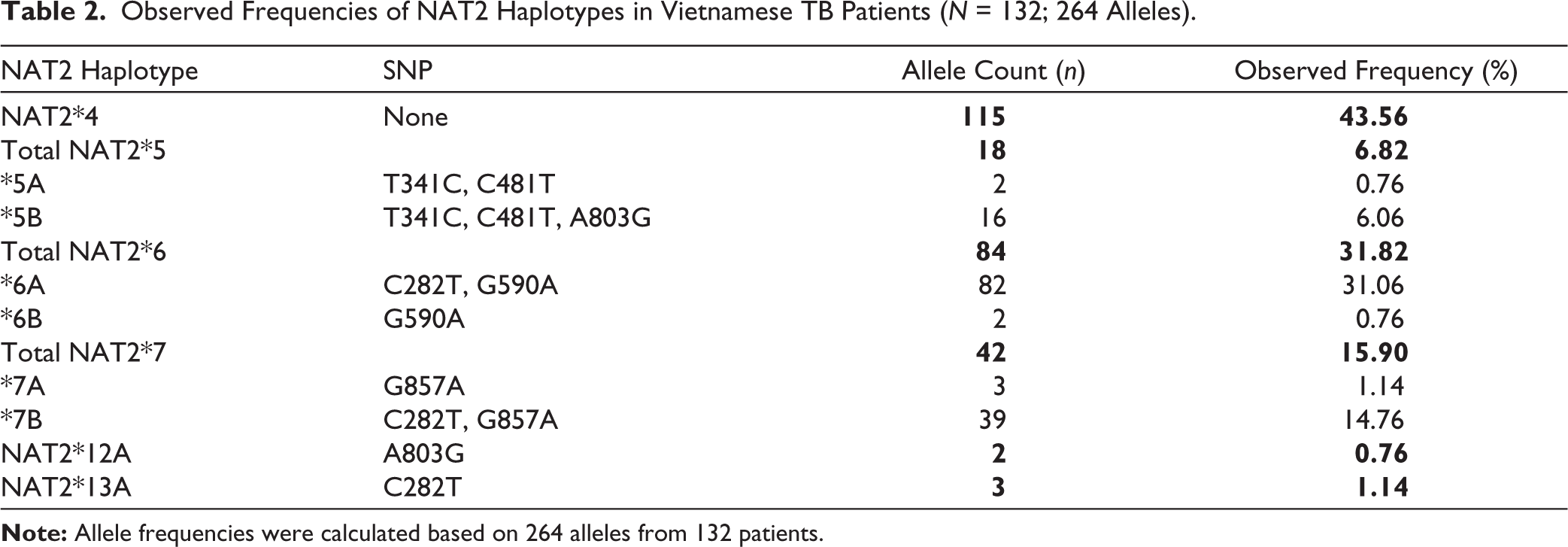
From December 2016 to April 2018, a total of 132 patients were recruited in the study (Table 1). Among them, the majority were newly diagnosed cases, accounting for 58.33%, while 36.36% had comorbid diabetes. The mean age and BMI of the population were 45.43 ± 15.76 years and 18.62 ± 2.49 kg/m 2 , respectively. The average body weight was 49.77 ± 7.96 kg, and the median dose per body weight was 5 mg/kg. Among the NAT2 acetylator phenotypes, the intermediate group was the most prevalent (37.88%), followed by the SAs (35.60%), whereas the RA group was the least common, comprising 26.52% of the population. Table 2 summarizes the nine NAT2 haplotypes identified in Vietnamese patients with TB. The most prevalent alleles were NAT2*4, NAT2*6A, and NAT2*7B, followed by NAT2*5B, NAT2*7A, and NAT2*13A. In addition, NAT2*5A, NAT2*6B, and NAT2*12A were each detected at frequencies below 1%.
The Characteristics of the Patients in the Study (N = 132).
Observed Frequencies of NAT2 Haplotypes in Vietnamese TB Patients (N = 132; 264 Alleles).
The mean administered dose of INH was 5.16 ± 0.83 mg/kg (range: 3.95–7.5 mg/kg). The majority of patients (99.24%) received INH as part of a three-drug fixed-dose combination (isoniazid [INH], rifampicin, and pyrazinamide), while only one patient was treated with the single-component formulation. A total of 528 steady-state plasma samples were collected, yielding 1,056 concentration observations for model development, comprising 528 INH and 528 AcINH concentrations.
Population Pharmacokinetic Model of INH and Its Metabolite AcINH
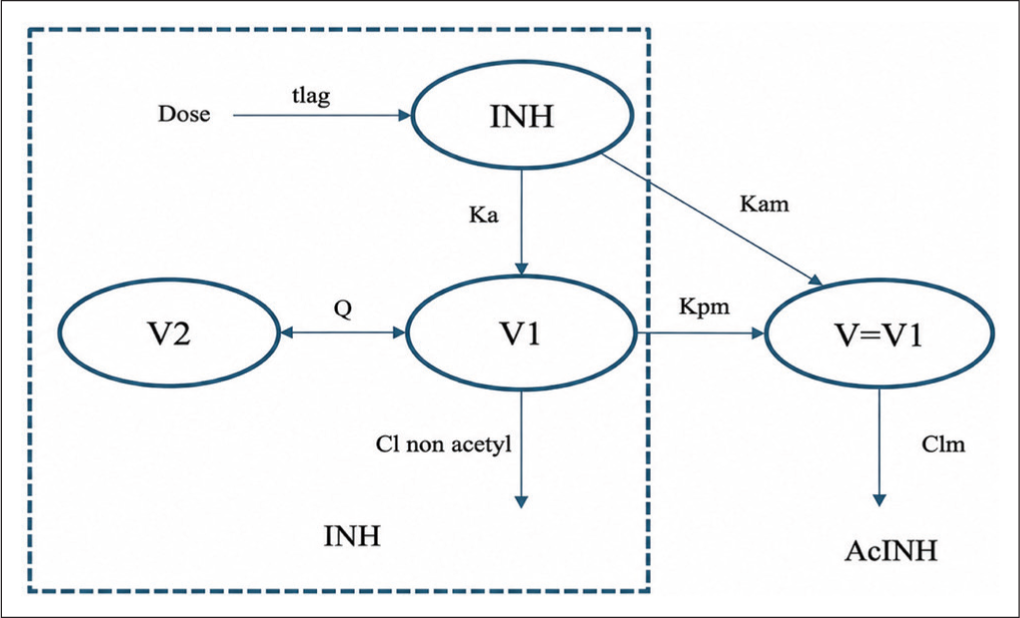
The concentrations of INH were best described by a two-compartment model with first-order elimination and first-order absorption with a lag time (tlag). For the metabolite AcINH, a one-compartment model with first-order elimination fitted the data. The structural model of INH and its metabolite AcINH was presented in Figure 1.
The model integrating covariate effects reduced the AIC value from 1,308 to 1,115.3 (ΔAIC = 192.7) compared to the basic model and improved the quality of visual plots evaluating the fit between observed and predicted concentrations by the model. The estimated results of the final model parameters are presented in Table 3.
The Estimated Population Parameters for INH and AcINH.
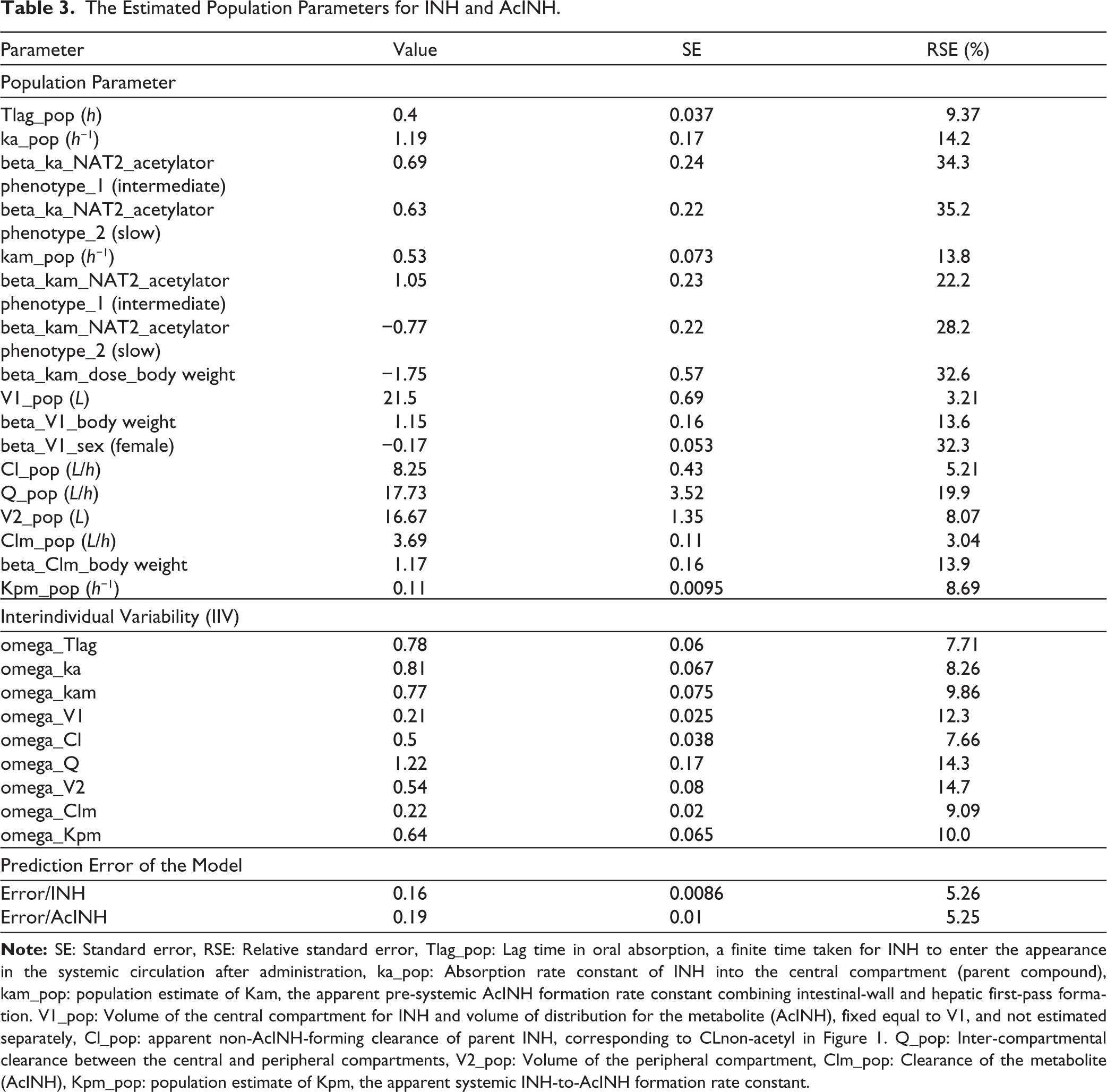
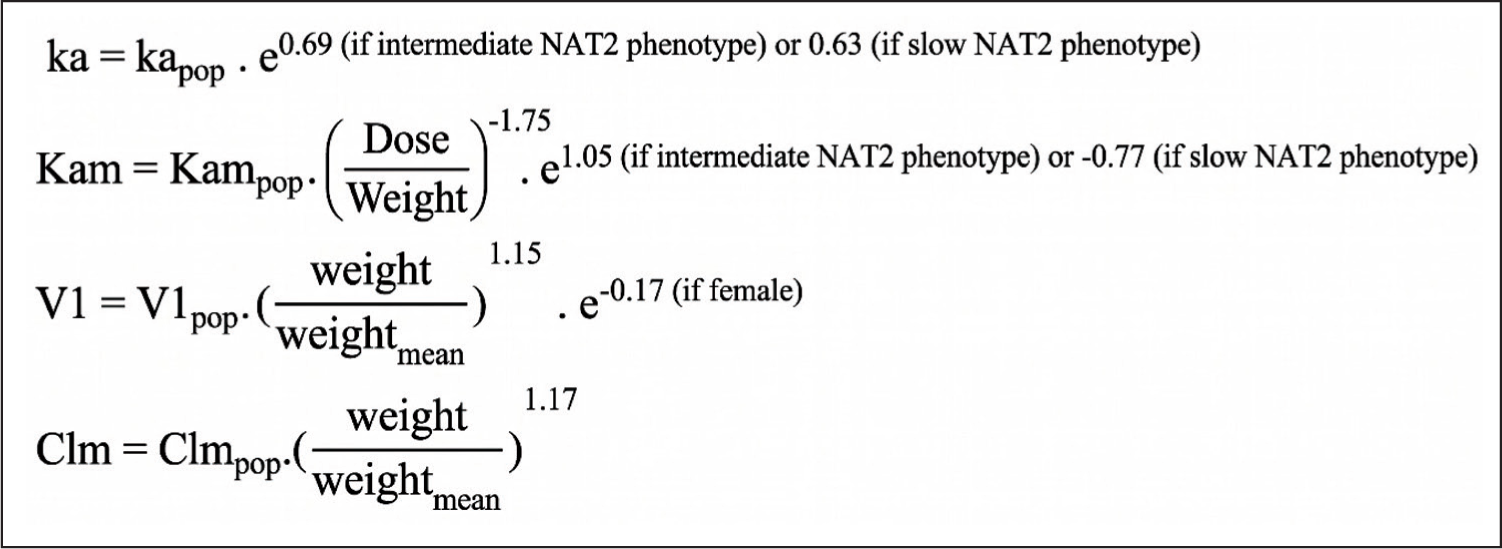
Model parameters were estimated with acceptable precision (relative standard errors [RSE] ≤ 35.2%, IIV ≤14.7%), confirming the robustness of the final model. NAT2 acetylator phenotype significantly influenced INH absorption (Ka) and metabolism (Kam). Dose normalized to body weight influenced Kam through a power-function relationship, body weight influenced V1 and Clm through allometric scaling, and sex was associated with V1 (Figure 2).
Covariate Formula for the Final Model.
Model Validation
The model was validated through charts showing the model’s fit. The correlation between observed concentration and predicted concentration GOF, plots of weighted residuals (WRES) versus time and predicted concentrations, the distribution of NPDE, and the VPC are presented below.
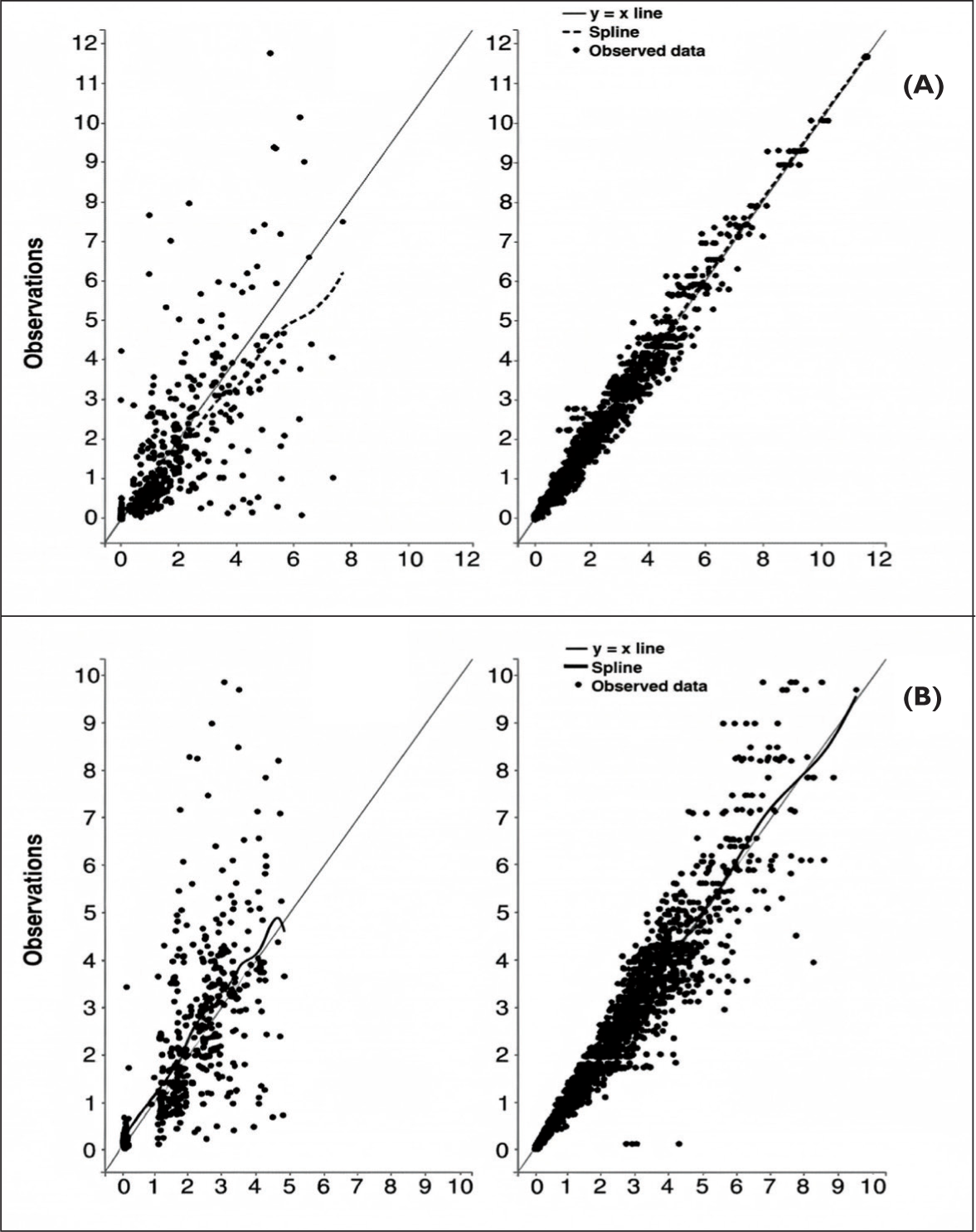
Figure 3 shows that individual parameters lead to more accurate predictions than population parameters. Compared to population-based predictions, the points on the chart for individual parameter predictions are closer to the line y = x, and the trend line (in yellow) closely follows the reference line y = x (in black).
Correlation Chart Between Observed Concentration and Predicted Concentration of INH (A) and AcINH (B).
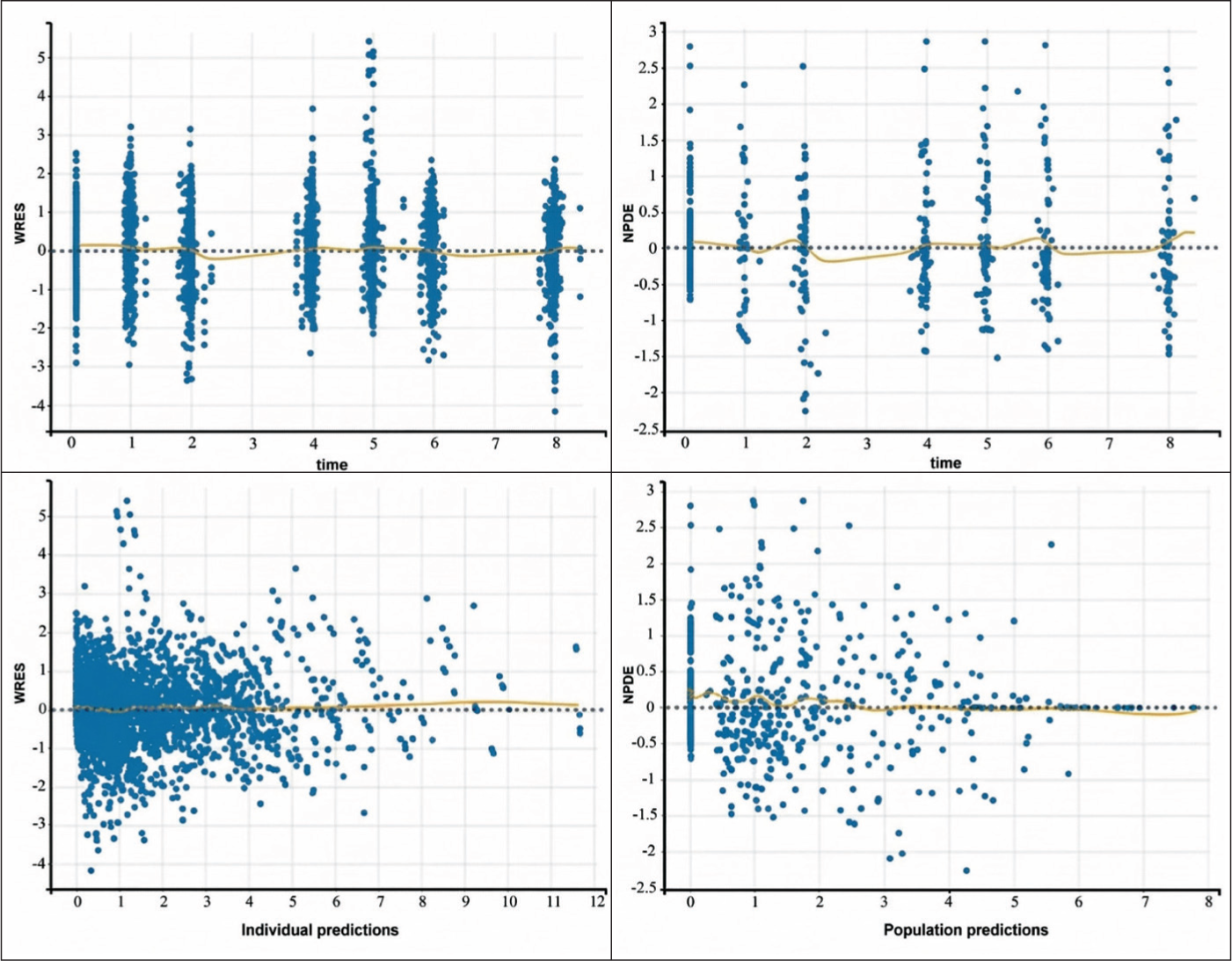
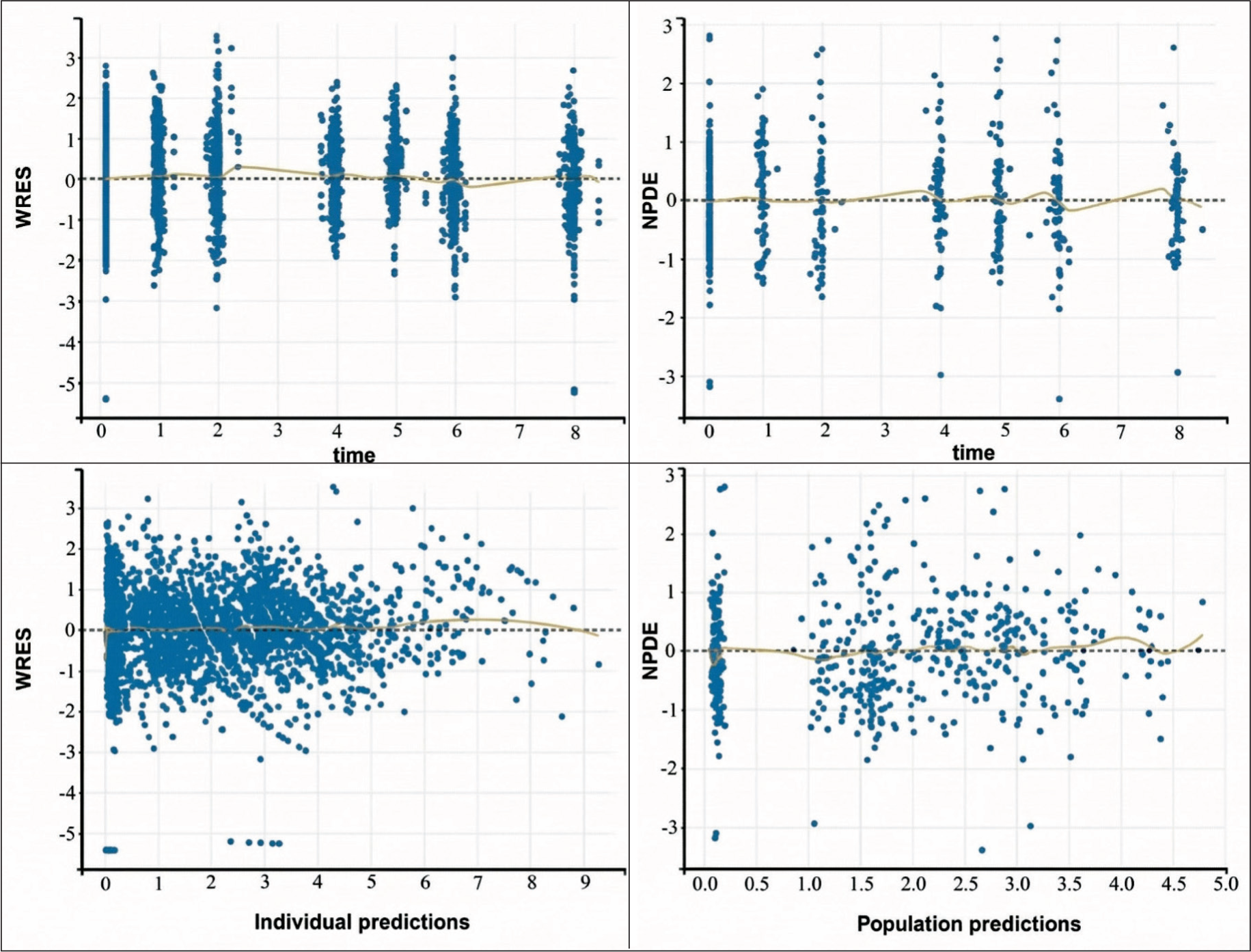
As shown in Figures 4 and 5, more than 95% of the prediction error values over time fall within the range of −2 SD and +2 SD and are evenly distributed, symmetrical around point 0, indicating no significant bias in the selected structural model. The prediction error values against predicted concentration are also within the range of −2 SD and +2 SD (over 95%) and are evenly distributed around point 0, suggesting no significant bias in the selected prediction error model for INH and its metabolite AcINH.
Prediction Error Chart Over Time and Predicted Concentration of INH.
Prediction Error Chart Over Time and Predicted Concentration of AcINH.
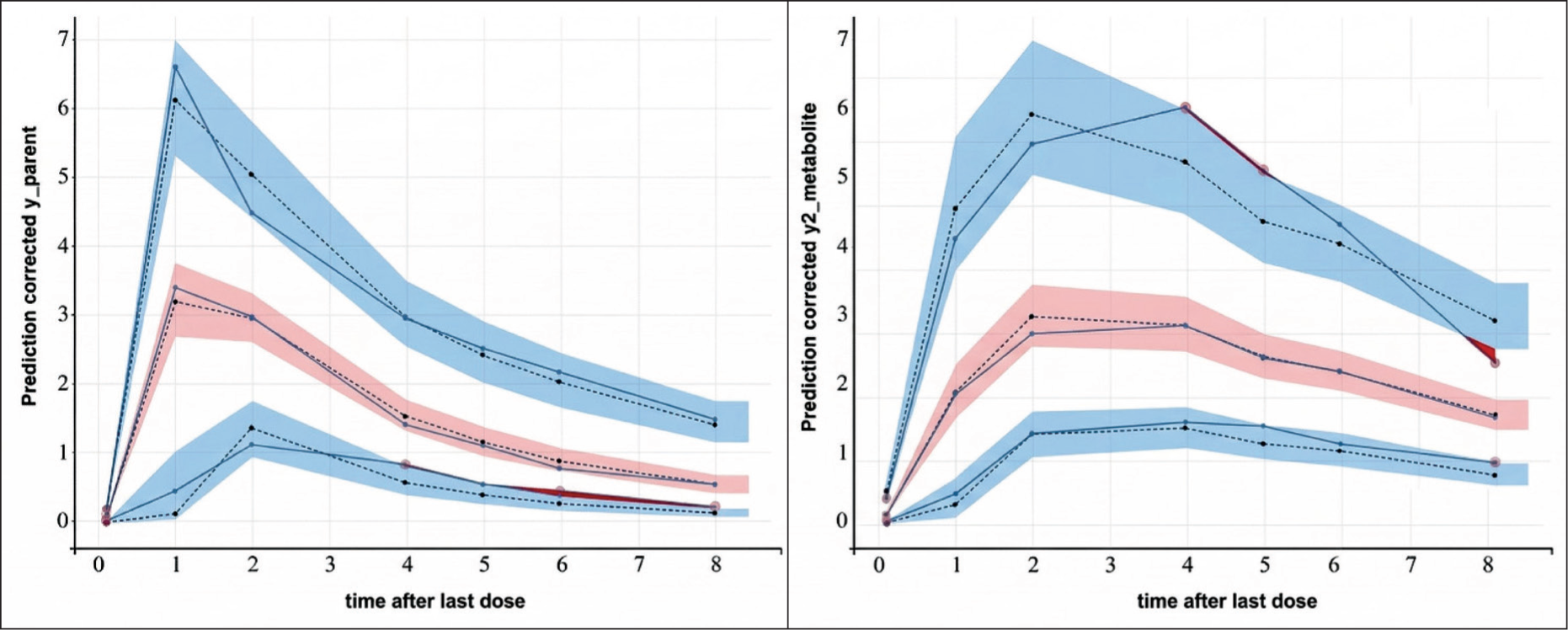
The VPC chart for INH and its metabolite, with 1,000 simulations, presented in Figure 6, indicates that the final model adequately describes the data for INH and its metabolite, AcINH. The line representing the observed concentration quartiles falls within the range (CI 90%) of the quartiles predicted by the model. Additionally, the line representing the quartiles of the observed data and the line representing the quartiles of the data predicted by the PopPK model tend to align closely.
Visual Predictive Check (VPC) Chart for INH and AcINH.
Discussion
Our study developed a PopPK model of INH and its primary metabolite AcINH, in Vietnamese TB patients, incorporating the influence of NAT2 acetylator phenotype. Given INH’s central role in first-line anti-TB therapy and the marked interindividual variability in its pharmacokinetics, largely attributed to NAT2 acetylator status, this model may provide a mechanistic framework to improve individualized dosing.
A simultaneous parent–metabolite model was used to characterize INH and AcINH. AcINH formation was described by two apparent pathways: Kam for pre-systemic formation through combined intestinal-wall/hepatic first-pass processes, and Kpm for systemic INH-to-AcINH formation from the central compartment. Because only peripheral plasma data were available, Kam should be interpreted as an apparent pre-systemic formation parameter rather than a purely hepatic first-pass parameter or total INH metabolism. This structure offers enhanced physiological relevance, particularly for assessing AcINH kinetics and its dependence on NAT2-mediated metabolism. Although AcINH has limited direct antimicrobial activity, its formation reflects acetylation capacity and may be indirectly associated with hepatotoxicity through downstream metabolites. Compared to simpler models, our approach provides a more nuanced understanding of genetic influences on drug disposition, consistent with prior genotype-informed PopPK studies.5,19
The final PopPK model consisted of a two-compartment structure for INH with first-order absorption and elimination, and a one-compartment model for AcINH. The two-compartment model for INH is consistent with findings from studies conducted in China, South Korea, and the Netherlands.20–22 In contrast, Chen et al. and Soedarsono et al. reported one-compartment models for INH, which may have been influenced by limited sampling designs or concerns about model overparameterization.14,19 In our study, a staggered sparse sampling design with alternating schedules provided broader temporal coverage of the concentration–time profile at the population level, enabling characterization of the absorption, distribution, and elimination phases of INH. Early sampling at 1 and 2 hours post-dose captured the absorption phase around the reported Tmax (approximately 1–2 hours), although dosing occurred under fed conditions. This may contribute to variability in the absorption process and potential delay in drug uptake, as food intake can slow gastric emptying and delay drug delivery to the primary absorption site in the small intestine. However, the limited number of samples per patient may reduce the precision of individual Tmax, Cmax, and Ka estimation. Nevertheless, this design remains appropriate for PopPK analysis and supports robust characterization of INH disposition.
The final PopPK model estimated apparent volumes of distribution for INH of 21.5 L (V1/F) and 16.67 L (V2/F), giving a total Vd/F of 38.17 L. These results are consistent with previous reports from Seng et al. (33.9 L) and Jing et al. (48.8 L), while Cho et al. described a larger peripheral distribution (53.3 L).13,20,21 In contrast, Soedarsono et al., using a one-compartment model, reported 40.5 L, likely reflecting structural simplification. 14 For AcINH, our one-compartment model estimated V/F = 21.5 L, similar to Chen et al. (12.4–25.7 L) and van Beek et al. (39.2 L), and lower than Seng et al. (97.4 L), possibly due to differences in model assumptions.13,19,22
Our total INH clearance (CL/F) was estimated at 8.25 L/h, which is lower than the value reported by Chen et al. (30.2 L/h), 19 but relatively comparable to those observed in SAs only (7.9–9.2 L/h).11,13,21 In our cohort, 35.6% of participants were classified as SAs, which likely contributed to the lower overall clearance. For AcINH, clearance was 3.69 L/h, within the range but lower than values reported by Seng et al., 13 Chen et al., 19 and van Beek et al., 22 reflecting population or design differences.
Covariate analysis revealed that log-transformed body weight significantly affected INH V1 and AcINH clearance, while female sex was associated with reduced V1. The NAT2 acetylator phenotype influenced both Ka and Kam. Intermediate and SAs exhibited increased Ka (β = 0.69 and 0.63, respectively), suggesting a more rapid systemic appearance of the parent drug compared to RAs. This phenomenon likely results from a reduced pre-systemic metabolic barrier in the intestinal wall and liver; with fewer active NAT2 enzymes to sequester the drug during its first-pass, a higher proportion enters the bloodstream at a faster rate. Interestingly, while both phenotypes showed faster absorption than the rapid group, the Ka for SAs was slightly lower than that for intermediates, potentially pointing to localized solubility limits or saturation of transport mechanisms when pre-systemic metabolism is minimal. In contrast, Kam followed a divergent path, increasing in intermediates (β = 1.05) but decreasing in slows (β = –0.77), highlighting that while systemic drug appearance is faster in both, the actual capacity for metabolite formation is severely impaired only in the SA group.
In addition, a power-function relationship of dose and body weight with Kam was identified in the model. The inverse association between dose/weight and Kam does not fully align with classical pharmacokinetic expectations, as rate constants are generally independent of dose and body size. This finding likely reflects the apparent nature of Kam in the model and the interplay between absorption and pre-systemic metabolism, rather than a direct physiological mechanism.
The NAT2 acetylator phenotype distribution in our cohort (35.6% slow, 37.88% intermediate, 26.52% rapid) was consistent with other Asian populations such as Singapore (33% slow, 45% intermediate, 21% rapid), 13 Indonesia (39.2% slow, 45.8% intermediate, 15% rapid), 14 and China (21.3% slow, 42.7% intermediate, 36% rapid), 20 but differed from Korea (11.7% slow, 46.7% intermediate, 40.5% rapid, 1.1% unknown) 21 and Rwanda (44% slow, 48% intermediate, 8% rapid). 11 This distribution aligned with clinical evidence that SAs had an increased risk of INH-induced hepatotoxicity, whereas RAs were more likely to experience subtherapeutic exposure and an associated risk of resistance.23–25 Prior studies demonstrated the benefit of NAT2-guided dosing, such as Azuma et al. and Sotsuka et al.7,26
While this study primarily focuses on the development of the PopPK model, its findings establish a critical link to clinical application. INH efficacy is widely recognized to be driven by the AUC0–24/MIC ratio, and its toxicity is closely associated with the accumulation of the AcINH metabolite.16,22 By accurately characterizing these exposures, our model serves as the essential foundational step for future PK/PD investigations. Although direct clinical outcomes, such as sputum conversion rates or hepatotoxicity scores, were not evaluated in this initial phase, the established population parameters allow for the prediction of target attainment in diverse patient scenarios.
Clinically, our model supports the implementation of individualized INH dosing strategies in Vietnam. By integrating the NAT2 acetylator phenotype and body weight into PopPK-based dose optimization, it provides a framework for therapeutic drug monitoring or Bayesian forecasting tools. Future prospective studies will leverage this model to directly correlate predicted exposures with clinical outcomes. Such MIPD has the potential to improve efficacy, reduce toxicity, and address regional variability in TB pharmacotherapy.
Conclusion
This study successfully developed a PopPK model of INH and AcINH that integrated NAT2 acetylator phenotype and individual covariates in Vietnamese TB patients. The model supported acetylator phenotype-guided dosing, improved understanding of interindividual variability, and held strong potential for clinical application in Vietnam and similar populations.
Footnotes
Authors’ Contribution
All authors made substantial contributions to conception and design, acquisition of data, or analysis, and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work. All the authors are eligible to be authors as per the International Committee of Medical Journal Editors’ requirements/guidelines.
Consent to Participate
Written informed consent was obtained from all patients or their legally authorized representatives before participation in the study.
Consent for Publication
Not applicable. This manuscript does not contain any identifiable individual patient data, images, or videos.
Data Availability Statement
All the data are available to the authors and shall be provided upon request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Ethics Committee in Biomedical Research of the School of Medicine and Pharmacy, Vietnam National University, Hanoi, under Approval Certificate No. 03/CN-HĐĐĐ dated 23 November 2016. The committee was registered as IRB-VN 01016 with the Ministry of Health and as IRB00010447 with the US Department of Health and Human Services–Office for Human Research Protections. The Committee was originally established under Decision No. 235/QĐ-KYD and continues to operate under valid IRB registrations. All study procedures complied with the Declaration of Helsinki and national regulations for biomedical research involving human subjects.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the Vietnam Ministry of Science and Technology and Newton Fund Vietnam (Grant Number HNQT/SPĐP/01.16).
Informed Consent
Written informed consent was obtained from all patients (or their legally authorized representatives) after full explanation of the study. All patient data were de-identified to ensure confidentiality.
Use of Artificial Intelligence-assisted Tools
The authors declare that artificial intelligence was used only for language polishing to improve grammar, sentence structure, clarity, and readability. It was not used to generate scientific content, data, or analyses. The authors reviewed and verified all content and take full responsibility for the final manuscript.