
Abstract
Abstract
Gynaecological problem makes up a sizable proportion of disease burden in women. Majority of these problems remain unaddressed as cultural and gender norms make women silent to report these problems. Undiagnosed and untreated gynaecological problems at young age may have physical and psychological consequences in later life. This article aims to understand the prevalence of gynaecological problems and its concomitants among young married women of rural West Bengal. We collected data on 1,107 young married women, aged 24 years or below, inhabiting the rural areas of three districts of West Bengal with at least one child of five years or below. A pretested structured schedule was used to collect data on socio-demographic variables and symptoms related to gynaecological problems and their management. Focus group discussions (FGDs) were conducted to get an in-depth understanding of the participants towards gynaecological problems and management. Around 41 per cent of women reported at least one of the gynaecological problems. Excessive vaginal discharge with bad odour, pain or burning sensation while passing urine, itching at vagina, lower abdominal pain, menstrual irregularities and painful menstruation were the most reported problems. Only 22 per cent of participants sought medical advice. FGDs reveal that there is a variation among the participants regarding the perception and awareness of gynaecological problems. Sexual activity, early marriage and menstrual hygiene were perceived to be the causes of gynaecological problems. The local healers were consulted at the initial stage of the problem; qualified medical practitioners were consulted when the problem persisted. We conclude from this study that socio-cultural factors remain the primary reason behind the high prevalence of gynaecological problem among the study participants.
Keywords
Introduction
A healthy reproductive life is an indispensable component of the general health and well-being of women (United Nations Populations Fund, 2014). Reproductive health problems including gynaecological problems account for 21.9 per cent of the disability adjusted life years lost by women aged 15–45 years (Abraham et al., 2014, p. 230). Defined as structural and functional disorders of the reproductive tract unrelated to pregnancy, gynaecological problem comprises 4.5 per cent of the overall global disease burden (Wizeratne & Fiander, 2018, p. 237). A study from five different states of India reveals the percentage of women reporting one or more gynaecological problems ranging from 55 per cent to as high as 84 per cent (Koenig, Jejeebhoy, Singh, & Sridhar, 1998, p. 86).
Of the various types of gynaecological problems, menstrual disorder is the most prevalent one (Vanitha, Edward, Varadharajan, & Muthuthandavan, 2017, p. 270). National Family and Health Survey-2 (NFHS-2) data documents that among all currently married women, the highest reported gynaecological problems include vaginal discharge, followed by severe lower abdominal pain and itchy vagina (International Institute for Population Sciences [IIPS] & ORC MACRO, 2001). In the state of West Bengal, 17.4 per cent rural women suffer from symptoms related to reproductive tract infection (IIPS & ORC Macro, 2013).
In India, the types and the prevalence of gynaecological problem vary with age, education, religion, family structure, marital status and rural-urban residence (Abraham et al., 2014, p. 233; Brunda, Kalasker, & Kurre, 2018, p. 3391; Hiwarkar, Dhekale, & Gokhe, 2015, p. 424; Reshmi & Unisa, 2006, p. 53). For example, women with low educational level (Naga & Babu, 2018, p. 5), who live in rural areas (Ghosh, Saha, & Dasgupta, 2012, p. 21) and those who get married at an early age (Desai & Patel, 2011, p. 55) suffer more frequently from gynaecological problems.
The Government of India launched the Reproductive and Child Health (RCH) Programme in 1997 following the International Conference for Population and Development (ICPD; United Nations Populations Fund, 1995). The major thrust of RCH programme was on maternal and child health issues but other gynaecological problems remain overlooked. Gynaecological problems of young women, especially in case of married group are unique as they step into the reproductive phase of their life. Owing to the ‘culture of silence’ (Shastri & Ram, 2015, p. 2), these gynaecological morbid conditions are often ignored until the issue goes up to the extent which needs medical intervention (Reshmi & Unisa, 2006, p. 41). The burden of gynaecological issues becomes more pronounced for young women because of early childbirth, high parity, short birth spacing and lack of reproductive decision-making. Gynaecological disorders at an early stage in life can lead to later health and developmental problems (United Nations Population Information Network, 2002), even if they can face emotional distress, marital discord and social rejection (Sharma & Gupta, 2009, p. 62).
Under this circumstance, we aimed to study the prevalence of gynaecological problem and its concomitants and management among young married women living in rural West Bengal.
Materials and Methods
Study Area
The study was conducted among a group of the young married women inhabiting the rural areas of three districts, namely Murshidabad, Maldah and Birbhum of West Bengal. The selection of rural areas was made using multistage random sampling technique. At the first stage, two community development blocks (CDBs) were randomly selected from each district, followed by random selection of one gram panchayat (GP; village council) from each CDB and five villages from each GP. Finally, a total of 30 villages were selected from three districts.
Study Population
At the initial level, we identified women on the basis of inclusion criteria for this study (aged 24 years and below, married, have at least one child of five years or below). Local community health workers were recruited to identify these participants. We excluded pregnant and those women who were in lactating amenorrhea to ensure all participants to be menstruating at the time of interview. A total of 1,585 participants fulfilled the inclusion criteria of this study; 266 (16.78 per cent) did not volunteer to participate and 212 (13.37 per cent) were not available at the time of data collection. Finally, data were collected from 1,107 participants.
Data Types
Information on socio-demographic profile, reproductive history, gynaecological problem of the participants was collected using pretested schedule/questionnaire. We translated and back-translated each of the questionnaire items from English to Bengali and back to English to check the consistency. Qualitative information was also collected using focus group discussion (FGD) technique.
Socio-demographic Profile
Information on socio-demographic variables includes age at the time of interview (in years) of the participants and their husbands, educational status, family type, working status, occupational types and per capita monthly household expenditure of the participants (in Indian rupees).
Reproductive History
Data on reproductive history include the age at menarche, first delivery, number of pregnancy(or pregnancies) and number of reproductive wastages experienced by the participants (miscarriage, abortion and stillbirth) and on the practice of family planning.
Gynaecological Problems
Data on self-reported gynaecological disorders include problems of menstrual irregularities (amenorrhea, oligomenorrhea, hypomenorrhea, polymenorrhea, menorrhagia, metrorrhagia and dysmenorrhea), urinary problems (leakage of urine while coughing and sneezing, burning sensation at the time of urination and frequently urinate), vaginal problems (lower abdominal pain with vaginal discharge, itching and irritation at vagina, white coloured discharge from vagina with or without bad odour, sores on the genital area and some mass coming out of vagina), and other gynaecological issues (like inability to conceive) and its care during the last six months period from the date of survey.
Anthropometry
Height and weight of the study participants were taken using standard protocol (Lohman et al., 1988). These two anthropometric variables were used for estimating BMI (kg/m2).
Data Collection Techniques
We conducted this study during the period from September 2011 to April 2013. Same-sex interviewer (NB) conducted all the interviews in Bengali language, the vernacular language of the study participants. NB is familiar with the local language and expression and she has prior experience of collecting data on gynaecological problem. Nine FGDs (three in each district) were conducted to understand the perception of the study participants towards gynaecological problem, reasons they perceive for having such problems and the way they managed the problems. Each of the FGD sessions comprised at least five to six participants of age group (15–24 years). Each FGD lasted for 20–30 minutes.
We categorised per capita monthly household expenditure of the participants into three groups on the basis of their tertile distribution. Category 1: ₹214.00–₹833.00; Category 2: ₹833.10–₹1,125.00 and Category 3: ₹1,125.10–₹5,000.00. The ages at menarche and first delivery and chronological age of participants at the time of data collection were documented in completed years. Age at menarche was ascertained by asking the exact age. Some of the participants, who could not recall their age at menarche were probed by referring to certain memorable landmark events or some festivals around the time of onset of menarche.
Ethical Clearance
The study protocol was approved by the ‘Ethical Clearance Committee’, University of Calcutta. Prior to the collection of data, content and purpose of the study and the voluntary nature of their participation was explained to the study participants and verbal consent was taken from them.
Statistical Analysis
Data were analysed using the software Statistical Package for Social Sciences (SPSS, version 16.0). Descriptive statistics and bivariate analysis were applied to understand the trend in the socio-demographic variables and gynaecological problems. Multivariate analysis was to examine the likelihood of association between different socio-demographic variables and gynaecological problems. For predicting the occurrence of gynaecological problem, the following independent variables were considered: age of the participants (below 20 years and above), religious affiliation (Hindu and Muslim), type of family (joint, extended and nuclear), education level (in completed years), working status (working and non-working), tertile distribution of category of per capita monthly household expenditure, age at menarche, age at marriage, parity (≥ 2 and ≤ 3), number of reproductive wastage (miscarriage, abortion and stillbirth), use of oral contraceptive pills, condoms, sterilisation(user and non-user) and BMI.
A minimum p-value of ≤ 0.05 was considered as statistically significant for all inferential statistics.
Results
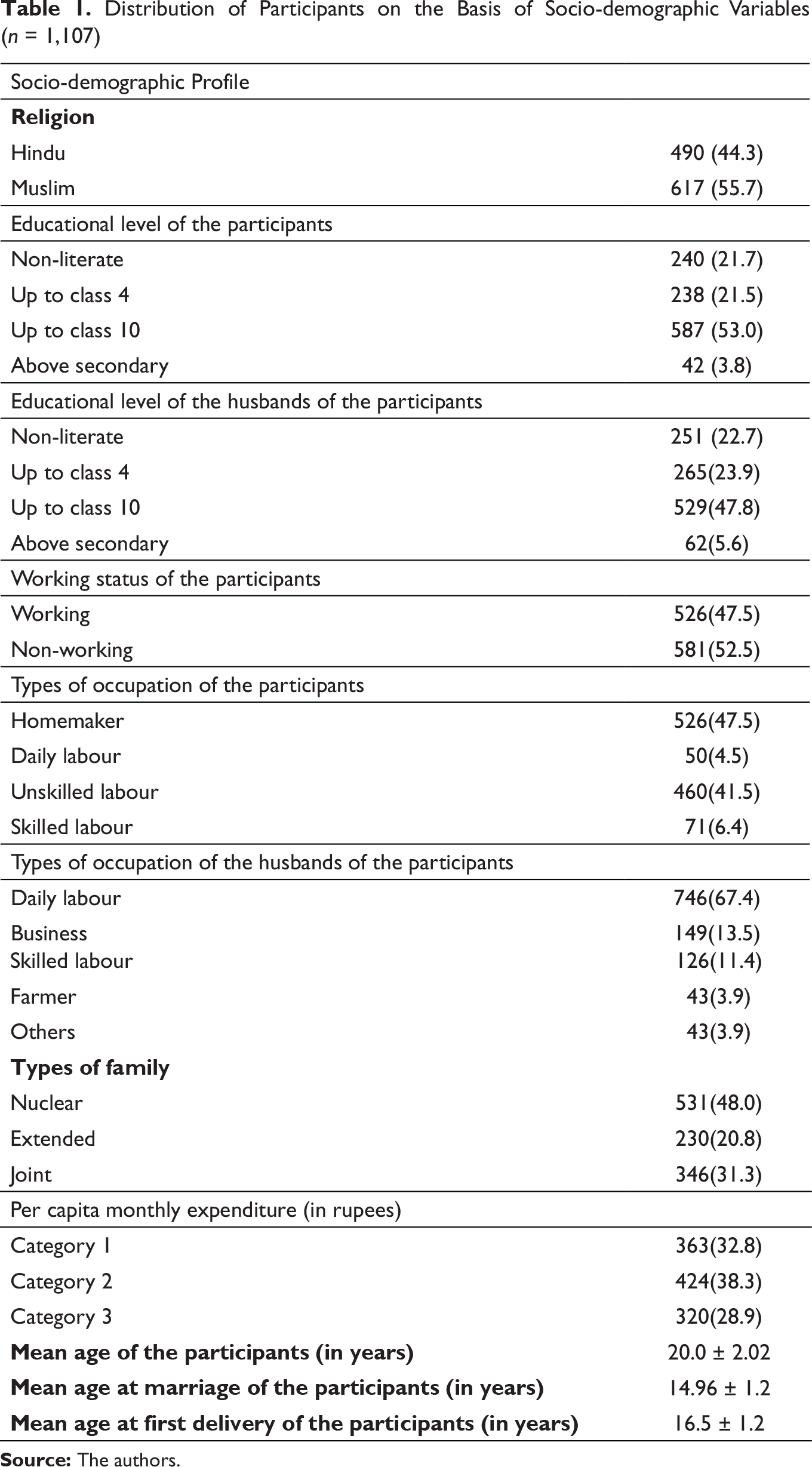
Table 1 describes the majority of the participants belonged to Muslim community, most of the participants and their husbands attained education up to secondary level. The working participants were mainly unskilled labours serving in bidi (a type of cheap cigarette made of unprocessed tobacco wrapped in leaves) factory (52.5 per cent) and their husbands worked as a daily labour in the agricultural field or in small scale industries. Most of the participants belonged to nuclear family (48.0 per cent) and fell under the second tertile of per capita monthly expenditure. The median age of the participants was 20.0 years, and majority got married around 15 years and delivered their first child approximately within a year after marriage.
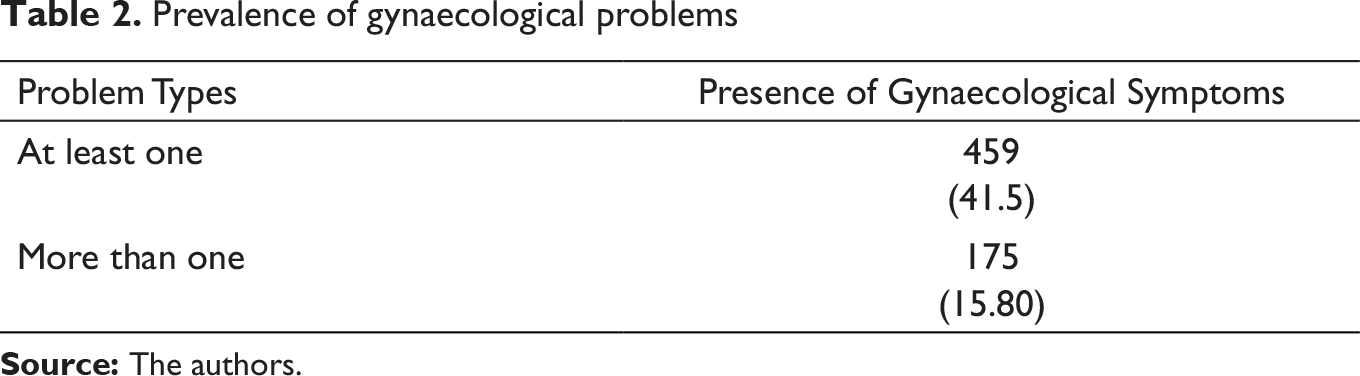
Table 2 shows that about 40 per cent of the participants reported at least one of the gynaecological problems and 15.8 per cent have experienced more than one type of gynaecological problems.
Distribution of Participants on the Basis of Socio-demographic Variables (n = 1,107)
Prevalence of gynaecological problems
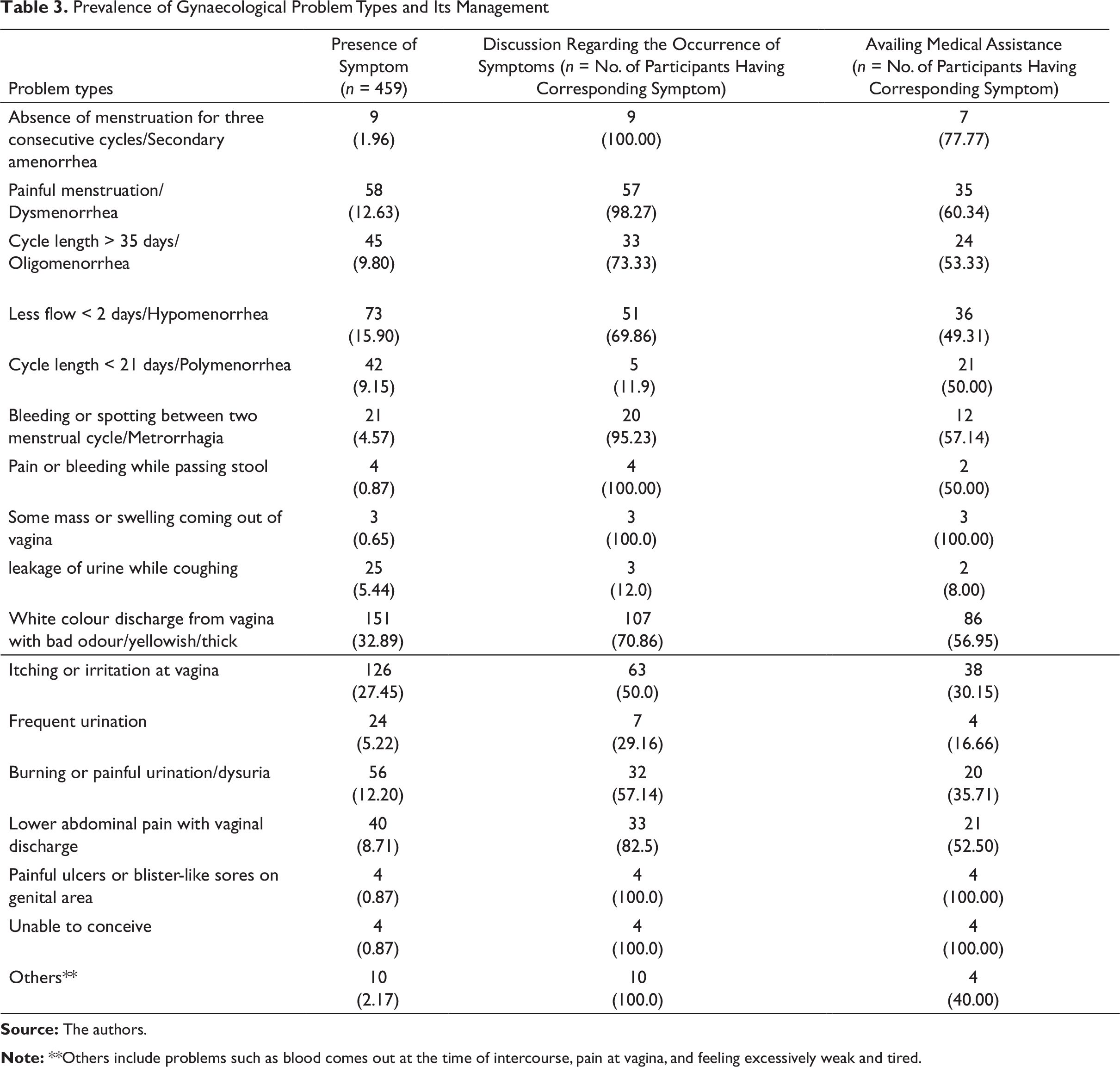
Only 22 per cent of these women sought medical consultation. In case of different menstrual problems such as polymenorrhea, hypomenorrhea, oligomenorrhea, menorrhagia, metrorrhagia, the participants visited medical practitioners for intervention (60 per cent, 31.50 per cent, 35.55 per cent, 60 per cent and 42.85 per cent, respectively). The trend is similar for problems such as some mass or swelling coming out of vagina, painful ulcers or blister-like sores on genital area and infertility (100.0 per cent). The participants mostly visited local healers (quacks, homeopath practitioners and ayurvedic doctors) for managing problems such as dysmenorrhea, white discharge from vagina with bad odour, itching or irritation at vagina and burning sensation while passing urine (36.36 per cent, 43.04 per cent, 19.84 per cent and 25 per cent, respectively). In most of the cases, the husbands of the participants were the sole or major decision-makers for undergoing any medical check-up.
Prevalence of Gynaecological Problem Types and Its Management
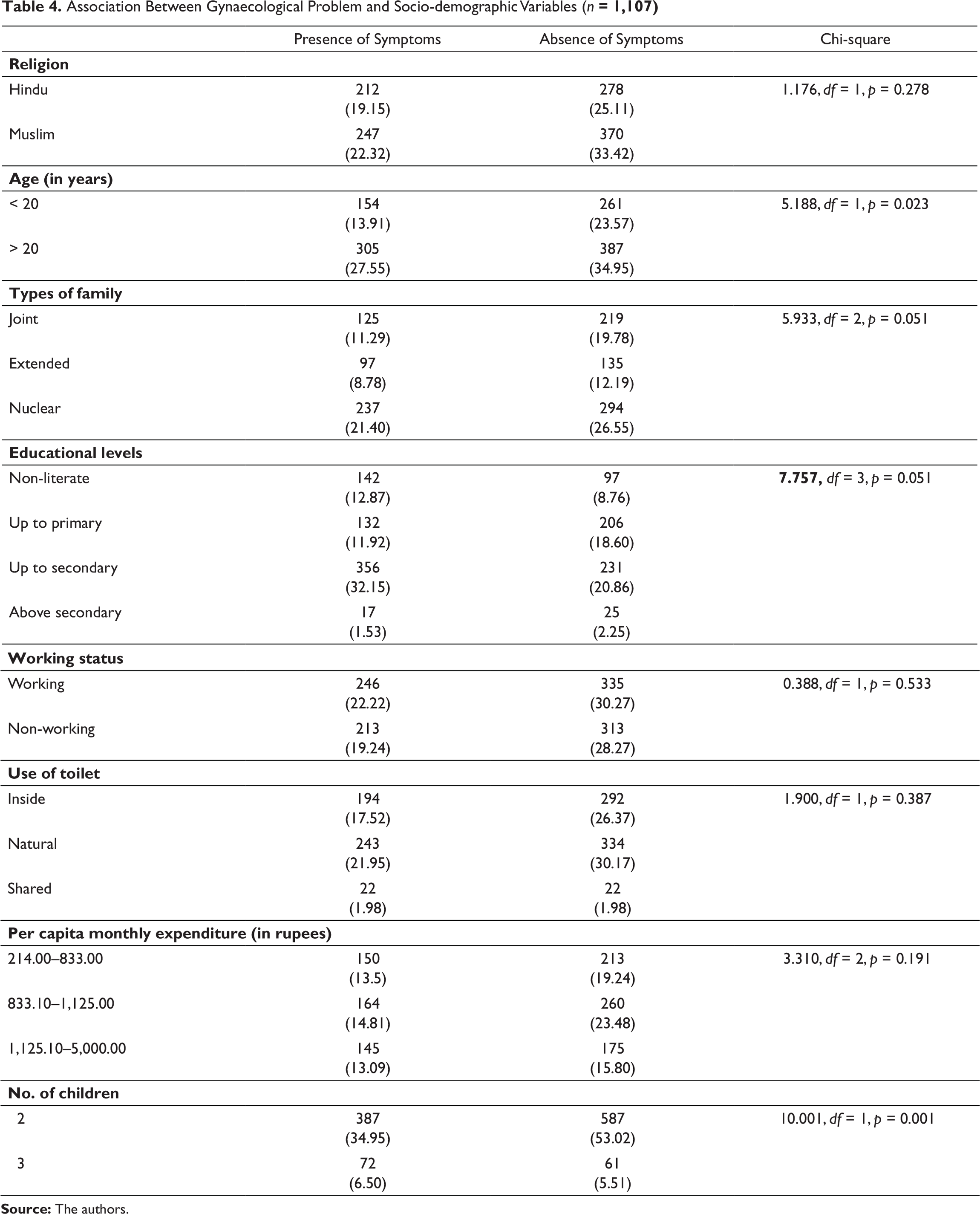
Association Between Gynaecological Problem and Socio-demographic Variables (n = 1,107)
Association of Any Gynaecological Problems with Socio-demographic Variables: Multivariate Analysis
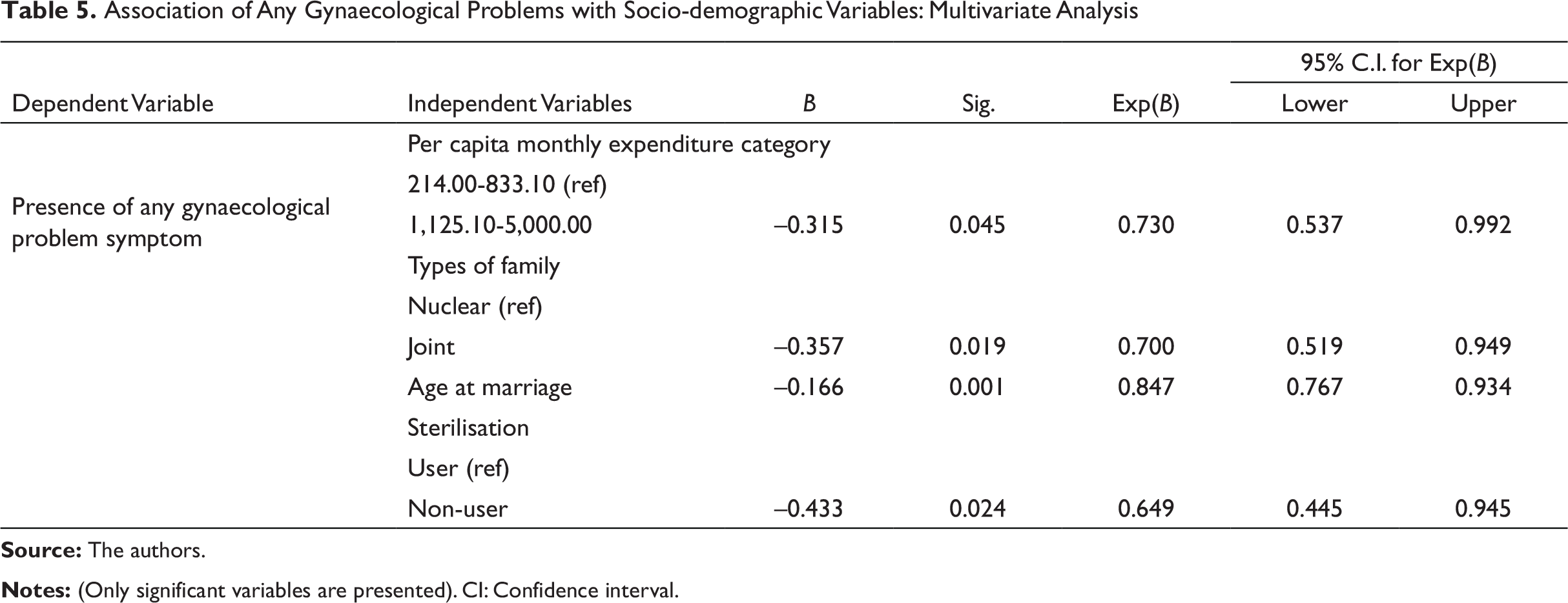
Table 5 shows that the likelihood of suffering from any gynaecological problem was more among the participants who belonged to the first tertile of monthly expenditure category (p < 0.045). Participants who lived in joint type of family were less likely to have any type of gynaecological problem than those who lived in nuclear family (p < 0.019). Early age at marriage increases the chance of suffering from gynaecological problem (p < 0.001). Participants who had undergone sterilisation have more chance to have gynaecological problems (p < 0.024).
Analysis of Focus Group Discussions
FGDs provided an insight into the participants’ perception of gynaecological problems and its causes as well as their treatment pattern.
Perception of Gynaecological Problems
Most of the participants termed or interpreted gynaecological problems as meyeli rog (ailment of females).
For example, a high school-educated young married woman told:
Gynaecological problems are women perceived. These diseases are known as ‘meyeli rog’ or ‘stree rog’.
As menstruation is unique to women so they often consider the menstrual problems as meyeli rog. For example, one young lady with primary level of education said:
Menstrual problems are the only ‘meyeli rog’
Some participants also perceived problems related to female sex organs as gynaecological problems.
For example, one illiterate woman said:
Any disease related to vagina is a gynaecological disease. Since vagina is a weak organ, it remains susceptible to disease.
Some of the participants were confused with the term ‘gynaecological diseases’ with ‘sexually transmitted diseases’. Many of these participants said that women whose husbands have multiple sex partners are prone to gynaecological problems. For example, one woman with primary education said:
I know a woman in a neighbouring village, whose husband regularly visits prostitutes, she has severe gynaecological problems.
There is a variation among the participants regarding the awareness towards gynaecological problems. Some participants thought that these types of gynaecological problems are different from other health issues and are less serious but others do not.
For example, an illiterate mother with two children said:
Menstrual health is a perpetual issue of every woman. But we generally ignore, until it becomes bothersome.
However, one literate mother with two children said:
Menstruation leads to childbirth and affects other health issues. So, women should address the menstrual health issues.
Another high school-educated participant said:
Problems such as irregular menstrual bleeding and excessive bleeding are serious health issues and should be treated properly as early as possible. Otherwise, it becomes a critical health problem for women.
Perceived Causes of Gynaecological Problem
While explaining about the causes of gynaecological problems, the participants expressed two major reasons. Sexual intercourse is perceived to increase susceptibility towards gynaecological problems. Early marriage initiates sexual activity and enhances the chance of having gynaecological problems.
For example, one participant aged 22 years, mother of three children said:
Early marriage means early entry into sexual life. Frequent sexual intercourse at tender age makes the vagina very weak for which young girls are affected with gynaecological problems.
Contradicting this view in the same group discussion another participant aged 20 years opined:
An unmarried girl also may have menstrual problems or problems related to passing of urine. The main reason is the use of unclean or open toilet or not cleaning the vagina properly after passing urine.
Another woman of 20 years added the point:
Bathing in a community pond spreads the problems such as vaginal discharge and vaginal itching.
Therefore, hygienic behaviour was considered to be another concomitant of gynaecological problems. Sources of water for cleaning private parts were thought to be responsible for poor hygiene.
Treatment Seeking Behaviour
In course of FGD, women reported that at the first level, they discuss their problems with their husbands, mothers and mothers-in-law regarding the management of gynaecological health issues. Decision on choosing health-seeking behaviour depends on the severity of the problem.
For example, a participant who received education up to junior high school and mother of two children told:
Until the problem becomes serious, we avoid doctors.
Some participants expressed that they always remain preoccupied with their household work and hardly find time to show concern about the gynaecological health issues.
For example, a young woman who was working as an unskilled labour in bidi industry with three children said:
I have to do all my household chores. I have to look after my children. So, I hardly find time to show concern about my gynaecological health issues.
In general, it appeared that women’s health is ignored. The only health issue arising from pregnancy is addressed.
For example, one young mother with three children told:
Women’s health issue becomes a concern during the period of conception to childbirth. The health centres can only cater to the management of pregnancy.
It is interesting that postpartum health issues are not a serious health concern to the participants.
In some cases, homemade remedies have been applied. For example, one working woman with high school education told:
I take batasa (a product made from jaggery) and fennel seeds soaked in water in the morning when I suffer from vaginal discharge.
To avoid menstrual pain, they prefer hot water compress. A non-working woman with primary school education said:
I pour hot water in a bottle and compress it on my lower abdomen to get rid of menstrual pain.
Self-medication is also practiced by the participants. Painkiller drugs, available across the counter, are generally used to pacify menstrual discomfort.
For example, a participant, who is a day labour said:
I bought painkiller from the compounder of a nearby medical store to control menstrual pain. Otherwise, it would be difficult for me to work in the field.
Many times, the choice of doctors or management depends on the financial condition. So, on many occasions, the participants resort to quacks for treatment.
For example, a working woman with three children told:
Where one should go for treatment depends upon the financial condition of the household at that time. So, in most of the time, professional health practitioners are avoided and quacks are preferred.
These quacks are always available in the village and their consultation fee is lower compared to the professional health providers.
For example, a non-working, high school-educated woman said:
We depend upon quacks for all our health issues. These problems are not different.
Another working woman with primary education told:
If the quack is unable to cure us, then we go to the private chambers.
Discussion
Our study shows high prevalence of gynaecological problem among the participants; commonest among these are abnormal vaginal discharge, itching or irritation at vagina and burning sensation while passing urine. Most of the participants reported menstrual problems such as less bleeding, painful menstruation, prolonged cycle length. Bivariate analysis shows socio-demographic variables have significant association with the occurrence of gynaecological problems. Multivariate analysis confirms lower age at marriage, participants living in nuclear family, and who are in Category 1 of per capita monthly household expenditure are more likely to suffer from gynaecological problem.
The symptoms of vaginitis are the most reported gynaecological problem among the study participants. Studies show that the symptoms of vaginitis are likely to be high who one enters into sexual union at an early age, belongs to poor economic status, and who do not take proper genital hygienic care (Shah et al., 2019, p. 155; Singh & Singh, 2018, p. 1.7; Verstraelen, Verhelst, Vaneechoutte, & Temmerman, 2010, p. 2). In the present study, women who belonged to lower category of per capita monthly expenditure were more likely to suffer from gynaecological problems. In the Indian context, early age at marriage marks the beginning of sexual activity at an early age (coitarche), making women more prone to gynaecological disorders (Abraham et al., 2014, p. 233; Brunda et al., 2018, p. 3391; Naga & Babu, 2018, p. 5). The present study also shows age at marriage as a significant predictor for the occurrence of gynaecological problem. The process of insertion of intrauterine devices (IUD) at the time of pelvic infections, female sterilisation and unsafe abortion also increase the risks of reproductive tract infection among married adolescent population of India as reported by several studies (Balamurugan & Bendigeri, 2012, p. 37; Desai & Patel, 2011, p. 58; Moshi, 2012, p. 426; Prusty & Unisa, 2013, p. 107; Reshmi & Unisa, 2006, p. 53). Multivariate analysis shows that the chance of occurrence of gynaecological problem increases among the sterilised participants. Most of the study participants got sterilised in the medical camps organised for mass sterilisation. Perhaps the hygienic conditions in these mass sterilisation camps were not adequate. This could be a plausible reason for high prevalence of gynaecological problems. Unawareness among the rural women about the health adversities of gynaecological problems, its cause and management, ‘culture of silence’ and limited healthcare facilities may trigger the load (Vanitha et al., 2017, p. 274).
Menstrual disorders are common presentation in late adolescence (Omidvar, Amiri, & Bakhtiari, 2018, p. 698). Dysmenorrhea and oligomenorrhea are found to be the commonest of all menstrual disorders among young women (Beevi, Manju, Bindhu, & Haran, 2017, p. 2995; Latha et al., 1997, p. 6). Most adolescents experiencing dysmenorrhea have primary dysmenorrhea, defined as painful menstruation in the absence of pelvic pathology (American College of Obstetricians and Gynecologists, 2018), whereas oligomenorrhea is common in adolescents due to fluctuating hormonal level. It can be caused due to the side effect of the use of hormonal birth control (Heitz, 2016). We found a large section of our study participants using oral contraceptive pills as birth control measure. This could be a reason behind high prevalence of oligomenorrhea among the participants.
Previous studies show that gynaecological problems are influenced by socio-cultural, demographic and behavioural factors (Babu, Radha, Nambisan, & Brahmanandan, 2016, p. 3430; Gopalakrishnan, Eashwar, Kumar, & Umadevi, 2019, p. 3607; Susila & Roy, 2013, p. 53). For example, the type of family is associated with the surge in gynaecological problem. Contrasting one study among young women in rural Bangladesh, our study found that living in nuclear family increases the susceptibility to gynaecological diseases (Rahman & Shahidullah, 2005, p. 8). Living in nuclear family set up increases the domestic workload of young women which often compromises with self-healthcare (Younis et al., 1993, p. 175). Unlike other studies based on NFHS-2 and NFHS-3, District Level Household Survey-3 (DLHS-3), Reproductive Child Health-2 (RCH-2), our study did not find any significant association between religion and occurrence of gynaecological problem (Desai & Patel, 2011 p. 58; Krishnakumar & Nair, 2007, p. 64; Prusty & Unisa, 2013, p. 107; Reshmi & Unisa, 2006, p. 53). Sharing the same geographical territory may not lead to marked differences in cultural practices. Significant association between parity of the participants with gynaecological problem has been revealed in several studies (Bhilwar, Lal, Sharma, Bhalla, & Kumar, 2015, p. 32; Mathew, Bengre, & Francis, 2017, p. 90; Sangeetha & Bendigeri, 2012, p. 2). Higher number of pregnancies increases the chance of getting gynaecological problems, especially reproductive tract infection. This could be due to the overgrowth of microorganisms that are normally present in the vagina during the pregnancy period because of hormonal changes (Sangeetha & Bendigeri, 2012, p. 2). In our study, the bivariate analysis shows significant association between parity and occurrence of any gynaecological problems.
The ‘culture of silence’ associated with gynaecological problem often hinders the participants to have an open discussion about their problems (Susila & Roy, 2013, p. 54). Some of the women feel shy and others find it a disgrace of self to the family and society at large. Even in FGDs, it has been observed that some women avoid disclosing their problems before others. The quantitative analysis also shows that they discussed their problems mainly with their husbands, mothers or mothers-in-law. FGDs also showed that the participants and their families often ignore the symptoms of gynaecological problems as these are perceived not so serious health issues like childbirth. ‘Self-limiting’ about the problem is the main reason for not seeking any healthcare (Hiwarkar et al., 2015, p. 426). Depending upon the severity and duration of distress, the participants decide what type of medical attention they would look for. Problems such as leakage of urine while coughing or sneezing, frequent urination, burning sensation while passing urine receive the least attention; homemade remedies are preferred at the initial stage for problems such as dysmenorrhoea or abnormal vaginal discharge, and this is a common practice among rural, low socio-economic societies (Hoa Binh, Gardner, & Elias, 2002, p. 163; Ilankoon, Goonewardena, Fernandopulle, & Perera, 2019, p. 12). Some also consult traditional healers, homeopath and ayurvedic doctors for managing gynaecological disorders as found in most of the rural societies (Das & Shah, 2008, p. 19; Rani & Bonu, 2003, p. 173; Singh, Prasad, Verma, & Pandey, n.d., p. 2). Added to it, the issue of poverty confines these women from undergoing medical check-ups from health professionals (Abraham et al., 2014, p. 234). Lack of decision-making among the young women remains a perpetual problem in the management of gynaecological health (Nayak & Varambally, 2017, p. 109). In our study, only 7 per cent women were able to decide on their own for seeking treatment for their gynaecological problems.
Limitations of the Study
The research work is based on the self-reported gynaecological problems and could not be confirmed using any clinical and/or diagnostic tests. ‘Culture of silence’ could have refrained some of the participants from actual reporting of the problems.
Conclusion
We conclude from this study that socio-cultural factors remain the primary reason behind the high prevalence of gynaecological problems among the study participants. Improvement in health infrastructure can only be useful in reducing the gynaecological problem provided socio-cultural issues are addressed. This can be only possible if social scientists, community leaders and voluntary health workers work together in addressing the gynaecological health issues of young married rural women.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.