
Abstract
COVID-19 lockdown had an impact on access to essential health care services, especially for people suffering from chronic diseases. Non-communicable diseases like heart disease, diabetes, cancer, anaemia etc. posed many inconveniences to the patients and the health care system during this pandemic situation. This study records the response of the islanders regarding their experiences during the lockdown, and keeping the island situation in purview, it also suggests some preparedness measures for the future.
To highlight the problems faced by these patients during the lockdown, a study was conducted in two different areas of Port Blair, Andaman and Nicobar Islands. Andaman and Nicobar Administration provided utmost care during this period that included preventive and supportive health care services to each household and all communities residing in the remote islands too. Several measures were taken to control the spread of infection among the islanders. As the focus shifted towards handling the COVID patients, there had been certain problems faced by chronically ill patients and their need for health care. The study was taken up in two villages in Port Blair, that is, Dairy Farm and Junglighat. In this study, it was observed that 41% of the males and 35% of the females suffer from hypertension and 36% of males and 44% of females suffer diabetes, respectively, in the study area, and 16.6% suffer from both these diseases. Pearson’s correlation calculated between hypertension, diabetes and kidney disease of male and female patients of all age groups shows a strong positive correlation. The results are significant at p < 0.05. During lockdown, several of them faced problems, as they were reluctant to visit health centres for the fear of contracting the disease. The virus being more harmful to comorbid conditions, these patients required additional attention. Numerous patients, who were referred to mainland India for treatment, as advanced medical facilities that were unavailable on the island, could not go due to the unavailability of transport during the period of lockdown. This aggravated the burden of these diseases enormously.
There must be a way where the Island’s health sector can provide access to regular essential health care services to people suffering from chronic diseases during health disaster as such. Their health care should not be restricted and then the fear and commotion in the minds of people regarding their health can be resolved.
Introduction
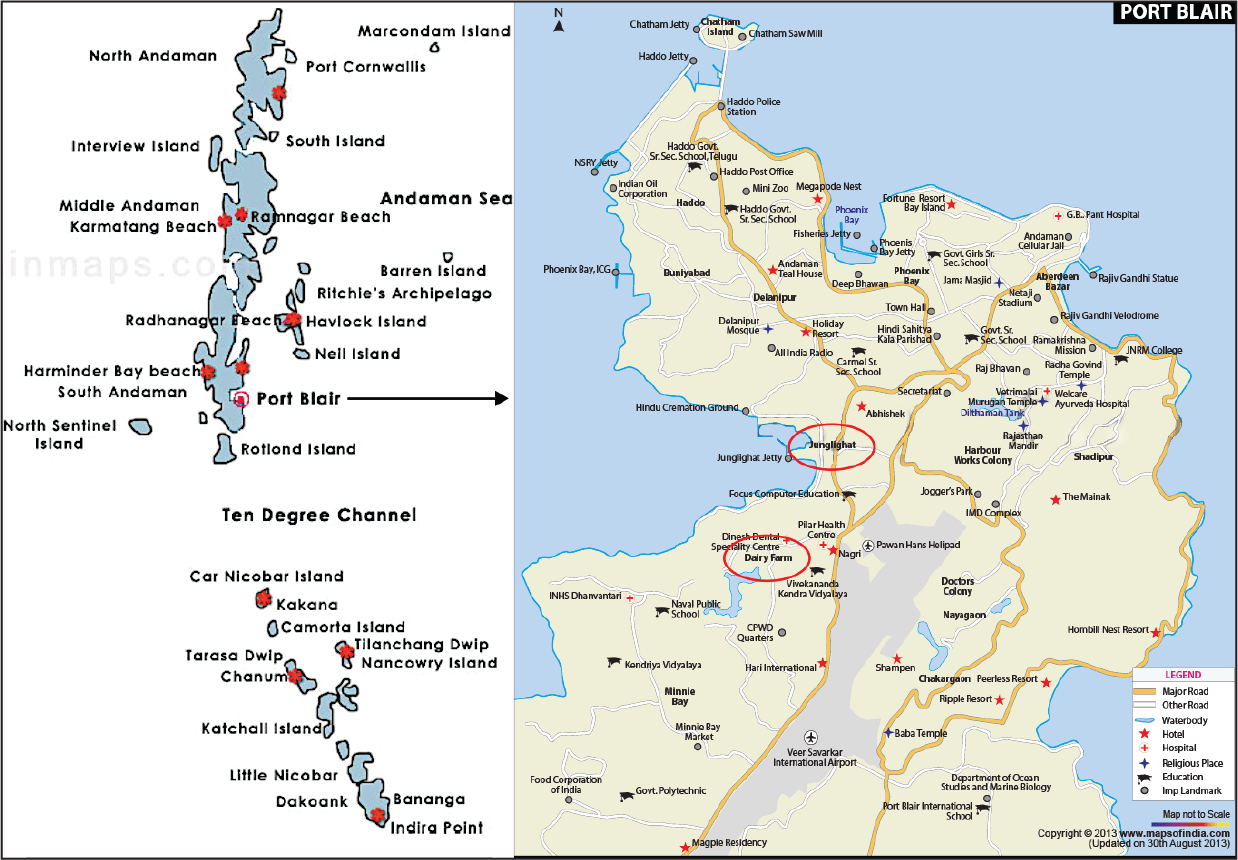
Port Blair, the capital of the Andaman and Nicobar (A&N) Islands located in the Bay of Bengal, is the headquarter for the district of South Andaman and the Union Territory’s (UT) only notified town. The modes of communication between the Island and mainland India are through air and sea. According to the 2011 Census, Port Blair town had a population of 100,608 with an average literacy rate of 89.76% (Census, 2011).
Presently, everywhere in the world, there has been a rapid epidemiological transition towards non-communicable diseases. The World Health Organization (WHO) released 2019 Global Health Estimates, which states that, out of the top ten causes of deaths globally, non-communicable diseases now make up to seven. For the past 20 years, heart disease remained the leading cause of death, at the global level. It now represents 16% of the total deaths from all causes. The number of deaths from heart disease increased by more than two million in 2000 and diabetes by 70% between 2000 and 2019 (World Health Organisation [WHO], 2020a). According to WHO (2020), ‘heart disease, diabetes, stroke, lung cancer and chronic obstructive pulmonary disease were collectively responsible for nearly 100 million additional healthy life-years lost in 2019 compared to 2000’. Therefore, a strong primary health care is the foundation on which everything rests, from combating non-communicable diseases to managing a global pandemic.
Illness or disease that lasts for more than 3 months is considered chronic. Common chronic diseases include cardiovascular disease, diabetes, arthritis, asthma, cancer, hypertension, kidney disease, etc. People suffering from chronic diseases are more prone to catching infections easily due to their low immunity caused by the ailments they are suffering from and the prolonged use of medication. In all the states and UTs of India, there has been a rise in the prevalence rates of overweight and obesity that could be a result of the change in nutritional habits over the past few years (Ahirwar & Mondal, 2019). The occurrence of overweight and obesity is attributed further to the industrialization and urbanization all over India that increased the tendency towards sedentary lifestyles and indulging in habits such as chewing and smoking tobacco, and alcohol consumption (Das et al., 2006). This posed a severe health problem for the quality of life of young and older people in India.
COVID-19 (SARS-CoV-2) was declared a pandemic by WHO on 11 March 2020, and all the countries around the globe were urged to take various measures to minimize physical contact, avoid gatherings, etc., in order to break the chain of the virus. When the cases of COVID infections reached India, the government also imposed a nationwide lockdown on 23 March 2020, to resist the spread of the virus. Complete lockdown in the country affected the socio-economic conditions of people from various strata. It also had severe repercussions on the physical and mental health of the common people and especially on people suffering from chronic diseases. There was a fear of the unknown in the minds of the people. It was a challenge for the health workers and administrators to give medical care for COVID-19-infected people and offer treatment to the non-COVID patients who require care at the hospital. Patients with chronic diseases had to suffer as the lockdown confined them to closed spaces and food and medication were not available as normal days. They could not avail their routine check-ups and only thing they depended on was their regular medication, which although was available to them at doorsteps, in some cases lack of prescription led to adverse consequences. These chronic conditions are a significant burden in terms of morbidity, mortality and health care, especially in the situation where suddenly a pandemic breaks out.
Researches were taken up globally, where the challenges faced during lockdown was studied. In a study approved by Pakistan Institute of Medical Sciences, Islamabad, Saqib et. al. (2020) showed that 53% of the chronically ill patients missed their routine medical check-up, 42% missed regular testing and 66% of them could not continue their daily exercise. In another study, Alyammahi et al. (2021) showed how patients with cardiovascular diseases, diabetes, respiratory system diseases and renal diseases are more susceptible to COVID-19. The article discusses the management plans to achieve the best therapeutic outcome for such patients.
Yet another study in Belgium examined how both content and delivery of chronic care are being affected by the pandemic (Danhieux et al., 2020). Another study among divorced or widowed and middle-aged female, adult patients with chronic diseases in Saudi Arabia showed that they were more vulnerable to have high levels of fear and health anxiety, which may lead to poor mental and physical health (Al-Rahimi et al., 2021). An online study in Kerala by Paul et al. (2020) shows the challenges to assess the medical care of chronic disease patients during the lockdown days. They concluded that there is a strong need for health policy reformations in the field of the chronic diseases health. No such study was carried out in A&N Islands, and there was a need to look into the lives of the patients with chronic illness in the island, as their situation is worse than anywhere in the world.
Significance of Study
This study was conducted to understand the conditions of the patients suffering from chronic diseases or comorbid health conditions, problems faced by them in accessing health services during the lockdown period and how they coped with the pandemic in the Island. The number of patients with chronic diseases is globally increasing every year and it positively correlates with the study area. It is an initiative to present an assessment of the health care services in Port Blair. The study aims to explore the scope for implementation of equitable and effective health care facilities for people suffering from chronic diseases during disruptive health care situation. The study would help health policy reformations in the field of chronic diseases and health care management and equip the stakeholders to respond adequately to medical emergencies during such natural disasters.
Methodology
Two villages, that is, Dairy Farm and Junglighat, under Port Blair tehsil, (Figure 1) South Andaman district, were selected for data collection. These densely populated areas of Port Blair were marked as containment zones during the pandemics. Under the National Programme on Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke, abbreviated as NPCDCS, community health workers regularly maintain a record of people suffering from chronic diseases. Therefore, data was collected from Community Health Centre, Dairy Farm and Urban Health Centre, Junglighat, on the people suffering from chronic diseases in the month of November and December 2020.
In the two health centres in the study area, 627 patients who suffering from chronic diseases from April to November 2020 were recorded. After collecting the details of these patients from the health centres, they were interviewed on telephone and in-person, using a structured and non-structured questionnaire to collect information on their health conditions and the problems faced by them in accessing health services during the lockdown and other constraints that affected their health directly or indirectly. Health workers were also interviewed to collect information on the measures taken by the administration to control and manage the pandemic situation and the problems faced by them in the distribution of health care services to people in the time of health disaster. To substantiate our findings, the NFHS-5 datasheet of different states and UTs of India was referred. The Director, Directorate of Health Services, Nodal Officer and health workers were consulted for data on programmes initiated and availed during the period of COVID lockdown for these patients and common people.
Results and Discussion
People Suffering from Chronic Diseases in the Area of Study
The most common chronic diseases observed in the study area are hypertension, diabetes, cardiovascular disease, stroke, lung and kidney disease, and cancer. The number of people suffering from chronic diseases was distributed according to different age groups (Table 1).
Distribution of Different Chronic Diseases by Age and Gender in the Study Area.
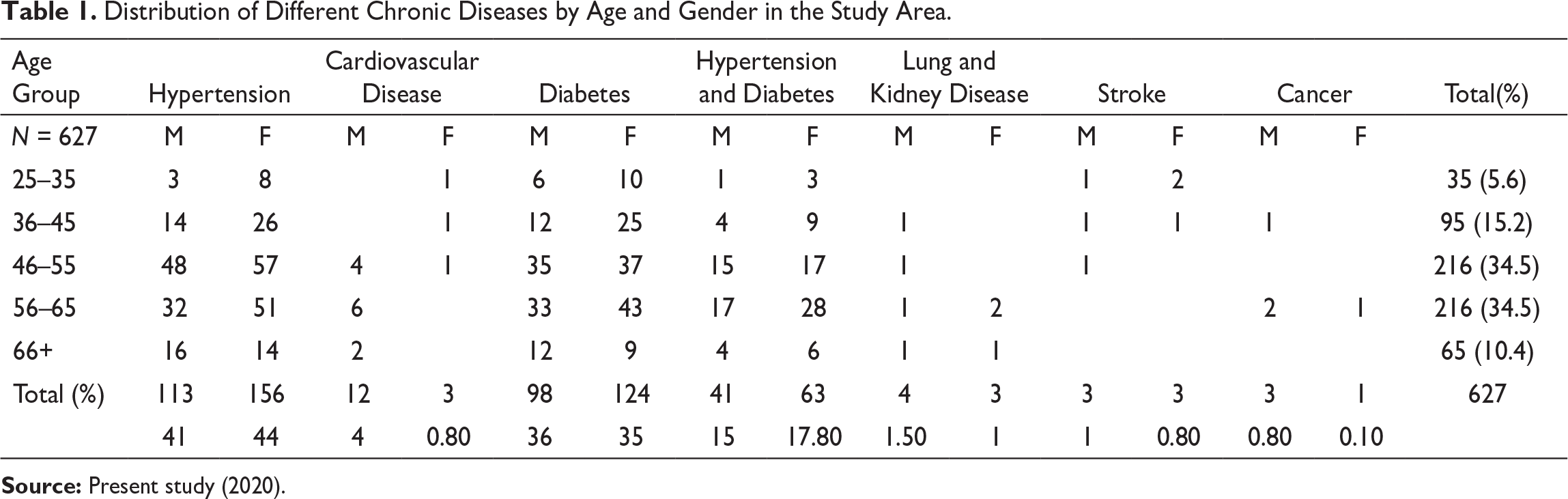
Hypertension and diabetes are the most prevalent chronic diseases in the area. It was observed that 41% and 36% of the males and 44% and 35% of the females suffer from hypertension and diabetes, respectively, and 16.6% suffer from both these diseases. Pearson’s correlation calculated among hypertension and diabetes male patients of all age groups shows a strong positive correlation (R = 0.9554 and p-value = 0.011231). Similarly, among females too, there was a strong positive correlation (R = 0.9555 and p-value = 0.000213). The results are significant at p < 0.05. Pearson’s correlation between hypertension and kidney disease also shows a strong positive correlation (R = 0.9312 and p = 0.006977). The result is significant at p < 0.05.
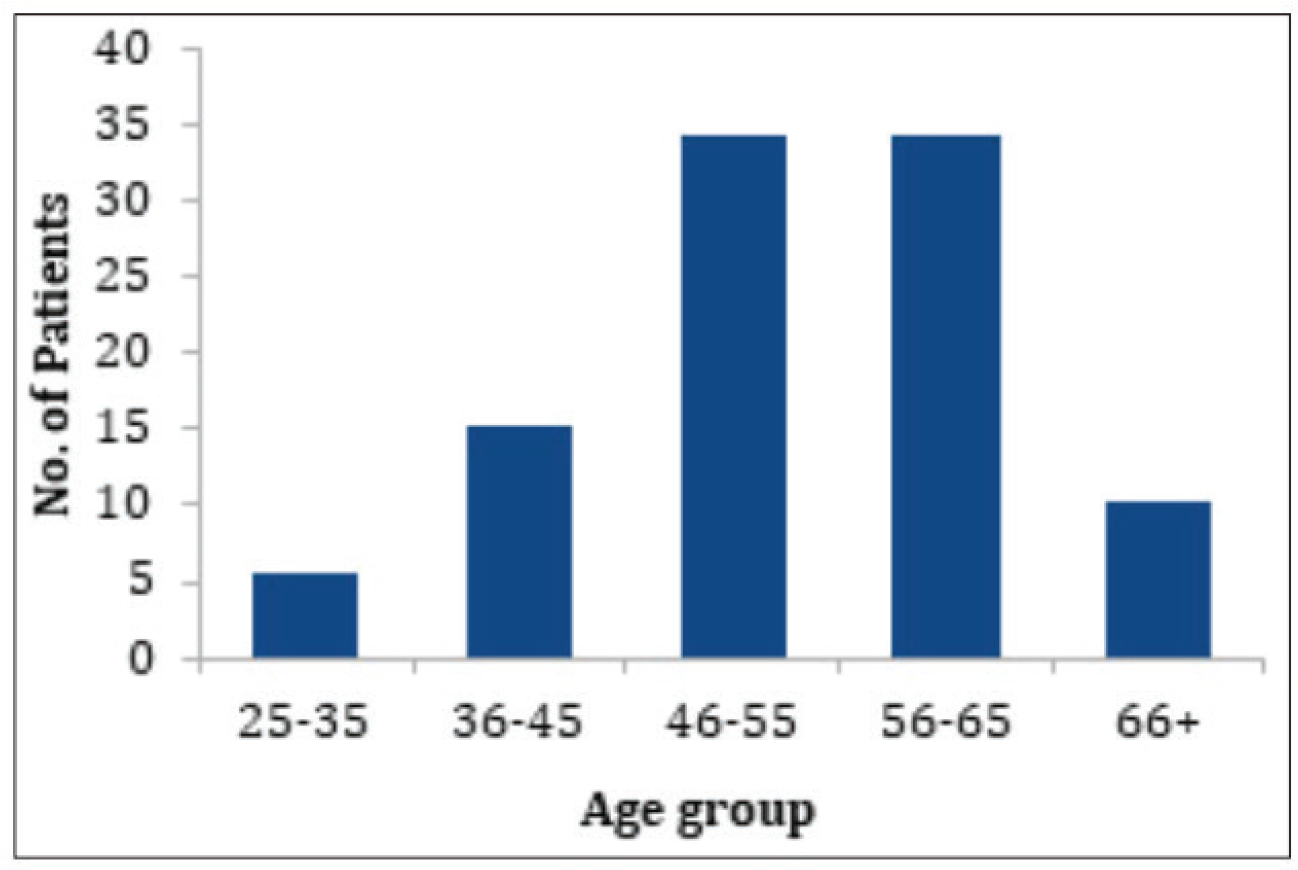
Figure 2 gives the distribution of the people suffering from chronic diseases in different age groups. It is observed that the maximum number of patients falls in the age group 46–65 years. The occurrence of lesser number of patients above 65 years in the data might suggest that probably the patients could not survive with the disease for a longer period, mostly due to stroke or myocardial infarction. Therefore, the age group 46–65 years is most vulnerable during pandemics and needs to be given special attention. It is alarming when lifestyle diseases are found among individuals in the age group 25–30 years (5.6%) as it increases with the advancement of age and medicines become a part of everyday life. In the study area, three individuals in this age group suffered from myocardial infarction. This condition was a result of hypertension and diabetes, of which they were unaware.
Chronic diseases tend to occur in older adults and are usually kept under control with regular check-ups, medications and following a healthy lifestyle. Therefore, continued care is required for these patients. During the lockdown, many of the respondents were not able to go for treatment for a long period, which aggravated their problems. Majority of the respondents are service holders, work in either government or private sectors and thus have a sedentary lifestyle.
A chi-square (χ2) test of independence was done to examine the association between chronic diseases and gender. The chi-square statistic is 9.6479 and the p-value is 0.046795. The result is significant at p < 0.05. This shows that all the variables are significantly correlated.
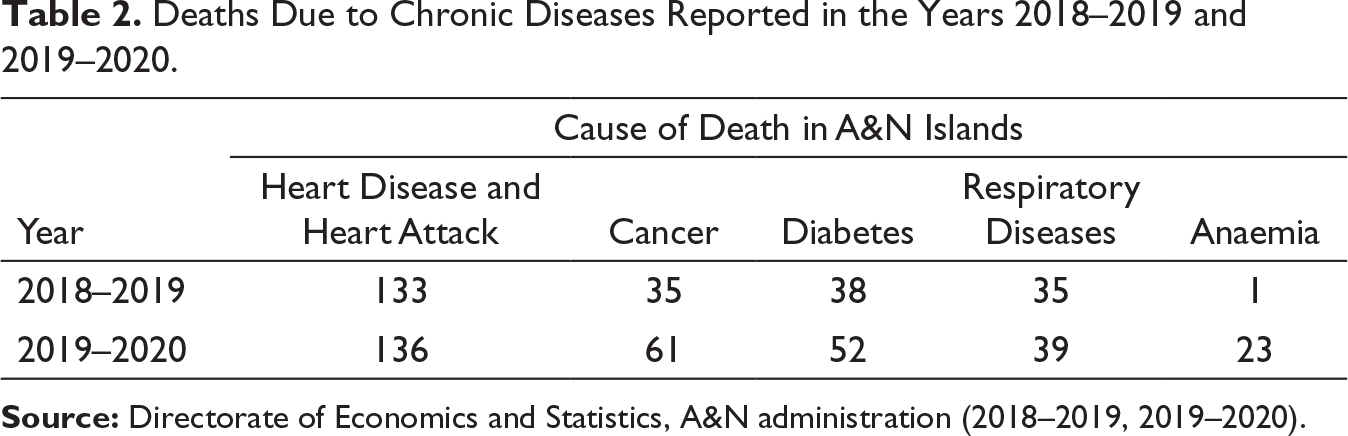
In Andaman Islands, there are numerous cases of deaths due to chronic disease each year. Cause of deaths in the years 2018–2019 and 2019–2020, given in Table 2, has been reported by the Directorate of Economics and Statistics, A&N Administration. It can be seen from the data that there is an increase in the number of deaths due to chronic diseases from the year 2018–2019 to 2019–2020. Heart disease is the leading cause of death in A&N Islands, and there is about a double increase in death due to cancer and diabetes in a span of 1 year. Reported deaths due to anaemia in 2019–2020 are alarming. Anaemia could be the result of poor nutrition and difficulty in procuring fresh vegetables and fruits on the Island as well as due to financial and other constraints.
Deaths Due to Chronic Diseases Reported in the Years 2018–2019 and 2019–2020.
The above observation is also substantiated by NFHS-5 (2020) report on health parameters from different states and UTs.
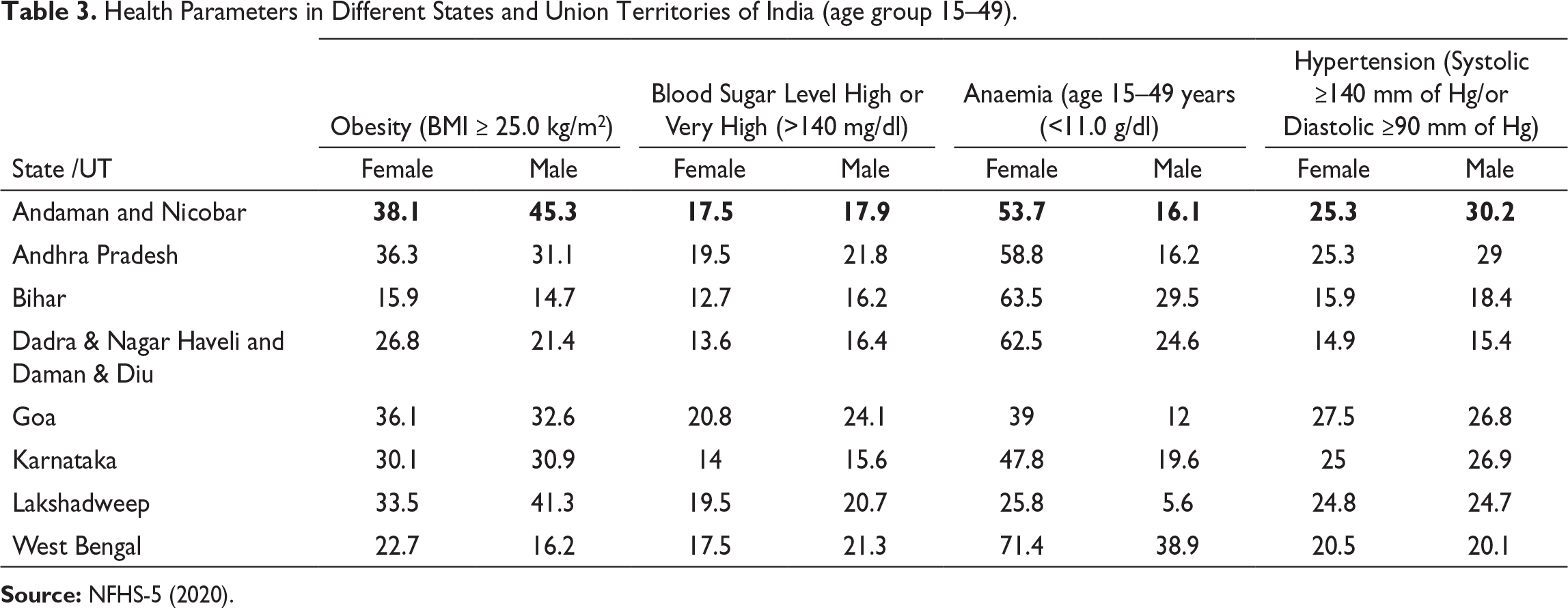
Table 3 shows gender-wise percentages of people suffering from obesity, blood sugar, anaemia and hypertension in four states and four UTs of India. (Selection of states and UTs for comparison of NFHS-5 data available has been done on the ground that either Port Blair has migratory population from these states or it has a tropical climate.). From the table, A&N Islands show the highest percentage of obesity and that obese people are vulnerable to diseases than normal individuals. According to NFHS-5, 45.3% of men and 38.1% of women recorded to be obese in A&N Islands. Around 17% of men and women have high blood sugar, 53% of women are anaemic and 30% of the men and 25.3% of women have hypertension, which again is the highest of all other places. Childbirth which is accountable for anaemia among women is often related to which is also high in Andaman (Directorate of Economics and Statistics, 2020a, 2020b). The high rate of addictions results in an increased number of people suffering from chronic diseases, which is a matter of serious concern.
Health Parameters in Different States and Union Territories of India (age group 15–49).
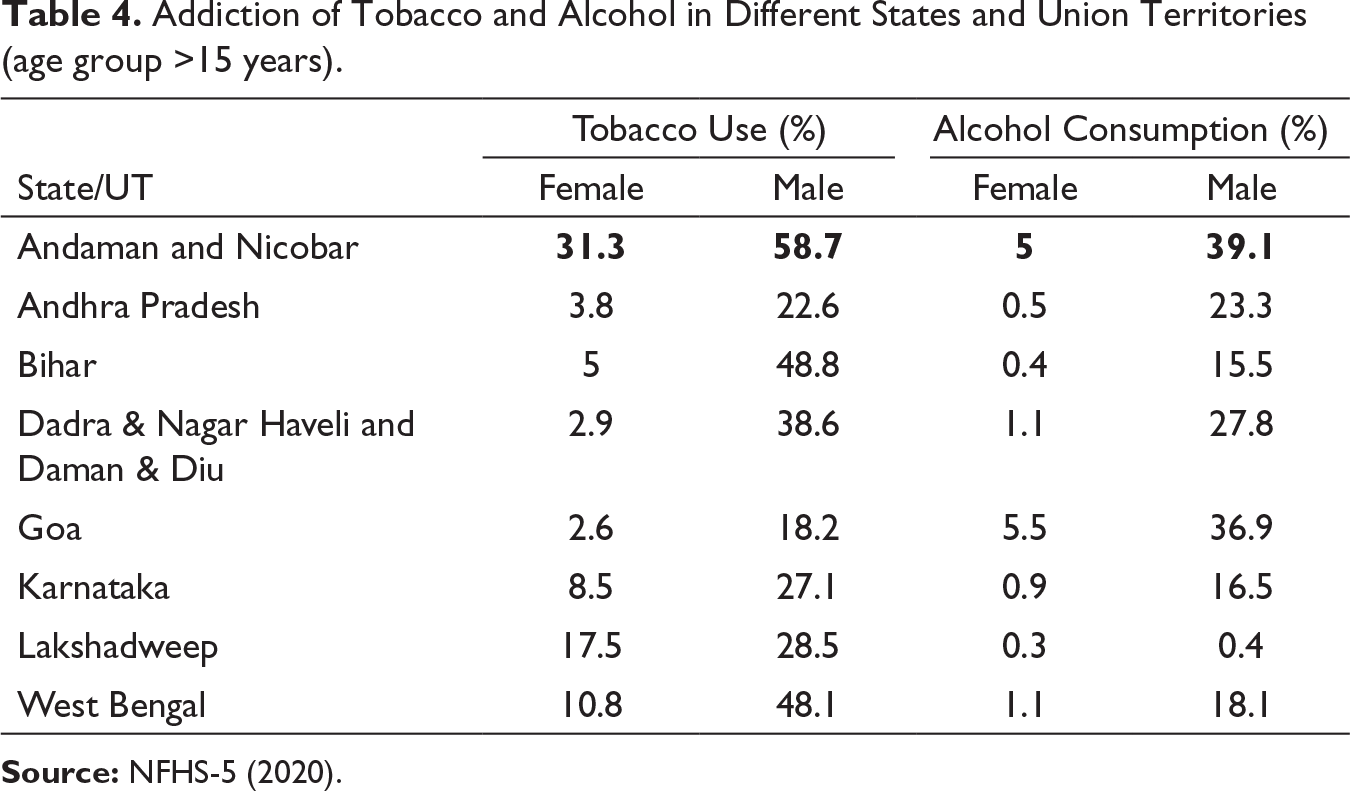
From the NFHS-5 data on tobacco and alcohol consumption (Table 4), it is observed that the use of tobacco and consumption of alcohol is high among the islanders compared to any other states or UT. Notably, 58% and 39% of the men use tobacco and alcohol, respectively. This high percentage of addiction, especially among adolescents and younger adults, lead to an increase in body weight, elevated blood sugar and blood pressure that ultimately results in hypertension and cardiovascular diseases in their later years.
Addiction of Tobacco and Alcohol in Different States and Union Territories (age group >15 years).
Tobacco intake and smoking, alcohol consumption, lack of physical exercise and sedentary lifestyle from a younger age aggravated chronic diseases and observed to be common among the respondents. Although traditional preparation of alcohol is illegal, yet few communities like Ranchi, Bhantu, and Nicobarese prefer to have their indigenous variety. Consumption of alcohol, tobacco and betel nuts among men start at a very young age. Betel nuts are an important cash crop of the island and are grown in many households; hence, it is easily accessible to women as well and they too consume it from a younger age. Studies have shown that betel nut chewing was significantly associated with blood pressure (Lin, 2008; Tseng, 2008, 2010). Older women are also addicted to tobacco and alcohol. There have been several news reports on the consumption and selling of drugs in the study area. These addictions may act as a catalyst for causing hypertension, diabetes and cancer.
With these observations, it may be assumed that the Islanders are more vulnerable to infections than any other place in the country, and therefore, they need special attention during such pandemic situation.
Health Care During Lockdown and the Dilemma
To curb the increasing number of COVID-positive cases in the Islands, A&N Administration took several measures. Starting from March 23, 2020, passenger flights were suspended for a considerable period. It was resumed after the lockdown, but the number of flights was reduced. Apart from nationwide lockdown in March–April 2020, complete lockdown was imposed on the island from 4 to 25 August 2020. Check posts were established at the entrance of various colonies and police officials kept strict vigilance on people. The news of 10 members of the indigenous Great Andamanese tribes being infected with the COVID forced the administration to take additional measures on the incoming passengers to the island. Rapid Antigen Test was a mandatory for the incoming passengers at the airport. The lockdown put strict restrictions on the movement of people. The Andaman Administration duly issued movement pass for people related to essential services.
Food, water, medicines and other essential commodities were made available during the lockdown, but there was an inconvenience in accessing them due to the complete closure of local transports. Online orders and home delivery of daily needs were also introduced in the Island during this period, but it had several constraints from both consumer and the supplier as Internet facility is in a developing stage on the island and still inaccessible to many areas of Port Blair city and other islands. Uncertainty of lockdown led to unrest and commotion among the local people towards procurement of food items and essential supplies, as the availability of many daily needs depends on the supply from mainland India. Fishing too was not carried out as earlier and few fishermen who went for fishing sold fishes for a higher price.
Technology took a centre stage in many areas during the pandemics in Port Blair. Telemedicine, teleconsultation, and online counselling were in practice during the lockdown to provide medical aid in time and to avoid any physical contact. Health workers and Auxiliary Nurse Midwife (ANM) were deputed for home delivery of medicines, whenever any person required. There was constant surveillance through phone and home visits on people under home quarantine. Govind Ballabh Pant Hospital is the only hospital with better and affordable facilities in the entire UT. Primary Health Centres, Community Health Centres, Urban Health Centres, AAYUSH Hospital, INS Dhanwantari etc. remained open throughout this period and was strengthened during the pandemic to cater to the needs of the patients in their respective areas/wards. The chief secretary ensured that medicines, milk and groceries would be available during the total lockdown in the UT and orders were issued for door delivery of all essential supplies and medicines. Masks and soap were distributed among the public by the administration.
The government used print and electronic media extensively for the awareness campaign among the public. Newspaper and government websites were taken to be reliable sources of information on COVID-19 pandemics. In Port Blair, All India Radio and Doordarshan were the most important medium of communication among the local people and health care service providers. Helpline numbers were constantly flashed on these platforms for medicines, online consultations and other health needs.
Despite all these, the Island still struggled to provide curative, preventive, rehabilitative and supportive health care services in many cases, across the islands. Different communities in remote areas of Port Blair faced difficulties in accessing health care services in time. Private hospitals remained closed during the lockdown, so the whole burden of treatment of the island population shifted to the government health units, which also led to the deterioration in the quality of services to the people suffering from chronic diseases at these hospitals. Govind Ballabh Pant Hospital under the Andaman & Nicobar Islands Scheme for Health Insurance (ANISHI) funds the referred patients who cannot be treated in Port Blair to Chennai and Kolkata for the treatment of diseases. Many patients could not avail this due to lockdown.
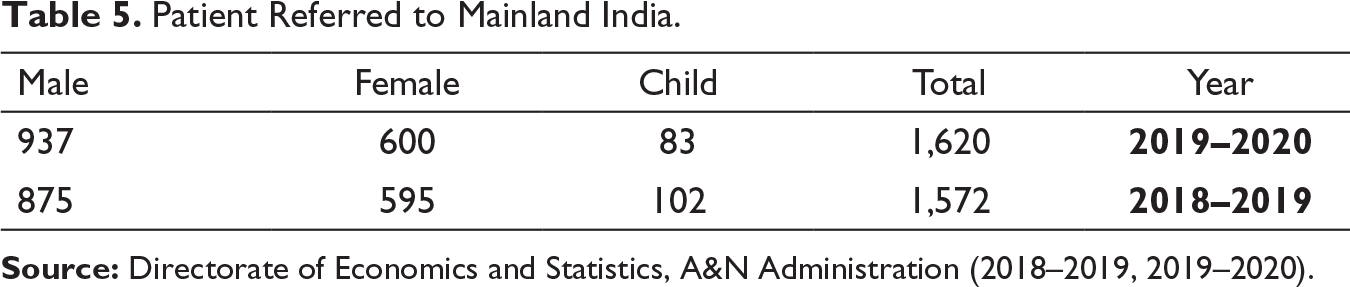
Notably, 1572 patients in the year 2018–2019 and a total of 1620 patients in the year 2019–2020 were referred to Chennai and Kolkata for treatment (Table 5), as per the data of the Directorate of Economics and Statistics. There was an increase in the number of patients referred for treatment in the mainland. During these pandemics, patients had to settle for other substitutive treatment available on the island that would just provide instant relief, but not a complete cure. Many such patients’ routine consultation was delayed and cancelled in the year 2020 due to the unavailability of transport and due to the patients and their family being sceptic about the being infected at the hospital. This greatly affected the patients with life-threatening diseases.
Patient Referred to Mainland India.
A grievous incident from the Dairy Farm area is an example of such consequence. A man in his late fifties complained of chest pain in March 2020 and was referred to Chennai by Govind Ballabh Pant Hospital for angioplasty as he had blocked artery. He had planned to visit Chennai in the month of May 2020, but the lockdown, disruption of flight services and the daily update of rapid increase in COVID transmission in Chennai in the news made him reluctant to go to a hospital anywhere for fear of being infected. In the month of May 2020, he suddenly fell sick, though he was taking his daily dose of prescribed medicine; he had severe chest pain and breathing problems. In August, his condition deteriorated further and had no option than going to the hospital. His family called for the ambulance, in the process of undergoing many formalities because of being in the containment zone, some valuable time was lost and when the ambulance finally arrived, he had breathed his last. This could have been avoided, had there been medical assistance on time and the patients had entrusted the health facilities available on the island during the pandemics.
Yet another incident from Prem Nagar speaks of the lacuna during emergencies. In August 2020, COVID Cell collected four samples from a family, and three members were found to be COVID positive, and the sample of a 58-year-old man went missing. The man fell sick with jaundice and he was already suffering from prolonged liver and kidney disease and diabetes. His wife who was COVID positive took care for him. Due to the lack of proper medical aid for his comorbid conditions, he could not survive. Other members of his family were COVID-19 negative in due course.
A respondent with kidney problem could not undergo dialysis and was asked to continue with the prescribed medicines; therefore, his conditions deteriorated with body swelling, itching and low haemoglobin due to a lack of proper treatment in time.
According to another respondent, Port Blair also had a spread of common flu in August 2020. It affected many people in Port Blair, especially the children. With many of its symptoms similar to COVID, it created additional fear in the minds of the people. Diseases like flu make the body weak and eventually weaken the immune system. This affected everyone, especially the patients suffering from chronic diseases, who are at greater risk of any kind of infection.
Some of the respondents reported that they used many home remedies for boosting their immunity. Again, the lack of knowledge about which ingredients to consume and in what quantity created confusion and resulted in developing other ailments in the patients with comorbid condition.
Patients requiring emergency operations, cancer patients undergoing chemotherapy, and other such patients were also in anguish, as the emergency treatment was given in the only hospital with a dire consequence at later stages. Health workers battled the pandemics at the forefront. Many of the doctors and nurses also contacted the infections during the time. To avoid such deplorable incidents, an integrated planning is required to reduce fatal cases and bring peace to the aggrieved family with people suffering from chronic diseases.
Pandemics Preparedness: Response and Suggestion
No generation alive in the country had witnessed any situation like this in their lifetime; therefore, there is a need to be well informed and prepared for such situations in the future. There was a sense of confusion everywhere about what are happening and what will happen next, especially among the common mass and those suffering from chronic diseases. To attain the goal of the most effective health care system during any emergency such as the current pandemics, we need to work upon the short- and long-term measures at all levels of the society from the stakeholders, to policy makers, to the community itself.
Advanced and timely communication with law enforcement agencies, health professionals, patients and their families can not only help to ensure the better health of the individuals but also increase trust in the health care services of their area. Effective communication can help build a need-centred approach, which may help in the equitable and effective distribution of services. Prior arrangements can be made for the patients with fatal cases to go for treatment to the mainland even during the lockdown, if the infrastructure is not present on the island as the period of lockdown witnessed many adverse incidences.
For the establishment of an efficient distribution channel of supply of medicine, information and health care facilities, a well-trained workforce and accessibility to advanced technology is required. Infrastructure to provide counselling and coordinate with the patients and family members may help allay any fear regarding health and disease. Integrated structure of hospitals was another issue of demotivation to avail health check-ups during the lockdown. It would be better to have separate wards for the treatment of such communicable diseases like COVID.
Various myths came up about the virus and certain ways to defy infection. Many people believed in them religiously as the fear was so intense than common sense. A special cell to keep a constant check on such activities and provide an authentic and easily accessible source of knowledge and information on the current situation should be established. Local language should be used for the dissemination of information among common people to ensure a better understanding and effective management of the area.
A general understanding of pandemics and epidemics should be included in the school curriculum. There is a need to develop a culture of proper hygiene. Hand washing, covering the face while coughing and other related health education and practice would be the key to attaining a better health status, especially in fighting against any pandemics in the long term.
Conclusion
This study was conducted among the people suffering from chronic diseases in Port Blair, A&N Islands, to bring out the inconveniences they faced during the COVID-19 lockdown. Non-communicable diseases, such as myocardial infarctions, strokes, diabetes, obesity, kidney disease, cancer and other premature deaths, became an enormous burden on the health care systems of the Island that worsened during COVID-19 pandemics. According to WHO (2020b), non-communicable diseases now make up to seven of the top ten causes of death. Studies across the Globe suggest the difficulties of the patients with chronic illnesses that worsen in an island situation during pandemic infection.
Two villages, that is, Dairy Farm and Junglighat in Port Blair tehsil, South Andaman district, were selected for data collection as these are densely populated and were marked as containment zones during the current pandemics. Data on patients with chronic illness was collected from Community Health Centre, Dairy Farm and Urban Health Centre, Junglighat.
The Director, Directorate of Health Services, Nodal Officer and health workers were consulted for data on programmes initiated and availed during the period of COVID lockdown for these patients and common people. Out of the 627 patients interviewed, 41% of the males and 44% of the females suffer from hypertension, 36% males and 35% suffer from diabetes, and 15% of males and 17% of females suffer from both. Others suffer from cardiovascular diseases, stroke, lung and kidney problems, and cancer. Most of these patients are in the age group 46–65 years (34.5%), though there are patients also in the younger age groups. Pearson’s correlation calculated between hypertension, diabetes and kidney disease of male and female patients of all age groups shows a strong positive correlation. The results are significant at p < 0.05.
Anaemia among women is also a concern on the Island. The respondents are service holders, working in either government or private sectors or businesses, and having a sedentary lifestyle. This could be attributed to shifts in the nutritional scenario over the past decades. Further, increased indulgence in habits such as smoking, betel nut chewing, tobacco intake, alcohol consumption, sedentary lifestyles and lack of physical activity resulted in an increase in overweight and obesity among the Islanders. This has a positive association with the lifestyle diseases like hypertension, diabetes etc., which pose severe impacts on health and quality of life of the adults.
NFHS-5 datasheet on health parameters of different states and UTs of India was referred where A&N Islands top the list in the lifestyle diseases as well as in addictions. Several studies show that these addictions are the reasons of increase in non-communicable diseases and thus it can be assumed that that the Islanders are more vulnerable to infections than any other places in the country. Lack of advanced medical facilities and health care during emergency proved fatal in some cases in the study area.
Among the respondents, some patients reported that their symptoms aggravated during the lockdown. Many respondents expressed their fear of being infected with the virus if they go for treatment in the hospital and tried to suppress their illness through medication. Many of these patients faced problems in emergency health care, as they were unable to go for advanced check-ups in the mainland. The situation became fatal in some cases.
A&N Administration had taken many initiatives to control the spread of infections in the island, but there is a need to make alternative arrangements for the patients suffering from chronic diseases.
Current pandemic situation has highlighted the need for pre-preparedness programmes. Government agencies, policy makers and executors together need to formulate an operating procedure, which could be followed in the A&N Islands to avoid fatal cases because of unavailability of transport and eventually lack of communication with the mainland during the lockdown. To prevent and reduce the burden of communicable and non-communicable diseases, emphasis on reducing addictions, changing lifestyle, and maintaining hygiene, sanitation and preventive health care need to be contemplated. This study also facilitates the enumeration and specification of the short- and long-term goals for attaining an effective health care system in the time of health emergency.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.