
Abstract
Background
Gastroesophageal reflux disease (GERD) is a common condition influenced by lifestyle, clinical, and psychosocial factors. This study examined the relationship between GERD symptoms and perceived stress among Lebanese adults, while accounting for key demographic, dietary, and clinical variables.
Method
A cross-sectional study was conducted among Lebanese adults between January and September 2024 using an online self-administered questionnaire. GERD symptoms and perceived stress were assessed using the GERDQ and PSS-10 scales. Bivariate analyses followed by multivariable logistic regression were performed to identify factors independently associated with GERD symptoms.
Results
A total of 440 participants were included (mean age of 36.4 ± 16.96 years), of whom 28.4% had probable GERD symptoms. Most participants (83.2%) reported moderate stress levels with a mean PSS score of 19.74±5.05. Higher perceived stress was independently associated with increased odds of GERD symptoms (ORa=1.110). Additional correlates included dietary factors (frequent intake of fatty/fried foods, carbonated beverages, and caffeinated drinks), medication-related factors (NSAIDs, bisphosphonates, and iron supplements), former smoking, and a personal or family history of gastrointestinal disease. Being married was associated with lower odds of GERD symptoms.
Conclusion
Probable GERD symptoms were independently associated with perceived stress, dietary habits, smoking history, medication use, and gastrointestinal disease history. These findings support a biopsychosocial understanding of GERD symptom burden and provide further evidence that psychosocial factors should be considered when investigating gastrointestinal health in vulnerable populations.
Introduction
Gastroesophageal reflux Disease (GERD) is highly prevalent worldwide, affecting approximately 14% of adults, with marked geographical variation and particularly high rates reported in the Middle East.1–3 GERD symptoms primarily include heartburn and regurgitation and may also involve atypical chest discomfort, respiratory manifestations, or laryngeal symptoms. 4
GERD is a multifactorial condition influenced by a complex interaction of physiological, lifestyle, and environmental factors. 5 Established contributors include obesity, smoking, dietary habits, alcohol consumption, and medications that affect lower esophageal sphincter tone or esophageal mucosal integrity.3,6–8 These factors may impair esophageal motility, delay gastric emptying, or increase intra-abdominal pressure, thereby facilitating reflux events. 9 Beyond these traditional risk factors, increasing attention has been directed toward psychosocial determinants that may modulate gastrointestinal symptom severity and perception. 10
Psychological stress has emerged as an important factor influencing both the development and perception of GERD symptoms. 11 Experimental and clinical evidence suggests that stress can alter esophageal motility, increase transient lower esophageal sphincter relaxations, and enhance visceral hypersensitivity, thereby amplifying symptom perception even in the absence of significant acid exposure pathways.12,13 In addition, stress-related neuroendocrine responses may influence gastrointestinal function through autonomic dysregulation and altered gut-brain signaling pathways. 14 Importantly, the relationship appears bidirectional, as chronic GERD symptoms may also contribute to increased psychological distress, creating a self-perpetuating cycle of symptom exacerbation. 15
In Lebanon, GERD represents a significant health concern, with previous research reporting a prevalence of approximately 24.8% among adults. 16 This burden may be further compounded by the country’s unique sociopolitical and economic context. Over the past decade, Lebanon has experienced multiple overlapping crises, including economic collapse, political instability, and major traumatic events, all of which have been associated with elevated levels of psychological stress in the population.17–19 Although previous Lebanese studies have reported the prevalence of GERD and its association with various lifestyle and clinical factors, limited evidence has explored the role of perceived stress using validated psychometric instruments or examined whether stress independently contributes to GERD symptoms after controlling for dietary, behavioral, and medication-related factors.
We hypothesized that higher perceived stress would be associated with increased odds of GERD symptoms independent of traditional risk factors. Therefore, this study aimed to evaluate the association between perceived stress and GERD symptoms among Lebanese adults while accounting for relevant demographic, lifestyle, and clinical factors.
Design and methods
Study design and sampling
The study was conducted between January and September 2024. It employed an observational cross-sectional design, which limits the establishment of temporal or causal relationships between perceived stress and GERD symptoms. The target population consisted of Lebanese adults residing across all six administrative governorates (Beirut, Mount Lebanon, North, South, Bekaa, and Nabatieh). Data were collected using an anonymous online questionnaire distributed through social media platforms and personal networks. Recruitment followed a non-probability snowball-sampling strategy, whereby initial respondents shared the survey link with others to facilitate broader geographic reach across Lebanese governorates. This approach was selected because of its feasibility, cost-effectiveness, and ability to rapidly recruit participants from different regions during ongoing socio-economic challenges in Lebanon. However, this method may have introduced selection bias by disproportionately recruiting younger, more digitally connected, more educated, and potentially more health-aware individuals, thereby limiting the representativeness of the sample and generalizability of the findings.
Lebanese individuals aged 18 years or older were eligible for inclusion. Participants were excluded if they reported peptic ulcer disease, a history of gastric surgery, systemic disorders affecting the upper gastrointestinal tract, or alarm symptoms such as unintentional weight loss, severe or progressive dysphagia, or gastrointestinal bleeding. Individuals currently using proton pump inhibitors (PPIs) or H2-receptor blockers were also excluded because acid-suppressive therapy may mask or reduce reflux symptoms, potentially affecting the accuracy of GERDQ-based symptom assessment and participant classification. Information regarding medication use, including PPIs and H2 blockers, was obtained through self-report within the questionnaire. Although this exclusion may have omitted some clinically relevant GERD cases, it was intended to minimize symptom misclassification related to ongoing pharmacological treatment.
Data collection tool
A structured questionnaire was designed using evidence from previously published literature and established assessment tools. Items assessing socio-demographic characteristics, lifestyle behaviors, dietary habits, smoking status, medication use, and clinical history were developed based on prior studies and refined through expert evaluation, although they did not represent a formally validated composite instrument.4,5,7 Conversely, the GERDQ and PSS-10 consisted of standardized validated scales with well-established psychometric validity and reliability.20–22 The survey was prepared and administered in both English and Arabic. The questionnaire was initially written in English, translated to Arabic following standard cross-cultural adaptation guidelines, then independently back translated to English. The questionnaire was reviewed by two faculty members with expertise in public health and pharmacy practice. A pilot test involving five individuals was conducted to assess questionnaire clarity, comprehensibility, and usability prior to data collection. Minor modifications were made accordingly, and pilot responses were excluded from the final analysis. However, the small pilot sample was intended for preliminary usability assessment rather than formal psychometric validation of the overall questionnaire.
The data collection sheet consisted of four main sections. The first section retrieved data regarding socio-demographic characteristics, whereas the second section collected information about the risk factors of GERD such as comorbidities, alcohol consumption, diet, hours of sleep, personal or family history of GI diseases and medications associated with GERD. Smoking status was categorized into current smokers (individuals who used any tobacco product within the past 30 days), former smokers (individuals who previously smoked but had abstained for at least 30 days prior to completing the survey), and non-smokers (individuals who had never smoked). This classification is consistent with commonly used epidemiological smoking classifications. 23 The third part included the 6-item GERDQ questionnaire, a standardized self-administered screening tool used to assess the frequency and severity of GERD-related symptoms. 22 Participants reported the number of days (0-7) with typical symptoms and use of over-the-counter remedies during the preceding week. Four symptom items were scored on a 0-3 scale, while two items (epigastric pain and nausea) were reverse-scored, yielding a total score between 0 and 18. A GERDQ cutoff score of ≥8 was used to classify participants as having probable GERD symptoms, in accordance with prior validation studies reporting acceptable sensitivity, specificity, and utility for symptom-based GERD screening in epidemiological and primary care settings. 24 The GERDQ scale displayed high internal consistency with a Cronbach’s alpha coefficient of 0.86. The fourth section comprised the perceived stress (PSS) scale, 20 a widely used psychological instrument for measuring perceived stress. The Arabic version of the PSS-10, utilized in this study, has previously been validated in a Lebanese population, and demonstrated acceptable reliability (Cronbach’s α = 0.74). 21 This 10-item scale assesses the thoughts and feelings of the participants over the past month by asking how frequently they experienced certain emotional and cognitive states. Responses were recorded on a 5-point Likert scale (0-4), with total scores ranging from 0 to 40 and categorized into low (0-13), moderate (14-26), or high stress (27-40). The PSS scale displayed acceptable internal consistency with a Cronbach’s alpha coefficient of 0.79.
Ethical approval
Ethical approval for the study was granted by the Lebanese International University Ethical and Research Committee (approval number: 2024ERC-014-LIUSOP). Participation was entirely voluntary. Written electronic consent was obtained prior to accessing the questionnaire, and no identifying data were collected. The study complied with the ethical principles outlined in the Declaration of Helsinki.
Sample size calculation
The minimum required sample size was estimated using Epi-Info (Centers for Disease Control and Prevention) for a cross-sectional prevalence study. 25 Assuming a prevalence of 50%, a margin of error of 5%, and a 95% confidence level, the minimum required sample size was 384 participants. A prevalence estimate of 50% was selected because it produces the largest sample size requirement when the true prevalence is uncertain, representing the most conservative approach for cross-sectional sample size calculation. Although previous Lebanese studies reported a GERD prevalence of approximately 24.8%, 16 the 50% assumption was retained to provide a conservative sample size estimate and minimize the risk of underestimating the required sample size. Furthermore, the final sample included 125 participants with probable GERD symptoms, providing a sufficient number of outcome events for multivariable logistic regression according to commonly recommended events-per-variable considerations. 26
Statistical analysis
Statistical analyses were conducted using IBM SPSS Statistics version 25. Descriptive statistics included frequencies and percentages for categorical variables and means with standard deviations for continuous variables. Normality of continuous variables was assessed using the Shapiro-Wilk test in combination with visual inspection of histograms and Q-Q plots prior to applying parametric analyses. Internal consistency of the scales was assessed using Cronbach’s alpha. Associations between GERD symptom status and independent variables were initially explored through bivariate analyses. Chi-square or Fisher’s exact tests were applied to categorical variables, while independent-sample t-tests were used for continuous measures such as age, BMI, and PSS score. Variables showing p<0.20 in the bivariate analysis were included in a multivariable logistic regression model, with probable GERD symptom status (GERDQ ≥8) as the dependent variable. A liberal threshold of p<0.20 was used during bivariate screening to minimize the risk of excluding potentially important explanatory variables or confounders prior to multivariable adjustment. Multicollinearity among independent variables was assessed using variance inflation factors (VIFs) and tolerance statistics prior to conducting the multivariable logistic regression analysis, and no evidence of problematic multicollinearity was identified. Linearity in the logit for continuous variables was assessed using the Box-Tidwell procedure, and no evidence of violation was identified for continuous variables included in the model. The final logistic regression model demonstrated acceptable fit according to the Hosmer-Lemeshow goodness-of-fit test (p>0.05), with a Nagelkerke R2 of 0.28, indicating moderate explanatory capacity. Statistical significance was defined as p<0.05.
Results
Socio-demographic characteristics of the participants
Socio-demographic characteristics of the participants.
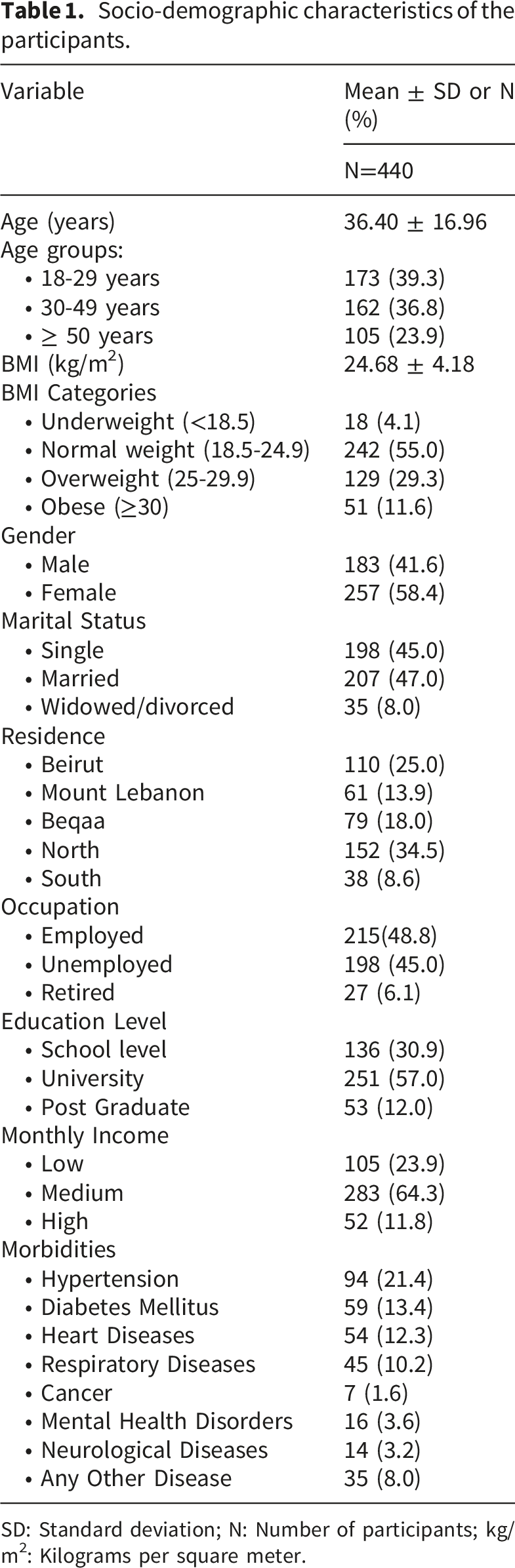
SD: Standard deviation; N: Number of participants; kg/m2: Kilograms per square meter.
Prevalence and frequency of GERD symptoms
Frequency of GERD symptoms among the participants based on GERDQ.
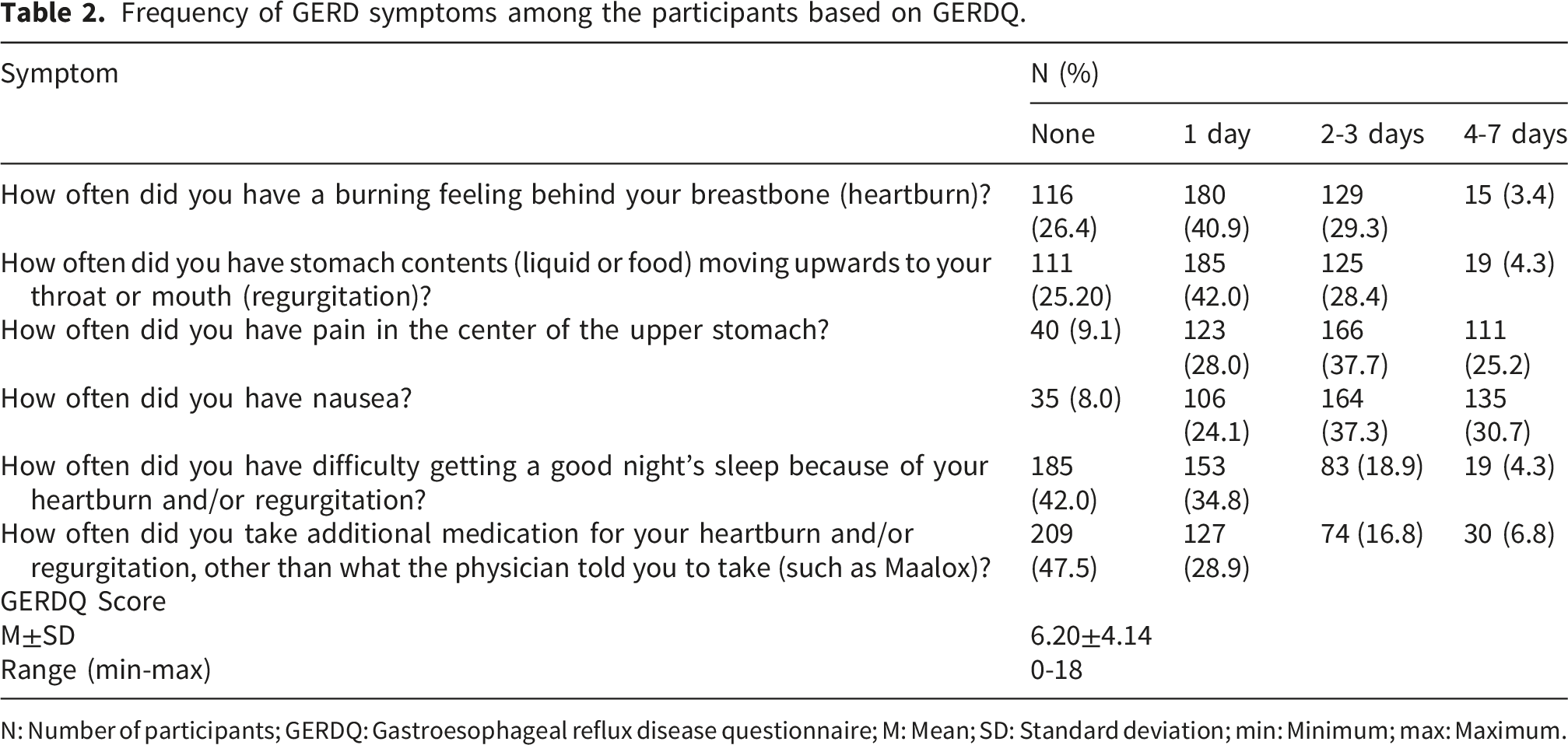
N: Number of participants; GERDQ: Gastroesophageal reflux disease questionnaire; M: Mean; SD: Standard deviation; min: Minimum; max: Maximum.
Prevalence of GERD symptoms risk factors
Dietary and lifestyle GERD-associated risk factors among the studied participants.
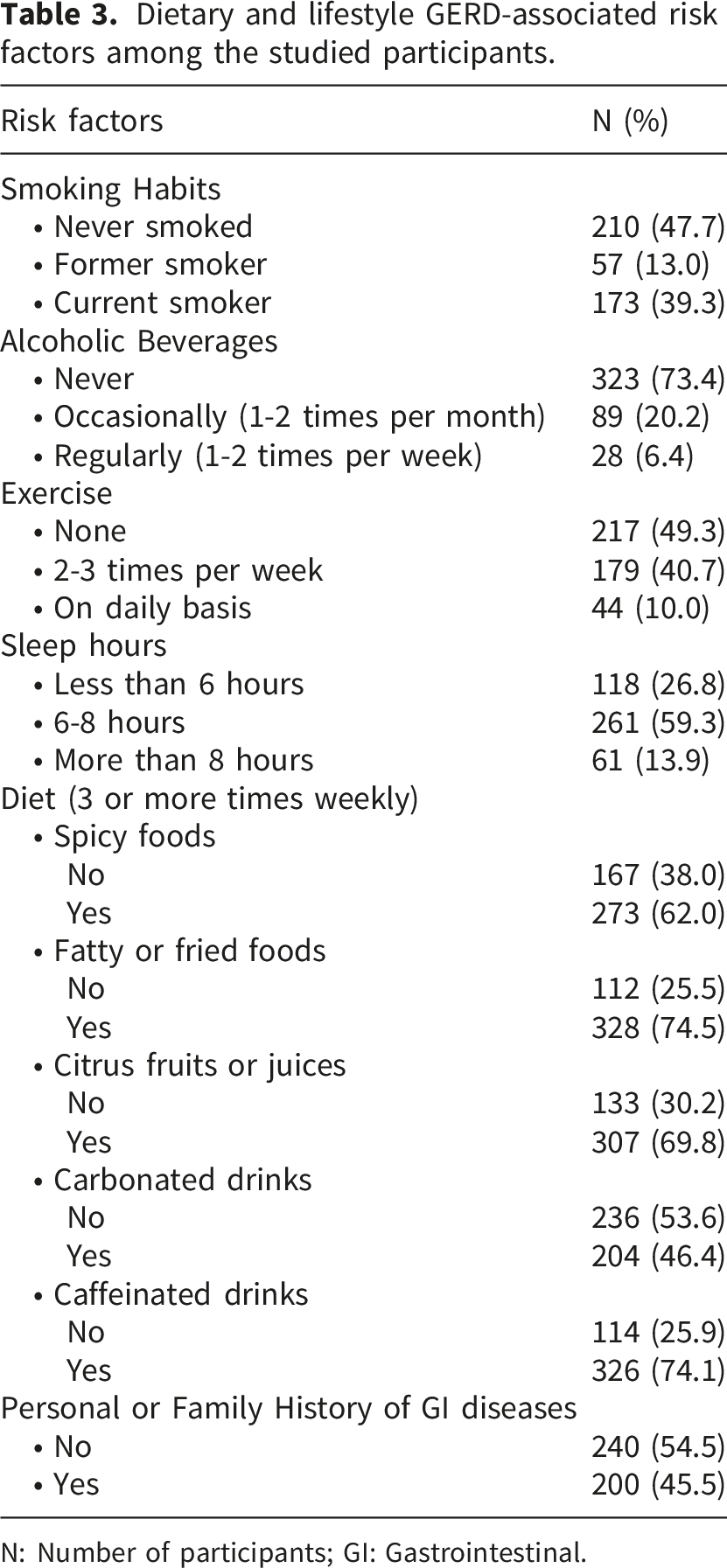
N: Number of participants; GI: Gastrointestinal.
Figure 1 illustrates the prevalence of medications potentially associated with GERD symptoms among the studied participants. Among the listed drugs, nonsteroidal anti-inflammatory drugs (NSAIDs) were the most commonly utilized (35.5%), followed by iron supplements (30.9%) and aspirin (21.6%). The least frequently reported medications were bisphosphonates (5.9%) and antidepressants (5.2%). Utilization of GERD-associated medications among the studied participants.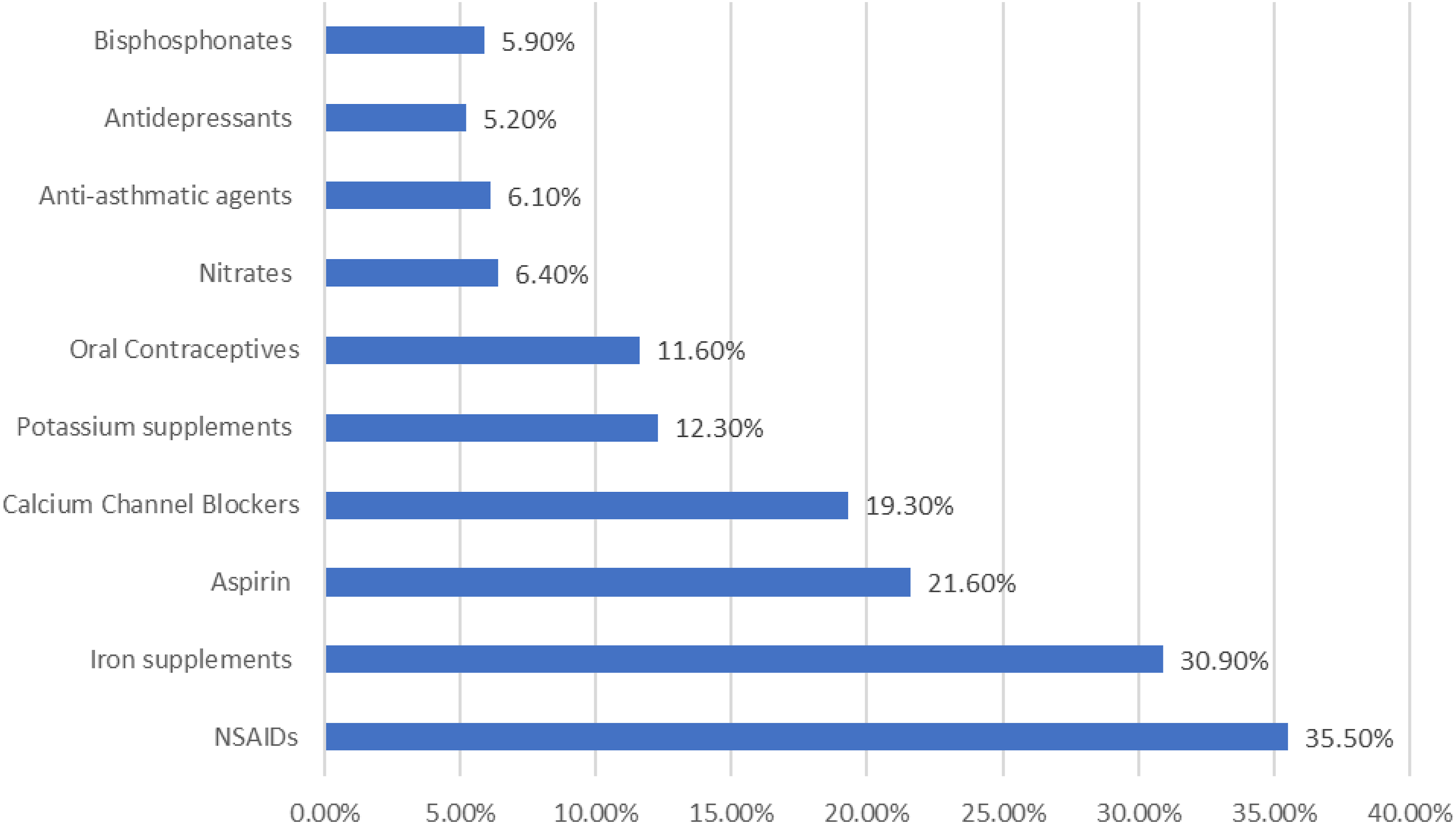
Perceived stress and stress levels among the participants
Perceived stress among the participants based on PSS scale.
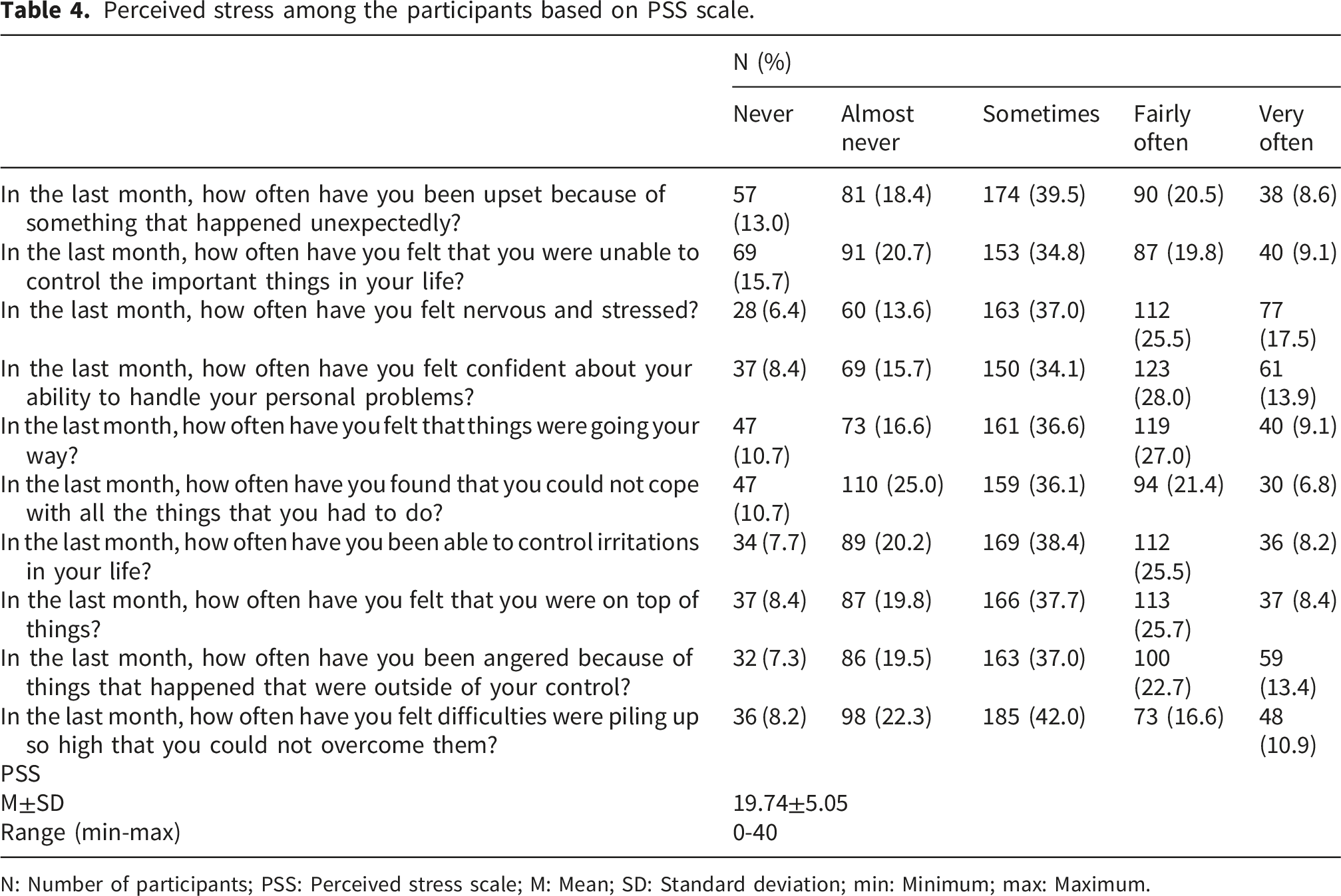
N: Number of participants; PSS: Perceived stress scale; M: Mean; SD: Standard deviation; min: Minimum; max: Maximum.
Factors associated with GERD symptoms
Bivariate analyses examining the associations between probable GERD symptoms and participants’ socio-demographic, lifestyle, dietary, clinical, medication-related, and stress-related variables are presented in Supplementary Table 1. Bivariate analyses demonstrated that participants with probable GERD symptoms were significantly older and had higher perceived stress scores compared with participants without GERD symptoms. Significant associations were also observed for marital status, smoking habits, several comorbidities, dietary factors, personal or family history of gastrointestinal diseases, and use of multiple medications including NSAIDs, oral contraceptives, bisphosphonates, and iron supplements.
A multivariable logistic regression analysis of the factors associated with GERD symptoms.
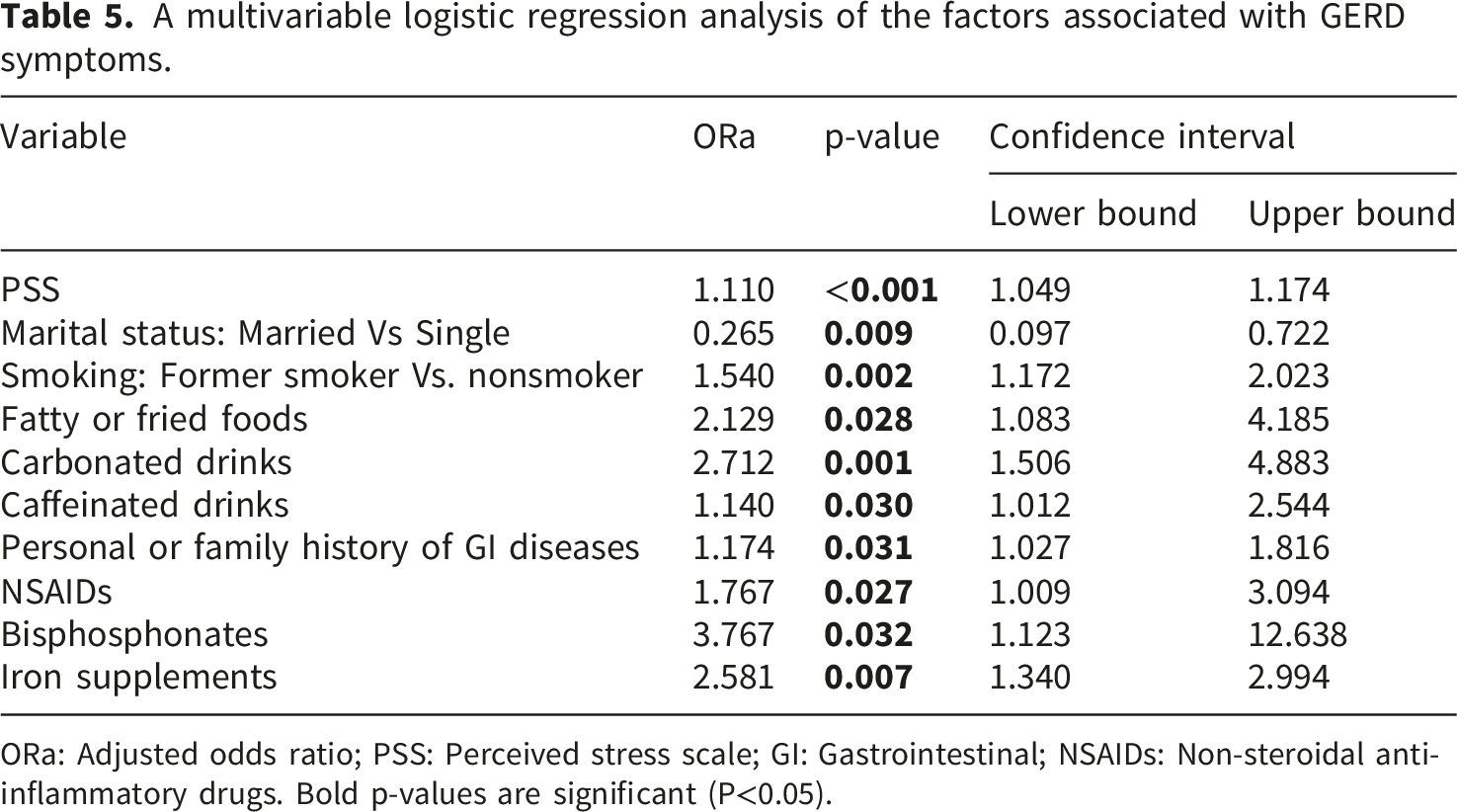
ORa: Adjusted odds ratio; PSS: Perceived stress scale; GI: Gastrointestinal; NSAIDs: Non-steroidal anti-inflammatory drugs.
Bold p-values are significant (P<0.05).
Discussion
This study examined the prevalence and factors associated with GERD symptoms among Lebanese adults, with particular emphasis on the role of perceived stress alongside lifestyle and clinical factors. Around 28.4% of participants met the GERDQ threshold, aligning with previous Lebanese data. 16 This prevalence appears higher than estimates reported in several regional and international studies, which generally range between 10% and 20% in Western countries and fall below 10% in several Asian and Middle Eastern populations.1,9 The findings may reflect the wide health consequences of chronic societal stress exposure in Lebanon, where prolonged economic instability and uncertainty have influenced dietary habits, healthcare access, sleep quality, and health-related behaviors. These interconnected stressors may collectively contribute to increased gastrointestinal symptom burden within the population.
Participants predominantly exhibited moderate perceived stress levels, aligning with recent Lebanese data documenting widespread psychological distress amid prolonged economic, political, and social instability.18,27 However, the distribution of stress levels was highly concentrated within the moderate stress category, with relatively few participants classified as having either low or high stress levels. Such a restricted distribution may have resulted in range restriction, a phenomenon whereby limited variability in an independent variable attenuates observed associations and reduces the ability to fully characterize dose-response relationships. 28 Consequently, the magnitude of the association between perceived stress and GERD symptoms observed in this study may underestimate the true relationship that could be observed in populations exhibiting greater heterogeneity in stress exposure. Similar attenuation of regression coefficients and effect estimates due to restricted variability in predictor variables has been widely recognized in regression and behavioral science research. 29 Although perceived stress was analyzed as a continuous variable in the multivariable model to preserve statistical information and maximize statistical power, caution is warranted when generalizing these findings to populations with substantially different stress distributions. Future studies involving more diverse stress profiles and longitudinal designs are needed to better characterize the relationship between stress severity and GERD symptom burden. Notably, despite the elevated stress burden, many respondents reported some confidence in managing daily challenges, indicating elements of adaptive resilience despite ongoing adversity. 30
Perceived stress emerged as a significant independent factor associated with GERD symptoms. This finding supports growing evidence implicating the gut-brain axis in the modulation of reflux symptom perception and gastrointestinal function. 31 Psychological stress may contribute to heightened visceral hypersensitivity, altered esophageal motility, and autonomic dysregulation, thereby amplifying reflux symptom perception even in the absence of substantial acid exposure. 32 Importantly, psychological stress may influence not only the occurrence of reflux symptoms but also symptom perception and reporting behavior. Consequently, individuals with elevated stress levels may perceive reflux symptoms as more severe or bothersome despite similar levels of physiological reflux exposure. This observation further supports the concept that GERD symptom burden may not depend solely on acid exposure but may also involve central pain processing and stress-related hypervigilance. Similar associations have been observed across diverse populations, including studies from Saudi Arabia, Iran, Korea, and the United States.12,33–35 Nevertheless, the cross-sectional design precludes establishing directionality, and reverse causation remains possible, as persistent reflux symptoms themselves may contribute to psychological distress and elevated stress perception. In a setting such as Lebanon, where population-level stress remains persistently elevated, 18 these findings highlight the potential value of incorporating psychosocial assessment into GERD symptom treatment. Collectively, these findings support a more biopsychosocial approach to GERD symptom management that extends beyond acid suppression alone and incorporates psychological wellbeing, lifestyle modification, and behavioral counseling.
Dietary behaviors also contributed significantly to GERD symptoms. The results of our study revealed higher odds of having GERD symptoms among individuals with frequent consumption of high-fat or fried foods, caffeinated and carbonated drinks. High-fat meals reduce lower esophageal sphincter (LES) pressure and delay gastric emptying, whereas caffeine and carbonated beverages promote transient LES relaxations and increase gastric distension.36,37 Our findings are consistent with previous reviews demonstrating that energy-dense foods and high caffeine intake increase the likelihood of GERD symptoms. 6 The observed associations between dietary factors, smoking history, and GERD symptoms likely reflect clustering of unhealthy lifestyle behaviors rather than isolated exposures alone. Such behavioral clustering may partially explain the persistence of reflux symptoms within high-stress populations. Considering that Lebanese dietary habits have increasingly shifted toward fried foods, sweetened beverages, and café culture, dietary modification should remain a key component of strategies aimed at reducing GERD symptom burden. Although caffeinated drink consumption remained statistically significant in the adjusted model, the association should be interpreted cautiously. The confidence interval was relatively wide and its lower bound was close to unity, indicating considerable uncertainty regarding the magnitude of the effect. Consequently, this finding may represent a statistically fragile association and requires confirmation in larger studies before firm conclusions regarding the role of caffeine in GERD symptom development can be drawn.
Interestingly, current smoking demonstrated a strong crude association with GERD symptoms but lost statistical significance after multivariable adjustment, whereas former smoking remained independently associated. This pattern suggests that the relationship between current smoking and GERD symptoms may be partially explained by other lifestyle and dietary factors included in the model, several of which remained independently associated with GERD symptoms after adjustment. In contrast, the persistence of former smoking may reflect cumulative effects of prior tobacco exposure or reverse causation, whereby individuals experiencing reflux symptoms may have reduced or discontinued smoking because of symptom aggravation. Previous research has demonstrated improvement in GERD symptoms following smoking cessation, supporting the plausibility of this explanation. 38 Given the cross-sectional design, the precise mechanism underlying this finding cannot be determined and warrants further longitudinal investigation.
Medication use also showed a significant association with GERD symptoms, particularly NSAIDs, bisphosphonates, and iron supplements. These agents are well-established esophageal irritants and can induce mucosal injury, impair mucosal defenses, or cause delayed esophageal transit.39,40 These findings are particularly clinically relevant because many of these medications are frequently used in community settings and may contribute to symptom aggravation when taken without adequate counseling regarding administration timing, posture, or gastrointestinal precautions. The observed associations reinforce the importance of careful medication review and patient counseling regarding appropriate administration practices in individuals presenting with reflux symptoms. Several other medications, including oral contraceptives, antidepressants, calcium channel blockers, aspirin, and anti-asthmatic agents, demonstrated significant associations with GERD symptoms in the bivariate analyses but did not remain significant after multivariable adjustment. This attenuation suggests that their crude associations may have been influenced by underlying demographic, clinical, or lifestyle characteristics rather than representing independent predictors of GERD symptoms. In particular, oral contraceptive use exhibited one of the strongest bivariate associations but lost significance after adjustment, indicating that the observed relationship may have been confounded by other factors included in the model. These findings underscore the importance of multivariable analyses in distinguishing independent risk factors from variables that primarily reflect broader clinical or behavioral profiles.
Marital status demonstrated the strongest protective association observed in the adjusted model, with married participants exhibiting substantially lower odds of GERD symptoms. Several mechanisms may explain this finding. Marriage may provide emotional support, social stability, and stress-buffering effects that reduce psychological distress and physiological stress responses implicated in gastrointestinal symptom perception. 41 Greater social support has been associated with improved coping capacity, lower perceived stress, and better gastrointestinal health outcomes in previous studies.32,42 Furthermore, married individuals may be more likely to engage in healthier daily routines, regular meal patterns, and appropriate healthcare-seeking behaviors, which could indirectly reduce GERD symptom burden. 43 Nevertheless, alternative explanations should also be considered. The observed association may partially reflect residual differences in socioeconomic stability, employment status, or other unmeasured psychosocial factors that were not fully captured in the regression model. Given the magnitude of the association, further studies are needed to determine whether marital status itself exerts a protective effect or serves as a marker of broader psychosocial advantages.
Several variables that demonstrated significant associations with GERD symptoms in bivariate analyses, including current smoking, spicy foods, citrus products, and certain medications and comorbidities such as hypertension, diabetes, and heart disease, did not remain significant after multivariable adjustment. This finding suggests that these associations may have been influenced by confounding or mediated through other interrelated behavioral, dietary, psychosocial, or clinical factors. For example, although spicy foods and citrus products were initially associated with GERD symptoms, these effects were no longer independent after adjustment for stress and other dietary exposures. Similarly, the attenuation of associations involving chronic comorbidities may reflect the influence of shared lifestyle and medication-related factors rather than direct independent effects.
The high frequency of over-the-counter medication use observed among participants may additionally indicate substantial self-management of reflux symptoms within the community. This may potentially reflect normalization of chronic gastrointestinal symptoms or barriers to healthcare access. Although multivariable adjustment was performed, residual confounding related to unmeasured dietary, psychological, or socioeconomic factors cannot be entirely excluded. Overall, the findings suggest that GERD symptom burden within the Lebanese population may reflect a complex interaction between psychosocial stress, lifestyle behaviors, dietary patterns, medication exposure, and broader societal challenges.
Strengths and limitations
This study has several strengths. It represents one of the few investigations exploring the association between GERD symptoms and stress within the Lebanese population using validated instruments, GERDQ and PSS, both of which showed high internal consistency. The inclusion of participants from all Lebanese districts enhances the geographical representation and generalizability of our findings. The study also included a relatively large sample size which improves its statistical power. However, several limitations must be acknowledged. The cross-sectional design precludes establishing temporal or causal relationships between perceived stress, lifestyle factors, medication use, and GERD symptoms. Therefore, reverse causation cannot be excluded, as GERD symptoms themselves may contribute to elevated stress perception. In addition, recruitment through social media platforms and the use of snowball sampling may have resulted in a non-representative sample by disproportionately capturing individuals with greater digital connectivity, higher health awareness, or education thereby limiting generalizability to the broader Lebanese population. Furthermore, several variables including dietary habits, smoking status, medication use, comorbidities, stress perception, and GERD symptoms were self-reported and therefore may be subject to recall bias, reporting inaccuracies, and social desirability bias. Moreover, the absence of clinical or endoscopic confirmation of reflux disease limits the ability to objectively verify reflux disease, as GERDQ is a symptom-based screening instrument rather than a definitive diagnostic tool. Additionally, perceived stress was assessed using the PSS-10, a validated subjective measure of psychological stress, without incorporation of objective biological stress markers such as cortisol levels. Also, the PSS-10 evaluates perceived stress over the preceding month, whereas the GERDQ assesses reflux symptoms during the previous week, resulting in a slight temporal mismatch between the evaluated constructs. In addition, physical activity was assessed using a simplified self-reported measure rather than a validated instrument such as the International Physical Activity Questionnaire (IPAQ) to minimize questionnaire length and participant burden within the online survey format. This may have limited the precision of physical activity assessment. Finally, data collection occurred between January and September 2024, and potential seasonal variations in dietary behaviors, environmental conditions, or symptom patterns could not be excluded. Despite these limitations, this study provides valuable epidemiological insight into the psychosocial and behavioral risk factors of GERD in Lebanon and serves as an important foundation for future longitudinal and interventional research.
Practical implications
The study findings have important clinical and public health implications in Lebanon. The high prevalence of GERD symptoms and its significant association with stress, unhealthy dietary habits, smoking, and certain medications highlight the need for a comprehensive, multidisciplinary approach to prevention and management. Integrating psychosocial screening and stress management into GERD care alongside promoting dietary modifications and smoking cessation could substantially reduce symptom burden. Healthcare providers should also review medication use carefully, particularly NSAIDs, bisphosphonates and iron salts to minimize esophageal irritation. At the population level, awareness campaigns and lifestyle education targeting stress resilience and healthy eating are essential to mitigate GERD symptoms amid Lebanon’s ongoing social, political and economic challenges.
Conclusion
This study demonstrated a considerable burden of probable GERD symptoms among Lebanese adults. GERD symptoms were independently associated with perceived stress, dietary habits, smoking history, medication use, and gastrointestinal disease history. These findings support a biopsychosocial model of GERD symptom burden, in which psychological, behavioral, and clinical factors interact to influence symptom occurrence and perception. Given the prolonged societal stress experienced in Lebanon, the results provide further evidence that psychosocial factors should be considered when investigating gastrointestinal health in vulnerable populations. Future prospective studies are warranted to establish temporal relationships and evaluate the effectiveness of interventions targeting psychosocial and behavioral risk factors in reducing GERD symptom burden and improving gastrointestinal health outcomes.
Supplemental material
Supplemental material - Perceived stress, diet, and medication use associated with GERD symptoms in Lebanese adults: A cross-sectional study
Supplemental material for Perceived stress, diet, and medication use associated with GERD symptoms in Lebanese adults: A cross-sectional study by Iqbal Fahs, Jana Hayek, Seham Kanaan, Faten Hamed, Mariam Dabbous, Jihan Safwan, Mohamad Rahal, Fouad Sakr in Journal of Public Health Research
Footnotes
Ethical considerations
This research was conducted in full accordance with the principles outlined in the Declaration of Helsinki and the Ethical Guidelines for Life Science and Medical Research Involving Human Subjects. The study was observational and cross-sectional in nature and did not involve any invasive procedures or interventions. The study protocol was reviewed and approved by the Ethical and Research Committee at the Lebanese International University (LIU) under approval number 2024ERC-014-LIUSOP.
Consent to participate
Electronic informed consent was obtained from all participants prior to study enrollment, and survey access was granted only after participants confirmed their willingness to participate.
Author Contributions
IF conceptualized the study, had the responsibility of the project administration, planned the methodology, and carried out the statistical analyses. IF, MD, JS, FS and MR supervised the project. IF, JH, FH, and SK wrote the manuscript text. All authors reviewed and edited the text, and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data supporting the findings of this study are available from the authors upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.