
Abstract
Spina bifida (SB) is a neurodevelopmental disorder characterised by the incomplete closure of the embryonic neural tube, resulting in a neural tube defect (NTD) that affects the development of the spine and spinal cord. Both genetic and non-genetic factors contribute to the occurrence of SB, including deficiencies in folic acid and vitamin B12, maternal obesity, smoking, epilepsy, alcohol consumption, drug use, and a history of previous pregnancies affected by SB. Complications associated with SB include meningitis, hydrocephalus, neonatal paralysis, and urinary or faecal incontinence. Considerable advancements have been made in raising awareness, improving diagnostic capabilities, and establishing specialised clinics and multidisciplinary teams (MDTs) dedicated to SB management. However, several gaps persist in its management. These include inadequate awareness and education among healthcare professionals, limited access to healthcare services, a scarcity of surgical workforce and MDTs, social stigma and discrimination, and research and data accessibility gaps. The implications of these management gaps in SB care encompass diminished quality of life, increased morbidity and mortality rates, and economic consequences related to surgical management. To improve SB management outcomes in Africa, strategic interventions should focus on enhancing healthcare infrastructure and resources, strengthening education and awareness programs for SB prevention and support, addressing cultural concerns, improving neonatal surgical care, and enhancing research and guidelines. By addressing these gaps through targeted, equity-focused interventions in healthcare infrastructure, education, cultural adaptation, neonatal surgical care, research, and policy, substantial improvements can be made in SB care and outcomes in Africa, reducing the disproportionate burden of disability in low-resource settings.
1. Introduction
Spina bifida (SB) is a neurodevelopmental disorder characterised by the incomplete closure of the embryonic neural tube, resulting in a neural tube defect (NTD) that affects the development of the spine and spinal cord.1,2 The most severe manifestation of SB, referred to as myelomeningocele, manifests as a dorsal opening of the spinal cord, resulting in a visible plaque on the fetus’ back. While the precise aetiology of SB is still subject to investigation, genetic factors are believed to play a significant role.1,2 Furthermore, there are several non-genetic risk factors associated with SB in neonates, including deficiencies in folic acid and vitamin B12, maternal obesity, smoking, epilepsy, alcohol consumption, drug use, and a history of previous pregnancies affected by SB.1,2 Consequently, individuals with SB frequently experience a range of complications, including meningitis, hydrocephalus, neonatal paralysis, and urinary or faecal incontinence.
The occurrence of SB varies among different populations, influenced by factors such as geographical location and ethnicity.1,3 Globally, it is estimated that approximately 320,000 newborns are affected by SB annually, with a higher incidence observed in low- and middle-income countries (LMICs).1,3,4 These countries face significant healthcare challenges contributing to the higher incidence of SB in their populations. In contrast, middle- and high-income countries have witnessed a decrease in SB incidence due to the implementation of mandatory folic acid fortification and the establishment of multidisciplinary teams (MDTs). 5 Nonetheless, disability remains a notable concern in marginalized communities within LMICs due to limited access to treatment. 6
In Africa, the estimated incidence of SB ranges from approximately 9.95 to 15.27 cases per 10,000 live births, with notable variations: higher in parts of East Africa (e.g., Ethiopia ∼3.2 per 1,000) and lower in North Africa (e.g., Libya/Tunisia <0.1 per 1,000), reflecting differences in folic acid fortification policies, prenatal care access, and reporting.7,8 The prevalence of SB in African nations is depicted in Figure 1. Prevalence of SB in African nations, with dot size reflecting cases per 100,000 live births; larger red dots indicate higher prevalence.
8
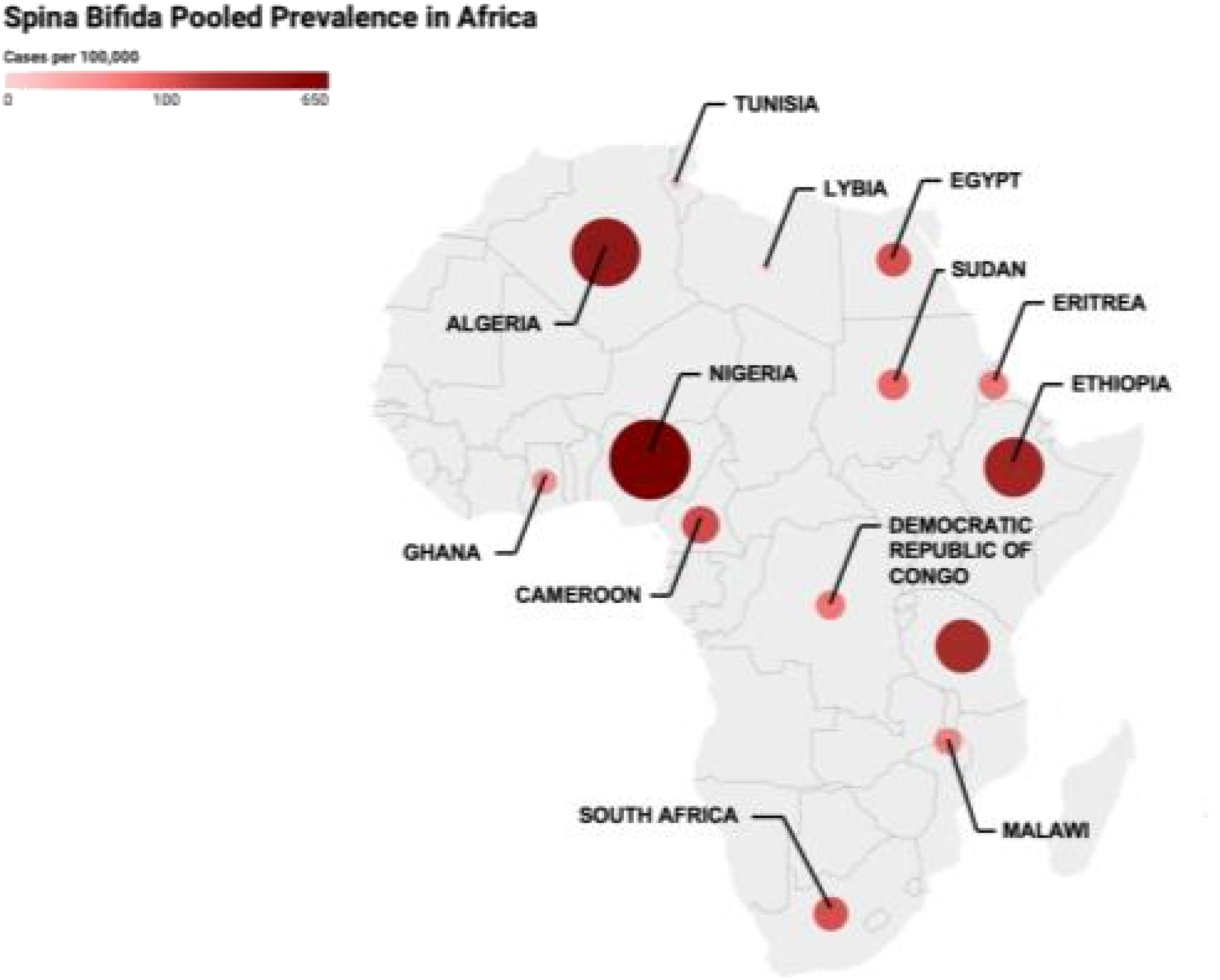
Despite the significant burden of SB in these African regions, it often goes unreported. Many SB patients in Africa are rarely documented in hospitals, primarily due to factors such as societal neglect and concerns regarding surgery-related mortality.9,10 The absence of accurate records regarding antenatal care, births, and deaths further limits the comprehensive understanding of SB in Africa.9,10
The use of over-the-counter medication, including opioids, is a common practice in Africa, and some studies suggest that it may pose a risk factor for congenital anomalies.11,12 Another challenge Africa faces in terms of SB risks is the prevalence of strict customs and norms that endorse the use of naturopathic medicine, primarily composed of herbs from unknown sources and may contain teratogenic substances, thereby increasing the likelihood of SB occurrence in offspring. 2
This perspective review adopts a public health systems lens, focusing on how structural health system weaknesses, socioeconomic disparities, and governance challenges contribute to poor SB outcomes across Africa, including SSA and North Africa, while highlighting key regional differences in health system capacity, resource allocation, and policy implementation. It critically examines why gaps persist, such as underinvestment in the health workforce and limited policy prioritization, and proposes actionable, context-adapted strategies to strengthen care delivery and improve outcomes.
2. Methods
This perspective review synthesized and critically appraised evidence on the burden, management gaps, health system challenges, and strategic interventions for SB in Africa. A comprehensive search was conducted in PubMed, EMBASE, Google Scholar, Scopus, and Web of Science. Search terms addressed epidemiology, prevention, surgical care, workforce capacity, stigma, rehabilitation, food fortification, and policy implementation.
Eligible studies were full-text, peer-reviewed articles in English focusing on SB epidemiology, prevention, diagnosis, management, or outcomes in African countries. Included designs comprised observational studies, case series, qualitative studies, systematic reviews, meta-analyses, policy analyses, and relevant global health reports. Selected international comparative studies were incorporated where necessary for contextualization. No strict date limits were applied, though priority was given to contemporary evidence reflecting current surgical practice, fortification policies, and health system structures.
Studies were excluded if they did not specifically address SB or NTDs in African populations, or lacked clinical or public health relevance. Reference lists and key organizational reports were manually screened for additional sources. Studies were prioritized based on methodological rigor, contextual relevance, and contribution to understanding SB outcomes.
Summary of methodology.

3. SB management gaps in Africa
The management of SB in Africa is shaped by multiple, interrelated barriers spanning health systems, socioeconomic conditions, and sociocultural contexts. These include limited awareness, restricted access to care, financial constraints, workforce shortages, social stigma, and gaps in research and data systems. Although discussed separately, these challenges frequently overlap and reinforce one another, contributing to delayed diagnosis, fragmented care pathways, and suboptimal long-term outcomes.
3.1. Lack of awareness and education
Limited awareness of SB remains a major barrier to timely diagnosis and appropriate care across many African settings. A significant proportion of parents possess inadequate knowledge of the condition, often attributing it to superstition, prenatal accidents, or environmental exposures.13,14 These misconceptions contribute to delayed care-seeking, concealment of affected children, and reliance on alternative or non-medical treatments.
In addition, low health literacy and ineffective communication within healthcare settings further compound these challenges. Even when families access medical care, inadequate counselling regarding surgical risks and outcomes may lead to treatment refusal or early withdrawal from care.15–17 For example, studies in Ethiopia highlight how limited awareness contributes to delayed presentation and discontinuity in treatment. 15
These issues are particularly pronounced in rural SSA, where literacy levels are lower and access to reliable health information is limited. In contrast, parts of North Africa and urban centres demonstrate relatively higher levels of awareness, likely reflecting stronger public health campaigns and improved healthcare access.8,16,17 Importantly, gaps in awareness not only affect initial presentation but also influence long-term engagement with care, including adherence to follow-up and rehabilitation.
3.2. Limited access to healthcare services
Access to specialised SB care in Africa is constrained by infrastructural, diagnostic, and geographic barriers. Many healthcare facilities lack essential diagnostic tools such as ultrasound, MRI, and maternal serum alpha-fetoprotein (MSAFP) screening, limiting early detection during antenatal care.6,18,19 In several SSA settings, the absence of these tools contributes to underdiagnosis and missed opportunities for early intervention.18,19
Following birth, delays in diagnosis are further exacerbated by limited availability of specialised expertise and diagnostic infrastructure. 20 These gaps reduce the likelihood of timely surgical intervention and increase the risk of preventable complications.
Geographic barriers also play a significant role. In many rural areas, patients must travel long distances to access tertiary care centres, often facing poor road infrastructure and limited transportation options. 19 As a result, access to care remains highly uneven, with urban populations benefiting from relatively better availability of specialised services compared to rural communities. 21
Importantly, these access limitations are closely intertwined with financial constraints and workforce shortages, reinforcing systemic inequities in care delivery across regions.
3.3. Financial constraints and socioeconomic challenges
Financial barriers represent a major limitation in the management of SB across Africa. The costs associated with diagnostic procedures, surgical care, transportation, accommodation, and long-term follow-up are often prohibitive, particularly for low-income households.6,20,22 Studies across multiple African countries demonstrate that these financial constraints contribute to delayed interventions, poor treatment adherence, and suboptimal outcomes.6,20
These economic challenges are closely linked to access barriers, as patients who are unable to afford transportation or medical costs are less likely to seek or complete care. For example, out-of-pocket expenditures for radiological investigations and surgical care frequently result in treatment delays or abandonment.20,22
Additionally, caregiving responsibilities, often borne primarily by mothers, further amplify the socioeconomic burden. Managing a child with SB alongside other household responsibilities can reduce income-generating capacity and increase financial vulnerability. 23 The absence of robust health insurance systems and social protection mechanisms in many African settings further exacerbates these challenges, reinforcing cycles of inequity and poor health outcomes.
3.4. Shortage of the surgical workforce and MDTs
Workforce limitations represent a critical bottleneck in SB care delivery across Africa. In sub-Saharan Africa, the neurosurgical workforce remains severely limited, with an estimated ratio of one neurosurgeon per seven million people, compared to one per 100,000 in Europe. 24 Moreover, there is significant regional disparity, with the majority of neurosurgeons (756 out of 1,165) located in North Africa, leaving Central, East, and West Africa markedly underserved. 25
This shortage is particularly evident in paediatric subspecialties. For instance, at the University of Nairobi, there remains a lack of fellowship-trained paediatric neurosurgeons despite a high burden of SB cases. 26 Similarly, Ghana, with a population of approximately 26 million, has only 11 paediatric surgeons available to manage complex conditions such as SB.20,27
Beyond surgical capacity, there is a significant shortage of MDTs, including paediatricians, orthopaedic surgeons, urologists, radiologists, and rehabilitation specialists. The absence of these teams limits the provision of comprehensive, long-term care. Diagnostic capacity is also affected, with some African countries reporting ratios as low as one radiologist per one million people, or none at all, further delaying detection and management.28–30
These workforce constraints not only limit immediate care delivery but also hinder training, mentorship, and the sustainability of specialised SB services.
3.5. Social stigma and discrimination
Social stigma and cultural beliefs significantly influence SB care-seeking behaviours and long-term outcomes. Misconceptions about the condition may lead to concealment, delayed presentation, or preference for traditional healing practices over biomedical care.2,17
The extent of stigma varies across regions. For example, in South Africa, where awareness and access to healthcare are relatively higher, stigma appears less pronounced, and many individuals with SB have access to specialised care and educational support. In contrast, in lower-resource settings such as Uganda or Somaliland, stigma and discrimination remain more pervasive, often driven by cultural beliefs and limited awareness.14,31
These social barriers extend beyond healthcare access, affecting education, social integration, and psychological well-being. Adolescents with SB may experience bullying, social isolation, and stigma-related concealment, which can further discourage engagement with healthcare services. 7 These factors often operate alongside structural barriers, compounding delays in care and negatively influencing long-term outcomes.
3.6. Research and data accessibility gaps
Research on SB in Africa is limited by significant gaps in data availability and quality. Existing evidence is concentrated in a small number of countries, restricting broader regional generalisability.32,33 This uneven distribution of data limits comprehensive understanding of SB epidemiology, outcomes, and healthcare needs across the continent.
Accurate estimation of SB incidence is further complicated by incomplete birth registries, underreporting, and poor case detection. 33 For example, studies in Zambia have highlighted high rates of loss to follow-up, underscoring challenges in longitudinal data collection and outcome tracking. 9
In addition, the limited number of dedicated research centres focused on SB restricts the development of context-specific interventions and clinical guidelines. Without reliable data systems, national planning, resource allocation, and evaluation of interventions remain significantly constrained.9,33 The gaps in SB management across Africa are visually represented in Figure 2. Gaps in SB management in Africa, with arrows highlighting key challenges: limited awareness and education, poor access to healthcare, financial and socioeconomic barriers, shortage of surgical and multidisciplinary teams, social stigma, and gaps in research and data.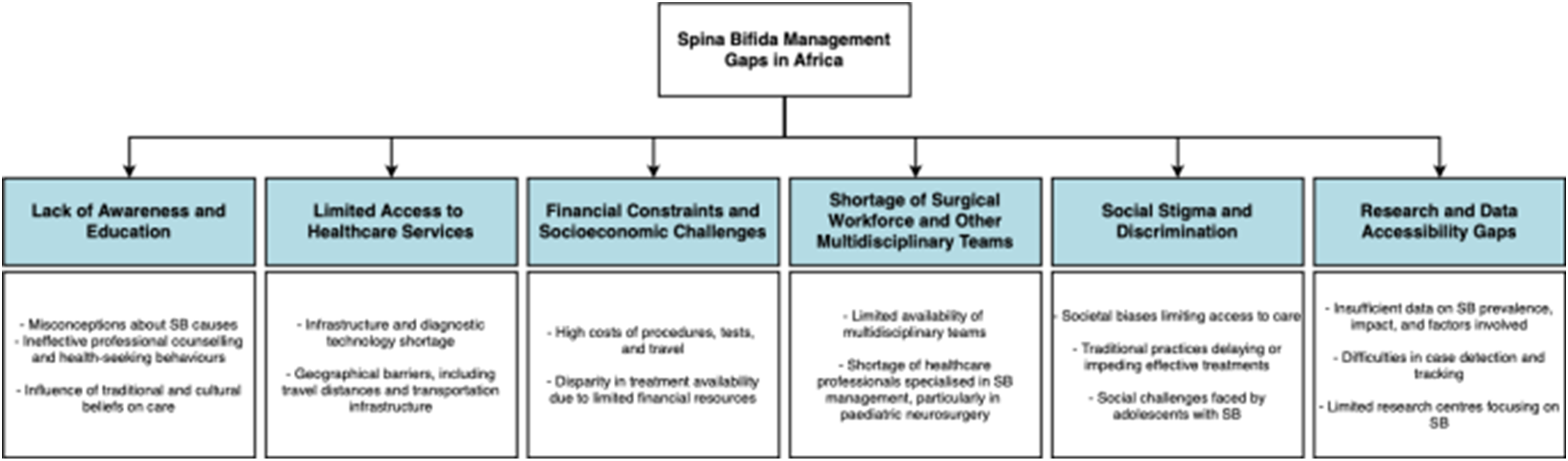
4. Implications of gaps in SB management
4.1. Poor health outcomes
The combined effect of limited awareness, restricted access, financial barriers, and workforce shortages results in delayed diagnosis and inadequate treatment, leading to poorer health outcomes for individuals with SB.
Delayed or absent surgical intervention increases the risk of complications such as hydrocephalus, meningitis, infections, and musculoskeletal deformities.10,34,35 Mortality rates remain significantly higher in settings with limited access to timely surgical care compared to regions with well-established services.34,35
Long-term outcomes are further compromised by inadequate follow-up and rehabilitation services. In SSA, up to 40% of individuals with SB lack access to appropriate rehabilitation, contributing to higher rates of functional disability and reduced quality of life. 36 Late presentation also remains common; for instance, studies in Nigeria report a median presentation time of three days for paediatric surgical conditions, including SB. 37
These outcomes reflect the cumulative impact of systemic barriers rather than isolated clinical challenges, highlighting the need for coordinated improvements across the care continuum.
4.2. Economic consequences
The burden of SB extends beyond clinical outcomes to significant economic consequences at both individual and societal levels. Limited access to appropriate care reduces functional independence, restricting educational attainment and employment opportunities for affected individuals.18,22
At the household level, ongoing medical needs, transportation costs, and caregiving responsibilities create sustained financial strain. Caregivers, particularly mothers, may experience reduced income-generating capacity, further exacerbating economic vulnerability. 23
At a broader level, reduced workforce participation and productivity contribute to economic losses within communities and health systems. Indirect costs, including complications during pregnancy and long-term disability, further increase healthcare expenditures and limit future economic potential.1,2 Collectively, these effects represent a substantial but often under-recognised burden on already constrained healthcare systems.
5. Management progress over the decades
Over the past two decades, remarkable progress has been made in the management of SB within low-income regions, particularly in Africa. The International Federation for Spina Bifida and Hydrocephalus (IF), an international organisation, has played a pivotal role in improving the quality of life for individuals with SB in developing countries, with a particular focus on Africa. In addition to providing comprehensive training programs to healthcare professionals to augment their skills and knowledge, the IFSBH has established a network of member organisations dedicated to SB. These organisations include the Festus Fajemilo Foundation, the Spinal Bifida and Hydrocephalus Association in Nigeria (SBHAN), the ReachAnother Foundation in Ethiopia, and the Waad Spina Bifida Foundation in Egypt. Through a collaborative partnership, these entities have made significant strides in improving the well-being of individuals living with SB in their respective countries. 38 Among these organisations, the ReachAnother Foundation in Ethiopia has made significant contributions. Recent reports indicate that these organisations have made provisions for life-saving surgeries of 5,000 Ethiopian babies with SB and hydrocephalus. 15
Similarly, the Festus Fajemilo Foundation in Nigeria has made significant strides in advocating for adolescents with spina bifida and hydrocephalus (SBH). Through training initiatives, 94 guidance counselors and 5 school administrators were equipped with the knowledge and skills necessary to support individuals with SBH, thereby altering perceptions and improving decision-making regarding their enrollment. Additionally, the foundation conducted five advocacy visits to relevant state agencies, organised a press conference, stakeholder meetings, and a peaceful protest at the governor’s office to advocate for SBH rights. Their Breaking All Barriers project targeted reducing discrimination against adolescents with disabilities, including SBH. 39
In addition to local initiatives addressing SB management challenges in Africa, the use of telemedicine and smartphone applications has seen a rapid rise, with smartphone usage for telemedicine consultations increasing annually for neurosurgical conditions such as SB in Africa. 40 Furthermore, international neurosurgical centres such as the Rabat Training Centre have enabled the training of more than 58 neurosurgical candidates from approximately 18 countries in Sub-Saharan Africa, including 30 neurosurgeons, with many returning to establish patient-care and training centres. 41 These endeavours demonstrate tangible progress in overcoming neurosurgical conditions such as SB management obstacles, showcasing innovative solutions and collaborative efforts in the region.
Recent studies have demonstrated a decrease in the incidence of SBs in recent years, which underscores the significant impact of collaborative efforts by the international community and government partnerships. 42 These achievements have been realised through the establishment of additional SB management centres, the training of healthcare professionals, the adoption of an MDT approach, the provision of nutritional counselling, the facilitation of cost-free surgical care, the implementation of awareness campaigns, and the introduction of various other initiatives.15,38
6. Strategies for improving SB management outcomes in Africa
The strategies below are presented in an order that broadly reflects the interrelated barriers identified above, moving from health system capacity and access to awareness, evidence generation, and prevention.
6.1. Enhancing education and awareness for SB prevention in Africa
In the short-to medium-term, enhancing education and awareness represents a cost-effective strategy for prevention and early intervention. To do this, it is important to engage various stakeholders in public initiatives. Medical professionals, paediatric surgical associations, hospitals, faith communities, and parents play a crucial role in raising awareness regarding neonatal surgical concerns, drug use, and naturopathic medicine. 24 Their active involvement in community outreach programs, workshops, symposia, meetings, and the distribution of educational materials can effectively disseminate knowledge on SB and its prevention.
In regions where traditional birth attendants play a significant role in childbirth, it is crucial to provide them with training in identifying neonatal surgical conditions, including SB. This training enables timely recognition of potential issues and prompt referral to healthcare facilities capable of managing neonatal surgical cases. Integrating traditional birth attendants into the healthcare system expands the reach of SB awareness and early intervention efforts.
Addressing cultural concerns and improving neonatal surgical care in Africa requires the promotion of health education, access to contraception, pre-pregnancy counselling, and obstetric care. By providing comprehensive reproductive healthcare services, the incidence of preventable birth defects, such as SB, can be reduced. Additionally, promoting the fortification of food with folic acid can have a significant impact on reducing the prevalence of the condition.11,43,44
6.2. Improving healthcare infrastructure and resources for improved outcomes in SB care
To improve the healthcare infrastructure and allocate resources effectively to achieve improved outcomes in SB care, several key measures could be implemented. Firstly, healthcare providers should prioritise vigilance during the critical initial 24 hours of a newborn’s life and establish robust follow-up programs for early detection and continuous care. Additionally, it is crucial to establish a comprehensive network for post-treatment care involving MDTs and support services.43,45 The incorporation of neonatal surgical training and telemedicine can significantly improve access to care, particularly in remote areas where resources may be limited. 45 Moreover, providing regular training programs for healthcare professionals is vital to ensuring that their skills and knowledge remain up-to-date and aligned with best practices.
To ensure effective care for individuals with SB, it is important to prioritise the establishment of dedicated facilities for neonatal surgery, including well-equipped Neonatal Intensive Care Units (NICUs) staffed by trained professionals. 45 Centralising services at regional or specialised children’s hospitals can improve access to specialised care, particularly in areas where dedicated facilities may be scarce. Encouraging the establishment of specialised children’s hospitals in countries that currently lack such facilities can further increase the quality and accessibility of care for individuals affected by SB. 45
6.3. Improving research and management guidelines for SB
In the medium-to long-term, strengthening research capacity and developing context-specific guidelines are essential to address existing knowledge and practice gaps. Firstly, the establishment of registries to maintain accurate records related to antenatal care, births, and mortality is essential to facilitate a comprehensive understanding of SB within the region. 46 Moreover, integrating surgical care within child health programs and determining its specific role based on evidence-based and cost-effective approaches is crucial.
Developing national guidelines specific to SB management and care can provide a standardised framework for healthcare providers across the continent. These guidelines should encompass best practices for the diagnosis, treatment, and long-term management of SB while taking into consideration local resources and cultural nuances. Additionally, enforcing legislation to ensure the availability of essential healthcare services for individuals affected by SB can help address disparities and improve overall care provision.
6.4. Adopting established healthcare frameworks to improve SB care
Adopting established healthcare frameworks could play a pivotal role in the management of SB in the region. As outlined before, SB management is prone to several challenges and integrating a comprehensive framework like International Classification of Functioning, Disability and Health (ICF) could offer set guidelines on navigating its treatment across the continent. 12 For this purpose, the ICF model recognises the multidimensional nature of disability, encompassing not only impairment but also activity limitations, participation restrictions and environmental influences. 12 This holistic perspective is crucial in the context of SB, where individuals face issues that extend beyond physical limitations.
In the context of SB specifically, ICF’s universality principle ensures that its application is not limited by health conditions or cultural contexts.
47
In Africa, where diverse cultures and healthcare systems exist, this facilitates a standardised approach to SB management, enabling effective communication and comparison of data across regions. Similarly, by emphasising functioning over specific health conditions, the ICF promotes parity and aetiological neutrality.
47
This is particularly relevant in SB management, where individuals have varying degrees of impairment. By focusing on functioning and participation, rather than diagnosis alone, the ICF ensures equitable treatment and care. Furthermore, the ICF’s recognition of environmental factors on functioning allows for addressing barriers and facilitators in SB management.
48
In Africa, where environmental factors such as accessibility, stigma and socioeconomic status can significantly impact individuals with SB, this aspect of the ICF is particularly relevant. The application of the primitive ICF model for SB management within the African context is elucidated in Figure 3. Application of the primitive ICF model for SB management in the African context, showing how environmental, social, and individual factors influence care and outcomes.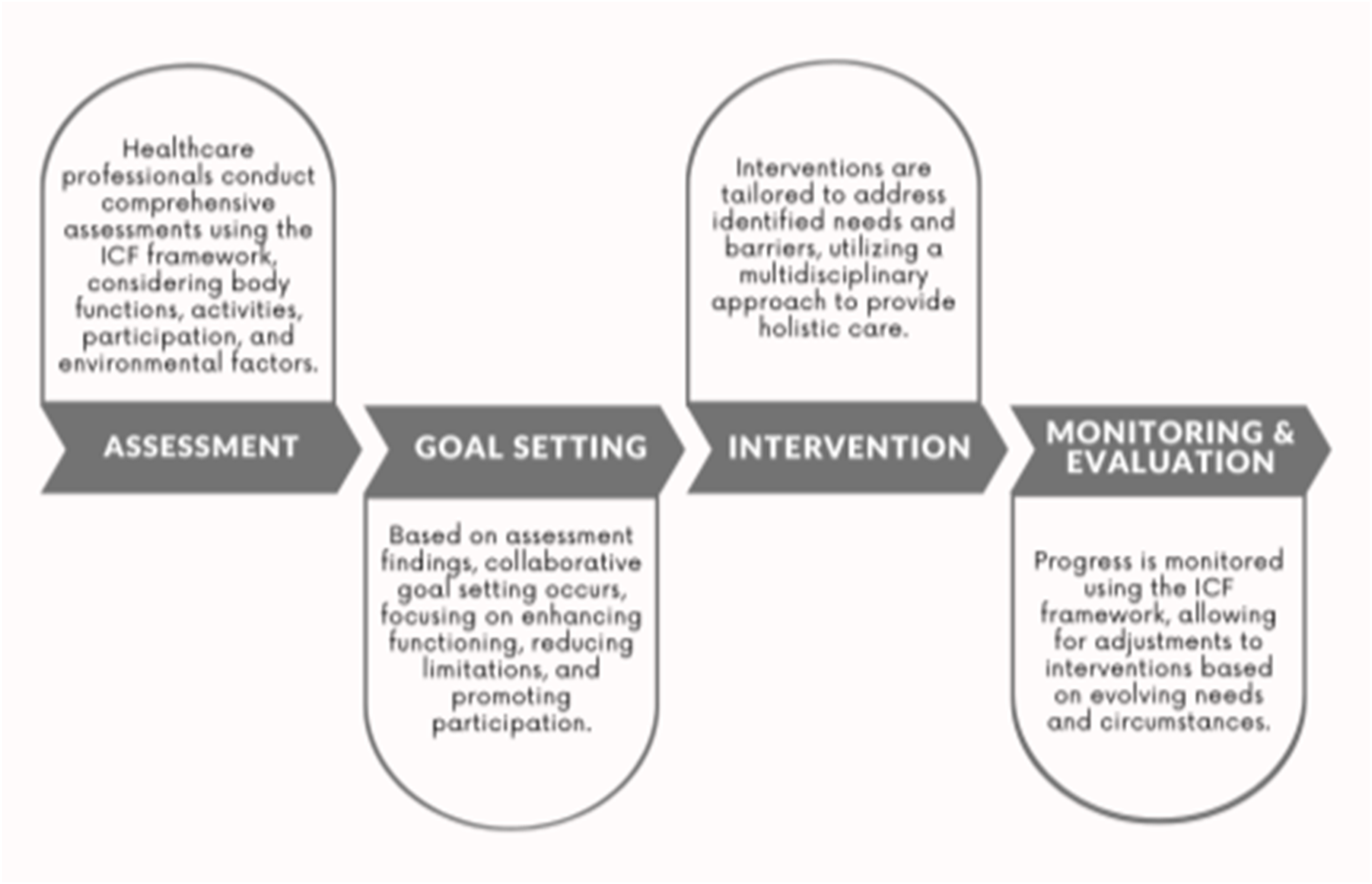
Aligned with the Institute for Healthcare Improvement (IHI) Triple Aim goals – population health, patient experience, and cost-effectiveness – is a structured approach to enhance healthcare delivery and outcomes. 49 Improving population health involves promoting wellness, preventing disease, and addressing health disparities within the community. 49 In the context of SB, initiatives such as comprehensive prenatal screening programmes and community-based education campaigns are pivotal. 50 These efforts aim to decrease SB incidence through preventative measures like folic acid supplementation and promote healthy lifestyles for individuals with the condition. Enhancing patient experience ensures care is respectful, responsive, and individualised, empowering individuals with SB to participate actively in their care plans. 51 This fosters autonomy and dignity while addressing emotional and informational needs. Optimising costs involves implementing evidence-based practices, utilising telemedicine, and investing in preventive care. 52 Standardising protocols, streamlining workflows, and reducing variations in practice ensure efficient and judicious resource utilisation.
6.5. Improving efforts on food micronutrient fortification to improve SB care
As a high-impact, long-term preventive strategy, scaling up food micronutrient fortification is critical to reducing SB incidence. This process which involves the adding of essential vitamins, minerals, or other nutrients to food to improve nutritional content, is crucial for the prevention of SB in Africa. The adoption of preventive measures outlined by international organisations such WHO should be mandatorily implemented. Preventive measures, like large-scale food fortification (eg., Folic acid supplementation) have been proven as a powerful, evidence-informed, and cost-effective intervention to combat the congenital conditions such as SB. 53
To maximise adoption of food fortification strategies in Africa, concerted efforts are essential at multiple levels. Governments could play a crucial role by implementing policies mandating fortification of staple foods (eg., wheat, rice, maize) and ensuring compliance with quality standards. In fact, a study by Atta et al. has demonstrated that mandatory fortification of staple foods effectively reduced live births prevalence of SB to 0.3 cases per 1,000 births in countries that have implemented food fortification effectively. 54 This underscores the unending possibilities in preventing this debilitating condition.
Furthermore, partnerships between governments, NGOs, the private sector, and organisations such as the Global Alliance for Improved Nutrition (GAIN), the United Nations International Children’s Emergency Fund (UNICEF), and Food Fortification Initiative (FFI) are vital.14,55–59 These partnerships provide technical support, resources, and advocacy for food fortification programs, ensuring their effectiveness and sustainability. By working together, stakeholders can promote widespread adoption of food fortification strategies, ultimately reducing the incidence of SB and improving public health outcomes in Africa.14,55–59 The strategies aimed at enhancing SB management outcomes in Africa are delineated in Figure 4. Strategies to improve SB management outcomes in Africa, highlighting improvements in healthcare, education and awareness, and research and guidelines.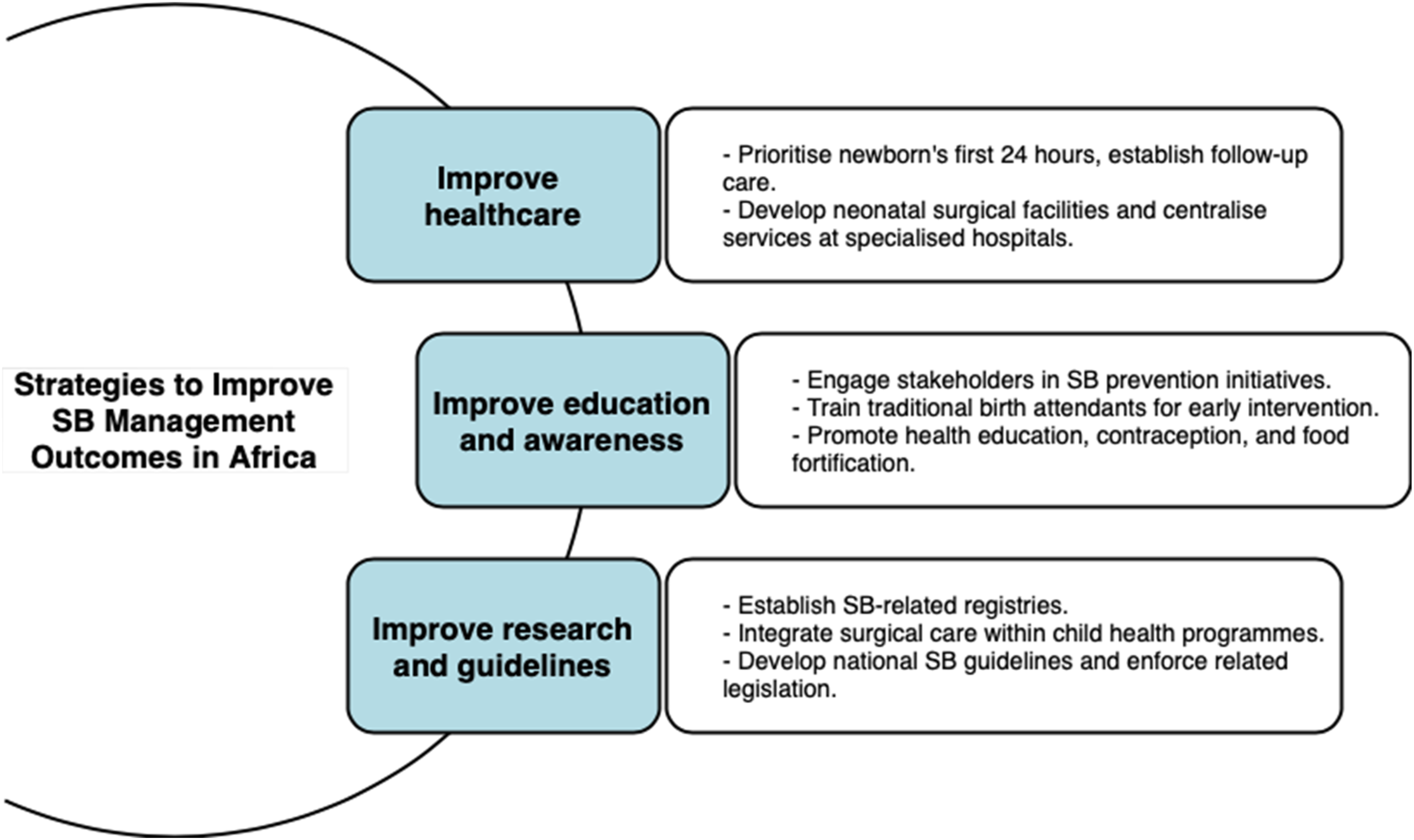
Importantly, the feasibility and impact of these strategies will vary across sub-regions and should be adapted to local health system contexts.
7. Limitations
This paper, while striving to offer a comprehensive overview of SB management, is inevitably constrained by several limitations. One limitation of this review is the complexity of the African context itself, which encompasses a wide range of cultural differences across its regions. These cultural variations influence healthcare practices, attitudes towards disabilities, access to medical services, and societal perceptions of conditions like SB. Therefore, it’s crucial to acknowledge that interventions and strategies must be tailored to accommodate these diverse cultural perspectives and practices when addressing SB management in Africa.
Another limitation lies in the reliance on available literature and data related to SB management. The quality, completeness, and reliability of these sources vary, potentially impacting the accuracy and robustness of the analysis. Moreover, the authors’ backgrounds, experiences, and biases may subtly influence the perspectives and interpretations presented in the paper, despite efforts to maintain objectivity. Furthermore, our paper does not extensively explore methodological considerations or feasibility of implementing proposed strategies, leaving room for future research to understand these aspects and assess their practical implications. Additionally, the predominance of English language sources may inadvertently exclude valuable information and perspectives from researchers unable to publish in English-language journals, thereby limiting the paper’s inclusivity. We also acknowledge significant data sparsity and uneven regional representation, which limits the generalisability of findings across diverse African sub-regions and settings.
8. Conclusion
In conclusion, the management of SB in Africa faces significant challenges, including limited awareness and education, barriers to healthcare access, and financial constraints. These factors hinder timely diagnosis and the provision of appropriate care for individuals affected by SB. It is imperative to address these gaps and implement targeted strategies to improve outcomes and ensure equitable access to care for affected individuals. Collaborative efforts are essential in strengthening healthcare infrastructure, enhancing education and awareness initiatives, and overcoming socioeconomic obstacles that impede effective SB management in Africa.
Footnotes
Acknowledgments
We acknowledge the Icormed Research Collaborative for providing the platform to conduct this project.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
No additional data is available.