
Abstract
Background
Women with elevated cardiovascular and systemic risks face major contraindications to combined hormonal contraceptives (CHCs). In humanitarian settings, limited healthcare access may lead to overreliance on CHCs. This study assessed the prevalence and predictors of CHC ineligibility among Syrian refugee women in Lebanon.
Methods
A cross-sectional survey was conducted with 105 current CHC users aged 18–50 years, extracted from a larger cohort. Sociodemographic, clinical, and reproductive data were analyzed using the WHO Medical Eligibility Criteria (MEC). Univariate and multivariable logistic regression identified predictors of MEC Category 3–4 ineligibility.
Results
Nearly half of the women (44.8%) were classified as MEC Category 3–4, indicating substantial risk. Migraine with aura was the most frequent comorbidity (25.7%), followed by migraine without aura (6.7%) and gallbladder disease (6.7%). In univariate analysis, age ≥ 35 years (UOR = 2.77, p = 0.01), residence in Mount Lebanon (UOR = 4.88, p = 0.001) or North Lebanon (UOR = 4.15, p = 0.001), and specific comorbidities were significantly associated with ineligibility. In multivariable analysis, only migraines with aura remained an independent predictor (AOR = 4.684, p = 0.04), suggesting high-risk clinical indicators are often overlooked during provision.
Conclusion
High ineligibility highlights deficiencies in contraceptive screening in humanitarian contexts. Routine MEC-based assessments, and safer alternatives are urgently needed.
Innovation and limitations
This study uniquely applies the WHO safety framework to a displaced population, revealing migraine with aura as a major safety barrier. Limitations include a cross-sectional design and reliance on self-reported medical data.
Keywords
Introduction
The severe disruption caused by forced displacement often deprives individuals of fundamental rights and healthcare access. 1 For women in humanitarian crises, this is especially significant, leading to limited access to essential reproductive health services, including contraception. 2 Oral contraceptive pills (OCPs) remain a cornerstone of family planning, empowering women to control their reproductive lives and contributing to improved maternal and child health outcomes.3,4
The World Health Organization (WHO) developed the Medical Eligibility Criteria (MEC) for contraceptive use, a globally recognized framework that ensures individuals receive the safest contraceptive options based on their health conditions. 3 The MEC categorizes health status from Category 1 (no restriction) to Category 4 (unacceptable health risk if the method is used). 3 This framework has become indispensable for clinicians and public health authorities worldwide.3,5
Despite their importance, these guidelines are inconsistently applied in humanitarian settings. 6 A central concern is the unsafe prescription of combined hormonal contraceptives (CHCs) to vulnerable women, such as Syrian refugees, due to fragmented healthcare systems and inadequate screening, which heightens preventable cardiovascular and systemic risks. 7
Syrian refugee women, exposed to prolonged conflict and displacement, face compounded vulnerabilities. They encounter fragmented healthcare, heightened exposure to risk factors, and intersecting social, economic, and cultural barriers to health-seeking behavior.7–9 Evidence shows that conflict-affected populations have reduced access to contraceptives and severely constrained financial resources.10,11
While family planning is acknowledged as a priority in crisis contexts, reproductive health services remain insufficient, and literature addressing these gaps is limited.8,12,13 Research largely emphasizes contraceptive prevalence or barriers such as economic hardship, lack of awareness, cultural restrictions, and communication challenges. 14 Although some studies discuss refugee women’s general obstacles to contraceptive use, such as fear of side effects or partner disapproval, few investigate contraceptive safety using a comprehensive WHO MEC assessment.14,15
Furthermore, the decision to use contraception should be a shared responsibility with the partner, emphasizing the importance of integrating male-focused clinical and cultural approaches into family planning strategies. 16 Moreover, implementing evidence-based guidelines like the MEC in low-resource settings is hampered by systemic and individual challenges. 17
This study addresses this gap by assessing OCP users among Syrian refugee women in Lebanon according to the WHO MEC. Our aim is to provide empirical evidence on the safety and appropriateness of OCP use in this population, highlight contraindications, and identify demographic and health characteristics associated with higher MEC categories. The findings can guide reproductive health services for displaced populations, ensuring contraception is not only accessible but also safe.
This study introduces a novel focus on the clinical safety of contraceptive methods within displaced populations through the application of the WHO MEC framework. A distinct methodological benefit is the use of this standardized, globally recognized tool to assess high-risk clinical markers, particularly migraine subtypes, that frequently go undiagnosed in humanitarian settings. However, the main disadvantage is the study’s reliance on self-reported medical history, which may be subject to recall bias in the absence of clinical records. By identifying these gaps, this research provides a practical pathway for safer prescribing patterns in crisis settings.
Methodology
Study design
This analysis is part of a larger exploratory, descriptive, survey-based project conducted between November 2023 and March 2024. It focuses on a subset of 105 married Syrian refugee women aged 18–50 years who were identified as OCP users, drawn from the full sample of 790 participants. Data were collected through face-to-face interviews conducted by trained female field workers.
Study setting and sampling technique
The main study was carried out in four Lebanese governorates—Beirut, Bekaa, South, and North Lebanon. A total of 790 participants were initially approached and interviewed for the broader maternal health project. From this larger group, a specific subset of 105 women who reported current use of combined oral contraceptives (COCs) was extracted for this analysis. Participants were selected proportionately based on the United Nations High Commissioner for Refugees’ (UNHCR) refugee registers. Proportionate cluster sampling ensured geographic representativeness. Within each cluster (e.g., camps, informal settlements, and urban neighborhoods), households were approached through convenience sampling due to the absence of household registries and security constraints. Recruitment took place at multiple sites, including homes, healthcare centers, and workplaces.
Because the data collection relied on face-to-face interviews, only those who successfully completed the interview were included in the final analysis, ensuring no missing data for the variables studied. The inclusion and exclusion criteria for this study were as follows:
Inclusion criteria
Married Syrian refugee women aged 18–50 years who were current users of combined oral contraceptives at the time of the interview.
Exclusion criteria
Women who were currently pregnant or who declined to provide oral consent for participation.
Questionnaire revision and pilot testing
The main study’s questionnaire underwent expert validation and pilot testing to ensure clarity, relevance, and cultural appropriateness. This analysis relied on data extracted from that validated tool.
Data protection and ethical considerations
This study represents a targeted analysis of a subset of 105 women extracted from a larger cohort of 790 participants enrolled in a broader maternal health project. The study protocol was approved by the Institutional Review Board (IRB) of Beirut Arab University (IRB Code: 2025-H-0105-P-P-0713) and conducted in accordance with the Declaration of Helsinki. Permission to access refugee camps was obtained from the Lebanese Army Intelligence Directorate and local municipalities. Study objectives were explained to participants, and oral consent was obtained to ensure voluntary participation and anonymity, given concerns about legal implications in refugee contexts. Participants could withdraw at any time.
Statistical analysis
Data were analyzed using SPSS version 24. Continuous variables were summarized as means ± standard deviations, while categorical variables were expressed as frequencies and percentages.
Univariate analyses examined associations between participant characteristics and ineligibility for OCP use (MEC Categories 3–4). Pearson’s chi-square test or Fisher’s exact test was applied, as appropriate. Variables with p < 0.2 were included in a multivariable logistic regression model. Predictors were assessed for multicollinearity (variance inflation factors [VIF] < 2.5). Confounders were retained if they altered coefficients by > 10%. Model fit was evaluated using the Hosmer-Lemeshow test. Adjusted odds ratios (AORs), 95% confidence intervals (CIs), and p-values were reported.
Questionnaire and data source
The structured questionnaire was designed after a review of the related literature.10,13,18,19 It collected sociodemographic data (age, education, employment, income, and household size), reproductive history (parity, breastfeeding, and smoking), contraceptive practices, and medical history. It was developed in English, reviewed by public health and pharmacy experts, translated into Arabic, and back-translated. Pilot testing with eight participants confirmed clarity and cultural appropriateness. Eligibility for OCPs was assessed using the following WHO MEC categories: • Category 1: No restriction • Category 2: Benefits outweigh risks • Category 3: Risks outweigh benefits • Category 4: Unacceptable health risk
Common self-reported conditions included hypertension, cardiovascular disease, migraine with or without aura, liver or gallbladder disease, and rheumatoid arthritis. These, alongside sociodemographic factors, were used to determine OCP eligibility.
Data handling
All questionnaires were reviewed for completeness during interviews. Clarifications were obtained immediately, eliminating missing data and the need for imputation.
Results
Sociodemographic and clinical profile of CHC users
The analysis included 105 current CHC users with a mean age of 31.25 years (SD ± 6.95; range: 18–50). The majority were aged 30–34 years (31.4%) and 35–39 years (22.9%). Most participants resided in North Lebanon (29.5%), South Lebanon (26.7%), and Beirut (23.8%). Nearly 70% (69.5%) lived in rented accommodations. The mean household size was 7.09 individuals (SD ± 2.997), with half of the participants (50.5%) living in households of 6–10 members, 38.1% in households of 5 or fewer, and 11.4% in households with more than 10 members.
Participants had lived in Lebanon for an average of 8.95 years (SD ± 4.73), with half (50.5%) residing there for 6–10 years. Regarding education, 83.8% had attended school, while 13.3% had never attended. Most women (89.5%) were unemployed, while almost all husbands (92.4%) were employed. The primary sources of household income were wages (93.3%), food vouchers (62.9%), and informal debt (58.1%). The average monthly household income was mostly between $151 and $300 (57.2%).
Participants’ sociodemographic data (N = 105).
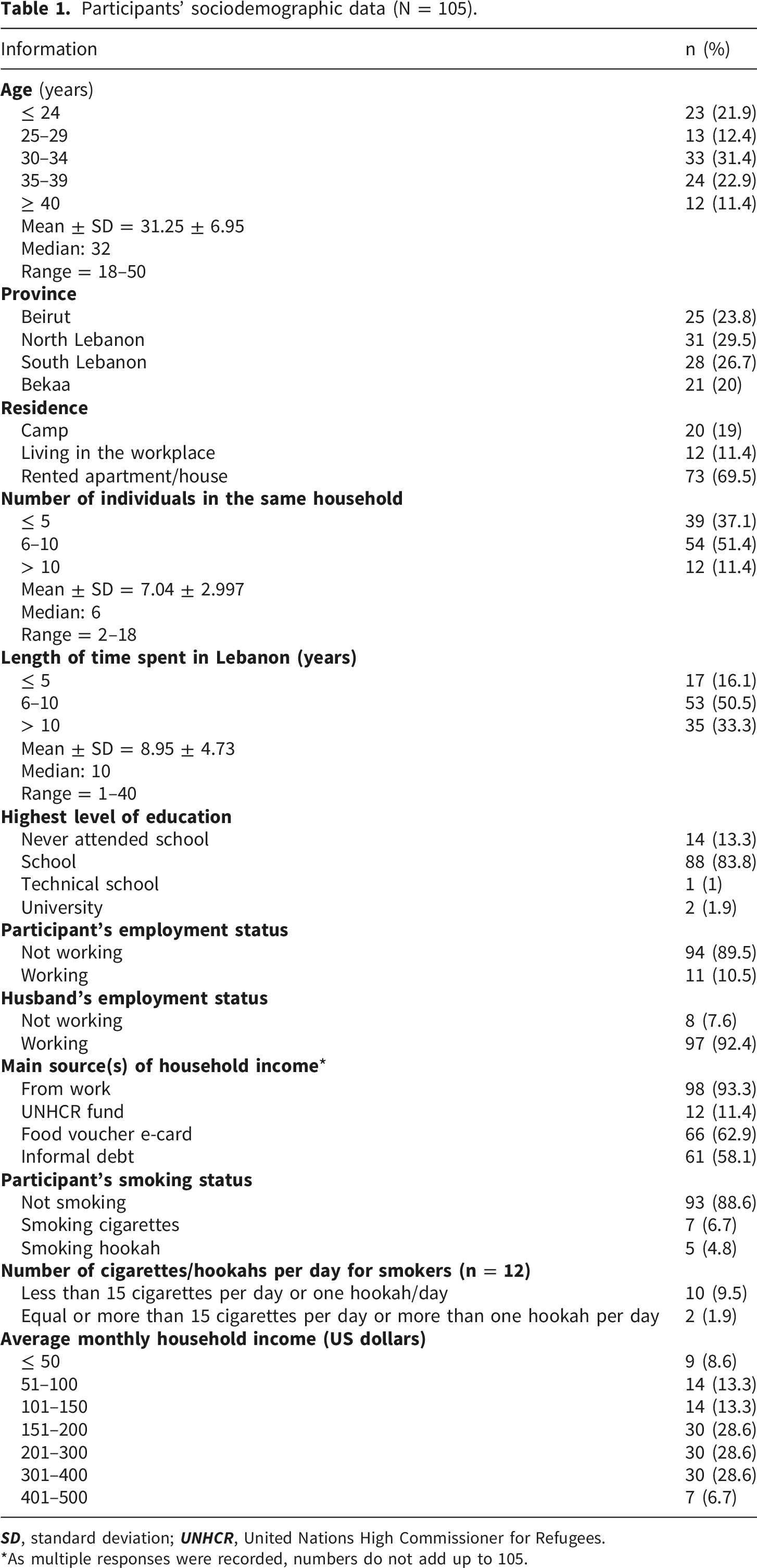
*As multiple responses were recorded, numbers do not add up to 105.
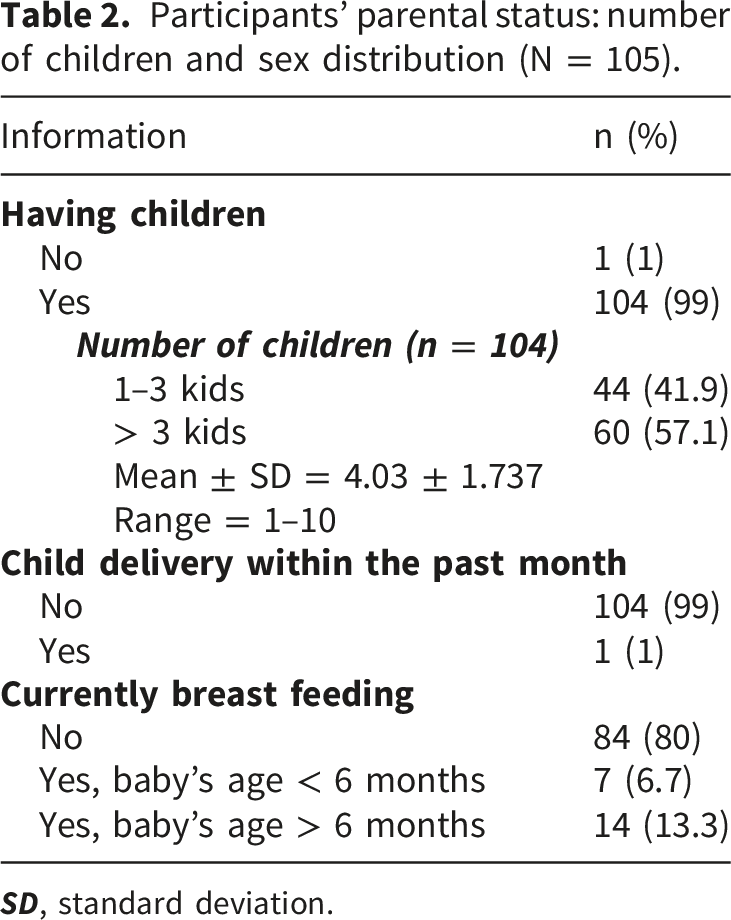
Participants’ parental status: number of children and sex distribution (N = 105).
Primary source of information about contraception methods (N = 105).
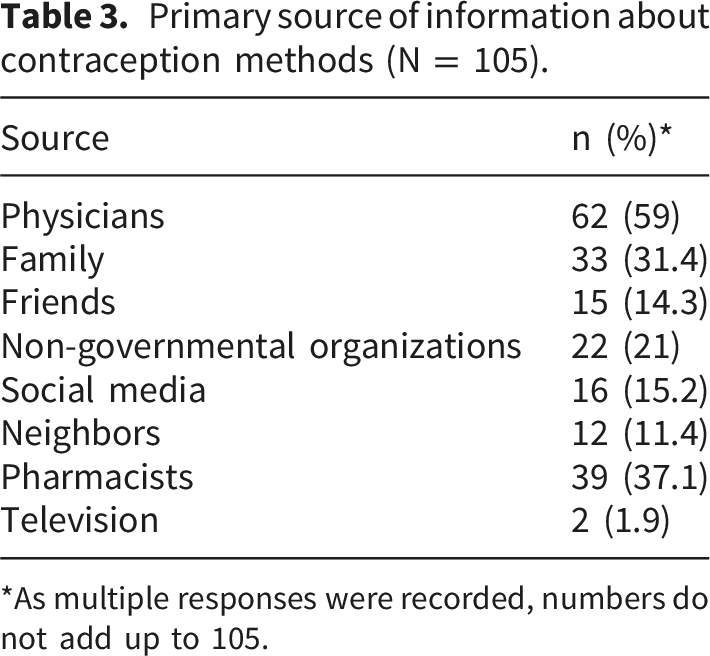
*As multiple responses were recorded, numbers do not add up to 105.
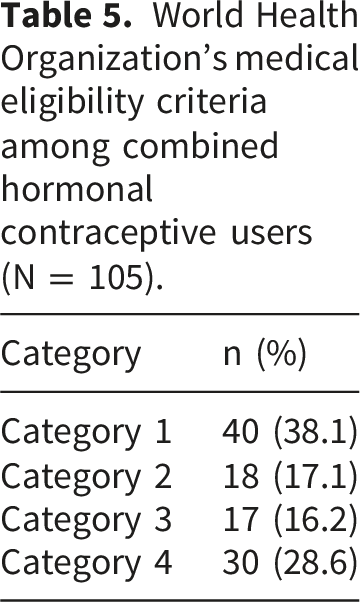
Prevalence of CHC ineligibility and WHO MEC classification
Medical comorbidities of combined hormonal contraceptive users (N = 105).
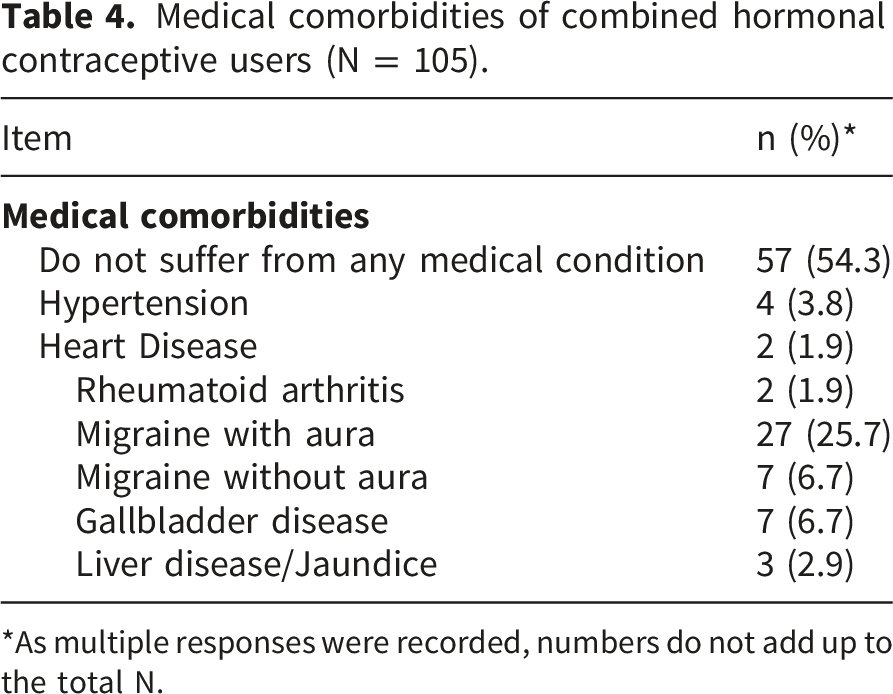
*As multiple responses were recorded, numbers do not add up to the total N.
World Health Organization’s medical eligibility criteria among combined hormonal contraceptive users (N = 105).
Predictors of medical ineligibility for CHC use
Univariate analysis of predictors associated with ineligibility for combined hormonal contraceptive use (N = 105).
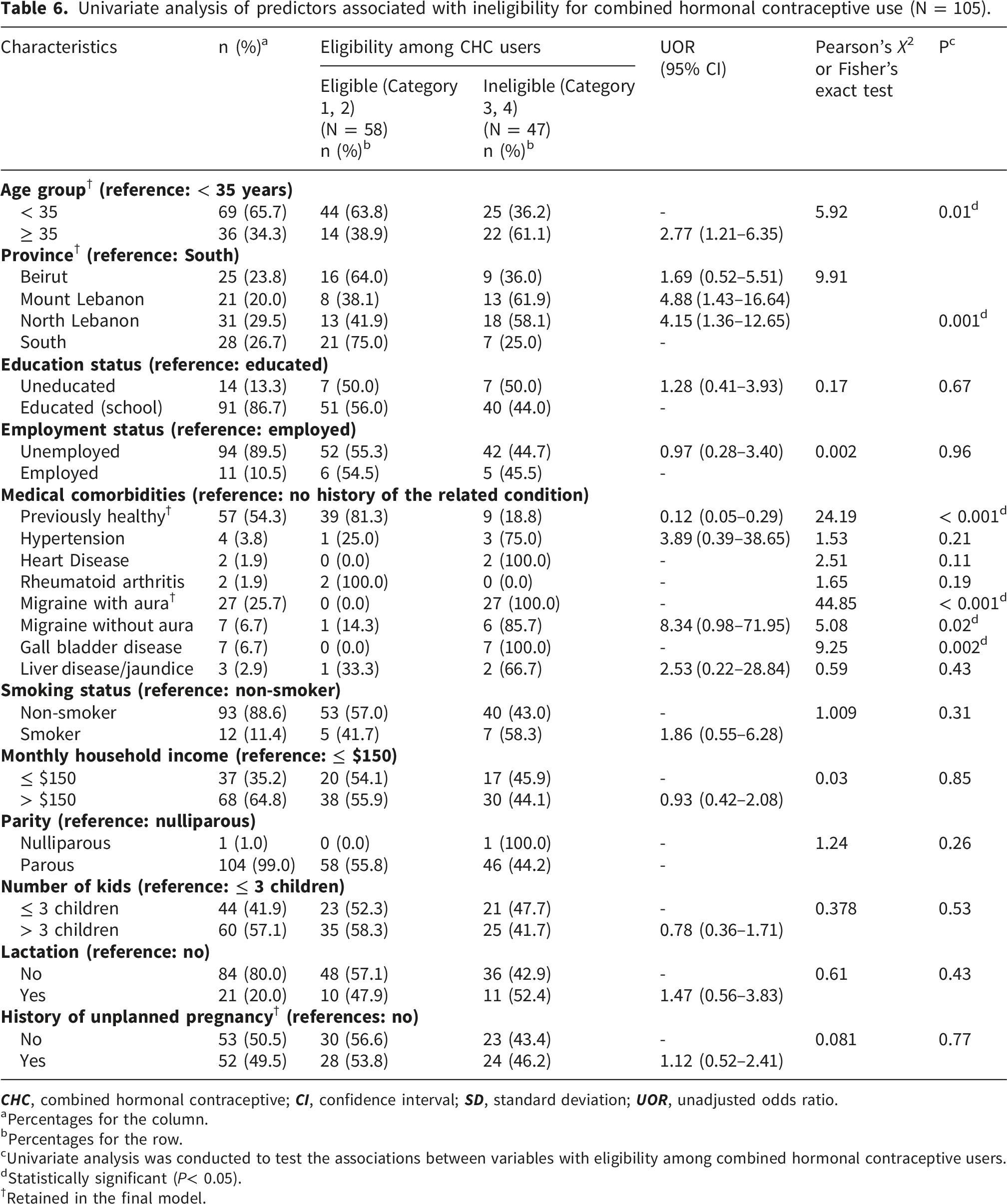
aPercentages for the column.
bPercentages for the row.
cUnivariate analysis was conducted to test the associations between variables with eligibility among combined hormonal contraceptive users.
dStatistically significant (P< 0.05).
†Retained in the final model.
Multivariable Logistic regression analysis a of the significant predictors of ineligibility for combined hormonal contraceptive use.
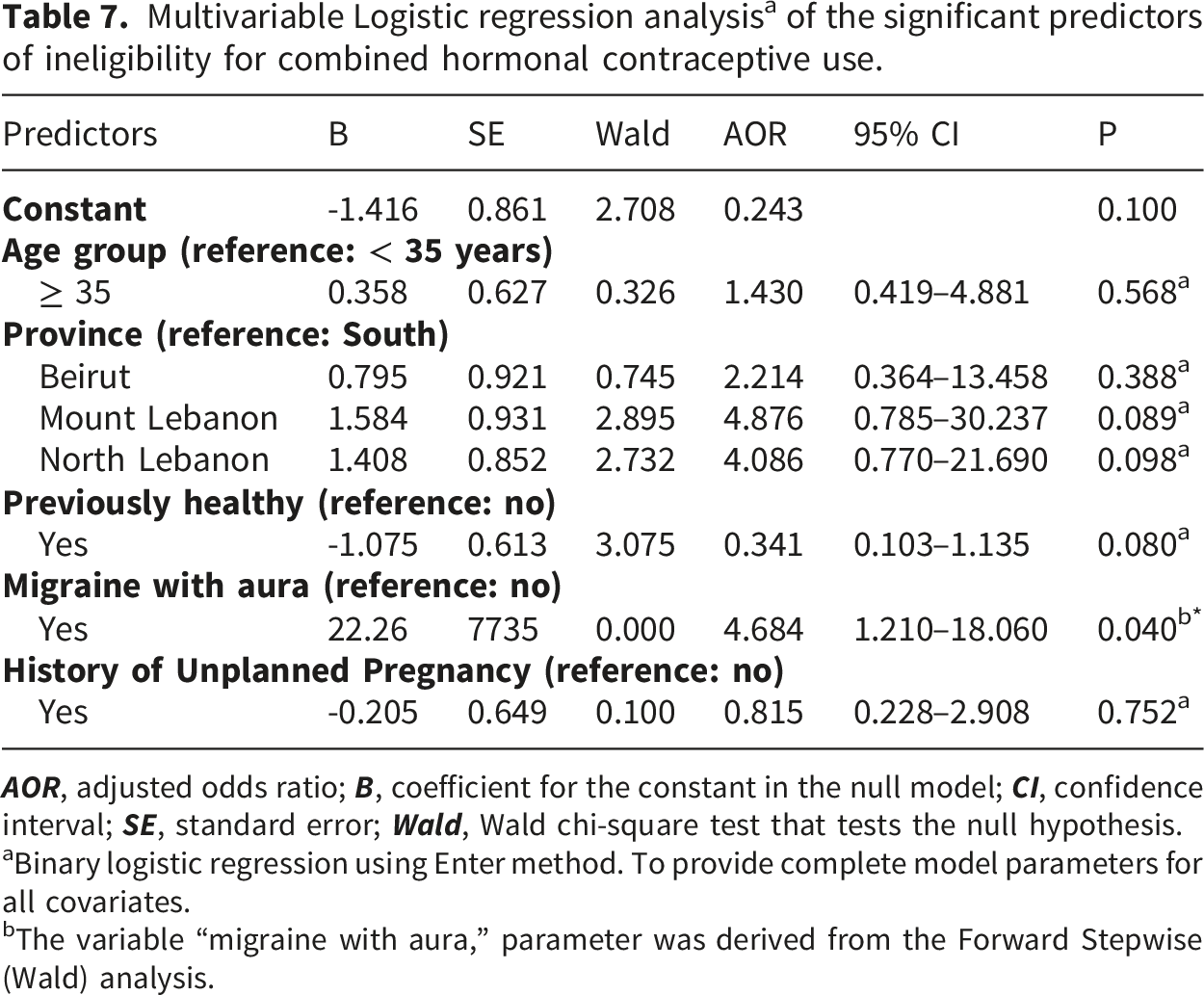
aBinary logistic regression using Enter method. To provide complete model parameters for all covariates.
bThe variable “migraine with aura,” parameter was derived from the Forward Stepwise (Wald) analysis.
Discussion
Prevalence of CHC ineligibility and WHO MEC classification
This study found that nearly 45% of Syrian refugee women using combined hormonal contraceptives (CHCs) were classified as Category 3 or 4 under the WHO Medical Eligibility Criteria (MEC), indicating substantial or unacceptable health risks. This prevalence is markedly higher than global estimates, where CHC ineligibility among screened populations typically ranges from 5% to 15%.3,5 Such a discrepancy underscores critical gaps in contraceptive counseling and eligibility screening. These shortcomings are even more concerning in humanitarian contexts, where resources are scarce, healthcare provider training is inconsistent, and contraceptive options are limited. 6
Predictors of medical ineligibility for CHC use
Medical conditions such as migraine with aura, hypertension, and hepatic or gallbladder disease are well known to increase the likelihood of adverse events among women using estrogen-containing contraceptives.20,21 Migraine with aura, in particular, is strongly associated with an increased risk of ischemic stroke in CHC users.20,22 In this study, migraine with aura was the only independent predictor of CHC ineligibility (AOR ≈ 4.7, p = 0.04). This finding aligns with WHO guidelines and previous research.3,5,23 Alarmingly, all women reporting this condition were still using CHCs, highlighting a significant gap in safe prescribing practices. Importantly, this contraindication could have been identified through a simple clinical history during patient interviews.24,25 Other factors, such as age ≥ 35 years, residence in Mount or North Lebanon, migraine without aura, and gallbladder disease, were significantly associated with ineligibility in univariate analysis but lost significance in multivariable models, possibly due to confounding effects. The absence of a strong adjusted association for gallbladder disease is consistent with evidence suggesting that, while CHCs modestly increase gallbladder risk, the overall clinical impact may be limited. 21
The impact of migraine with aura and clinical risk factors
The emergence of migraine with aura as the main independent predictor of ineligibility aligns with the pathophysiology showing that estrogen-containing contraceptives significantly increase the likelihood of ischemic stroke in this subgroup. 26 Migraine with aura is considered a complex vascular condition involving cortical spreading depression, which, when combined with the prothrombotic effects of ethinyl estradiol, generates a synergistic effect that increases the risk of cerebrovascular accidents. 27 In our study, the alarming rate of ineligibility among female refugees with this condition reveals a major clinical oversight. Moreover, social and economic factors in humanitarian settings additionally aggravate this risk profile. Refugee women frequently experience chronic stress and malnutrition, which can increase the frequency and severity of migraine.28,29 Furthermore, the lack of affordable specialized care means that these neurological subtypes are often underdiagnosed, consequently leaving women to rely on CHCs without screening. 30 Additionally, the normalization of severe headaches and their consideration as life stressors may lead women to underreport symptoms during general health visits. 31
Clinical implications for humanitarian settings and screening practices
These findings highlight the urgent need for routine MEC-based screening in contraceptive counseling. In humanitarian settings, where literacy and resource limitations prevail, simplified tools such as pictorial checklists could be invaluable. For example, an image of a brain with flashing lights could symbolize migraine with aura, improving both patient and provider understanding. Role-play or storytelling (e.g., “Fatima has severe headaches with flashing lights—this means she should not take this pill”) could also personalize risk and enhance recall.
Equally important is expanding access to safer alternatives, including progestin-only pills, injectables, implants, and non-hormonal methods. Without a broader contraceptive method mix, women with contraindications risk being left without safe and viable options.6,32,33
Improving provider education is critical. Training community health workers (CHWs) and midwives to use simplified MEC tools, such as the WHO MEC wheel or pictorial aids, can help ensure safer prescribing. 33 At the same time, community-level education should empower women to understand risks and benefits, facilitating informed choices. This is particularly important in refugee settings, where stigma, misinformation, and partner influence often restrict method switching. 12
In contrast to high-resource healthcare systems, such as in the United States—where only 6% of CHC users were found to have contraindications under proper screening5,34—our findings illustrate the heightened vulnerabilities of displaced populations. Similar trends have been observed in South Sudan and Bangladesh, where inappropriate contraceptive use was linked to limited training among healthcare workers and restricted contraceptive availability. 33 By recognizing migraine with aura as a key clinical marker, this study provides a practical pathway for improving contraceptive safety in humanitarian contexts. 22
In summary, nearly half of the Syrian refugee women interviewed were using combined hormonal contraceptives despite having medical contraindications. The link between migraine with aura and medical ineligibility, exacerbated by diagnostic normalization and easy access to CHCs, underscores the need for a drastic change in how reproductive health services are delivered to vulnerable displaced populations. Future perspectives should emphasize the integration of simplified, WHO-based screening tools during pharmacy dispensing. Moreover, broadening the available contraceptive inventory to include non-hormonal and progestin-only options is essential to guarantee that the essential right to family planning does not compromise cardiovascular safety.
Study limitations
This study is among the few to evaluate the medical eligibility of CHC use among Syrian refugee women in a humanitarian setting using the WHO MEC as a standardized framework. While the findings provide valuable insights, several limitations should be acknowledged.
First, the analysis relied on secondary data drawn from a larger survey, which restricted the variables and definitions to those previously collected. Second, the cross-sectional design prevents any causal inference between the identified predictors and ineligibility. Third, medical conditions such as migraine subtypes and chronic illnesses were self-reported rather than clinically confirmed, which may have introduced recall and misclassification bias. Another limitation concerns the relatively small number of CHC users included in this subset, which may have reduced the statistical power to detect associations, particularly for less frequent comorbidities. Finally, some medical conditions relevant to CHC eligibility may have been underdiagnosed or unreported due to limited healthcare access, which could have led to an underestimation of the true ineligibility rates.
While acknowledging the limitations mentioned, this study reveals several strengths. It provides rare, firsthand clinical data on the safety of contraceptive use among Syrian refugee women in Lebanon, a community often overlooked. Moreover, the use of the WHO MEC as a standardized assessment tool allows comparison of our findings with global trends and permits the translation of the findings directly into clinical practice guidelines for humanitarian settings.
Conclusions
Nearly half (44.8%) of the Syrian refugee women in this study who were using CHCs were classified as medically ineligible (WHO MEC Category 3 or 4). This finding reflects significant shortcomings in contraceptive screening and counseling practices within humanitarian settings. Migraine with aura emerged as the sole independent predictor of ineligibility (AOR = 4.684, p = 0.04), emphasizing the importance of routinely assessing this condition before initiating CHCs. The results point to an urgent need for the institutionalization of WHO MEC-based screening, improved access to safer contraceptive alternatives, and strengthened provider and community education. Such measures are essential to safeguard the reproductive health of women living in vulnerable humanitarian contexts.
Beyond the clinical data, this study involves broad multidisciplinary relevance across medicine and clinical pharmacy, as it mandates rigorous screening during the dispensing process; meanwhile, for social and political sciences, it highlights how displacement and economic challenges can normalize serious health risks. Therefore, addressing the gaps identified in this study necessitates a paradigm shift in how we deliver safe, reproductive care worldwide.
Footnotes
Ethical considerations
The study was conducted in accordance with the ethical principles outlined in the World Medical Association’s Declaration of Helsinki. Ethical clearance was granted by the Institutional Review Board (IRB) of Beirut Arab University.
Consent to participate
The study’s objectives and purpose were explained to all participants, and they were informed of their right to withdraw at any stage. Oral consent was obtained to maintain anonymity and ensure voluntary participation, as requesting written consent could have raised concerns about potential legal consequences. Authorization to conduct interviews in camps was secured from the Lebanese Army Intelligence and local municipal authorities.
Author contributions
The authors confirm their contribution to the paper as follows: study conception and design: SK, HMJK, TLM and AEL; data collection: SK; analysis and interpretation of results: SK; draft manuscript preparation: SK, TLM, HMJK and AEL; manuscript copy-editing: HMJK, TLM and AEL. All authors reviewed the results and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset presented in this article is available only upon reasonable request since it contains confidential information. Requests to access the datasets should be directed to the first author (