
Abstract
Background
Neonatal sepsis is a leading cause of neonatal mortality, yet data on its prevalence and associated factors remain limited. This study aimed to assess the prevalence of neonatal sepsis and associated factors among neonates admitted to the neonatal intensive care unit of a university hospital in eastern Ethiopia.
Methods
An institution-based cross-sectional study was conducted on randomly selected neonates admitted to the NICU of Hiwot Fana Comprehensive Specialized Hospital from January 1, 2016 to December 31, 2019. Sociodemographic and feto-maternal data were collected and analyzed using Epi Data 3.1 and Stata 14. Bivariate and multivariate analyses identified factors associated with neonatal sepsis through binary logistic regression, presenting results as adjusted odds ratios (AORs) with 95% confidence intervals (CIs), with statistical significance set at p < 0.05.
Results
Of the 414 neonates included, with a mean age of 3.6 (±2.3 SD) days, 264 (63.7%) were diagnosed with neonatal sepsis. Significant factors associated with neonatal sepsis included; being under seven days old (AOR = 2.18), rural residence (AOR = 1.70), lack of antenatal care (AOR = 0.61), premature rupture of membranes (AOR = 1.66), shorter labor duration (AOR = 0.40), meconium-stained amniotic fluid (AOR = 1.92), birth asphyxia (AOR = 2.25), and neonatal comorbidity (AOR = 1.98).
Conclusion
Nearly two-thirds of NICU-admitted neonates had sepsis, with associations such as age, rural residence, and lack of antenatal care, premature rupture of membranes, shorter labor duration, meconium-stained amniotic fluid, birth asphyxia, and neonatal comorbidity highlighting the need for targeted interventions to improve outcomes.
Introduction
Neonatal sepsis is a clinical syndrome characterized by infection-related signs and symptoms occurring within the first 28 days of life and is a leading cause of neonatal mortality. 1 It can be classified into early-onset sepsis, which occurs within the first 72 hours, and late-onset sepsis, which occurs after 72 hours. 2 Global estimates indicate that infections account for approximately 35% of neonatal deaths, whereas other significant causes include preterm birth (28%), intrapartum-related complications (24%), and asphyxia (23%). 3
In intensive care units, infection rates can reach as high as 30% among highly immature preterm neonates, making bacterial and fungal sepsis leading causes of morbidity and mortality. 4 The World Health Organization (WHO) reported that, in 2017, the incidence of neonatal sepsis ranged from 6.5--38 cases per 1,000 live births globally, contributing to a substantial proportion of neonatal deaths. 5 Neonatal sepsis remains a significant concern in low- and middle-income countries (LMICs), 6 with sub-Saharan Africa reporting that 17% of all neonatal deaths are attributable to this condition, compared with only 6% in developed countries. 7 In Ethiopia, neonatal sepsis is a major cause of neonatal mortality, accounting for more than one-third (33%) of all neonatal deaths. 8
Despite a decline in neonatal mortality from 49 deaths per 1,000 live births in 2000 to 29 in 2016—a 41% reduction over 16 years—neonatal sepsis continues to pose a major public health challenge in resource-constrained environments such as Ethiopia. 9 Limited data are available regarding the prevalence and risk factors for neonatal sepsis, particularly in our study area. Existing studies have identified several common risk factors, including premature rupture of membranes (PROM), maternal urinary tract infections/sexually transmitted infections (UTI/STI), intrapartum fever, foul-smelling amniotic fluid, and an Apgar score of less than 7. 10 Additional factors include being a preterm neonate, receiving resuscitation at birth, and having a maternal history of UTI/STIs. 11
Preventive strategies such as ensuring skilled and clean deliveries, increasing maternal immunization, securing clean umbilical cord cutting, early detection and treatment, and implementing closed medication systems are essential for reducing neonatal sepsis.12,13 Identifying risk factors and initiating timely treatments can significantly lower neonatal mortality and morbidity. 7 Therefore, this study aimed to assess the prevalence and factors associated with neonatal sepsis in the neonatal unit of Hiwot Fana Specialized University Hospital in eastern Ethiopia.
Methods
Study setting and population
An institution-based cross-sectional study was conducted from June 20 to July 19, 2020. The reporting of this study conforms to the STROBE statement 14 (Supplemental File). The study was conducted at Hiwot Fana Comprehensive Specialized University Hospital, located 525 kilometers from the capital, Addis Ababa, in eastern Ethiopia. This hospital serves as the primary referral university hospital affiliated with Haramaya University and houses the only neonatal intensive care unit (NICU) in the region during the study period. The NICU comprises a Kangaroo Mother Care Room and an intensive care unit, with a total of 28 beds. It is staffed by four paediatricians, three NICU nurses, six general nurses, and six medical interns.
Population and sampling
The study population comprised all neonates admitted to the NICU from January 1, 2016 to December 31, 2019. Neonates with incomplete medical records were excluded from the study.
The sample size was determined using both a single and double population proportion formula. The maximum sample was achieved by using a double proportion formula by considering the assumptions: 95% confidence level, 80% power, and one-to-one ratio, proportions; premature rapture of membrane (p1= 52.2%, p2= 47.8%) based on a study conducted in southern Ethiopia 15 resulting in a maximum sample size of 414.
A sampling frame was created on the basis of the medical registration numbers of all NICU admissions during the specified period. Eligible cases were then selected via simple random sampling facilitated by a computer-generated random list (Figure 1) Schematic presentation of sampling procedure of prevalence of neonatal sepsis among neonates admitted to a neonatal intensive care unit in a university hospital in Eastern Ethiopia, 2022 (n=414).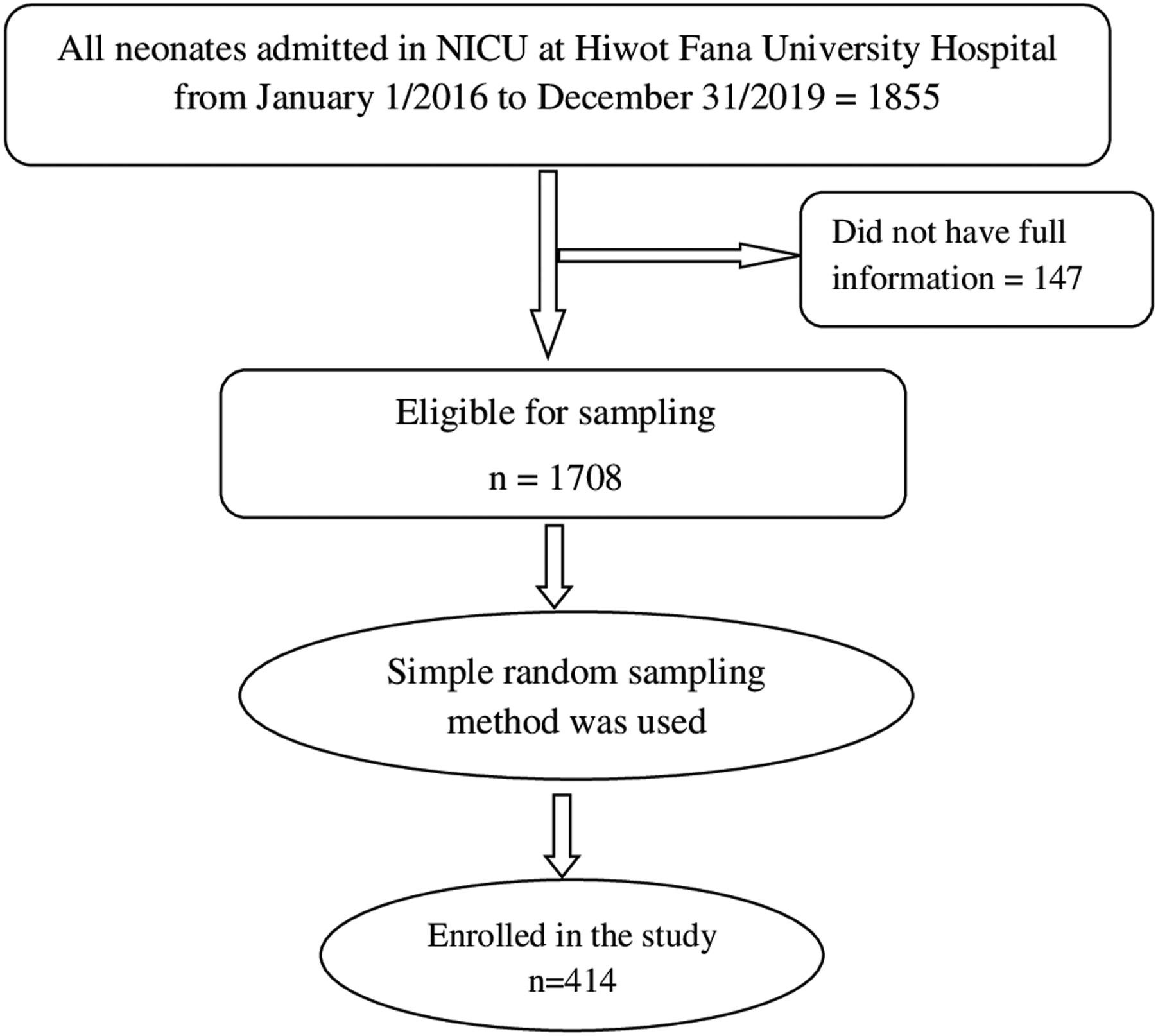
Data collection and quality control
The data was collected using checklist prepared by reviewing different literatures. If maternal information on the neonatal card was incomplete, the maternal card was traced by using neonatal card number. Data were collected by trained research assistants through a review of medical records from neonatal ICU register in NICU. Study was conducted entirely on secondary, anonymous data. The collected data included sociodemographic characteristics, maternal information, neonatal details (clinical or laboratory data), and care-related variables.
The tools were pre-tested in hospital with similar status on 5% of a total sample size. Two days training was given for data collector and supervisors on data collection procedures and coding of the questionnaire. Every day questionnaires were reviewed and checked for completeness by the supervisor and principal investigator. Double data entry was used to ensure validity and compared with the original data.
Operational definition
Data processing and analysis
The collected data were checked for completeness, coded, and double-entered into Epi Data 3.1 before being analysed via Stata 14. Descriptive analysis was performed to compute proportions and summary statistics. Bivariate and multivariate analyses were conducted to assess the associations between variables and neonatal sepsis. The Hosmer–Lemeshow statistic was used to evaluate model fit. Adjusted odds ratios (AORs) along with 95% confidence intervals (CIs) were estimated to identify factors associated with neonatal sepsis, with statistical significance set at p < 0.05.
Results
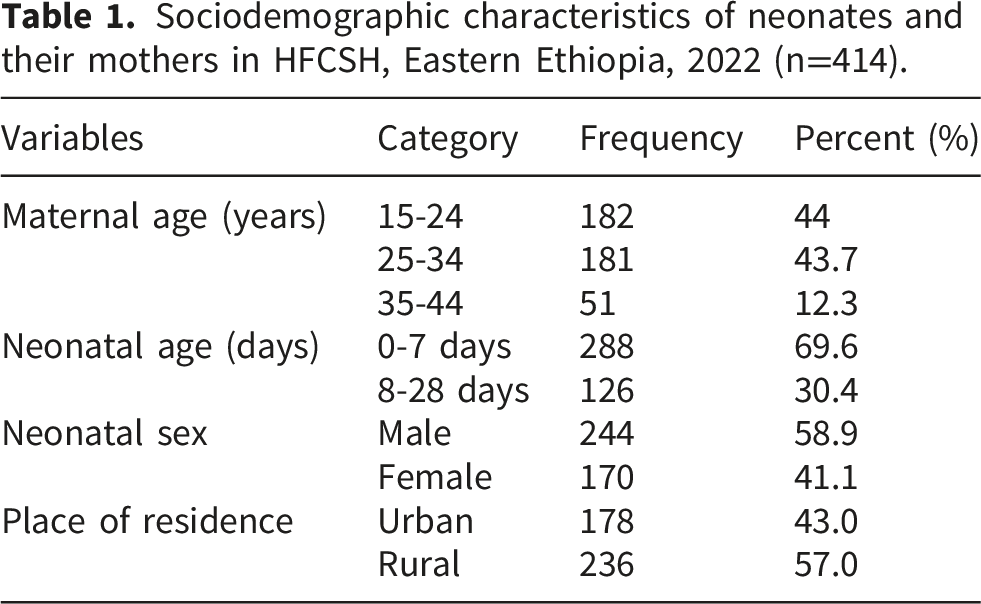
Sociodemographic characteristics of neonates and mothers
Sociodemographic characteristics of neonates and their mothers in HFCSH, Eastern Ethiopia, 2022 (n=414).
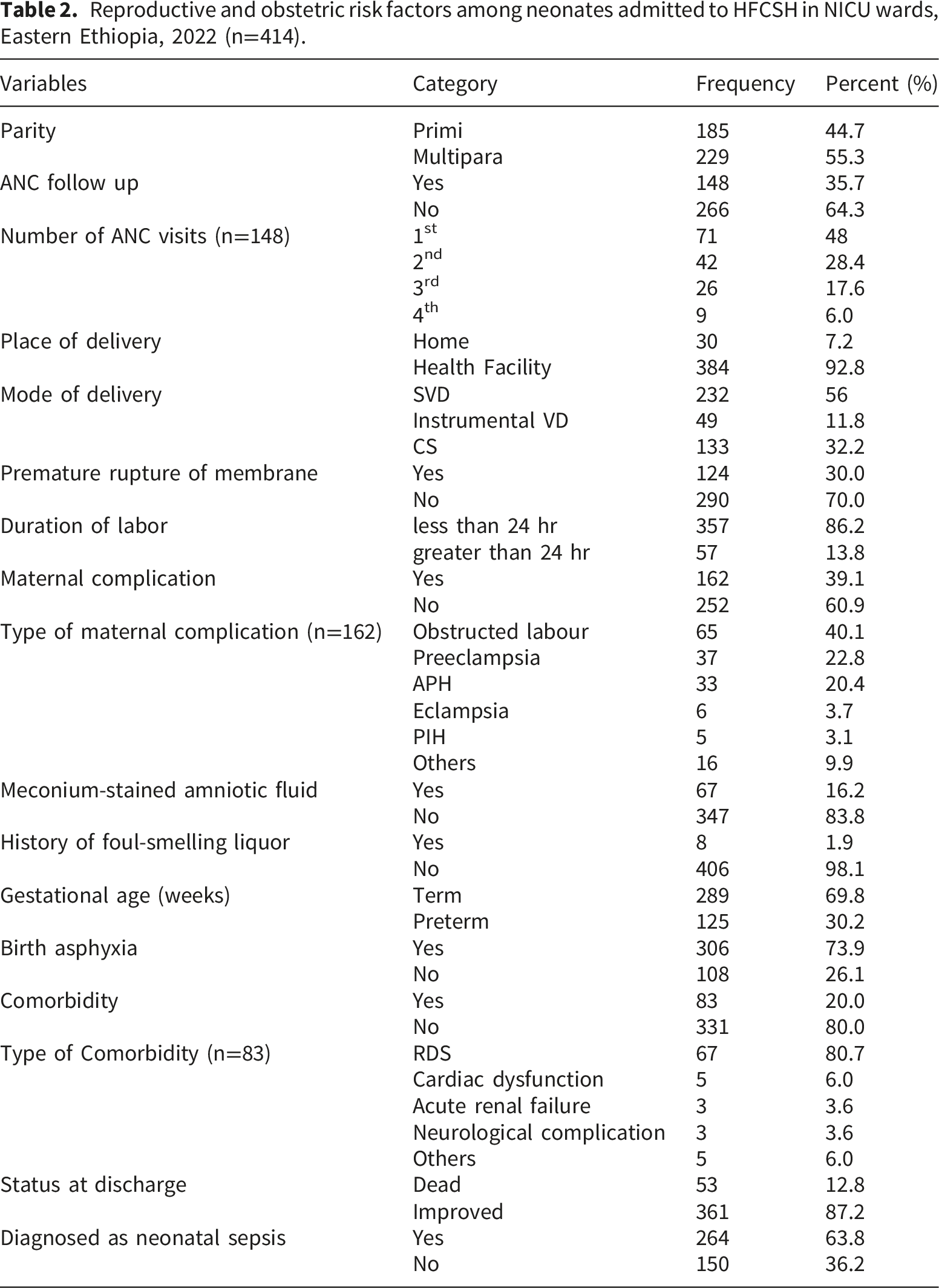
Reproductive and obstetric characteristics
Reproductive and obstetric risk factors among neonates admitted to HFCSH in NICU wards, Eastern Ethiopia, 2022 (n=414).
Factors associated with neonatal sepsis
Factors associated with neonatal sepsis included neonate age, residence, antenatal care follow-up, duration of labour, premature rupture of membranes, meconium-stained amniotic fluid, birth asphyxia, and neonatal comorbidity.
Compared with those older than seven days, neonates aged less than seven days were 2.18 times more likely to develop neonatal sepsis (AOR = 2.18; 95% CI: 1.10–4.34). Those from rural areas were 1.70 times more likely to develop neonatal sepsis than their urban counterparts were (AOR = 1.70; 95% CI: 1.08–2.67). Neonates born to mothers with antenatal care follow-up were 39% less likely to develop neonatal sepsis (AOR = 0.61; 95% CI: 0.38–0.97), as were those with a shorter duration of labour (<24 hours), who were 60% less likely to develop sepsis (AOR = 0.40; 95% CI: 0.18–0.89).
Analyses of factors associated with neonatal sepsis in neonates admitted to a university hospital in Eastern Ethiopia (n=414).
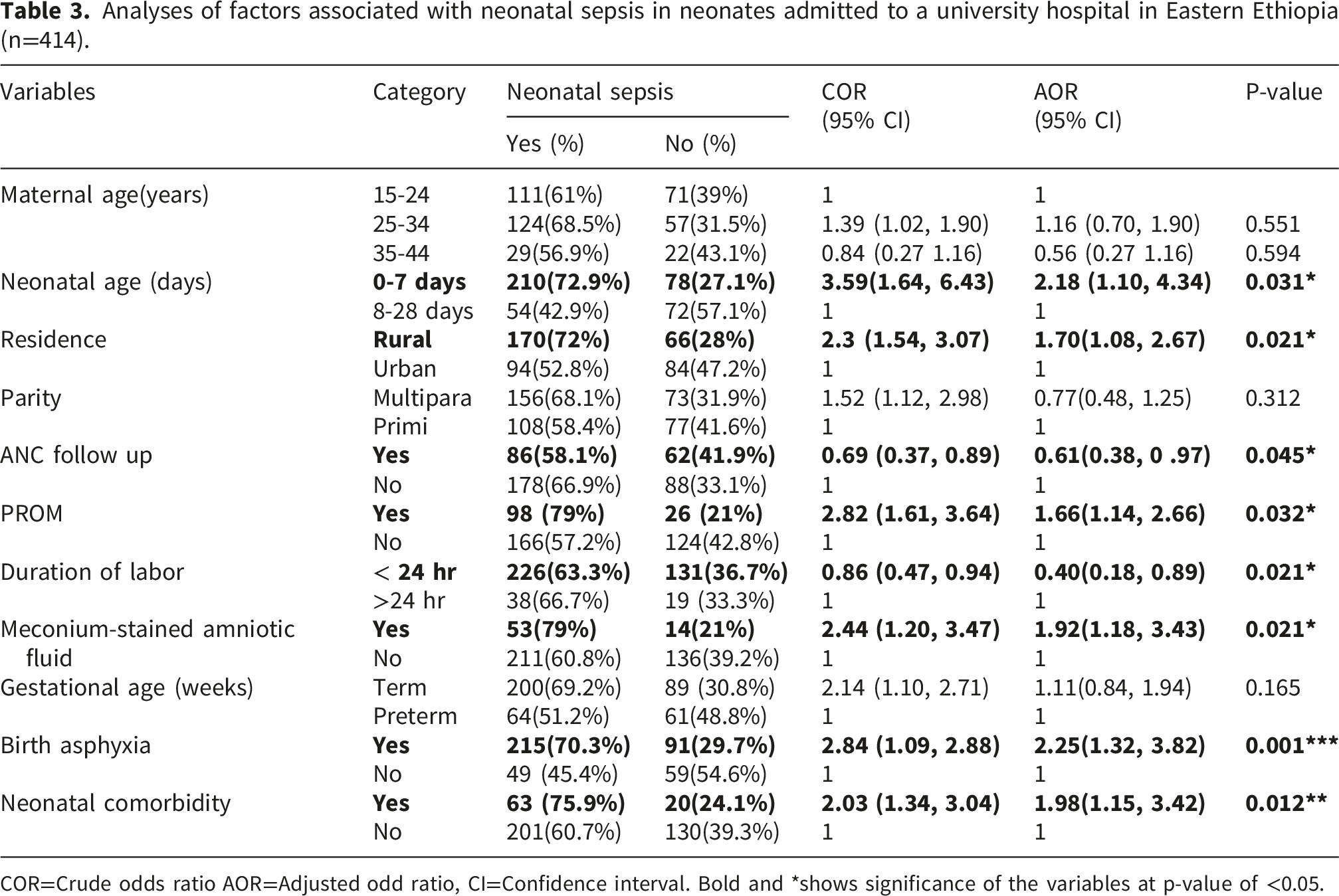
COR=Crude odds ratio AOR=Adjusted odd ratio, CI=Confidence interval. Bold and *shows significance of the variables at p-value of <0.05.
Discussion
This study assessed the prevalence of neonatal sepsis among neonates admitted to the neonatal intensive care unit of Hiwot Fana Comprehensive Specialized University Hospital in eastern Ethiopia. The overall prevalence of neonatal sepsis was 63.7% (95% CI: 59%–68%). Neonatal sepsis was more likely among neonates who were younger than seven days, born to mothers without prenatal care, experienced prolonged labour, had a history of meconium-stained amniotic fluid, suffered from birth asphyxia, and had comorbidities.
Our findings are lower than those reported from Ethiopia (77.9%) 16 but higher than those from Nepal (37.12%) 17 and Egypt (40.7%). 18 These differences may be related to variations in healthcare access, quality of care, infection control practices, or socioeconomic factors.
Several maternal- and neonatal-related factors associated with neonatal sepsis were identified. Neonates younger than seven days were more likely to develop sepsis, which is consistent with studies conducted in Shashemene Town, Ethiopia, 16 and Mogadishu, Somalia. 19 This increased vulnerability may be due to the immature immune status of early-born neonates.
Additionally, neonates from rural areas were more likely to develop neonatal sepsis than were those from urban areas, possibly because of better healthcare infrastructure and health-seeking behaviour in urban communities. Our study also revealed that neonates born to mothers with antenatal care (ANC) follow-up were less likely to develop sepsis, which aligns with findings from studies in Uganda 20 and India. 21 Women receiving ANC may have better awareness and management of risk factors.
As expected, neonates born to mothers with premature rupture of membranes (PROM) were more likely to develop sepsis, corroborating studies from Mexico 2 and the USA. 22 This may be attributed to the increased risk of ascending microorganisms into the amniotic sac due to early membrane rupture. Neonates born to mothers with a shorter duration of labor (<24 hours) were less likely to develop sepsis than those with longer labor durations were, which is consistent with studies from the Democratic Republic of the Congo 23 and southern Ethiopia. 1 A shorter labor duration may reduce the risk of meconium and amniotic fluid aspiration.
Moreover, neonates born to mothers with a history of meconium-stained amniotic fluid are more likely to develop sepsis, as shown in studies from Ghana, South Africa, and Mexico, 24 , 25 and. 2 This is likely due to the risk of aspirating contaminated fluid. Neonates with birth asphyxia are also at increased risk for sepsis, as supported by studies from Mexico 2 and Jinka, southern Ethiopia. 26 Contaminated resuscitation equipment may introduce pathogens into the infant’s lungs. Finally, neonates with comorbidities are more likely to develop sepsis, likely because of a compromised immune system.
Limitations of the study
This study is not without limitations. The generalizability of findings is limited by the use of secondary data, which may include biases from inconsistent or incomplete records. The cross-sectional design restricts the ability to explore temporal links between risk factors and outcomes, and data on the timing of sepsis development were not recorded, complicating our ability to determine whether sepsis developed in the NICU. Early-onset and late-onset cases didn’t separately analysed since timing of sepsis development were not recorded. Relevant variables like antibiotic use, clinical chorioamnionitis, and GBS status were missing.
Conclusion
This study demonstrated that the prevalence of neonatal sepsis at Hiwot Fana Teaching Hospital remains high. We identified several sociodemographic, maternal, and neonatal factors significantly associated with neonatal sepsis, including place of residence, antenatal care (ANC) follow-up, duration of labor, premature rupture of membranes (PROM), meconium-stained amniotic fluid, age less than seven days, birth asphyxia, and neonatal comorbidity.
These findings underscore the urgent need to address modifiable maternal and neonatal factors to reduce the prevalence of neonatal sepsis. Given the high neonatal mortality rate and the goal of achieving a target of 12 neonatal deaths per 1,000 births by 2030, it is critical to implement strategies that mitigate complications associated with neonatal sepsis.
Supplemental material
Supplemental material - Prevalence of neonatal sepsis among neonates admitted to a neonatal intensive care unit in a university hospital in eastern Ethiopia: A cross-sectional study
Supplemental materia for Prevalence of neonatal sepsis among neonates admitted to a neonatal intensive care unit in a university hospital in eastern Ethiopia: A cross-sectional study by Mesud Abrahim, Lemesa Abdisa, Tesfaye Assebe Yadeta, Dawit Firdisa, Abera Kenay Tura in Journal of Public Health Research.
Supplemental material
Supplemental material - Prevalence of neonatal sepsis among neonates admitted to a neonatal intensive care unit in a university hospital in eastern Ethiopia: A cross-sectional study
Supplemental materia for Prevalence of neonatal sepsis among neonates admitted to a neonatal intensive care unit in a university hospital in eastern Ethiopia: A cross-sectional study by Mesud Abrahim, Lemesa Abdisa, Tesfaye Assebe Yadeta, Dawit Firdisa, Abera Kenay Tura in Journal of Public Health Research.
Footnotes
Acknowledgements
We would like to thank Haramaya University College of Health and Medical Science for allowing us to conduct this study. Additionally, we would like to thank all the hospital management and staff.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki. Ethical approval for this study was obtained from the Institutional Health Research Ethics Review Committee (IHRERC) of Haramaya University with reference number of IHRERC/139/2020. Before beginning data collection, an official letter was obtained from the College of Health and Medical Sciences and submitted to the responsible body, and after the purpose and the possible benefit of the study were explained, permission to gather data was obtained from the medical director of the respective hospital. There was no mention of patients’ names in the data collection format, and patients’ cards were returned to the card room as soon as the data collection format was filled, which helped secure patients’ information.
Author contributions
MA, LA, and DF designed the study protocol, extracted and analyzed the data, and wrote the first draft of the manuscript. MA, LA, DF, TAY, and AK designed the study, conducted the literature review, statistically analyzed the review, provided critical appraisal, extracted data, and critically revised the manuscript. All authors read and approved the final version before submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors without undue reservation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.