
Abstract
The study aimed to understand the effect of primary infertility on the psychological well-being of women. In addition, the study has assessed the impact of socio-demographic variables, reproductive trajectories and lifestyle variables on psychological well-being independently and in light of their dynamic interaction among North Indian women. This study was conducted among 250 infertile women with primary infertility attending the Gynaecology OPD and 250 age-matched fertile women from Delhi. Pretested quantitative interview schedule and WHO-5 perceived well-being scale were used for data collection. The results depicted that infertile women were found to have higher prevalence of poor psychological well-being than fertile women. Of all the variables, education, duration of infertility, physical activity, exercise, sleep pattern and family structure were significantly associated with the psychological well-being of infertile women. Infertility is a major cause of the decline in psychological well-being in infertile women. In most hospitals and infertility clinics, women are treated for infertility, but their psychological well-being is often ignored. To improve the psychological well-being of women dealing with primary infertility, infertility education and awareness, physical activity and family counselling must be integrated into the infertility treatment.
Introduction
Primary infertility refers to couples who have not become pregnant after at least one year of having sex without using birth control methods (World Health Organization [WHO], 2018). Infertility affects approximately 9% of reproductive-aged couples worldwide (Boivin et al., 2007; Maroufizadeh, et al., 2019; Wasilewski, et al., 2020). Globally, primary infertility accounts for 2% of infertile women (Mascarenhas et al., 2012). In India, primary infertility prevalence is estimated to range from 3.9% to 16.8% (De et al., 2017). Infertility is a multidimensional stressor requiring many emotional and psychological adjustments (Greil, 1997). When these negative emotions persist for long periods and interfere with a person’s ability to function in daily life, their psychological well-being is compromised. Psychological well-being is defined as ‘the combination of feeling smart and functioning effectively’ (Huppert, 2009, p. 137). Psychological well-being at a most basic level is quite similar to other terms that refer to positive mental states, such as happiness or satisfaction. A positive mental state is associated with better health across various physical health outcomes. Infertility has a negative effect on couples’ psychological well-being and sexual relationships (Luk & Loke, 2015). It can cause anxiety, stress and depression and can affect the whole well-being of an individual, leaving a long-lasting impact (King, 2003; Lechner et al., 2007). Infertility affects both men and women reasonably equally (Schuiling & Likis, 2017; Nicola et al., 2019), despite the fact that in many societies, women are most often criticised when they do not get pregnant, resulting in mental health distress, stigma, discrimination, social exclusion and abandonment (Dattijo et al., 2016; Inhorn, 2003; Marshall & Raynor, 2014; Satheesan & Satyaranayana, 2018; Venkatesan, 2018). Women are mainly blamed for infertility (Bhat & Byatt, 2016), which is associated with lower quality of life, marital conflicts (Sarkar & Gupta, 2017) and more significant psychosocial consequences for women (Patel et al., 2018; Saleem et al., 2017). Generally, Indian couples are expected to conceive within the first year of marriage, and if this doesn’t happen, they face considerable social pressure and coercion (Roberts et al., 2012; Roberts & Montogomery, 2016; Satheesan & Satyaranayana, 2018), resulting in increased distress related to infertility (Patel et al., 2018). Studies on culture-specific infertility and the mental health consequences in India (Bharadwaj, 2016; Patel et al., 2016; Saleem et al., 2018) are lacking.
Therefore, the present study aims to understand the relationship between infertility and psychological well-being among North Indian women. The study aims to understand the effect of infertility, socio-demographic variables, reproductive trajectories and lifestyle variables on psychological well-being independently and in light of their dynamic interaction.
Material and Methods
The present research is a case-control study in which data was collected from 500 women, which included 250 fertile and 250 infertile individuals aged 22 to 35 years. Data collection for infertile women was done from the Gynaecology Outpatient Department (OPD) of the Lady Harding Medical College (LHMC) and Smt. Sucheta Kriplani Hospital, Delhi in North India. Inclusion criteria for recruitment of infertile and fertile women was married women in reproductive age and hailing from North India
(Delhi and National Capital Region, such as Haryana, Uttar Pradesh, Rajasthan, Punjab, etc.). Infertile women were selected from women seeking infertility treatment or given any infertility-related diagnosis in LHMC. One fertile age-matched woman was selected for each infertile woman who met the matching criteria and lived in a similar locality. Inclusion criteria for fertile women was successful pregnancies and having at least one child older than one year.
The ethical committee of the LHMC and the Department of Anthropology, University of Delhi, approved the work. Further, informed written consent was obtained from all the participants before data collection.
For collecting data from the infertile and fertile women, a non-probability consecutive sampling method was used. A pretested modified interview schedule was used, which included demographic variables (name, age, household composition, educational status, husband’s occupational status, social-economic status and family structure), reproductive profile (duration since marriage, age at menarche, disturbed menstruation and possible cause of infertility) and lifestyle variables (sleep pattern, their belief system, fast, physically active or not, and how often they do physical exercise). The factors used for this study were mostly based on the review of previous research. The variables selected are more concerned with the psychological effects of infertility than with the infertility itself (Katole & Saoji, 2019; Ogawa et al., 2011; Sohbati et al., 2021). The psychological tool used was WHO-5 perceived well-being scale pertaining to psychological well-being.
The WHO-5 is a five-item questionnaire assessing general functional and subjective and psychological well-being over the prior two weeks (Topp et al., 2015). The WHO-5 is a short and easy-to-use questionnaire with satisfactory reliability and validity that appears suitable for use as a screening test for depressive symptoms in infertile people (Bech et al., 1996). It was derived from the WHO (Ten) Well Being Index (Omani-Samani et al., 2019) and is used to measure psychological well-being.
The five positively worded items of WHO-5 are as follows:
I have felt cheerful and in good spirits. I have felt calm and relaxed. I have felt active and vigorous. I woke up feeling fresh and rested. My daily life has been filled with things that interest me.
Respondents rated these items on a six-point Likert scale from ‘0 is at no time’ to ‘5 is all of the time’. In a raw score, 0 is the absence of well-being and 25 is maximum well-being, which was used for the mean values. In the case of percentage, which is raw score × 4, 0 is the worst possible quality of life, less than 50 is poor well-being and 100 is the best quality (Omani-Samani et al., 2019). The percentage score was used for the distribution of variables with respect to psychological well-being.
Statistical Analysis
Descriptive statistics were used for quantitative variables and expressed as mean, standard deviation, frequencies and percentages. Pearson’s chi-square test was carried out for comparing categorical data. Crude odds ratio was used to analyse the risk factor analysis for poor psychological well-being. An independent t-test was used to determine whether there is a statistically significant difference between the mean scores of WHO-5 infertile and fertile women. Logistic regression analysis was performed to understand the association of different confounding variables with psychological well-being among infertile and fertile women. All statistical analyses were carried out using SPSS, IBM version 24, with a significance level of 0.05.
Results
A total of 500 women were interviewed during this study, among whom 250 were infertile and 250 were fertile. The mean age of infertile and fertile women was 27.104 years ± 3.74 years. A majority (44%) of women belonged to the 26—30 years of age group, followed by the age group 22—25 years (39.6%) and then by the 31—35 years age group (16.4%).
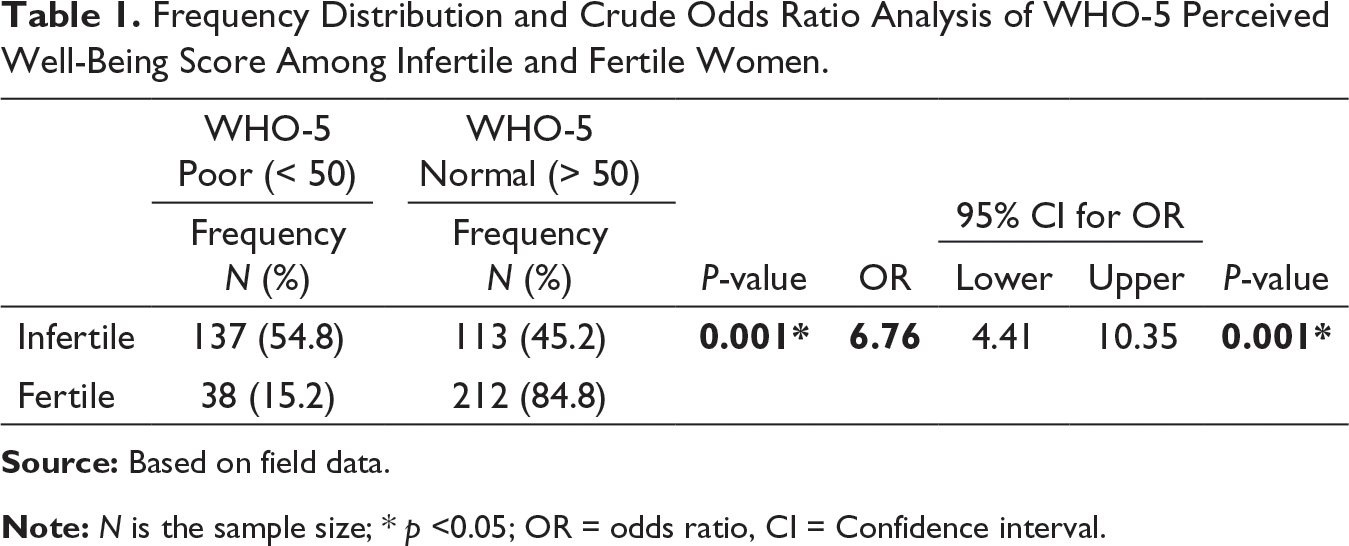
Frequency Distribution and Crude Odds Ratio Analysis of WHO-5 Perceived Well-Being Score Among Infertile and Fertile Women.
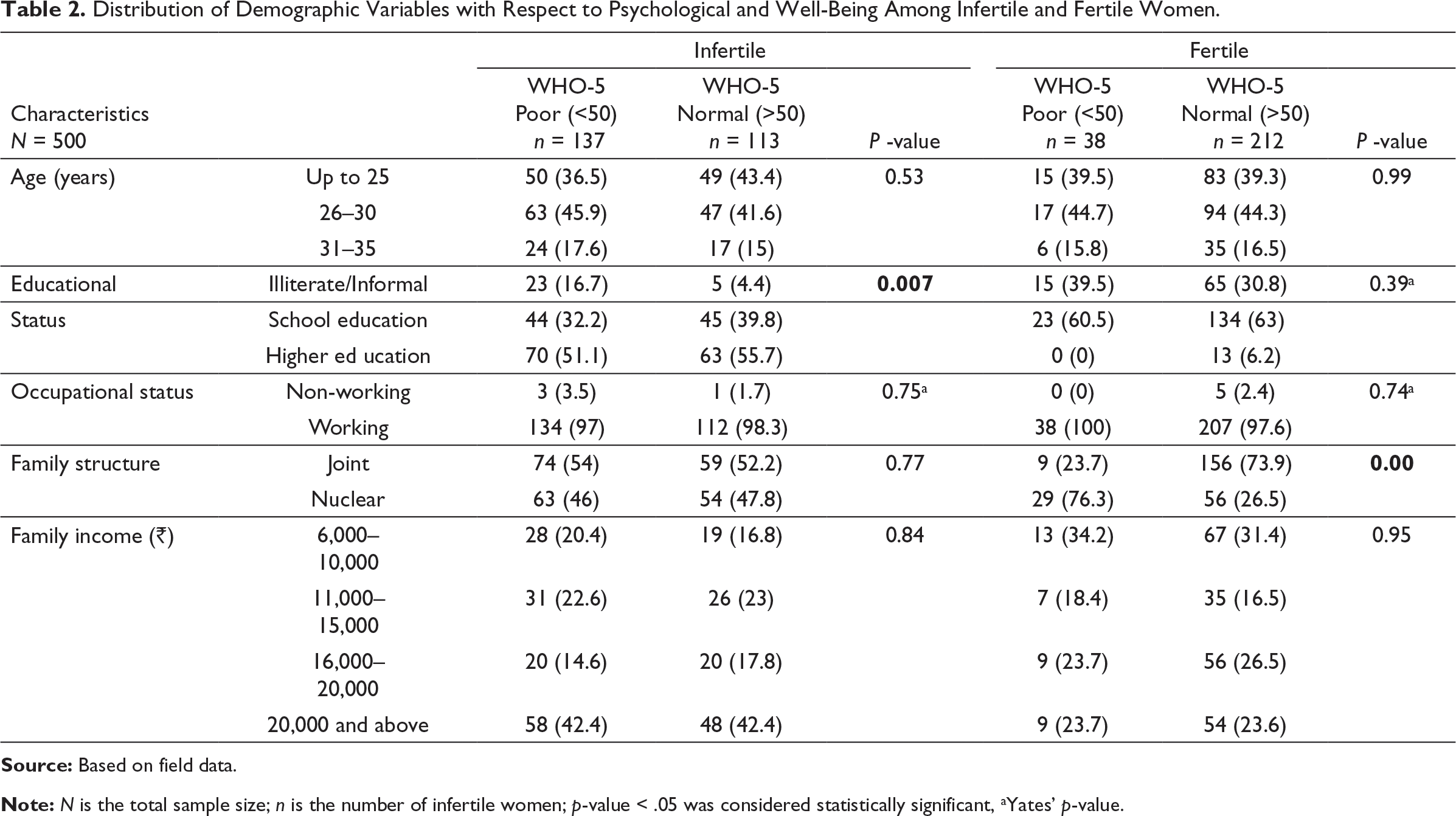
Distribution of Demographic Variables with Respect to Psychological and Well-Being Among Infertile and Fertile Women.
Distribution of Reproductive Profile Trajectories with Respect to Psychological Well-Being Among Infertile and Fertile Women.
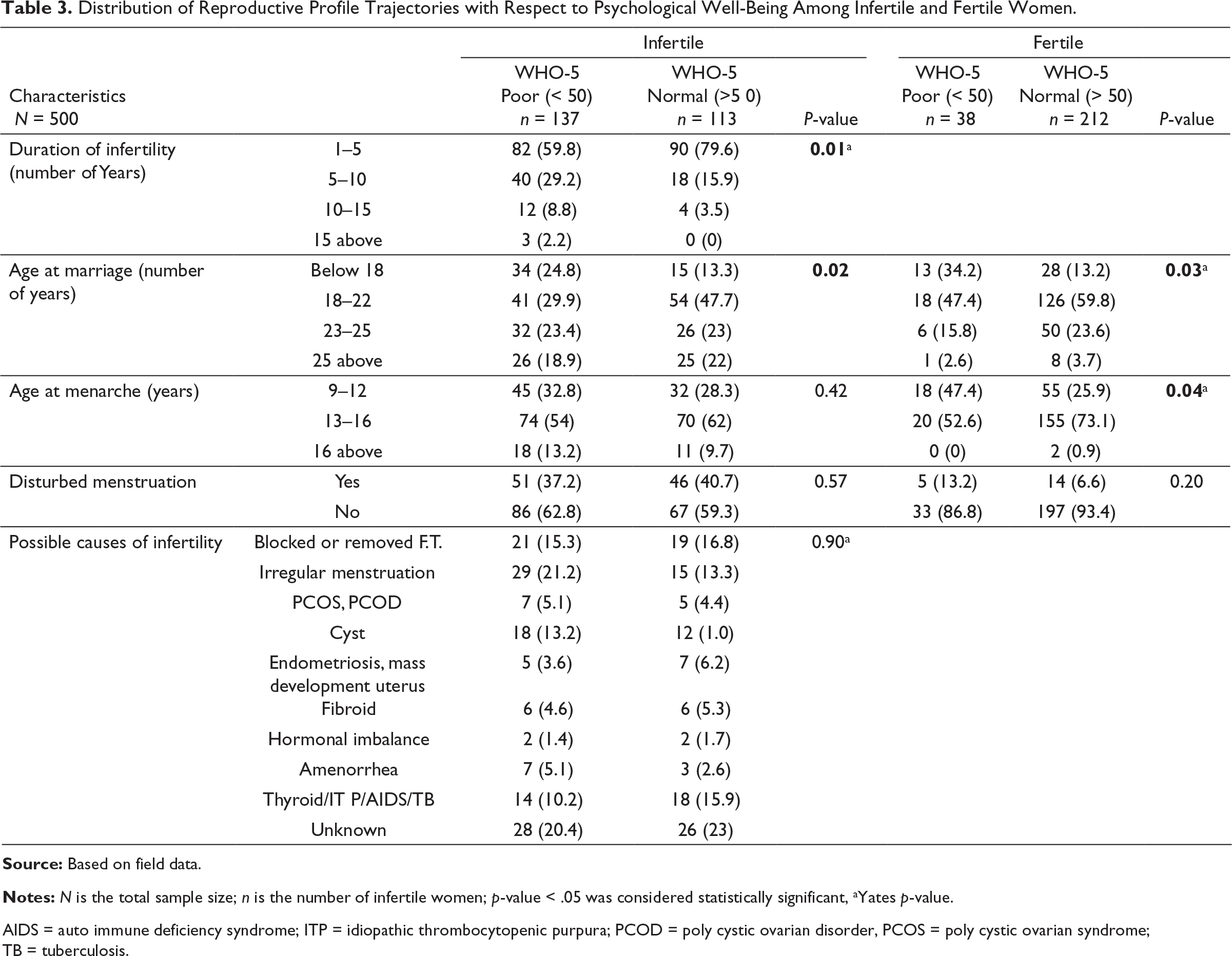
AIDS = auto immune deficiency syndrome; ITP = idiopathic thrombocytopenic purpura; PCOD = poly cystic ovarian disorder, PCOS = poly cystic ovarian syndrome; TB = tuberculosis.
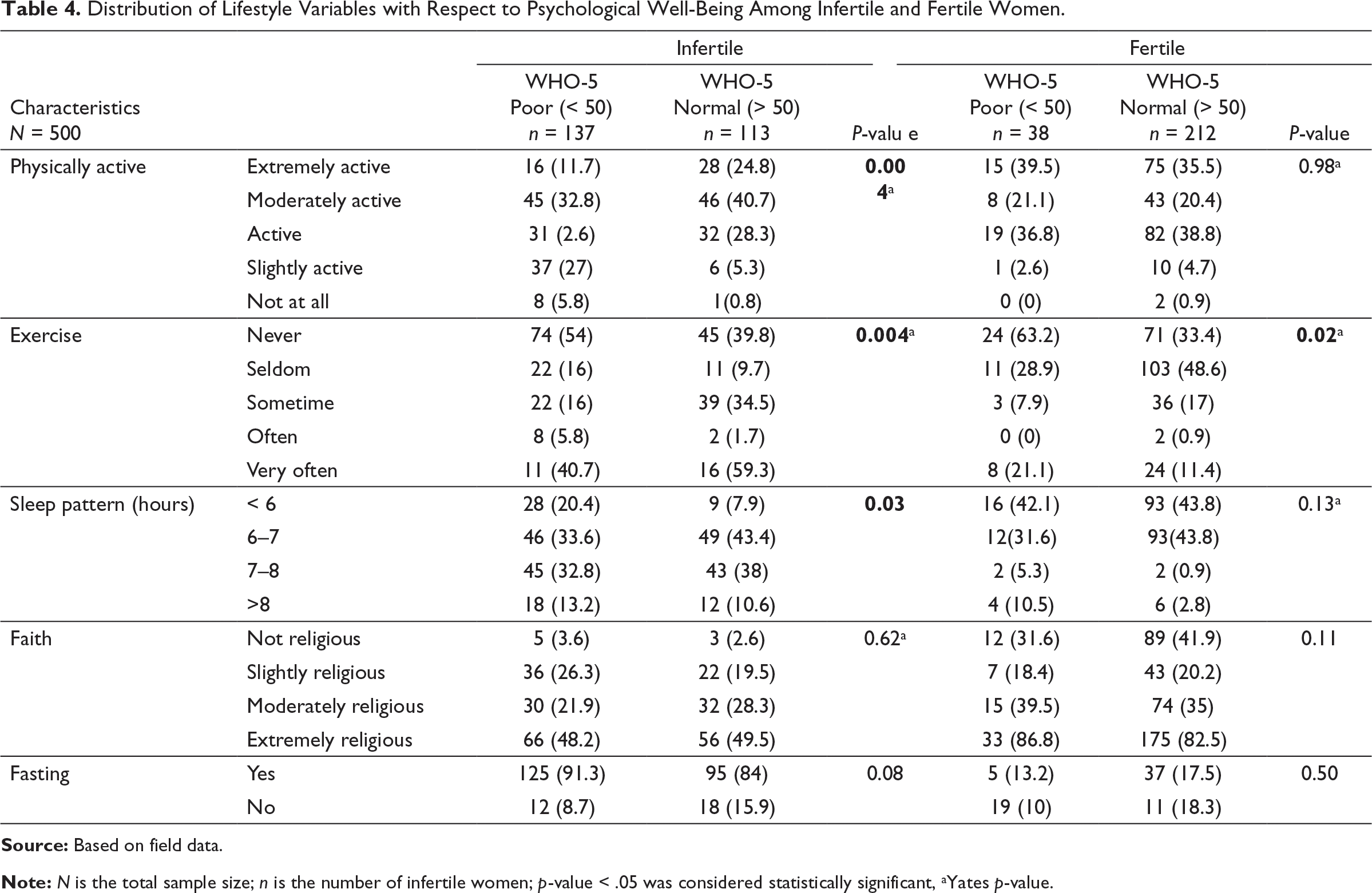
Distribution of Lifestyle Variables with Respect to Psychological Well-Being Among Infertile and Fertile Women.
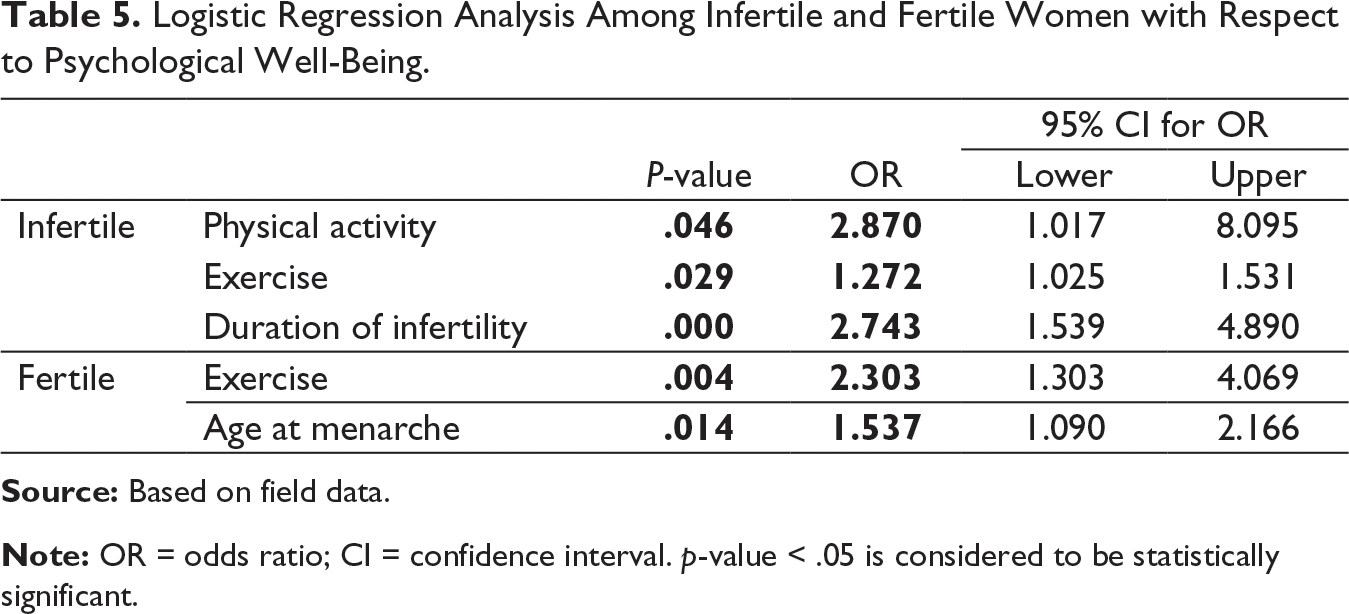
Logistic Regression Analysis Among Infertile and Fertile Women with Respect to Psychological Well-Being.
Discussion
The present study revealed that there is a significantly higher prevalence of poor psychological well-being among infertile women. Supporting our findings, other studies depict infertility as a risk to the psychological well-being of infertile women (Dargahi et al., 2018; Rani, 2018; Sadiq & Arshad, 2018; Hatamloye & Hashemi, 2012). When compared to fertile women, infertile women had lower mean scores in the components of positive interpersonal relationships, life purpose, self-acceptance, environmental mastery and personal growth (Dargahi et al., 2018; Khosla et al., 2021; Sadiq & Arshad, 2018). A systematic review shows that infertility affects a couple’s psychological well-being and quality of life (Karimzadeh et al., 2017). Further, infertility is found to show a sixfold significantly increased risk for poor psychological well-being. Infertility impacts psychological well-being through mental engagement, psychological turmoil and emotional-affective reactions (Abbey, Halman & Andrews, 1992). Infertile women who became parents experienced greater overall well-being than infertile women who had not become parents (Abbey, Halman & Andrews, 1992).
In developing countries, some socio-cultural factors such as demography, lifestyle and reproductive variables may aggravate psychological distress. Of the demographic variables, none of the variables except education impacted infertile women’s psychological well-being. As per the results, the lower the educational status, the poorer the psychological well-being of infertile women. In this regard, the results of a study conducted by Marufizadeh et al. (2016) and Greil et al. (2011) demonstrated that women with primary education had lower psychological well-being than those with higher education. The present study shows a significant difference with respect to family structure between poor and normal psychological well-being among fertile women. A nuclear family leads to poor psychological well-being among fertile women, which might be because of the physical and mental burden shared among family members in the joint family structure. Studies depict that psychological well-being and health are closely linked to older age (Steptoe, et al., 2015), which is in contrast to the results of the present study where there is no association between age and psychological well-being.
Of all the reproductive profile variables, duration of infertility and age at marriage are related to infertile women’s psychological well-being. The more the duration of infertility, the poorer was the psychological well-being. Women sense that their ‘biological clocks’ are running down, that is, an increase in the duration of infertility; they are likely to experience fertility as being even more urgent and unattainable. Therefore, it is more distressing. The present study determines that early age at marriage (below 18 years) causes poor psychological well-being among infertile and fertile women. Another study that supports the current study found that women who married as children (before the age of 18 years) had a higher overall lifetime and 12-month prevalence of psychiatric illnesses than women who married as adults (Marphatia et al, 2000). Girls who marry early are at higher risk of psychological disorders as they are denied the right to freely express their views and be defended against devastating traditional practices that will increase the risk of a lifetime and recurrent psychiatric disorders (Ahmed et al., 2013). Those marrying at an early age might be more susceptible to domestic violence, poor mental health and malnutrition (Prentice et al., 2010). In the present study, early age at menarche causes poorer psychological well-being among fertile women, which might be due to biological, socioeconomic status or nutritional reasons. Contrasting results are seen in another study, which depicts that evidence from developing countries shows that menarche occurs at an older age, suggesting indirectly that food insecurity on menarche may be more through nutritional mechanisms (Paluska & Schwenk, 2000). Various studies depict that clinical signs of PCOS, PCOD, anovulation and cessation of menstruation were associated with psychological distress (Hahn et al., 2005; Militello et al., 2021; Zangeneh, et al., 2012), which is not in line with the findings of the present study where there is no association between psychological well-being and disturbed menstruation and other possible causes of infertility.
Infertility affects the holistic existence of couples. Among the lifestyle variables, poor psychological well-being was present more among the infertile individuals who were less physically active and did less exercise. Supporting the present study, another study by Paluska and Schwenk (2000) depicts that people with depression tend to be less physically active than non-depressed individuals; increased aerobic exercise or strength training has been shown to reduce depressive symptoms significantly (Tucker et al., 1998). Sleep patterns among the infertile women showed that women who did not sleep for 7–8 hours a day were more prone to poor psychological well-being. Supporting the present study, another study where individuals who did not have a proper sleep schedule were associated with poorer psychological and physical health (Ekkekakis et al., 2000). Whereas, in fertile women, poor psychological well-being was found in women who did less exercise (p < .05). Supporting the present study, another revealed four themes of exercise relating to the maintenance of general well-being: exercise as a socially supportive activity, exercising to maintain well-being, exercising to maintain independence, and exercise as liberating (Sohbati et al., 2021). Conflicting the results of the present study another study depicts that spirituality and faith play a protective role and help improve the psychological aspects of infertile patients (Braga et al., 2018).
Further, regression analysis was performed to determine the association of different confounding variables with psychological well-being among infertile and fertile women. Of all the variables, physical activity, exercise and duration of infertility seem to affect the psychological well-being among infertile women (p < .05). Low physical activity poses an almost threefold increased risk of poor psychological well-being among infertile women. Early five years of infertility poses a threefold higher risk for poor psychological well-being among infertile women. This observation was in contrast to a study that does not show a significant relationship between infertile women’s demographic variables and the psychological well-being of infertile women (Ekkekakis et al., 2000). Physical activity has a considerable potential to enhance the well-being of infertile women. Even a short burst of 10 minutes of brisk walking increases our mental alertness, energy and positive mood (Stoll & Alfermann, 2000). Participation in regular physical activity can boost self-esteem and reduce stress and anxiety (Salmon, 2001).
Conclusion
The study aimed to understand the effect of primary infertility on the well-being of women. In addition, it has assessed the impact of socio-demographic variables, reproductive trajectories and lifestyle variables on psychological well-being independently and in light of their dynamic among North Indian women. The study ascertained that infertility was a major cause of the decline in psychological well-being in infertile women. In most and infertility clinics, women are treated for infertility, but their psychological well-Is often ignored. To improve the psychological well-being of women dealing with infertility, infertility education and awareness, physical activity and family counselling must be integrated in infertility treatment.
Footnotes
Acknowledgement
The authors express their gratitude to the National Commission for Women (NCW) of India for funding the project. They are thankful to the staff of Lady Hardinge Medical College, New Delhi, and the participants who cooperated with the research team. They also thank the research team for carrying out fieldwork in the time of the pandemic.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by grants from the National Commission of Women (Sanction Letter No. – F. No. 16(86)/2019-20)/NCW(RS)), India, and by research from Department of Anthropology, University of Delhi, India, and Lady Hardinge Medical College, New Delhi, India.