
Abstract
Background
The COVID-19 pandemic exposed critical gaps in health workforces and highlighted the need to strengthen pandemic preparedness and response within health professions education. This study examines pandemic preparedness within undergraduate biomedical and health sciences education in Georgia and identifies strategies for strengthening future preparedness and response.
Design and Methods
A mixed-methods design integrated findings from four related studies. Quantitative data were collected and analyzed from final-year students (n = 296) and alumni graduating between 2015 and 2024 (n = 203), assessing perceived preparedness, COVID-19 response participation, and pandemic-related competencies. Qualitative data were collected and analyzed through semi-structured interviews with Georgian educators and curricular committee members (n = 30) and public health experts (n = 21) to identify priorities for curricular reform.
Results
Student preparedness was moderate (M = 3.50, SD = 1.14), while alumni reported lower overall preparedness (M = 2.95, SD = 1.15). Practical skills showed the strongest association with preparedness among students (r = .739), whereas pandemic-related knowledge was the strongest correlate among alumni (r = .698). Participation in COVID-19 response activities and extracurricular training was associated with higher preparedness in both groups. Qualitative findings revealed fragmented curricular integration and emphasized the need for structured training, simulation-based education, experiential learning, interdisciplinary collaboration, and stronger public health communication competencies.
Conclusion
Embedding pandemic preparedness and response competencies into undergraduate biomedical and health sciences education represents a proactive strategy to strengthen health workforce capacity and build more resilient health systems for future public health emergencies.
Keywords
Introduction
The COVID-19 pandemic exposed significant gaps in health workforce preparedness across countries and health systems. Despite differing national responses, no country was fully prepared for the scale or duration of the crisis, and although COVID-19 is no longer classified as a pandemic emergency, SARS-CoV-2 continues to circulate globally while the emergence of future pandemics remains unpredictable. 1 These challenges occurred alongside longstanding workforce shortages, with the World Health Organization (WHO) projecting a global deficit of approximately 18 million healthcare workers by 2030, particularly in low- and middle-income countries. 2 During COVID-19, these shortages intensified, contributing to service disruptions and increased risks for healthcare workers. 3 These systemic burdens highlighted a fundamental gap: health systems cannot respond effectively to pandemics without a workforce that is adequately prepared before crises occur.
Pandemics place extraordinary demands on health systems, frequently causing workforce shortages, high infection rates among healthcare personnel, and disruptions in service delivery. 4 As a result, contemporary preparedness frameworks increasingly emphasize workforce development, interdisciplinary collaboration, and sustained investment in training as central components of health system resilience.5,6 Within this context, undergraduate biomedical and health sciences education has gained recognition as both a foundational approach and a proactive mechanism for strengthening preparedness capacity. Structured disaster and emergency preparedness training has been shown to significantly improve students’ perceived readiness, risk assessment abilities, and confidence in responding to emergencies, 7 while educational approaches integrating simulation-based learning, competency-based instruction, and interdisciplinary training have demonstrated improvements in preparedness knowledge and practical skills among health professions students. 8 Despite these advances, key preparedness-related competencies remain unevenly integrated into undergraduate curricula, underscoring the need to evaluate how well future health professionals are being prepared for pandemic response.
Within this broader global landscape, Georgia offers a particularly relevant yet underexamined case for exploring pandemic preparedness and response within a health system undergoing structural transition. As an upper-middle-income country, Georgia faces persistent health system challenges, including workforce imbalances, weaknesses in primary health care, uneven urban-rural access to services, and a critically low nurse-to-physician ratio of approximately 0.3:1.9,10 During the COVID-19 pandemic, the country implemented early containment measures and expanded surveillance, testing, and emergency coordination through national public health institutions.11,12 However, subsequent waves exposed systemic vulnerabilities, including workforce shortages, hospital system pressure, and difficulties related to vaccine uptake and public trust. 13 By 2022, Georgia had recorded more than 1.8 million confirmed COVID-19 cases and nearly 17,000 deaths. 14
Amid these pressures, universities took an active role in supporting the national response, with more than 1,800 final-year medical students mobilized to assist with surveillance, contact tracing, and teleconsultations. 15 While these initiatives demonstrated institutional adaptability, they were largely reactive and highlighted the lack of systemic preparedness frameworks embedded within undergraduate curricula. This is reflected in evidence showing that pandemic preparedness content across Georgian biomedical and health sciences programs remains fragmented, often limited to individual courses such as epidemiology or infectious diseases, without explicit preparedness learning outcomes or interdisciplinary training.9,16 However, understanding and evaluating how effectively undergraduate education prepares future health professionals for pandemics requires a multi-level perspective that goes beyond individual participant perspectives and isolated curricular components to consider broader educational, institutional, and workforce contexts.
To address this gap, the present mixed-methods study integrates quantitative data from final-year students and alumni with qualitative evidence from Georgian educators, curricular committee members, and public health experts. The study was conducted as part of doctoral research entitled Strengthening Pandemic Preparedness and Response through Undergraduate Education in Biomedical and Health Sciences. By combining preparedness outcomes measured among students and graduates with educator and expert insights on curricular content, implementation constraints, and reform priorities, the study produces a multi-level synthesis of preparedness outcomes across educational, institutional, and public health dimensions. To our knowledge, no prior study has integrated quantitative preparedness assessments from both students and alumni with qualitative insights from educators, curricular committee members, and public health experts within a unified analytical framework in this context.
By examining preparedness across cohorts graduating before, during, and after the COVID-19 pandemic, the study explores how effectively undergraduate biomedical and health sciences education in Georgia prepares future health professionals for pandemic prevention, communication, and response. Specifically, the study aims to: 1. assess perceived pandemic preparedness competencies among biomedical and health sciences students and alumni in Georgia; 2. evaluate the extent to which pandemic preparedness competencies are integrated within undergraduate biomedical and health sciences curricula in Georgia; and 3. identify priorities and opportunities for strengthening pandemic preparedness and response education within Georgian higher education institutions. The findings aim to generate evidence-based recommendations for strengthening pandemic preparedness education, health workforce preparedness and health system resilience in Georgia and comparable settings.
Design and methods
Mixed-methods synthesis
This manuscript synthesizes findings from four independent studies on pandemic preparedness in undergraduate biomedical and health sciences education in Georgia. The studies included quantitative surveys of final-year students and alumni, qualitative research with Georgian educators and curricular committee members, and interviews with public health experts. Each study was designed, conducted, and analyzed independently before integration.
A mixed-methods synthesis was particularly important for this research because pandemic preparedness in health professions education is a complex and multidimensional issue that cannot be fully understood through a single methodological approach. Quantitative findings provided measurable evidence on perceptions, preparedness levels, and educational gaps, while qualitative findings offered deeper insight into curricular decision-making, institutional challenges, expert perspectives, and system-level needs.
The findings were integrated using a convergent mixed-methods framework, allowing identification of cross-study patterns, contextualization of quantitative results within institutional and expert perspectives, and development of evidence-based recommendations for strengthening pandemic preparedness education in Georgia. Integration was conducted by the primary researcher in collaboration with the doctoral supervisor to ensure analytical consistency and strengthen interpretation across all four study components.
This manuscript represents a distinct contribution that extends beyond any individual component study. While the qualitative findings from Georgian educators and curricular committee members have been previously published and the quantitative findings from final-year students are currently under consideration elsewhere, the alumni survey and public health expert data have not been previously published or submitted. None of the individual studies synthesized findings across all four datasets within a unified analytical framework, and the present manuscript therefore provides a novel multi-level analysis that could not have been achieved through any single study alone. The reporting of this study conforms to the GRAMMS guidelines for Good Reporting of A Mixed Methods Study. 17 [See Supplementary File #3].
Quantitative components
Two cross-sectional surveys were conducted as part of the quantitative component of this study: one targeting final-year students and the other targeting alumni of Georgian biomedical and health sciences programs. Both instruments were developed through a systematic and iterative process. Following a structured review of previously published, piloted, and validated instruments related to pandemic preparedness and health professions education, relevant items were selected, adapted, and contextualized to reflect the Georgian educational setting. This process involved multiple rounds of review by both researchers. All items underwent forward and backward translation by a certified professional translation company to ensure linguistic equivalence. The finalized instruments were reviewed and approved by the institutional ethics committee prior to administration. Although the instruments were not formally pilot tested, they were grounded in previously validated scales and further refined through a rigorous iterative development process. Informed consent was obtained from all participants prior to their inclusion in the study (Supplementary File 1) (Supplementary File 2).
Final-year student survey
Eligible participants included final-year students in medicine, dentistry, nursing, pharmacy, and public health expected to graduate in 2024. Exclusion criteria comprised students not in their final year of study, students not expected to graduate in the 2023–2024 academic year, and students not enrolled in the specified programs. Participants were recruited through purposive sampling via institutional channels and networks, including deans’ and administrative offices. Data were collected between April and October 2024 through online questionnaires distributed via institutional mailing lists and in-person recruitment at participating universities. A total of 302 responses were received, with 296 retained after exclusion of incomplete submissions. The survey included demographic variables, participation in COVID-19 response activities, and perceived pandemic preparedness, measured using a 20-item Likert-scale instrument assessing theoretical knowledge, preventive competencies, and clinical and practical preparedness. Internal consistency was high across both factors (Cronbach’s α = .96 and .93), and exploratory factor analysis confirmed the structural validity of the scale.
Alumni survey
Eligible participants included graduates from medicine, dentistry, nursing, pharmacy, and public health programs who graduated from Georgian biomedical and health sciences programs between 2015 and 2024. Exclusion criteria comprised individuals who graduated outside this period and specified programs. Participants were recruited through purposive sampling via alumni networks and targeted outreach. Data were collected between April 2024 and December 2025. A total of 208 responses were collected, of which 203 were included after data screening. The survey captured demographic characteristics, COVID-19 response participation, extracurricular pandemic-related training, and perceived preparedness using a 10-item Likert-scale instrument assessing foundational knowledge and practical preparedness. The scale demonstrated high internal consistency (Cronbach’s α = .934), and exploratory factor analysis supported a two-factor structure accounting for 71.6% of total variance.
Quantitative data analysis
Quantitative analyses were conducted using IBM SPSS Statistics version 30.0 for the student dataset and version 31.0 for the alumni dataset. Descriptive statistics were calculated for all variables. Exploratory factor analysis using principal axis factoring with oblimin rotation examined the structure of preparedness measures, and internal consistency was assessed using Cronbach’s alpha. Correlations examined associations between competencies and preparedness. Group differences were analyzed using independent samples tests and analysis of variance. Multiple linear regression identified predictors of preparedness, and logistic regression examined factors associated with willingness to participate in future pandemic response activities. Statistical significance was set at p < .05.
Qualitative components
Two qualitative studies were conducted as part of this research: one involving public health experts and the other involving Georgian educators and curricular committee members. Trustworthiness was established through multiple complementary strategies. Credibility was enhanced through purposive sampling, thematic saturation, and the use of verbatim participant quotations. Dependability was supported by iterative coding, repeated recoding, and systematic documentation of analytic decisions to ensure consistency throughout theme development. Although coding was conducted by the primary researcher, analytical rigor was strengthened through multiple rounds of independent review, with codes and themes revisited and refined iteratively until consistency was achieved. Confirmability was strengthened by grounding interpretations in direct participant quotations, thereby reflecting authentic respondent perspectives. Transparency was maintained through comprehensive audit trails and supplementary descriptive analyses, including word frequency and code co-occurrence mapping, to support pattern identification and thematic refinement.
Public health expert interviews
Semi-structured interviews were conducted with public health experts between August 2024 and September 2025. Participants were purposively sampled based on expertise in public health policy, global health, or health professions education and were based in Georgia and comparator countries including the United States, United Kingdom, Germany, Australia, Denmark, and Armenia. Interviews were conducted via Zoom or collected as written responses using the same interview guide addressing preparedness competencies, curricular priorities, and lessons from COVID-19. Interviews were recorded where applicable and transcribed verbatim.
Educator and curricular committee interviews
Additional qualitative data were collected from Georgian educators and curricular committee members involved in biomedical and health sciences education across medicine, nursing, pharmacy, dentistry, and public health programs. Data were gathered through semi-structured interviews and written responses between May and August 2024. Responses from three international curricular experts based in Germany, Belgium, and Armenia were excluded from thematic analysis and used only for triangulation. Questions addressed curricular structure, preparedness-related content, and opportunities for curricular reform.
Qualitative data analysis
Qualitative data were analyzed using inductive reflexive thematic analysis in ATLAS.ti version 23.2.1 and MAXQDA24 version 24.5.1. The process included familiarization, coding, iterative theme development, and refinement. Coding and theme development were conducted by one researcher, with saturation determined through thematic redundancy. Quantitative findings did not inform qualitative coding decisions.
Ethical considerations
Ethical approval was obtained from the Biomedical Research Ethics Board of the University of Georgia, School of Health Sciences (Approval No. N:11-6461). Participation was voluntary and informed consent was obtained from all participants prior to inclusion.
Results
Final-year students
A total of 296 valid responses were analyzed across five disciplines. Most respondents were aged 18–22 years (63.5%), followed by 23–27 years (31.4%) and ≥27 years (5.1%). The sample was predominantly female (69.3%), with 28.4% male and 2.4% preferring not to disclose gender. Most respondents were enrolled in medicine (65.5%) or dentistry (29.1%), with smaller proportions from public health (3.0%), nursing (2.0%), and pharmacy (0.3%).
Overall perceived pandemic preparedness was moderate (M = 3.50, SD = 1.14, 95% CI [3.37, 3.63]). Based on the single item measure, 18.9% of students reported being unprepared, 23.6% were neutral, and 57.4% reported being at least somewhat prepared. Across the 20 preparedness items, mean scores ranged from 2.95 to 4.02. The highest scores were observed for hygiene knowledge (M = 4.02), volunteer readiness (M = 3.96), epidemiological knowledge (M = 3.93), and safety measures knowledge (M = 3.91). The lowest scores were reported for telemedicine (M = 2.95), practical skills (M = 3.27), and simulation-based training (M = 3.32), indicating lower confidence in applied competencies.
Exploratory factor analysis of the 20 preparedness items identified a two-factor structure explaining 66.9% of the total variance (KMO = .965; Bartlett’s χ2(190) = 5827.1, p < .001). Factor 1, representing theoretical, preventive, communicative, and clinical knowledge, demonstrated high internal consistency (Cronbach’s α = .96) and had a mean score of 3.76 ± 1.01 (95% CI [3.64, 3.87]). Factor 2, representing clinical and practical pandemic response preparedness, also demonstrated high internal consistency (Cronbach’s α = .93) with a mean score of 3.42 ± 1.08 (95% CI [3.30, 3.54]) (Figure 1). Conceptual hierarchy of pandemic preparedness factors, domains, and subdomains.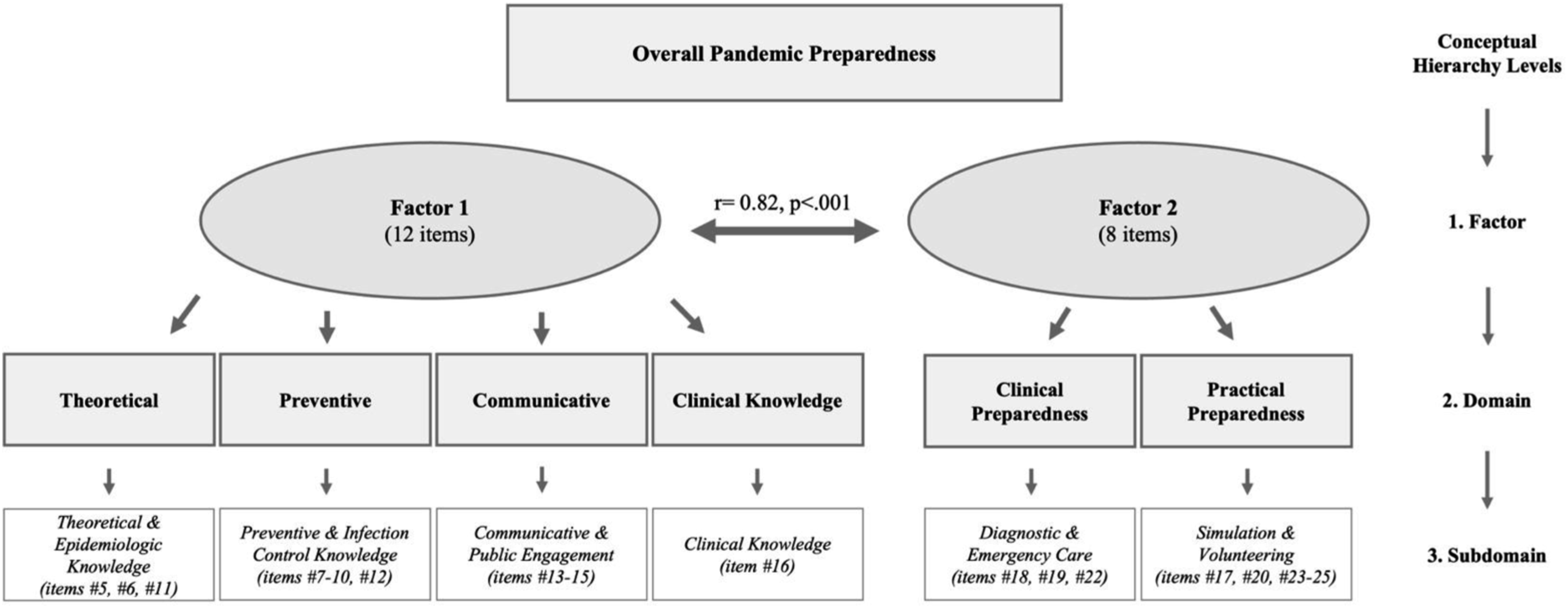
Correlation analysis demonstrated significant positive associations between overall preparedness and all preparedness items. The strongest correlations were observed for preparedness in practical skills (r = .739) and the weakest correlation was observed for epidemiological knowledge (r = .535), although this association remained statistically significant after Bonferroni correction (Figure 2). Pearson’s correlation of 20 survey items with overall pandemic preparedness (n = 296).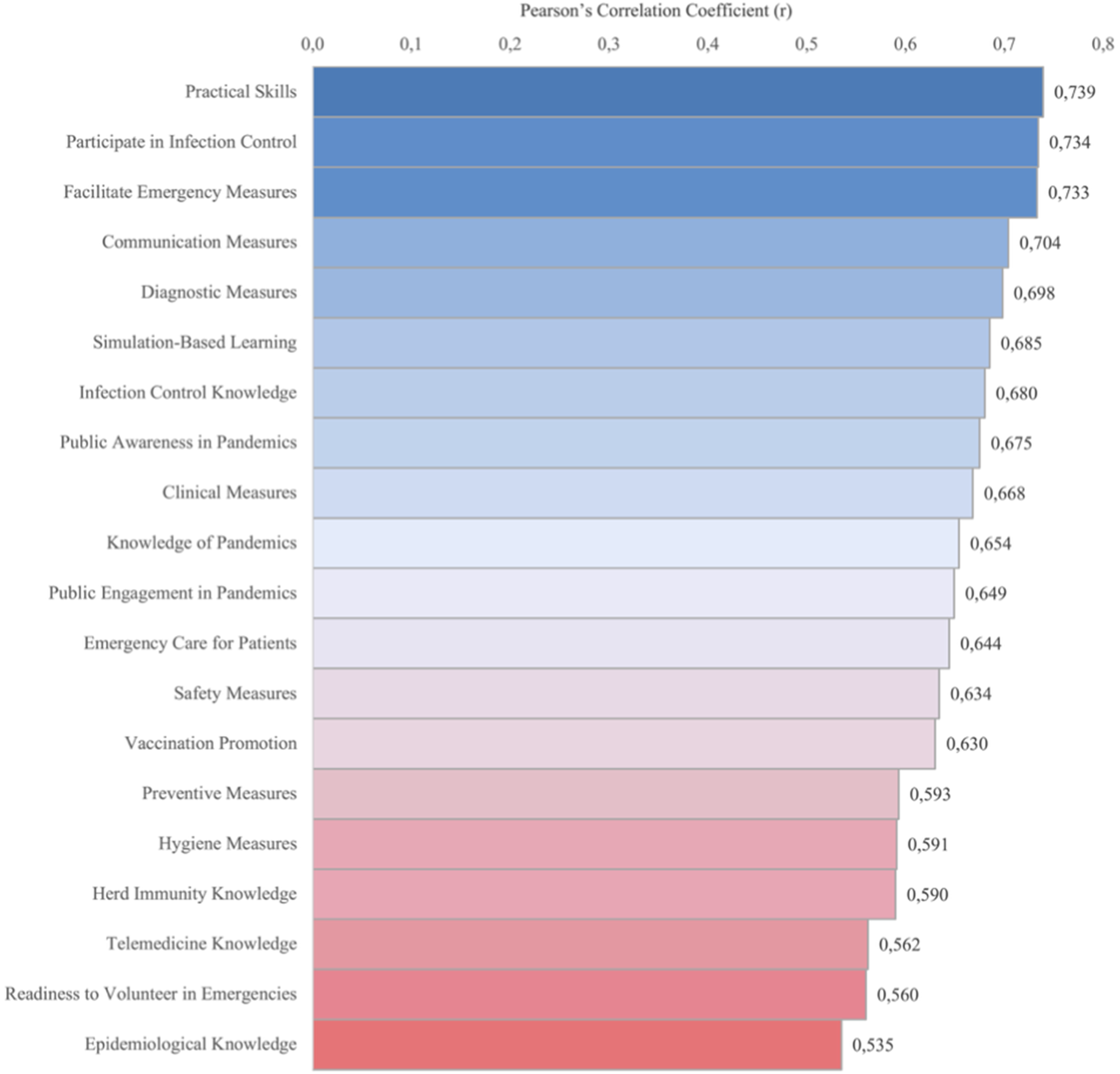
Multiple linear regression indicated that both preparedness factors independently predicted overall preparedness. Clinical and practical preparedness exerted the stronger effect (B = .739, β = .634) compared with theoretical and preventive knowledge (B = .246, β = .213), explaining 67.7% of variance (R2= .677).
No statistically significant differences in preparedness were observed by gender or age. Differences by academic program were identified, with public health students reporting higher preparedness (M = 3.80) than medical students (M = 3.36; p = .009). Participation in COVID-19 response activities was reported by 26.7% of students and was associated with higher preparedness across both domains (Factor 1: d = .38; Factor 2: d = .53). Extracurricular pandemic-related training was reported by 20.6% of students and was more common among older respondents. Higher clinical and practical preparedness was associated with greater odds of participation in extracurricular training (OR = 5.86).
Students generally supported the role of undergraduate education in pandemic preparedness (M = 4.04, SD = 1.09), and 81.1% supported explicit inclusion of pandemic-related topics (M = 4.32, SD = 0.95). Clinical and medical training was the most frequently prioritized area for reform (43.6%), followed by preventive measures (25.0%), theoretical knowledge (16.6%), and communication measures (14.9%).
Alumni
A total of 203 alumni responses were analyzed. Most respondents were aged 27–31 years (49.3%), followed by 22–26 years (39.9%) and ≥32 years (10.8%). The sample was predominantly female (65.0%), and most graduates were from medicine (71.4%) or public health (22.7%), with smaller representation from dentistry (3.9%) and pharmacy (2.0%). Slightly more respondents graduated from private universities (55.2%) than public universities (44.8%).
Overall perceived pandemic preparedness was low to moderate (M = 2.95, SD = 1.15, 95% CI [2.79, 3.11]).
Preparedness differed significantly across graduation cohorts, F(4, 198) = 5.15, p < .001 (η2= 0.094; ω2= 0.076). Preparedness was highest among 2023–2024 graduates (M = 3.54, SD = 0.91, 95% CI [3.24, 3.83]) and lowest among 2021–2022 graduates (M = 2.41, SD = 1.12, 95% CI [2.05, 2.77]). Games Howell tests showed significantly lower preparedness among 2021–2022 graduates compared with 2023–2024 graduates (mean difference = −1.12821, p < .001) and among 2015–2020 graduates compared to 2023–2024 (mean difference = −0.65846, p = .016).
Preparedness also differed across educational programs, F(3, 199) = 5.39, p = .001 (η2= 0.075; ω2= 0.061). Mean preparedness was highest among medicine (M = 3.03, SD = 1.15, 95% CI [2.84, 3.22]) and public health graduates (M = 3.00, SD = 0.99, 95% CI [2.71, 3.29]), followed by dentistry (M = 2.25, SD = 1.28, 95% CI [1.18, 3.32]) and pharmacy (M = 1.00, SD = 0.00). Pharmacy graduates reported significantly lower preparedness than medicine and public health graduates (both p < .001), although the small pharmacy sample (n = 4) warrants cautious interpretation. Preparedness did not differ between male and female respondents or across age groups (all p > .05). Given this highly limited sample size, the pharmacy finding should be treated as indicative rather than conclusive, and cross-disciplinary comparisons involving this group should not be generalized beyond the present sample.
Pandemic-related experience was associated with higher preparedness. Alumni who participated in COVID-19 response activities (n = 77) reported higher preparedness (M = 3.23, SD = 1.17) than non-participants (n = 126; M = 2.78, SD = 1.11), t(201) = −2.79, p = .006, Cohen’s d = 0.40. Preparedness was also higher among those who received extracurricular pandemic-related training (M = 3.47 vs M = 2.78), t(201) = −3.85, p < .001. Alumni willing to participate in future pandemics reported higher preparedness (M = 3.03 vs M = 2.43), t(201) = −2.62, p = .009. Among COVID-19 participants, preparedness did not differ by emotional or professional support variables (all p > .05).
Preparedness items by factor and domain means, SDs, and 95% CIs (M = Mean, SD = Standard Deviation, CI = Confidence Interval. Statistical significance set at α = .05 (two-tailed).

Preparedness correlated strongly with pandemic-related knowledge (r = .698), theoretical knowledge (r = .681), informational and communication measures (r = .660), practical skills preparedness (r = .682), confidence in applying practical skills (r = .661), and use of expertise for public welfare (r = .653), with moderate correlations for clinical application measures (r = .503 to .583), all p < .001. Multiple linear regression showed strong model fit, F(14, 188) = 27.43, p < .001, explaining 67.1% of variance (R2= .671). Pandemic-related knowledge (β = .294, p < .001), preparedness in practical skills (β = .182, p = .022), and use of expertise for public welfare (β = .184, p = .010) independently predicted preparedness.
Most alumni supported curricular reform. Undergraduate curricula improvement was reported by 88.6%, and 86.7% supported inclusion of pandemic-related topics. Priority areas included clinical and medical measures (38.9%), preventive measures (20.7%), informational and communication measures (18.7%), and strengthened theoretical instruction (17.7%).
Qualitative results
Participant characteristics and analytic overview
Qualitative data were obtained from two complementary participant groups. The first group comprised 21 public health experts, including 14 female and 7 male participants, based in Georgia (n = 11) and internationally in the United Kingdom (n = 3), the United States (n = 2), Germany (n = 2), Australia (n = 1), Denmark (n = 1), and Armenia (n = 1). The second group consisted of 30 Georgian participants, including 25 educators and 5 curricular committee members, representing biomedical sciences, clinical disciplines, public health, dentistry, nursing, and pharmacy. Responses from three international curricular experts based in Germany, Belgium, and Armenia were excluded from thematic analysis and used only for triangulation.
Across both datasets, inductive thematic analysis identified convergent priorities for strengthening pandemic preparedness in undergraduate biomedical and health sciences education. Supplementary analytic techniques, including word frequency analysis and code co-occurrence mapping, were used to support pattern identification and thematic refinement.
Educators and curricular committee members
Qualitative analysis of responses from Georgian educators and curricular committee members identified three core themes related to strengthening pandemic preparedness within undergraduate biomedical and health sciences education: strengthening institutional readiness, enhancing public health communication, and building research and collaborative capacity (Figure 3). Thematic coding analysis of Georgian educators and curricular committee members identifying qualitative indicators for pandemic preparedness.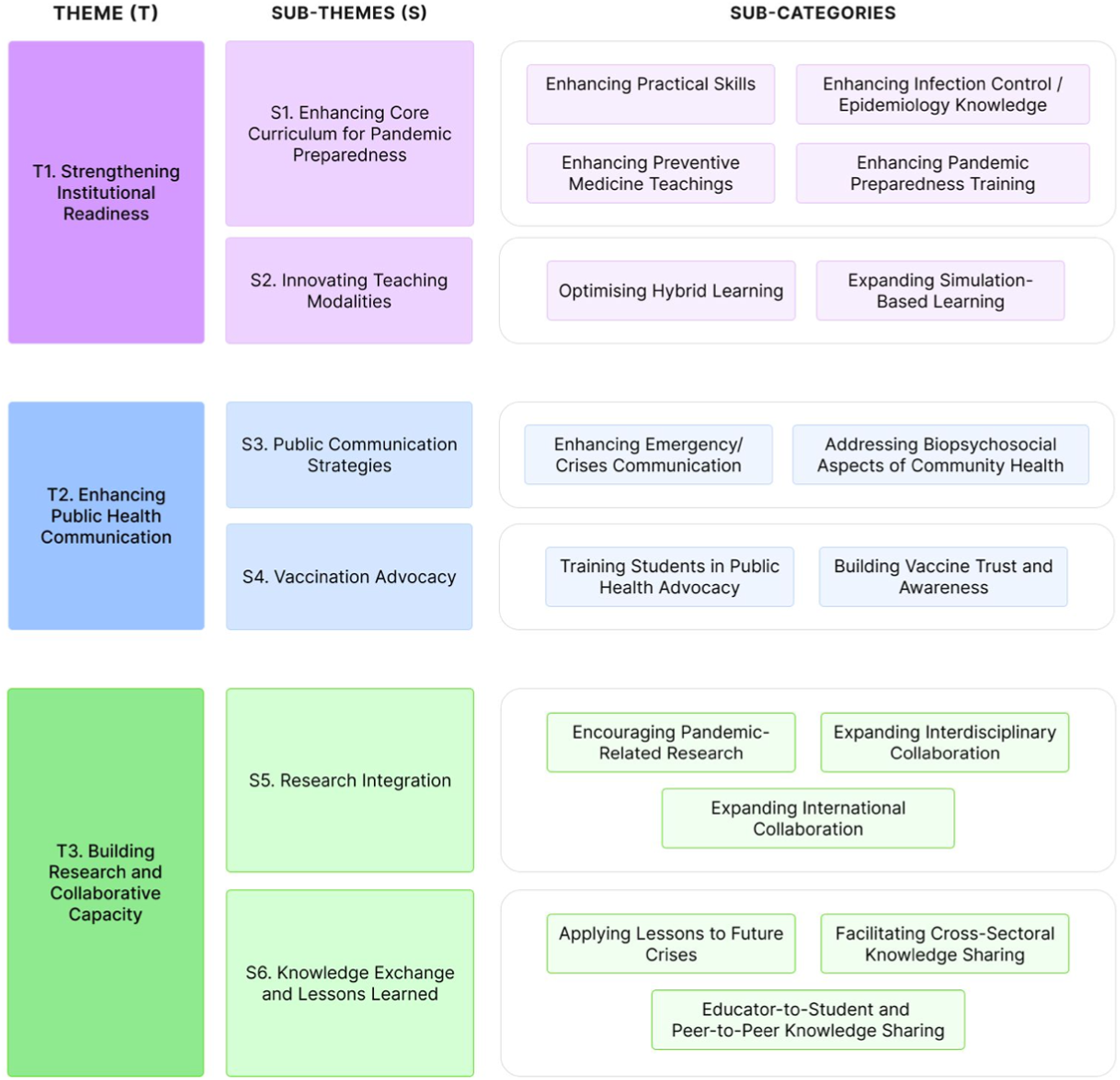
The first theme, strengthening institutional readiness, reflected the need to equip students and faculty with essential crisis management competencies. Over half of participants (55%, n = 16) indicated the integration of pandemic preparedness training within undergraduate curricula. Nearly half (48%, n = 14) identified infection control and epidemiology as essential curricular components. In addition, 31% of participants (n = 9) prioritized strengthening practical skills and preventive medicine teaching, indicating that existing curricula were perceived as overly theoretical. Simulation-based and hybrid learning approaches were highlighted by 38% of participants (n = 11), with emphasis on emergency simulations and pandemic scenarios to support decision-making and response skills.
The second theme, enhancing public health communication, focused on preparing students to engage effectively with the public during health crises. Vaccine advocacy was identified as a key competency by 45% of participants (n = 13), with most of these responses (92%, n = 12) emphasizing the importance of training students in public health advocacy to build vaccine confidence and address misinformation. A smaller number of participants also highlighted the importance of addressing biopsychosocial aspects of pandemics, including community well-being and emotional resilience.
The third theme, building research and collaborative capacity, underscored the importance of integrating research and interdisciplinary collaboration within undergraduate education. Nearly half of participants (48%, n = 14) advocated for the inclusion of pandemic-related research within curricula. Knowledge exchange was highlighted by 66% of participants (n = 19), with 47% (n = 9) specifically prioritizing cross-sectoral collaboration across public health, clinical, research, and technical disciplines. A smaller proportion (7%, n = 2) noted the importance of expanding international engagement to support both local and global preparedness.
Public health experts
Qualitative analysis of interviews with public health experts identified four major themes related to strengthening pandemic preparedness and response in undergraduate biomedical and health sciences education: foundations and core competencies for preparedness, embedding preparedness within undergraduate education, building institutional and expert capacity for preparedness, and preparedness as a shared societal and public health responsibility (Figure 4). Thematic coding analysis of public health experts identifying qualitative indicators for pandemic preparedness.
The first theme recognized foundational competencies required for pandemic preparedness. Approximately 90% of participants highlighted epidemiology, surveillance, and outbreak management as essential undergraduate competencies. Experiential and hands-on learning was underscored by approximately 75% of participants, reflecting the importance of early exposure to real-world public health practice. Simulation, emergency, and crisis training was endorsed by approximately 80% of participants, with emphasis on structured simulations to develop decision-making, teamwork, and adaptive responses in high-pressure contexts.
The second theme focused on embedding preparedness within undergraduate education. Approximately 80% of participants stressed the need for systematic curricular integration of pandemic preparedness across courses and learning outcomes. Ethics, policy, and governance education was highlighted by approximately 75% of participants as an essential component of preparedness, reflecting the need to prepare students to navigate ethical dilemmas, policy frameworks, and governance structures during public health emergencies.
The third theme addressed building institutional and expert capacity for preparedness. Approximately 80% of participants reinforced the importance of faculty development, specialized expertise, and institutional readiness to support consistent implementation of preparedness-oriented education.
The fourth theme conceptualized preparedness as a shared societal and public health responsibility. Public health communication and misinformation management were emphasized by approximately 85–90% of participants. Student engagement in pandemic response activities was endorsed by approximately 80% of participants, while community engagement and social responsibility were noted by approximately 70% of participants, highlighting the role of academic institutions in supporting broader public health preparedness.
Discussion
Overview of study findings
This mixed-methods study provides an integrated examination of pandemic preparedness within undergraduate biomedical and health sciences education in Georgia, combining quantitative preparedness assessments from students and alumni with qualitative perspectives from educators, curricular committee members, and public health experts. Unlike prior studies focused on single participant groups or isolated educational settings, the present study synthesizes preparedness experiences across cohorts trained before, during, and after the COVID-19 pandemic while incorporating institutional and expert perspectives on curricular reform. This multi-level integration allows preparedness to be examined not only as an educational outcome but also within the broader workforce and public health systems contexts that shape it.
Across both quantitative datasets, perceived preparedness remained uneven, with theoretical, preventive, and communicative competencies rated more positively than clinical and practice-based preparedness. In the student sample, practical skills demonstrated the strongest association with overall preparedness, while pandemic-related knowledge emerged as the strongest correlate among alumni. These patterns suggest that applied and experiential competencies play a central role in shaping preparedness yet remain comparatively underdeveloped within current curricula. The strong support expressed by both students and alumni for the explicit inclusion of preparedness content further indicates that this gap is widely recognized among those most directly affected by it.
Qualitative findings from educators, curricular committee members, and public health experts contextualized these quantitative patterns, revealing that preparedness content is frequently delivered indirectly through existing courses rather than through defined frameworks or explicit learning outcomes. Experts consistently emphasized the need for stronger experiential learning, simulation-based training, interdisciplinary collaboration, faculty development, and public health communication competencies. Together, the quantitative and qualitative findings converge on three interconnected gaps in Georgian biomedical and health sciences education: fragmented preparedness curricula, insufficient experiential training, and uneven preparedness education across disciplines. These gaps form the basis for the recommendations that follow.
Pandemic preparedness in undergraduate health professions education
International evidence indicates that undergraduate health professions education often provides limited preparation for large-scale health emergencies. Studies conducted during and after the COVID-19 pandemic show that healthcare students frequently demonstrate strong willingness to contribute during crises despite limited formal preparedness training, reflecting a persistent willingness-preparedness gap.18–21 Similar findings have been reported across multiple educational settings.22,23 The present study extends this literature by demonstrating that the willingness-preparedness gap may persist even among students and alumni who participated directly in COVID-19 response activities, suggesting that crisis participation alone is insufficient to produce sustained preparedness competencies without structured and supervised experiential learning. These findings reinforce the argument that pandemic preparedness should be embedded longitudinally within undergraduate curricula rather than delivered through ad hoc emergency training.24,25 Preparedness competencies such as infection prevention, outbreak management, and crisis communication should be integrated alongside core clinical education. Evidence from disaster and emergency medicine education further demonstrates that structured preparedness curricula can improve student confidence, triage ability, and exposure risk assessment.7,26 The present findings extend this evidence by showing that curricular fragmentation is recognized not only by students and graduates but also by educators and curricular committee members, supporting the interpretation that preparedness gaps are systemic rather than isolated individual perceptions.
Expanding experiential learning and practical preparedness
Experiential learning is widely recognized as a key mechanism for developing preparedness competencies. Simulation-based learning, case-based training, and supervised service learning strengthen decision-making, communication, and teamwork skills necessary for emergency response.27–29 Consistent with this literature, the present study identified practical skills as the strongest predictor of preparedness, while participation in COVID-19 response activities and extracurricular preparedness training was associated with higher preparedness levels among students and alumni. However, experiential engagement during COVID-19 often occurred informally rather than through structured educational programs, limiting opportunities for supervised competency development. These findings highlight the importance of institutionalizing experiential preparedness training within undergraduate education.
Interdisciplinary preparedness education
Preparedness levels varied across educational programs, with medicine and public health graduates reporting higher preparedness than pharmacy and dentistry graduates. These differences indicate uneven distribution of preparedness training across disciplines. Pandemic response requires coordinated collaboration across clinical and public health professions, and international literature increasingly emphasizes interdisciplinary approaches to preparedness education involving physicians, nurses, pharmacists, and public health professionals. 30 The present findings support these recommendations by demonstrating variability in preparedness across disciplines within the Georgian educational context, suggesting that preparedness competencies may currently depend on program-specific curricular exposure rather than standardized interdisciplinary frameworks.
Educational recommendations for Georgian higher educational institutions
The mixed-methods findings highlight three priorities for strengthening preparedness education in Georgia: integrating preparedness competencies within curricula, expanding experiential learning, and promoting interdisciplinary training. Together with insights from international literature, these findings suggest several practical opportunities for reform within Georgian higher education institutions.
Curricular integration of pandemic preparedness competencies
Pandemic preparedness and response competencies should be explicitly integrated into undergraduate biomedical and health sciences curricula. Core competencies may include epidemiological surveillance, infection prevention and control, outbreak investigation, public health communication, vaccination strategies, and ethical decision-making during health emergencies. Defining clear preparedness learning outcomes across programs would address the curricular fragmentation identified in qualitative findings and respond to strong student support for preparedness education.
Dedicated and interdisciplinary preparedness courses
Georgian universities could introduce dedicated courses focused on pandemic preparedness and health emergency response. Several universities internationally have implemented similar models. For example, the University of Melbourne offers a course covering surveillance systems, outbreak risk assessment, health system resilience, and community engagement. 31 The NextGenU and Yale pandemic preparedness program similarly provides modules on outbreak detection, modeling, vaccine development, and risk communication. 32 The interdisciplinary Pandemic Preparedness Summer School at the University of Antwerp demonstrates how preparedness education can also be delivered through intensive programs combining lectures, case studies, and collaborative exercises. 33
In Georgia, similar initiatives could be implemented as interdisciplinary electives within existing curricula or as intensive formats such as summer schools, certificate programs, or extracurricular courses awarding ECTS credits. Faculties of biomedical and health sciences could jointly design such programs, allowing students from medicine, nursing, pharmacy, dentistry, and public health to participate together through case-based and simulation-based scenarios.
Experiential and simulation-based training
Experiential and simulation-based learning opportunities should also be expanded. The strong relationship between practical competencies and preparedness observed in this study highlights the importance of applied training environments. Simulation exercises may include outbreak investigation scenarios, infection control drills, and emergency triage exercises. Disaster preparedness programs implemented in other universities demonstrate that structured simulation training significantly improves preparedness and student confidence. 7 Incorporating such approaches into undergraduate education would allow students to practice decision-making, teamwork, and crisis management in realistic environments.
Faculty development and institutional capacity
Finally, faculty development and institutional capacity building should accompany curricular reform. Educators interviewed in this study emphasized that many instructors lack formal training in disaster medicine or emergency preparedness. Faculty development initiatives could support instructors in integrating preparedness competencies into teaching and implementing interdisciplinary and experiential learning approaches. Evidence suggests that preparedness depends not only on individual competencies but also on institutional leadership and organizational readiness. 34
Significance for public health
This study highlights the critical role of undergraduate biomedical and health sciences education in strengthening health workforce readiness for future public health emergencies. The COVID-19 pandemic demonstrated that students and recent graduates often become essential components of national response efforts, supporting surveillance, contact tracing, clinical services, and public communication. Ensuring that these future professionals are adequately prepared therefore has important implications for national and global public health policy.
The present findings provide context-specific evidence that may help inform curriculum development, workforce preparedness strategies, and future public health planning in Georgia and comparable settings. Integrating pandemic preparedness and response competencies into undergraduate biomedical and health sciences education is essential for strengthening workforce capacity, improving coordinated response across disciplines, and enhancing health system resilience. For upper-middle-income countries such as Georgia, where longstanding workforce challenges heighten the urgency of preparedness reform, embedding these competencies within undergraduate education represents both an educational necessity and a critical public health priority. Systematic integration of pandemic preparedness into undergraduate education is therefore essential for strengthening workforce resilience, as education functions as a form of primary prevention within public health systems.
Conclusion
This mixed-methods study provides a post-COVID examination of pandemic preparedness within undergraduate biomedical and health sciences education in Georgia, integrating perspectives from students, alumni, educators, curricular committee members, and public health experts. By linking preparedness outcomes to educational experiences across cohorts trained before, during, and after the pandemic, the study demonstrates that although willingness to contribute during crises is high, preparedness remains uneven and is more strongly associated with experiential and practice-based competencies than with theoretical instruction alone. These findings move beyond descriptive accounts of pandemic-era education to identify discipline-specific, cohort-based, and institutional gaps to inform evidence-based curricular reform.
Undergraduate education has an important role to play as a core component of public health preparedness, functioning as a proactive mechanism for workforce development and health system strengthening. Embedding competency-based training in areas such as epidemiology, infection control, crisis communication, ethics, and simulation-based learning can enhance workforce readiness while fostering interdisciplinary collaboration and health promotion. For Georgia, such reforms may help address structural workforce vulnerabilities and reduce reliance on reactive emergency responses. More broadly, the findings offer relevant insights for upper-middle-income and transitioning health systems seeking to strengthen pandemic preparedness through undergraduate health professions education.
Limitations
Several limitations should be considered when interpreting the findings of this study. First, the cross-sectional design precludes causal inference, and differences in training conditions across graduation cohorts may affect comparability over time. Second, preparedness was assessed using self-reported measures, which reflect perceived rather than objectively demonstrated competency and may be subject to social desirability and recall bias. Future research should incorporate objective or performance-based assessments, such as standardized simulation exercises or objective structured clinical examinations, to provide more externally valid measures of pandemic preparedness. Third, although both instruments were adapted from previously validated tools, they were not formally pilot tested prior to administration. Fourth, uneven disciplinary representation, particularly among pharmacy and nursing respondents, limits the generalizability of discipline-specific findings and warrants caution in cross-program comparisons. Finally, recruitment through institutional and professional networks may have introduced selection bias.
Nevertheless, the study has several important strengths, including its mixed-methods design, novel integration of perspectives from multiple stakeholder groups, inclusion of cohorts graduating before, during, and after the COVID-19 pandemic, and synthesis of quantitative and qualitative findings within a unified analytical framework. Together, these features provide a comprehensive and context-specific examination of pandemic preparedness within undergraduate biomedical and health sciences education in Georgia and may help inform evidence-based curricular reform, health workforce preparedness, and broader public health resilience in comparable settings.
Supplemental material
Supplemental material - Strengthening pandemic preparedness and response through undergraduate education in biomedical and health sciences: A mixed-methods study from Georgia
Supplemental material for Strengthening pandemic preparedness and response through undergraduate education in biomedical and health sciences: A mixed-methods study from Georgia by Dea Goderdzishvili, and Elza Nikoleishvili in Journal of Public Health Research.
Supplemental material
Supplemental material - Strengthening pandemic preparedness and response through undergraduate education in biomedical and health sciences: A mixed-methods study from Georgia
Supplemental material for Strengthening pandemic preparedness and response through undergraduate education in biomedical and health sciences: A mixed-methods study from Georgia by Dea Goderdzishvili, and Elza Nikoleishvili in Journal of Public Health Research.
Footnotes
Acknowledgements
The authors would like to thank all participants who contributed their time and perspectives to this study, as well as the colleagues who provided support throughout the development and completion of the research. A special thank you is extended to Dr. Giorgi Aladashvili for his contributions and continued support. This mixed-methods study was conducted as part of doctoral research in Public Health. Artificial Intelligence (AI) tools were used solely for grammatical and stylistic refinements. All research design, data collection, analysis, and interpretation were conducted entirely by the authors. Elements of this research are derived from four related studies conducted as part of the author’s doctoral research. One qualitative study reporting findings from Georgian educators and curricular committee members has been previously published. One quantitative study reporting findings from final-year students is currently under consideration elsewhere. The findings from the alumni survey and public health expert interviews have not been previously published or submitted for consideration. The present mixed-methods manuscript represents a novel integrated analysis incorporating all four datasets within a unified interpretive framework. It extends beyond the individual study components by synthesizing quantitative and qualitative findings to generate broader, context-specific conclusions regarding pandemic preparedness in undergraduate biomedical and health sciences education in Georgia. This manuscript has not been submitted to, reviewed by, or published in any other journal.
Ethical considerations
Ethical approval was obtained from the Biomedical Research Ethics Board of the University of Georgia, School of Health Sciences (Approval No. N:11-6461). Participation was voluntary and informed consent was obtained from all participants prior to inclusion.
Consent to participate
Participation was voluntary, and informed consent was indicated by participants through written and verbal confirmation when taking part in the surveys and interviews.
Author contributions
D.G. conceptualized and conducted the study, developed the mixed-methods design and research instruments, performed data collection and analysis, and drafted the manuscript. E.N., PhD supervisor of D.G., contributed to study design refinement, supervised the research process, oversaw ethical approval procedures, coordinated and supported questionnaire distributions, and contributed to the interpretation of findings and the discussion section.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset cannot be publicly shared due to potential participant identification; de-identified data are available upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.