
Abstract
Background
Primary dysmenorrhea has a main impact on quality of teenagers ‘life, productivity and daily activities. Due to the potential risks associated with pharmacological treatments, non-pharmacological approaches have gained importance in managing primary dysmenorrhea. In this study, isometric exercises and self-care activities were combined into a structured program aimed at alleviating menstrual pain.
Aim
The current study was conducted to evaluate the effect of isometric exercises and self-care activities on primary dysmenorrhea among secondary school students.
Design
A quasi-experimental research design was utilized.
Sample
A purposive sample of 97 secondary school students who had primary dysmenorrhea was recruited for the research for ten weeks.
Setting
two schools; Dr. Mohamed Rabie Falah Studied for Girls and Mohamed Nasr Abdeen Compound Schools at Diarb Negem City, Zagazig, Sharkia Governate.
Tools
three tools were used; 1) A structured Interview Questionnaire, 2) Visual Analogue Scale (VAS), and 3) Abdominal muscles force measuring tests.
Results
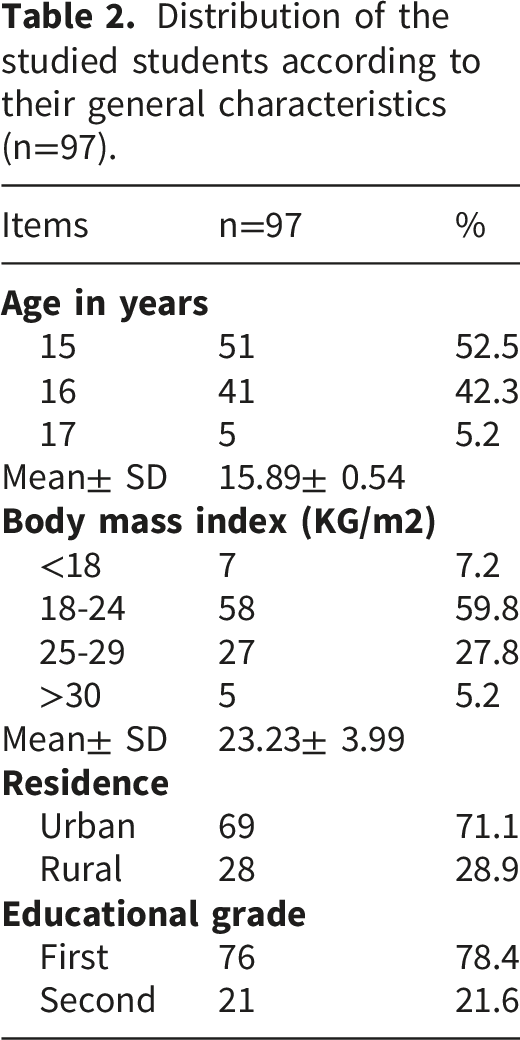
The mean age was of the studied students was15.89± 0.54 years. There was a highly statistical significant difference in pain intensity among studied students pre and post-intervention (p= 0.001). In which mean & SD of pain intensity pre-intervention was 7.61 ± 1.91 compared to 4.68 ± 2.39 post-intervention.
Conclusion
The study hypothesis was accepted. There were highly statistically significant differences pre and post intervention. A combined structured program of isometric exercises and self-care activities was effective for reducing intensity of primary dysmenorrhea among secondary school students.
Recommendation
Designing and implementing efficient programs to raise awareness of students about different benefits of isometric exercises and self-care activities on primary dysmenorrhea intensity.
Introduction
Dysmenorrhea is the most common gynecological complaint among female of reproductive age. It refers to painful menstruation that interrupts participation in daily living activity. 1 Dysmenorrhea can be classified into primary and secondary. Primary dysmenorrhea (PD) refers to painful menstruation without any underlying pelvic lesion and characterized by suprapubic colic-type pain that begins a few hours before or after the start of menstrual bleeding. 2 Whereas secondary dysmenorrhea is caused by several identifiable pathological conditions, such as endometriosis, adenomyosis, leiomyomas, and pelvic inflammatory disease and pain might begin before the start of menstrual bleeding and remain after its end from 8 to 72hrs. 3
Dysmenorrhea symptoms varies from one female to another; as many as 50-70% with symptoms such as cramps and pain in the pelvic area can be spread to the back and to the legs. 4 Additionally, menstrual pain significantly lower scores in physical and social functioning, role performance, bodily pain, and general health perception, leading to an overall reduced quality of life during menstruation. 5 There is a wide variety of management options of PD including pharmacological and non-pharmacological management. For the pharmacological management it is medically not recommended as it can interfere with renal function on long run period and decrease pain threshold. Also due to the high costs of pharmacological management, complications, and contraindications of some drug therapies in addition to the accessibility and public desire for using complementary treatments. 6
The non-pharmacological management is considered a modern investigation and research to strengthen the body and treat the disease without side effects. They include either self-care activities or isometric exercises and other complementary and alternative management. 3 The self-care activities can include eating fresh vegetables and fruits especially date palm fruits, drinking milk and eating its products, and drinking large amount of water. Also reducing physical activity, keeping warm, drinking warm beverages, avoiding cold drinks, spicy greasy foods, caffeine, and sugary foods. 2
In response to the limitations of pharmacological management including concerns about its side effects and the desire for natural alternatives, non-pharmacological interventions have received growing attention. Among these interventions, physical exercise has emerged as one of the most promising modalities. Exercise promotes endorphin release, improves pelvic circulation, relaxes uterine muscles, and reduce inflammation, all of which contribute to pain relieve. 7
Isometric exercises are a subcategory of exercises in which the length of the muscle and angle of the joint remains constant during contraction. Isometric exercises are those in which there is a change in muscle tension but no change in muscle length, no muscle or joint movement occur. Isometric exercises may have the potential mechanism of strengthening pelvic muscles, facilitating blood leakage and excreting waste containing prostaglandins, which cause excessive contractions. 8
Also, it stimulates the constant muscles, which are of A-delta type and C fibers, which in turn reduce the pain via pain inhibitory effects. In addition, regular exercise relieves stress and further reduces the activity of the sympathetic nervous system, which induces contraction and pain in the uterine muscles. 7 In addition, it is inexpensive as special facilities or equipment are not required, and it is not time-consuming. Hence, isometric exercise seems to be an appropriate nonpharmacological method for reducing the pain intensity of primary dysmenorrhea. It is easy and safe for females as it is non-invasive and implemented at low intensity. 2
There are few studies indicating that self-care activities can reduce menstrual cramps and associated symptoms; however, it is used in Europe to deal with health problems. Improvement of research evidence was found in quality, quantity, and reporting, but still more studies are needed, particularly for self-care activities. 9 The current low-quality evidence suggests that isometric exercises decrease the intense of pain during menstruation. So further researches are recommended. 10
Significance of the study
Dysmenorrhea is the most common cyclic pelvic pain. Globally, the prevalence of dysmenorrhea has been reported as 25% to 97%, and nearly 20% of cases have debilitating pain. A critical review found that 28% of women reported that their sleep was disturbed by menstrual cramps or pain during the first few days of menstruation. 11 Most females with primary dysmenorrhea experienced more depression, somatic, somatic-cognitive, gastrointestinal, self-esteem, anxiety and interest-desire problems. 12
Prevalence of primary dysmenorrhea in Mansoura city, Egypt was 91.9 % and 60 % of them had severe dysmenorrhea. Also, 84.5% of them had back pain and half of them were not able to concentrate at the class. In addition, (60%, 61.5%, 66%, & 66.7%) experienced anxiety, stress, mood swings and sadness respectively. 13 Although, Human Rights and Menstrual Health emphasize that women and girls have the inherent right to manage their menstruation without stigma. According to Sustainable Development Goals (SDGs), females have the right for good menstrual health (SDG-Goal3). Additionally, improving the surrounding environment will allow girls not to miss school, allowing them to have a quality of education (SDG-Goal4). 14
A recent study found that 49.1% of females reported that their sleep was disturbed by menstrual cramps or pain during the first few days of menstruation. 15 Also, primary dysmenorrhea increased the females’ rates of absenteeism from school, reduced participation in the class, group activities and assignments and poor time management. 16 So, the researcher decided to carry out this study.
Aim of the study
The current study aimed to evaluate the effect of isometric exercises and self-care activities on primary dysmenorrhea among secondary school students.
Research hypothesis
To fulfill the aim of the study, the following research hypothesis is formulated:
Secondary school students have less intensity of menstrual pain after receiving intervention than before.
Subjects and methods
Research design
A quasi-experimental research design (one group pre-post-test) was utilized to achieve the study’s aim. The study adhered to the guidelines provided in the TREND Statement Checklist. 17
Setting
The study was conducted at two schools; Dr. Mohamed Rabie Falah Studied for Girls and Mohamed Nasr Abdeen Compound Schools at Diarb Negem City, Zagazig, Sharkia Governate because they are the only secondary schools at Diarb Negem City. The first one was operated on an afternoon shift and works from 11.30 a.m. to 3.30 p.m. The second one was operated on a morning shift and works from 8.00 a.m. to 1.00 p. m. Students numbers in the first school included 500 students at the first grade and 300 students at the second grade. The second school student numbers included 193 students at the first grade and 122 students at the second grade. The third-grade students were not admitted to the school as it was not recommended for class work activities.
Sample
A purposive sample of 97 secondary school students selected from two secondary schools at Diarb Negem City, Zagazig, Sharkia Governate, Egypt. They were chosen according to inclusion & exclusion criteria. Inclusion criteria were students who; aged 15- 18 years, have normal body mass index, have regular menstrual cycle, and have dysmenorrhea rating their pain ≥4 on Visual Analogue Scale. Exclusion criteria was students who have psychological or gynecological disorders that effect on menstrual pain.
Sample size
The sample size for studying primary dysmenorrhea, was calculated using research software (https://clincalc.com). Based on the results of a similar previous study done by ElShora, Abd Elnabi, & Elbeltagy, (2023), that noticed a significantly improvement in the intervention group than in the control group after 8 weeks of performing exercises, to calculate the sample size with precision/absolute error of 5% and type 1 error of 5%, Sample size is calculated according to the following formula.



Tools for data collection
Three tools were used.
Structured interviewing questionnaire
This tool was developed by the researcher after reviewing the literature review. 3 , 18 , 9 It consisted of two parts: a) The first part: General characteristics of studied students such as: (age, body mass index, residence and educational grade categories…etc). b) The second part: Menstrual characteristics of studied students such as: (menarche age, frequency of menstrual cycle, duration of menstrual flow, first experience of dysmenorrhea, frequency of dysmenorrhea, onset of pain at each period, total duration of pain in hours, rest during the time of dysmenorrhea, number of pads per day during menstruation, menstrual blood loss, skipping meals during dysmenorrhea and measures taken during each cycle to get relief from pain…etc).
Visual Analogue Scale (VAS)
It was adopted from Crichton (2001) and used to assess the menstrual pain severity. Scores are based on self-reported pain measurements that are recorded with a single hand-written mark placed at one point along a 10-cm line that represents a continuum between the two ends of the scale, with “no pain” on the left end (0 cm) and the “worst pain” on the right end (10 cm). This tool scoring system was divided into three main sections; the first section was graded from 1-3 cm, which represents mild pain; the second section was rated from 4-7 cm, which represents moderate pain; and the third section was graded from 8-10 cm, which represents severe pain. Higher scores indicate the worst pain.
Abdominal muscles force measuring for studied students
This tool developed by the researcher after reviewing the literature review (Brhm & Abo Nmra, 1995) It consist of three tests: a) First test; sit-up-Legs Straight test in 20 seconds that aimed to measure the muscle strength of the abdominal muscle groups and the trunk flexor muscles. The instruments used were stopwatch to determine time assumed and neat or level which are a small table that used to evaluate the flexibility of leg and back muscles. Performance Specifications: The student laid on her back on the mattress (or flat surface) with her feet open by 30 cm. So that the palms touch the neck from behind and the elbows are bent (a colleague stabilizes the legs). Immediately upon hearing the start signal, the student bended the torso to reach a tall sitting position with the knees bent according to the last modification, then repeated this as many times as possible in twenty seconds. Test instructions: Both knees or one of them must not be bent at all during performance. The student must not stop during the performance. Registration: The researcher recorded the number of correct times performed in 20 seconds. b) The second test; test of raising the legs high at a 45-degree angle that aims to measuring of static muscle endurance of the abdominal flexor muscles and trunk flexor muscles. The instrument used was stop watch to determine time assumed. Performance Specifications: The student assumed a lying position on the back with the hands placed aside and the legs together at their length, then raises the legs together high at an angle of 45 above the ground and remains in this position for as long as possible. Test instructions was the time calculation begins as soon as the tester takes a stable position and raises her legs high. The time calculation stops when the feet are apart from each other, or when the legs are lowered or raised high. One attempt for every student. Registration: The student’s score is based on the number of seconds it records when maintaining the correct performance mode. c)The third test; bending the torso forward from standing that aimed to measuring the flexibility of the spine on the horizontal axis. The instruments used were a chair without a back, fifty (50) cm high and a non-flexible ruler, divided from zero to one hundred (100) cm, fixed vertically on the seat so that the number (50) is parallel to the surface of the ruler and the number (100) is parallel to the lower edge of the seat and a wooden pointer that moves on the surface of the ruler. Performance Specifications: The student stood on the bench with her feet together, placing the toes on the edge of the bench, and keeping the knees straight. The student bended her torso forward and down so that she pushed the pointer with her fingertips as far as possible and remained at the last distance she reached for two seconds. Directions was the student has two attempts, the best of which is recorded, the torso must be flexed slowly and the researcher must hold still at the last distance the student reached for two seconds. Registration: The researcher recorded the distance achieved in the two attempts and calculated the greater distance in centimeters.
Tools validity and reliability
Data collection tool was tested and juried for the content validity by five specialists in Woman’s Health and Midwifery Nursing and the recommended modifications were done. Some modifications were done to the structured interview questionnaire (i.e.,changing in the ordering and sequences of some sentences and paraphrasing of some sentences) and the final form was utilized for data collection. The tools were tested for reliability by using Cronbach’s alpha test in statistical package for social science (SPSS) version 23. The Cronbach’s alpha value (internal consistency) of the psychological well-being tool was (0.87) which indicated high reliability. The test R-test was used for physical tests tool (Sitting up from lying down in 20 seconds, Raising the legs high at a 45-degree angle and the trunk bent forward from the lying position) were (0.88 - 0.92 - 0.90) and (0.92) for Numeric Rating Scale.
Pilot study
The pilot study was conducted prior to data collection on 10% of students (10) to evaluate the clarity and applicability of these tools to confirm that the questions of the tools were consistently delivered to the studied students and carried the intended meaning they were designed to achieve. It also helped to estimate the time needed to complete the questionnaire.
Ethical consideration
An ethical approval letter was obtained from the Research Ethics Committee of Faculty of Nursing, Mansoura University (IRP. No.478). An official permission and approval for conducting the study was obtained from the Dean of Faculty of Nursing, Mansoura University and from the head of Educational Management and from the managers of Dr. Mohamed Rabie Falah School for Girls and Mohamed Nasr Abdeen Compound Schools at Diarb Negem City. Then an informed written consent was obtained from all studied parents’ students after explaining the objectives of all the study to everyone. Participant assent was also secured after providing students with age-appropriate information regarding the study. All studied students were assured that their participation in the study was voluntary and the collected data was treated confidentially and students were informed that they have the right to withdraw from the study at any time without giving any reason.
Procedure
The data collection was conducted from the beginning of October 2024 to the end of December 2024 through four phases; planning and designing, initial baseline assessment, implementation, and evaluation and follow up phases.
The planning and designing phase included taking the official permissions from Research Ethics Committee of Faculty of Nursing, Mansoura University (IRP. No.478) and then from the head of Educational Management and from the managers of the previously mentioned setting.
The researcher designed a colored instructional booklet in a simple Arabic language after reviewing Arabic and English literatures. Considering students’ culture, the educational booklet was designed at an appropriate reading level and in a culturally appropriate style. Photos were added to it to provide further illustration and to aid the students in understanding the material.
The researcher prepared the educational and training content after reviewing national and international literatures related to the topic. 3 , 18 , 9 The researcher insured that all students have a smart phone with WhatsApp. The researcher created a WhatsApp group included contact number of all studied students to plan for the sessions and upload the educational and training materials.
The initial baseline assessment phase was interviewing of the studied students at the previously mentioned setting three days per week (Sunday, Tuesday, Thursday) according to their shift of work (morning or afternoon) for 10 weeks. The studied students were selected based on the previously mentioned inclusion& exclusion criteria. Then the researcher assessed the students’ eligibility to participate in the study. The researcher made a list of eligible students and the students signed a written consent to share in the study after explanation of the nature and aim of the study.
Then the pre-test measures were conducted (to collect the base line data) for the students. The researcher asked the studied students to fill in the first two tools to cover general characteristics and menstruation characteristics. Then the researcher measured the students’ abdominal muscles strength by applying the physical tests using tool III.
The implementation phase; after baseline assessment (pre-test), the researcher attended the second school (morning shift) three days per week (Sunday, Tuesday, Thursday) from 8:00 a.m. to 10:00 a.m. and the first school (afternoon shift) from 10:30 a.m. to 1:30 p.m. for 10 weeks for implementation of the program sessions. The program sessions consisted of ten sessions; two theoretical and eight practical sessions. Theoretical sessions declared the isometric exercises benefits, types and how to perform. In addition, it clarified types of self-care activities. While, the practical sessions included eight training sessions related to isometric exercises which started with simple exercises and gradually increased in strength to help in relieve of primary dysmenorrhea.
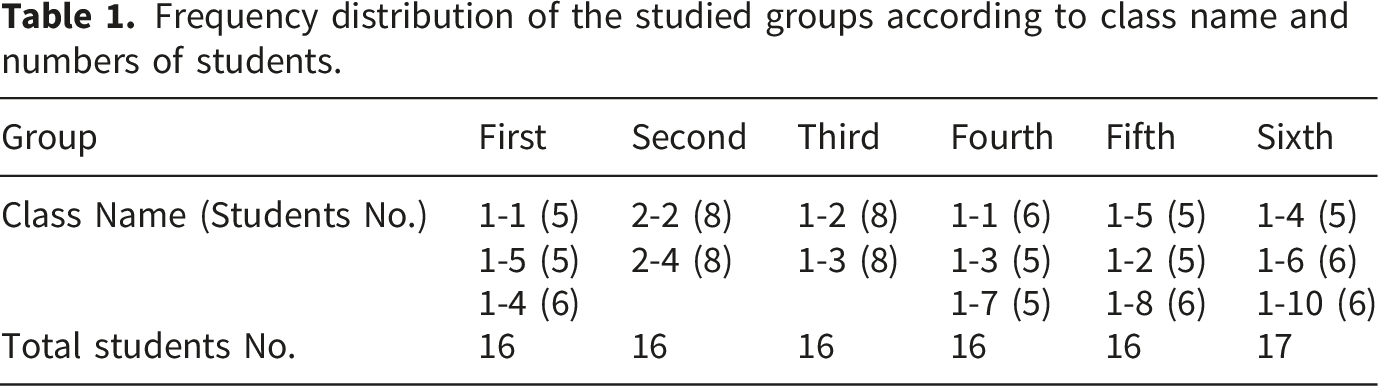
The researcher divided the students into six groups to facilitate the implementation of the happiness sessions (three groups for the second school (first, second and third groups) and three groups for the first school (fourth, fifth and sixth groups):
Then the researcher provided an illustrative booklet with types of isometric exercises, duration and intervals. The researcher documented the frequency of performance for all the group on a follow up diary. The program sessions included self-care activities sessions and isometric exercises sessions. The self-care activities sessions: it included two theoretical sessions. The first theoretical session: The researcher welcomed and introduced these elements to the students: (Introduction about primary dysmenorrhea, types of dysmenorrhea, definition of primary dysmenorrhea, signs and symptoms of primary dysmenorrhea, causes of primary dysmenorrhea, ways to alleviate pain in primary dysmenorrhea, a brief overview of the self-care activities to decrease primary dysmenorrhea, a brief summary of isometric exercises and their main importance for primary dysmenorrhea and a brief overview of the program for isomeric exercises).
The second theoretical session: Self-care activities to reduce primary dysmenorrhea were discussed, such as: (applying warm compresses on the abdomen and back, engaging in sports such as brisk walking, cycling, swimming or any other aerobic activity for at least 30 minutes most days of the week, drink plenty of water, drink a lot of warm drinks, such as lemon, ginger, mint, anise, fennel, and caraway, avoid drinking too much caffeine, get rid of stress by: (getting plenty of sleep, practicing progressive muscle relaxation or deep breathing exercises to help reduce headaches, anxiety, or disturbed sleep (insomnia) and doing exercises to relax and relieve stress) and modify the diet by: (eating smaller, more spaced meals to reduce bloating and feelings of fullness, reducing the intake of salt and salty foods to reduce bloating and retain fluids, choosing foods high in complex carbohydrates, such as fruits, vegetables, and whole grains and choosing foods rich in calcium, such as eggs, cheese, yoghurt, fish and sesame).
The isometric exercises sessions: it included eight practical sessions; each session consisted of four parts; warm-up exercises, flexibility exercises, main part and relaxing exercises. The warm-up exercises used for warming the body and avoiding injury it included three exercises for five minutes. The flexibility exercises used for helping for elastic muscles and joints. It was two exercises for five minutes every one for 2.5 minutes. The main part consisted of five isometric exercises. It was for 30 minutes every exercise was for 6 min. The relaxing exercises was used for relaxing and calming the body after the end of the practicing session. It consisted of two exercises for five minutes 2.5 min for everyone.
Frequency distribution of the studied groups according to class name and numbers of students.
Statistical design
Collected data were analyzed by assigning codes and then entering them into a computer for tabulation. All statistical analyses were performed using SPSS for windows version 23.0 (SPSS, Chicago, IL). Continuous data were normally distributed and were expressed in mean ±standard deviation (SD). Categorical data were expressed in number and percentage. Chi-square test (or fisher’s exact test when applicable) was used for comparison of variables with categorical data. The reliability (internal consistency) test such as Cronbach’s alpha test for the questionnaires used in the study was calculated. Statistical significance was set at p≤0.05.
Results
Distribution of the studied students according to their general characteristics (n=97).
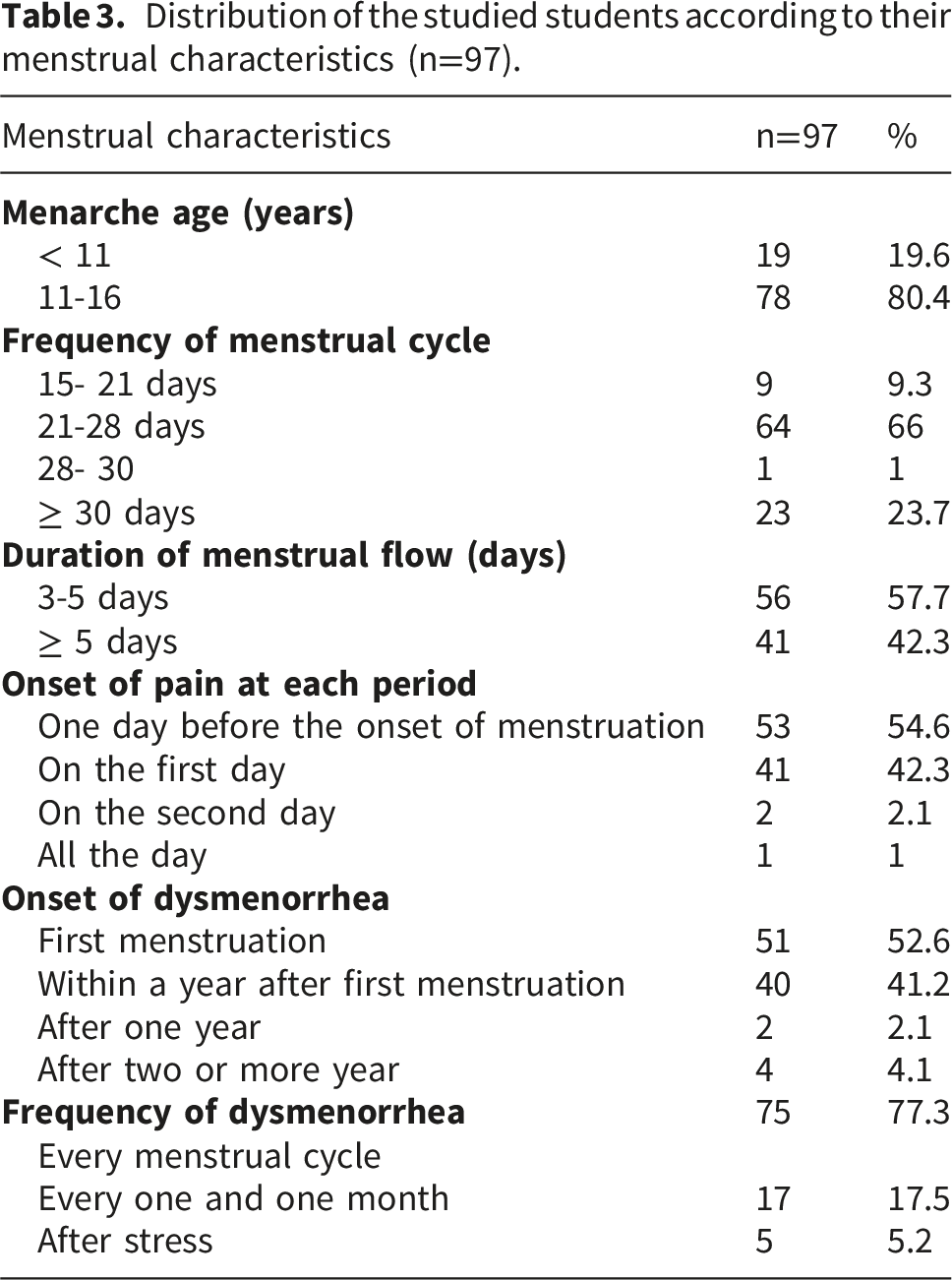
Distribution of the studied students according to their menstrual characteristics (n=97).
Comparison of dysmenorrhea relief measures among the studied students pre and post-intervention (n=97).
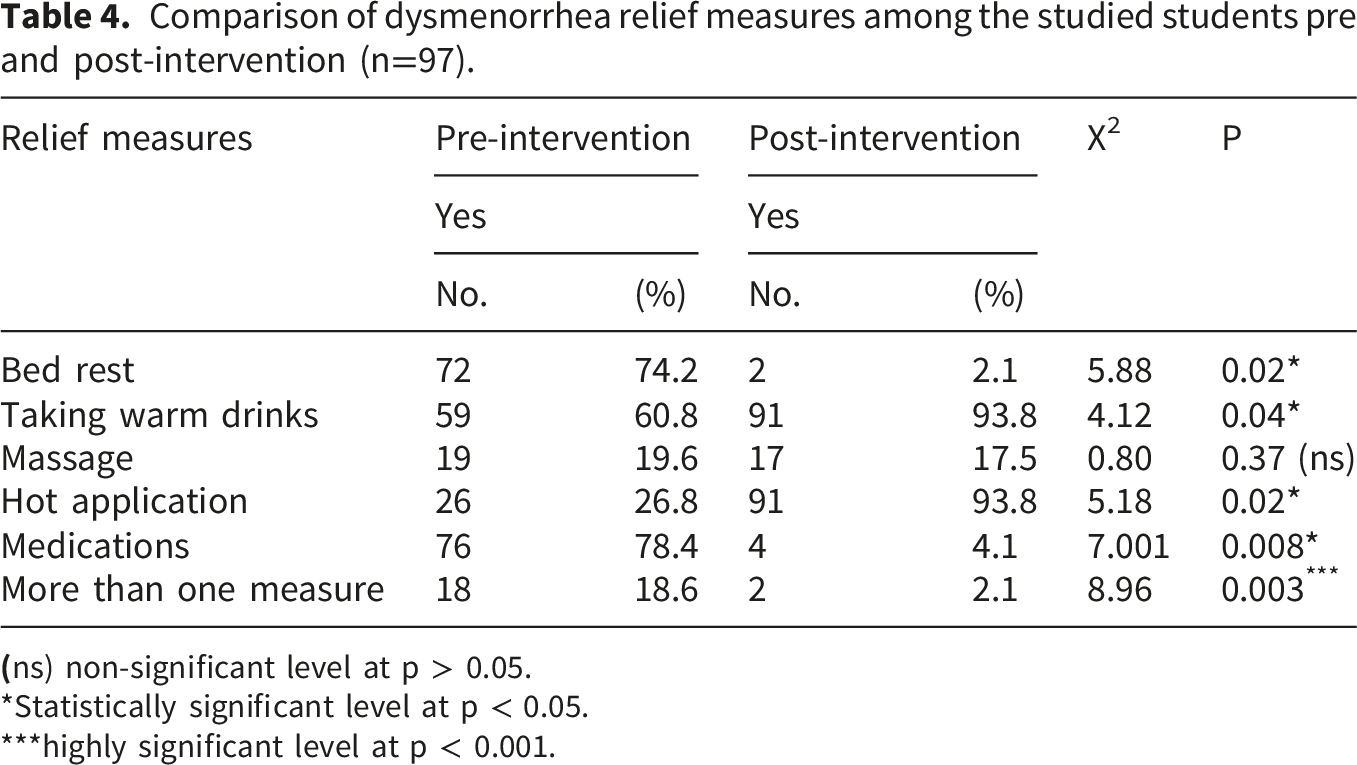
*Statistically significant level at p < 0.05.
***highly significant level at p < 0.001.
Comparison of mean differences of pain intensity among studied students pre and post intervention (n = 97).
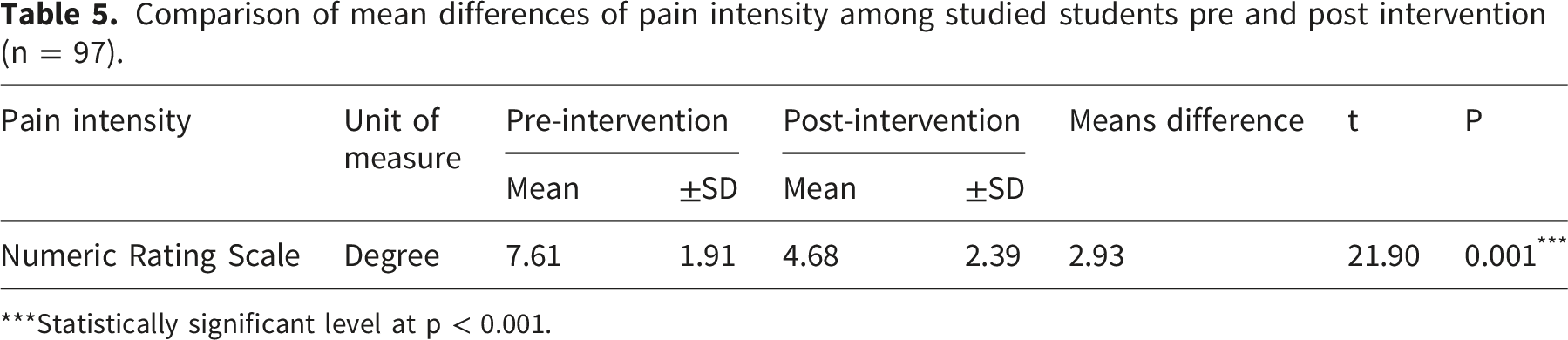
***Statistically significant level at p < 0.001.
Figure 1 Illustrates that 56.7% of the studied students had severe pain pre-intervention compared to 11.3% of them post-intervention. Also, 43.3% of the studied students had moderate pain pre-intervention compared to 35.1% of them post-intervention. While 27.8%& 25.8%, respectively of the studied students had mild and no pain post-intervention. Levels of dysmenorrhea pre and post-intervention among the studied students (n= 97).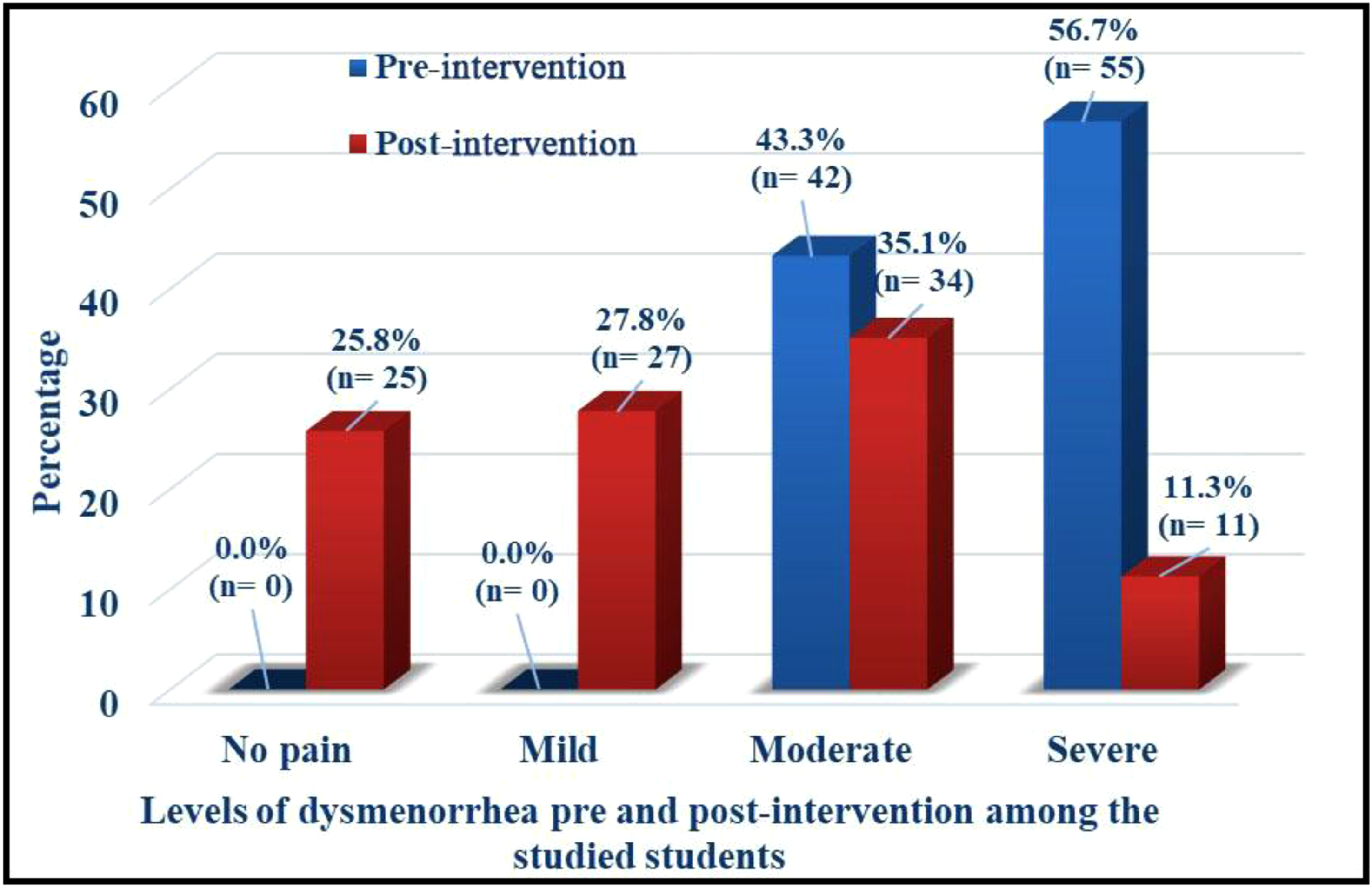
Correlation coefficient between the results of the post-intervention of the physical tests, the psychological well-being, and Dysmenorrhea (n= 97).
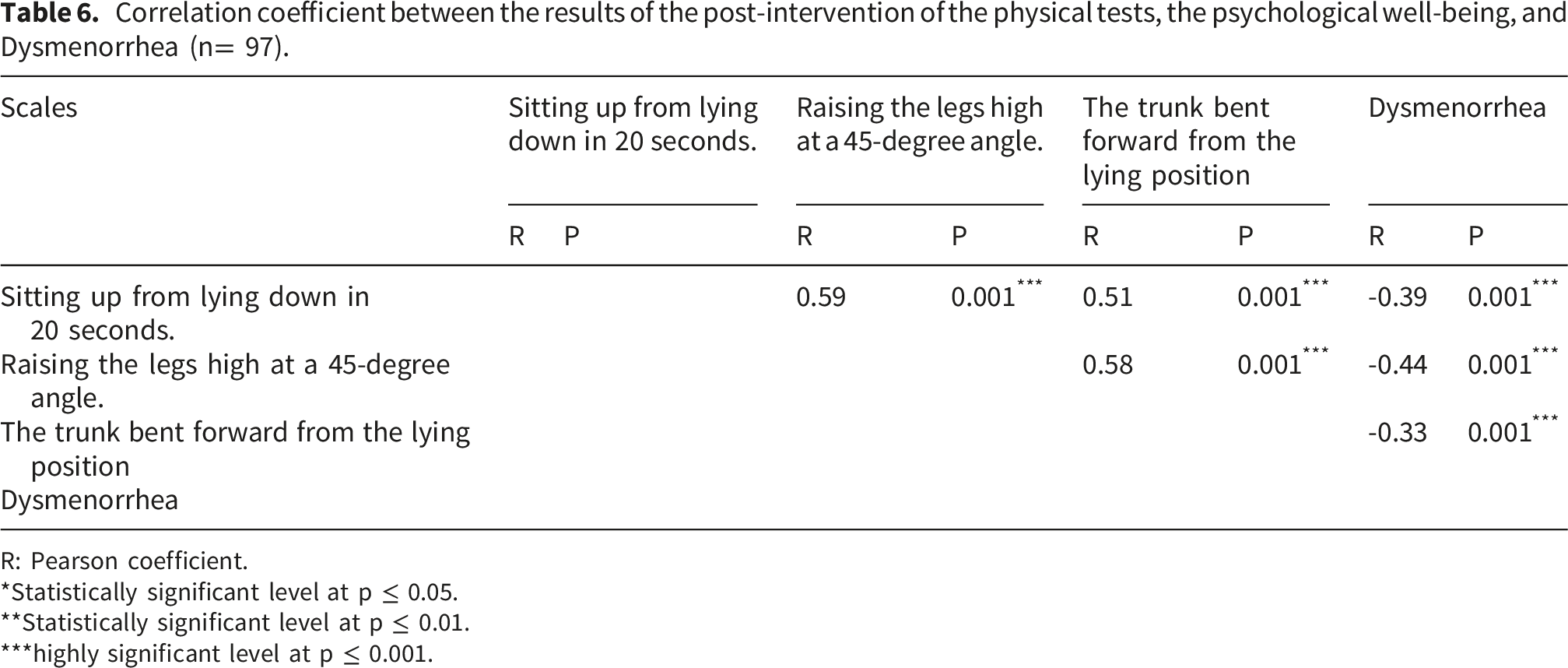
R: Pearson coefficient.
*Statistically significant level at p ≤ 0.05.
**Statistically significant level at p ≤ 0.01.
***highly significant level at p ≤ 0.001.
Discussion
The present study aimed to evaluate the effect of isometric exercises and self-care activities on primary dysmenorrhea among secondary school students. From our best knowledge it is the first study that examined the effect of isometric exercises and self-care activities on primary dysmenorrhea. The aim and the hypotheses of the study were supported by the study findings which highlighted that the intensity of menstrual pain was decreased after performing intervention sessions.
The study findings attributed to the effectiveness of intervention sessions content and the clarity of the educational, practical sessions after eight weeks of isometric exercises and two weeks of self-care activities three times per week and each time lasting for 45 min. Regarding the supporting studies that utilized isometric exercises on primary dysmenorrhea intensity and duration an experimental study conducted by 6 in Malaysia who evaluated the effect of isometric exercises in reducing the intensity and duration of primary dysmenorrhea among young females and showed that there were significantly reduction of intensity and duration of pain after eight weeks of isometric exercises.
In addition, the present study findings were supported by an Egyptian study conducted by 19 who investigated the impact of isometric exercises on menstrual pain severity and showed that there was a significantly reduction in menstrual pain intensity after intervention. Also, the present study finding was supported by an Egyptian study conducted by 18 who assessed the effect of a group of merged exercises on primary dysmenorrhea. The researchers reported that eight weeks of a group of merged exercises program was effective in reducing pain severity.
Additionally, the present study findings were supported by 20 who compared Pilates and yoga’s effectiveness in managing menstrual pain, absenteeism, and sleep quality among Primary Dysmenorrhea School Students and reported that Pilates and yoga effectively alleviate dysmenorrhea symptoms, reduce absenteeism, and enhance overall wellbeing among adolescent females.
Moreover, a systematic review and network meta-analysis conducted by 21 to assess the effect of non-pharmacological interventions for primary dysmenorrhea and showed that exercise was the most effective non-pharmacological intervention for reducing menstrual pain. Also, a recent systematic review and meta-analysis conducted by 22 to evaluate the impact of exercise on pain severity in individuals with primary dysmenorrhea and showed that eight weeks exercise with sessions occurring more than three times per week and lasting for thirty minutes was effective in reducing pain intensity of primary dysmenorrhea.
Furthermore, the present study findings revealed that there were highly statistical significant differences between pre-post intervention in skipping meals during dysmenorrhea except breakfast meal. The present study findings were supported by a study conducted in Indonesia by 23 to discover the association between breakfast and dysmenorrhea. The researchers reported that there was no significant association.
Concerning the supported studies that utilized self-care activities on primary dysmenorrhea, an Egyptian study conducted by 3 to evaluate the effect of self-care activities on primary dysmenorrhea and showed that it was very effective in relieving primary dysmenorrhea. In addition, a systematic review was conducted by 24 to assess the effect of oral and topical ginger as a part of self-care activities on primary dysmenorrhea and showed that it was effective intervention for pain relief in primary dysmenorrhea.
Another supported study conducted by 25 to assess the risk factors of primary dysmenorrhea and the effect of complementary and alternative methods in female students especially abdominal hot application, taking hot shower and ginger consumption and were effective in reducing pain in primary dysmenorrhea.
Not only improving the teenagers’ female students’ awareness about how to deal with primary dysmenorrhea by performing the recognized self-care activities during this period but also improve physical fitness by applying isometric exercises can decrease the intensity and duration of menstrual pain. So, the present study findings proved that happiness sessions are effective in decreasing intensity of primary dysmenorrhea.
Conclusion
In summary, this study employed a quasi-experimental design (one group pre-posttest). The main objective of the study was to examine the effect of isometric exercises and self-care activities on primary dysmenorrhea among secondary school students. Based on the present study findings, it is concluded that the study hypothesis was accepted. There were highly statistically significant differences pre and post intervention. A combined structured program of isometric exercises and self-care activities was effective for reducing intensity of primary dysmenorrhea among secondary school students.
Recommendation
In light of the study`s findings, the following are recommended: - It is recommended that students perform isometric to reduce the negative impacts of primary dysmenorrhea. - Designing and implementing effective programs to raise students’ awareness regarding the various benefits of isometric exercises and self-care activities on primary dysmenorrhea intensity.
Limitations of the study
This study has several limitations that should be acknowledged. First, the research employed a one-group pre-post design without a control group, which limits the ability to attribute observed improvements solely to the intervention. Second, the sample was drawn from a single geographical area, which may reduce the generalizability of the findings to broader populations. Third, the data relied on self-reported measures, which are subject to recall bias and social desirability bias. Additionally, the short follow-up period did not allow assessment of the long-term sustainability of the intervention`s effects. Finally, variations in students’ baseline physical activity levels, pain tolerance, and adherence to the sessions may have influenced the outcomes. These limitations should be taken into consideration when interpreting the results and highlight the need for future studies.
Footnotes
Acknowledgements
The authors would like to thank all the students who participated in this study.
Ethical considerations
All methods were conducted in accordance with relevant guidelines and regulations. Ethical approval was obtained from the Research Ethics Committee of nursing faculty, Mansoura University (IRP. No. 478). Informed consent was obtained from all participants involved in this study.
Author contributions
All authors contributed significantly to drafting the manuscript or critically revising it for important intellectual content. All the authors contributed equally to the conceptualization, design, analysis, and preparation of the manuscript. The Researchers W.A, E.F, T.E and H.E collected the collection.
Funding
This research paper was conducted without external funding or financial support.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Data Availability Statement
The corresponding author will provide the data supporting the study’s findings upon a reasonable request.