
Abstract
Abstract
Drug-resistant tuberculosis remains a major global public health challenge due to its complex treatment regimens and prolonged treatment duration. Drug-resistant tuberculosis treatment requires more expensive second-line medications, intensive monitoring, and longer hospitalization, resulting in substantially higher healthcare costs. Vietnam is one of 30 countries with a high burden of tuberculosis and drug-resistant tuberculosis.
Objective
This study aims to investigate direct medical costs and associated factors of the costs in drug-resistant tuberculosis inpatients.
Methods
A retrospective study was conducted at the National Lung Hospital. Medical and financial data of 629 inpatients with drug-resistant tuberculosis inpatients who discharged from the hospital from January 1st to December 31st, 2024, were collected.
Results
The median of total inpatient treatment cost for a hospital stay was $707.2, and costs of drugs and intravenous fluids accounted for the highest proportion (38%) of total costs. Length of stays, number of comorbidities, and age were independent predictors of increased the direct medical costs of drug-resistant tuberculosis inpatients.
Conclusions
Treatment costs for DR-TB in Vietnam remain high, highlighting the need for targeted financial support for vulnerable patients.
Introduction
DR-TB (DR-TB) is a type of Tuberculosis (TB) that occurs when Mycobacterium tuberculosis is resistant to one or more anti-tuberculosis drugs used in the standard treatment therapy. 1 The causes of DR-TB can come from many different factors, including treatment-related problems and biological factors.1,2 Previous studies have identified the causes of DR-TB such as prescriptions of doctors, the quality and quantity of drugs, lack of understanding between doctors and tuberculosis patients, and factors related to nutrition.3–5 According to WHO (2022), an estimated 410,000 new cases of multidrug-resistant (MDR-TB) or rifampicin-resistant tuberculosis (RR-TB) occurred globally. One of the biggest challenges is the gap between the estimated number of these cases and the actual number of cases diagnosed and treated.6,7 In 2022, only about 175,650 of the estimated 410,000 cases were diagnosed and treated, representing a detection and treatment rate of about 43%. This gap is primarily concentrated in 10 countries, accounting for approximately 70% of undetected cases, including high-burden countries such as India, China, and Indonesia. 8 Mortality from DR-TB remains high, with more than 1.3 million TB-related deaths in 2022, a significant proportion of which are due to DR-TB cases. Treatment of DR-TB has lower success rates than that of drug-susceptible TB cases, especially in the case of extensively DR-TB (XDR-TB). 1
Vietnam is one of 30 countries with a high burden of Tuberculosis (TB) and DR-TB. According to WHO reports, TB incidence accounts for the majority of new cases in Southeast Asia. 2 The epidemiological situation of DR-TB globally and in Vietnam remains challenging, especially during the COVID-19 pandemic, which has caused significant disruptions to TB detection and treatment.9,10 .Currently, patient support programs in Vietnam such as rapid detection testing and treatment support have been promoted. 11 However, to achieve the WHO’s goals in the “End TB” strategy, Vietnam needs to improve further the quality of diagnosis and treatment, as well as reduce economic barriers to accessing health services.2,12,13 Although most patients have health insurance from the Vietnamese government, the cost of treating DR-TB in Vietnam is not fully covered by health insurance. Nguyen Viet Nhung et al. found that 63% of households affected by tuberculosis or MDR-TB faced costs exceeding 20% of their annual income. The most significant costs were related to lost income, the purchase of nutritional supplements, transportation, and accommodation. 14 In Vietnam, limited evidence is available on direct medical costs of DR-TB patients and associated factors.11,12,14,15
To address this gap, we conducted this study to investigate the direct medical costs of DR-TB and associated factors with these costs at National Lung Hospital, the highest-level specialized hospital for lung diseases in Vietnam.
Material and methods
Study design
This is a retrospective study using secondary medical and financial data extracted from National Lung Hospital from January 2024 to December 2024.
Study setting
National Lung Hospital is a national hospital located in Hanoi City, Capital of Vietnam. It is a primary referral hospital of northern Vietnam, as well as a center for research and postgraduate training in lung diseases. Patients were admitted to National Lung Hospital in cases such as patients from non-specialized healthcare facilities were referred to the hospital after being diagnosed with tuberculosis. Patients from lower level health facilities was tranfered to the National Lung hospital due to treatment failure. Patients were admitted as an emergency case due to severe clinical conditions such as hemoptysis, pleural effusion or other serious complications.
TB treatment in Vietnam is implemented under the National Tuberculosis Control Program, coordinated by the Ministry of Health. Vietnam has adopted the World Health Organization (WHO) recommendations for the diagnosis and management of drug-susceptible and DR-TB. TB diagnosis is supported through a nationwide network of healthcare facilities, with the use of rapid molecular diagnostic techniques such as Xpert MTB/RIF, culture, and drug susceptibility testing. Patients diagnosed with TB are managed according to standardized treatment regimens and follow-up protocols.
Vietnam’s TB control policy is the extensive financial support. First-line anti-TB drugs for drug-susceptible TB are generally provided free of charge through the National Tuberculosis Program. In recent years, many second-line medications for MDR-TB, including newer drugs such as bedaquiline and linezolid, have also been subsidized through international donor support and government programs. 16
Study population
The inpatient was diagnosed with DR-TB (DR-TB) according to the guidelines of the Vietnam Ministry of Health. Since AFB smear microscopy cannot detect drug resistance, resistance status was determined separately using molecular and/or phenotypic drug susceptibility testing methods. Rifampicin resistance was primarily identified using the GeneXpert MTB/RIF assay, while additional resistance patterns were confirmed by culture-based drug susceptibility testing (DST) when available.
Inclusion criteria
Patients diagnosed with DR-TB (DR-TB), according to the Ministry of Health guidelines, were included in the study. DR-TB included Drug-resistant TB; Rifampicin-resistant TB; Poly-resistant TB; Multi-drug-resistant TB; Pre-extensively drug-resistant TB; Extensively drug-resistant TB ( Supplemental file) Patients discharged to the hospital between January 1, 2024, and December 31, 2024. Medical records and financial data were required to have compete information regarding treatment processes, laboratory results, and healthcare costs.
Exclusion criteria
Records lacking essential information for cost assessment were excluded. Patients with severe comorbidities unrelated to pulmonary tuberculosis (such as end-stage cancer or chronic renal failure) were also excluded. Medical records in which drug-resistance status could not be clearly identified were excluded from the study.
Sample size and sampling method
The minimum sample size was calculated using the formula for estimating a population mean: n: minimum required sample size. α: Type I error probability. With α = 0.05, σ = 1897.03
The sample size parameters were derived from the study by Akalu et al., which reported a mean direct cost of $ 1936.25 with SD of $1897.03 among inpatients with MDR-TB. 17
d = 193.625 (10% of the expected mean)
Substituting these values into the formula yielded a minimum required sample size of 370 participants.
During the study period, 629 inpatients with DR-TB discharged from the National Lung Hospital met the study eligibility criteria. Therefore, all 629 eligible patients were included in the study, resulting in a sample size that exceeded the minimum required number.
Data collection
Data were extracted from the medical records and financial data of patients with DR-TB inpatients who was discharged from the National Lung Hospital between January 1, 2024, and December 31, 2024. Social-demographic and clinical characteristic of DT-TB inpatients was extracted from the medical record. Cost data was exacted from the financial data after the inpatient was discharged from the hospital. Direct medical costs were defined cost invoiced by the hospital after the DT-TB inpatients was discharged from the hospital. These costs included the total direct medical costs as well as costs per service category such cost of bed-day cost, cost of laboratory, cost of diagnostic imaging, cost of functional tests, cost of surgery, cost of drugs and intravenous fluids, cost of medical supplies, cost of other services.
Variables
Outcome variables
The primary outcome variable was the total direct medical cost of DR-TB inpatients which were defined as the total amount invoiced by a hospital after the inpatient was discharged from the hospital. All cost data were extracted from the hospital records and converted to USD using an exchange rate of 1 USD=25.000 Vietnamese Dong (VND) (2024).
Covariates
Social-demographic and clinical characteristics of drug-resistant TB inpatient were extracted including gender, age, education level, occupation, health insurance, length of stay, classification of definitive diagnosis of pulmonary, classification of DR-TB.
Statistical analysis
Data were transferred to SPSS 20.0 for analysis. Firstly, descriptive statistics (percentage, mean, IQR, min, max) for all characteristic of inpatients were calculated and detailed statistics on total direct medical cost as well as costs per service category were generated. Following this, cost differences among DR-TB groups were calculated. Secondly, we first estimate unadjusted associations with cost (mean cost differences) and then estimated how large the cost differences were adjusting on characteristic of drug-resistant TB inpatients. We used robust variance estimates to adjust for heteroskedasticity of residuals in the multivariable linear regression models.
Results
Social-demographic and clinical characteristics of study participants.

Type of medical direct costs of DR-TB inpatients (USD).
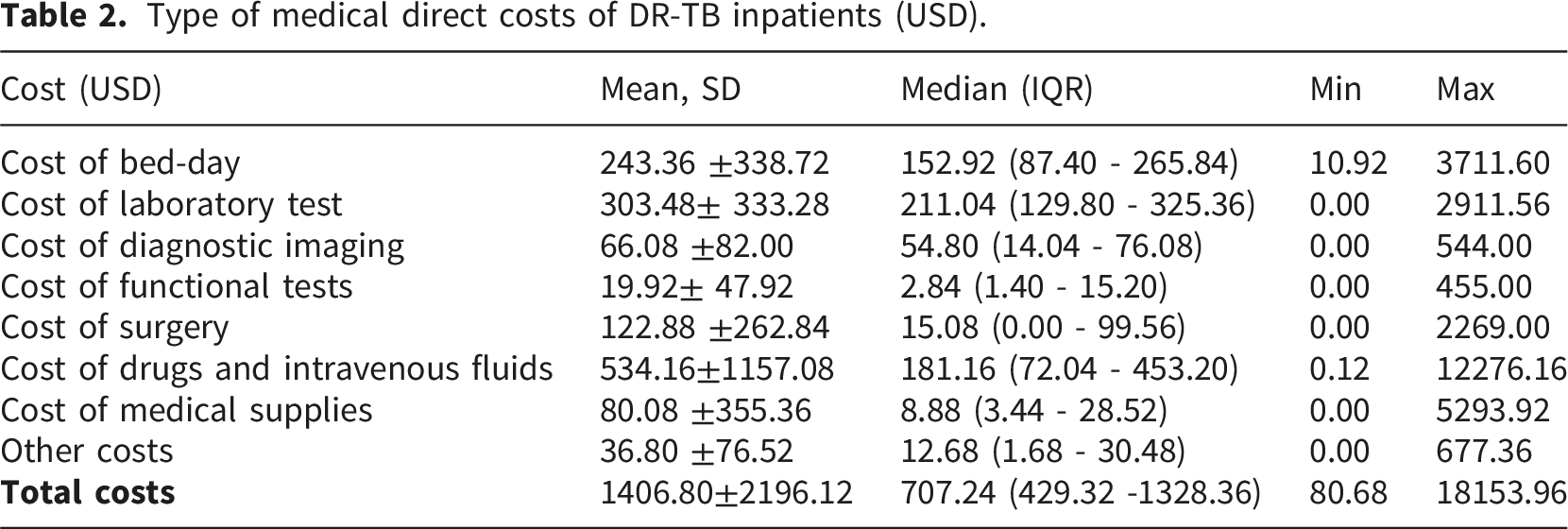
Figure 1 illustrates the cost structure of direct medical cost of DR-TB inpatients. Drug costs constituted the largest component (38%), followed by laboratoy test costs, whereas funtional test costs accounted for the smallest proportion (Figure 1). Structure of the direct medical costs of DR-TB inpatients.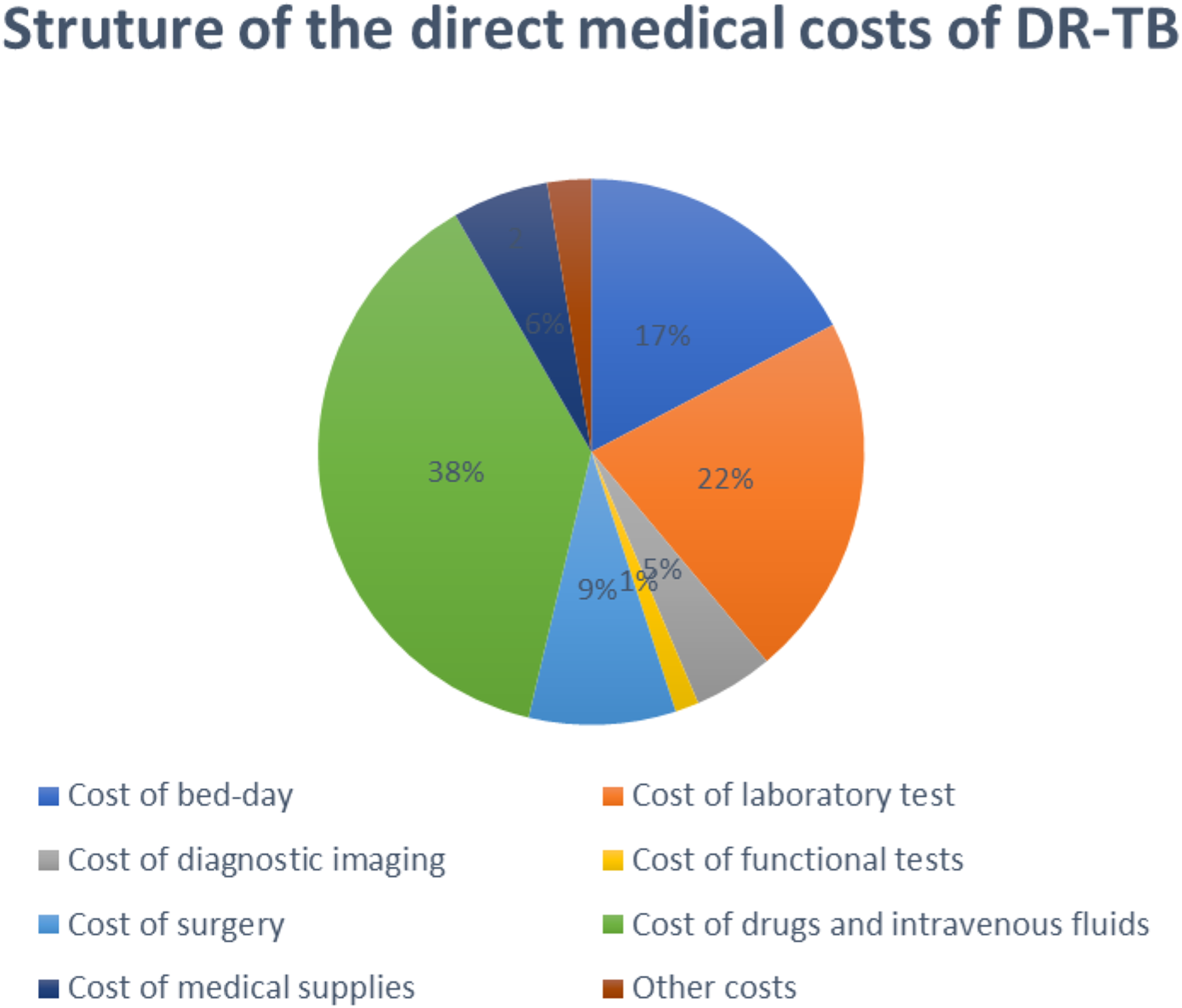
Direct medical costs among different DR-TB groups (USD).
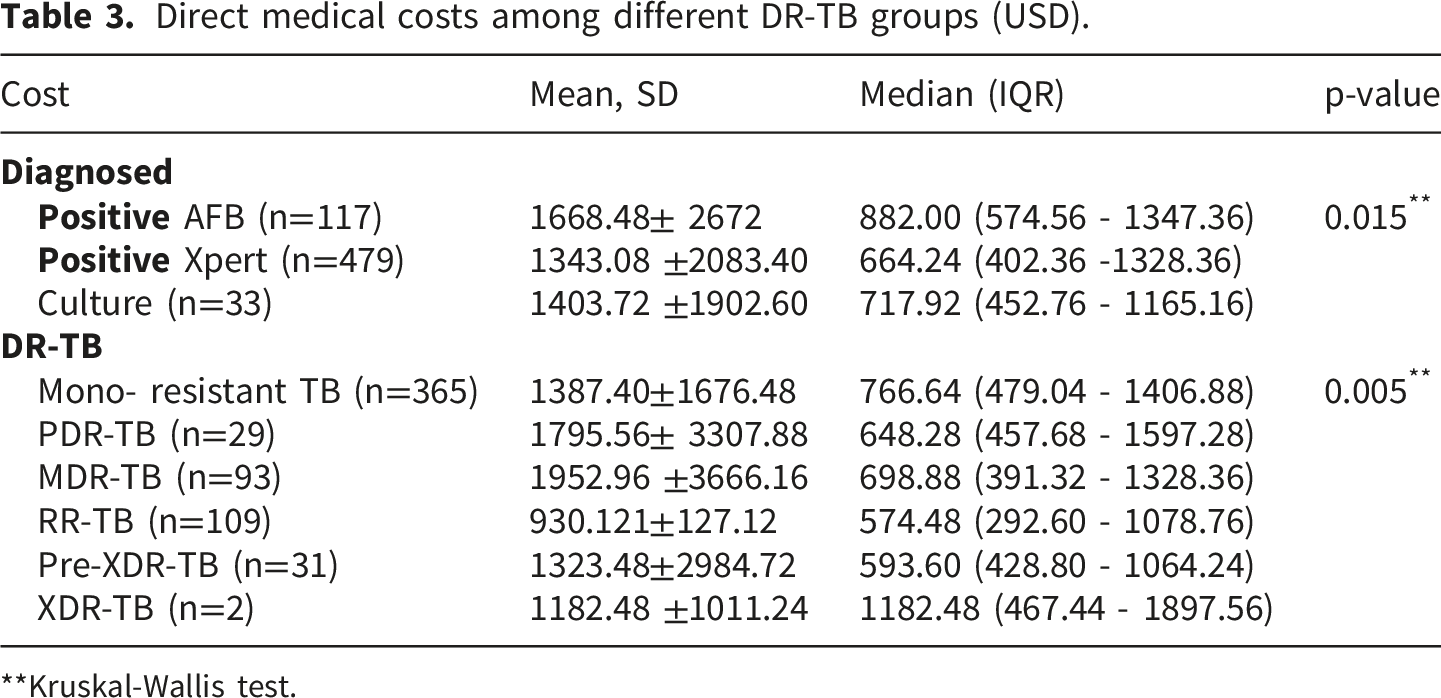
**Kruskal-Wallis test.
Factors associated with direct medical costs among DR-TB inpatients.

R 2 = 0.51, p < 0.001.
Discussion
The average of total direct medical cost of DR-TB inpatients was $ 1406.80 3 and the median was considerably lower, at approximately $80.68, suggesting a highly skewed cost distribution. Thi results was approximately 6 times higher than the medical cost for drug-susceptible tuberculosis in other study conducted in Vinh Long province. Hoang Dinh Tieng et al. (2024) reported that the average direct medical cost of inpatient treated in Vinh Long Province, where most inpatients had drug-susceptible TB, was only around 6 million VND (≈$240). 18 This difference provides further evidence that the medical cost of DR-TB is substantially higher than that of drug-susceptible TB due to more complex treatment regimens, longer treatment duration, and a higher risk of complications.
Drug costs accounted for the largest proportion of total direct medical costs (38%). This finding is consistent with the study conducted in Vinh Long Province, which reported that cost of drug represented 47.5% of the total costs of TB inpatients. 18 On the other hand, bed-day costs accounted for approximately 17% of total costs in our study, which was lower than that reported in other countries. Pooran et al. (2013) in South Africa found that bed-day costs accounted for nearly 70% of the total MDR-TB treatment costs. 8 This difference may be attributed to the fact that South Africa adopted a different strategy for MDR-TB patients, often requiring hospitalization for several months. In Vietnam, MDR-TB patients are typically hospitalized only during the initial treatment phase or when severe complications occur, after which they continue outpatient treatment. This finding shows that the model of combining short-term inpatient and outpatient treatment at the local level proven effective.
Average direct medical cost of MDR-TB inpatients in this study was highest compared to those of other DR-TB groups. Previous studies indicated that the cost of MDR-TB treatment is higher other DR-TB groups due to many associated factors such as level of resistance, complications, comorbidities, age, economic status, place of residence.3,19,20 Yet, this finding was relatively low compared to result of other study. Diel et al. (2021) in Germany reported an average cost of approximately EUR 73,552 (∼85,000 USD) per MDR-TB patient which was much more higher than the cost in Vietnam. 21 This disparity may be explained by the substantially higher prices of healthcare services and medications in high-income countries. In addition, the use of newer anti-TB drugs such as Bedaquiline and Linezolid, which are more expensive, further increases treatment costs. In contrast, in Vietnam and many low- and middle-income countries, newer anti-TB drugs are often subsidized or provided free of charge through national tuberculosis control programs, thereby reducing the direct medical costs.
Our study indicated some factors associated with increased direct medical costs of DR-TB, including over 60 years old, multiDR-TB (MDR-TB), the number of comorbidities, and length of stays (p < 0.001). Older age, comorbididities, and prolonged hospitalization have also been reported in previous studies as important associated factors with higher treatment costs 17
Length of stays had a particularly high regression coefficient (β = 3.018; p < 0.001), highlighting the substantial impact of lenghth of stays on total costs. This finding is consistent with the report by Qi et al. (2023) in China showed that inpatients with prolonged treatment duration or extended hospitalization had a significantly higher healthcare costs compared with those receiving shorter length of stays or outpatient treatment. 22 Similarly, a study conducted in Vinh Long Province demonstrated that the leghth of stays was one of the factors significantly associated with increased treatment costs (p < 0.05). 18
Comorbidities also had a strong impact on treatment costs (β ≈ 7.125; p < 0.001). Patients with DR-TB often present with underlying diseases such as diabetes,HIV infection, hepatitis, or TB-related complications including pleural effusion, respiratory failure, and multi-organ damage. These comorbidities complicate the treatment process and consequently increase healthcare expenditures. The study conducted in Vinh Long Province also found that the number of underlying diseases significantly affected treatment costs, with patients having multiple comorbidities having higher average costs (p < 0.05). 18 This finding suggests that good management of comorbidities such as diabetes and HIV will contribute to reducing treatment costs and hospital stays.
Over 60 years old and multidrug resistance (MDR-TB) were both associated with increased treatment costs (β ≈ 12.593 and 14.932, respectively; p < 0.01). Our findings are consistent with previous studies showing that MDR-TB treatment costs are typically 3–6 times higher than those with drug-susceptible TB in middle-income countries, and even 10–20 times higher in high-income countries where healthcare costs are substantially higher. 23 Many households with MDR-TB patients experience financial hardship or poverty as a result of high treatment costs and reduced income during the treatment period.15,17 Nhung et al. (2018) reported that the average cost per MDR-TB patient in Vietnam was approximately USD 4,302 per treatment episode, nearly four times higher than that of drug-susceptible TB (USD 1,054). 14 Globally, the cost of treating a single MDR-TB case ranges from approximately USD 2,000 to USD 20,000 depending on the country and healthcare setting. 22
Limitations
The study still has some limitations. The study employs a cross-sectional design, which does not reflect the costs over time or across different stages of treatment. The scope of cost calculation is limited to direct medical costs from the health facility’s perspective, excluding indirect medical and indirect non-medical costs, this may not fully reflect the actual economic burden on DR-TB patients. The study were conducted at a central specialized hospital, which may limit the generalizability of the findings. Future studies may consider extending scope of cost calculation and number of health facilities to explore these dynamics more comprehensively.
Conclusion
Overall, the direct medical costs of DR-TB inpatients in Vietnam, although lower than the average of developed countries, is still a considerable economic burden for patients. The median of total inpatient treatment cost was $707.24. Drugs and intravenous fluids costs accounted for the highest proportion (38% of total costs). Length of stays, comorbidities, and age were independent predictors of increased direct medical costs (p < 0.05). The study has provided quantitative evidence into direct medical costs of DR-TB inpatients and suggests that strengthening financial protection for patients through health insurance, optimizing the outpatient treatment model, effectively managing comorbidities may help reduce costs for patients and the health system.
Supplemental material
Supplemental material - Direct medical costs for drug-resistant tuberculosis inpatients at the national lung hospital, Vietnam: A one-year study
Supplemental material for Direct medical costs for drug-resistant tuberculosis inpatients at the national lung hospital, Vietnam: A one-year study by Do Minh Ngo, An Thi Binh Nguyen Hanh Duc Nguyen, and Hau Van Hoang in Journal of Public Health Research.
Footnotes
Acknowledgements
The authors would like to express their sincere gratitude to the leadership and staff of National Lung Hospital for their support and cooperation during the study.
Ethical considerations
The study was approved by the Ethical committee of Thang Long University with approval number 141/2024/HĐĐĐ.
Author contributions
HanhDN, AnTBN contributed to the conception and design of the study. DoNM, HanhDN, and HauVH were responsible for data collection and performed statistical.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to ethical restrictions and the inclusion of potentially identifiable participant information but are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.