
Abstract
Background
Misuse of antibiotics in diabetic foot infections (DFI) promotes multidrug-resistant (MDR) bacteria. Objectives: To describe antibiotic resistance patterns in patients with prior antibiotic exposure before tertiary hospital admission.
Methods
A descriptive cross-sectional study followed STROBE guidelines from November 2022 to May 2023. Inclusion criteria were DFI patients with ≥ 48-hour prior antibiotic exposure at lower-level facilities. Clinical characteristics, infection severity, and bacterial cultures were assessed.
Results
Among 51 patients (64.7% male, mean age 61.1 years), results showed elevated inflammatory markers (WBC: 15.1 k/uL; CRP: 109.2 mg/L) and poor glycemic control (HbA1c: 10.2%). Ulcers were large (mean: 10.1 cm^2) with 85.3% moderate-to-severe infections. Out of 51 samples, 38 (74.5%) yielded positive isolates. Among these isolates, the MDR prevalence was 84.2% (32/38). MDR infection was significantly associated with moderate-to-severe ulcers (OR: 10.8; 95% CI: 1.48–78.8; p=0.007).
Conclusion
A high prevalence of MDR bacteria was identified among referred DFI patients, indicating a significant resistance burden in this population. These findings suggest a potential link between prior antibiotic exposure and increased resistance risk, underscoring the need for robust antimicrobial stewardship within referral networks.
1. Introduction
Diabetes currently affects approximately 422 million individuals globally, accounting for 8.5% of the adult population, with prevalence rising more rapidly in low- and middle-income countries. Notably, 80% of individuals with diabetes reside in low- and middle-income countries, 1 where access to many diagnostic tools remains limited and is not anticipated to improve in the near future.
Diabetic Foot Ulcers (DFUs) are a common and serious complication of among Type 2 diabetic patients (T2DPs). These ulcers typically arise due to a combination of neuropathy, peripheral arterial disease, and foot deformities, along with poor glycemic control. Neuropathy can lead to a loss of protective sensation, making patients unaware of trauma or pressure on their feet, which can subsequently progress to ulceration. 2 The prevalence of DFUs among T2DPs is approximately 6.3% globally. Belgium has the highest prevalence at 16.6%, while the rate in Asia is 5.5%. In contrast, Australia has the lowest prevalence at 1.5%. 3 Approximately 15 to 25% of individuals with diabetes mellitus are likely to experience a diabetic foot ulcer at some point in their lives, 4 and about 50% of ulcers will lead to infection, and many infected ulcers progress to severe cases that require hospitalization for treatment. 5
Management of DFU requires a multidisciplinary approach, including wound care, glycemic control optimization, and treatment of any underlying infections. In severe cases, surgical intervention may be necessary to prevent further complications, such as amputation. Education on foot care and regular foot examinations are crucial components in preventing the occurrence of DFUs in T2DPS. 6 Regardless of the severity of the disease, it is currently recommended to obtain a deep tissue culture for guiding antimicrobial therapy in the treatment of Diabetic Foot Infection (DFI). 7 Both the Infectious Diseases Society of America (IDSA) and the International Wound Group Diabetic Foot (IWGDF) advise against using a superficial wound swab for microbial evaluation of infections. 8 In instances where cultures are not obtained, empirical antibiotic therapy should focus on the most likely pathogens, including Staphylococcus aureus and Streptococcus spp. 9 The IDSA/IWGDF also recommends selecting antibiotics based on initial empirical evidence when DFI is infected and changing antibiotics according to the culture results when there is no clinical response. 8 The previous study indicated that larger ulcer areas were linked to higher levels of infection. 10 The classification of infections ranges from mild to severe based on clinical assessments and laboratory markers. 11 Furthermore, tissue damage is assessed using the Wagner Score system, which ranges from 1 to 5; higher scores signify more severe conditions and an increased likelihood of complications such as amputation. 10
DFI frequently contributes to the emergence of MDR bacteria. MDR bacterial infections are characterized by the lack of susceptibility to at least one agent in three or more antimicrobial categories. 12 The prevalence of infections caused by MDR bacteria is on the rise, presenting a significant public health challenge that has led to increased morbidity, mortality, healthcare costs, and antibiotic consumption.13,14 The consolidated study by Yang in 2024, based on 21 articles with a research population of 4,885 DFI patients, shows that the rate of multidrug-resistant bacteria accounts for 50.86%, with Gram-positive bacteria representing 19.81% and Gram-negative bacteria making up 32.84%. Additionally, it notes that the rate of multidrug-resistant bacteria varies across studies depending on the definitions used and the characteristics of the patient populations. 15 Furthermore, MDR bacterial infections in DFI are linked to longer hospital stays, higher treatment costs, increased mortality rates, and a greater risk of lower extremity amputation.16,17 Hence, our study aimed to describe the antibiotic resistance of diabetic patients exposed to antibiotics before hospital admission in relation to the characteristics of foot infection at Cho Ray Hospital, Vietnam.
2. Methods
2.1. Study site and study population
This was a single-center, descriptive cross-sectional study with an exploratory purpose. The study was conducted at Cho Ray Hospital, a tertiary care center in Ho Chi Minh City, Vietnam, from November 2022 to May 2023. The research followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
2.1.1. Inclusion criteria
Patients were eligible for inclusion if they met the following criteria. 1. Aged 18 years or older with a confirmed diagnosis of Type 2 Diabetes Mellitus. 2. Presenting with a diabetic foot infection (DFI) graded Wagner 2 to 5. 3. Having a documented history of continuous antibiotic use for at least 48 hours at a primary or secondary healthcare facility immediately prior to admission to Cho Ray Hospital. 4. Providing informed consent to participate in the study.
2.1.2. Exclusion criteria
Patients were excluded based on the following: 1. Patients with foot ulcers of non-diabetic etiology (e.g., purely venous or arterial ulcers without underlying diabetes). 2. Pregnancy or breastfeeding. 3. Patients who were transferred to another department or hospital before a complete clinical and microbiological assessment could be performed. 4. Patients with incomplete medical records regarding their prior antibiotic history.
A convenience sampling method was employed, including all patients who met the inclusion criteria during the study period. Given the exploratory nature of this research and the specific focus on a high-risk subgroup (those with prior antibiotic exposure), a formal sample size calculation was not conducted. The study recruited all T2DPs with DFI (n=51) who met the hospitalization criteria as per Infectious Diseases Society of America (IDSA). 18 The 48-hour threshold is a well-established clinical benchmark. According to the CDC’s National Healthcare Safety Network (NHSN), 48 hours is the standard timeframe used to distinguish between community-acquired and healthcare-associated infections. 19 Furthermore, the Infectious Diseases Society of America (IDSA) guidelines emphasize that clinical response to empirical therapy should be evaluated within 48 to 72 hours; patients referred after this period often represent cases of initial treatment failure, which is frequently associated with MDR pathogens. 20 Importantly, this inclusion criterion is intended to identify a previously treated, healthcare-associated referral population rather than to serve as a direct quantitative measure of cumulative antibiotic exposure. Consequently, the duration of hospitalization at lower-level facilities serves as a clinical proxy for healthcare-associated antibiotic exposure and pre-referral treatment complexity.
The participant selection process is summarized in the STROBE flow diagram (Figure 1). Initially, 51 patients met the clinical inclusion criteria, including a history of prior antibiotic exposure. From these patients, 38 bacterial isolates (74.5%) were successfully recovered and subjected to antimicrobial susceptibility testing, while 13 samples (25.5%) yielded no bacterial growth. Flowchart of participant enrollment and bacterial culture outcomes.
2.2. Foot ulcer assessment
To assess the infected ulcers upon hospital admission, we collected information on age, gender, BMI, length of stay at the primary care level, and the antibiotics used prior to admission. To evaluate the extent of tissue damage of the ulcer, we measured the size of the ulcer and utilized the simple Wagner classification, which is easily applicable in clinical practice. The severity of foot ulcers was graded using the Wagner classification system, which is widely utilized in clinical practice for its simplicity in assessing ulcer depth. While it does not formally include a vascular component, clinical assessment of peripheral pulses was performed for all patients. The Wagner Scale assesses ulcer depth and the presence of osteomyelitis or gangrene by using the following grades
21
• • • • • •
When evaluating a T2DP with DFI, the clinician must first check for any signs of infection and, if found, determine the severity of that infection. We diagnosed diabetic foot infection based on the IWGDF/IDSA classification system. 8 Various prospective and retrospective studies have confirmed the IWGDF/IDSA DFI classification, either in whole or in part, as a component of a broader diabetes-related foot classification system (See Appendix 1).
While deep tissue biopsy is recommended by international guidelines,19,20 superficial wound swabs were utilized in this study following standardized cleansing and debridement. This approach was chosen based on its feasibility and non-invasive nature in a high-volume clinical environment.
2.3. Microbiology and antibiotic susceptibility testing
Sampling and Transport: After thorough cleansing of the ulcer with sterile 0.9% saline and surgical debridement of necrotic tissue, samples were obtained using the Levine technique, where a sterile swab is rotated over a 1 cm2 area of viable tissue with sufficient pressure to express tissue fluid. Swabs were placed in sterile transport containers and delivered to the microbiology laboratory within two hours of collection to ensure specimen viability.
Bacterial Identification: At the laboratory (ISO 15189 accredited), specimens were inoculated onto Blood Agar, MacConkey Agar, and Chocolate Agar (for fastidious organisms). Plates were incubated aerobically at 37°C for 18–24 hours, and up to 48 hours if no growth was initially observed. Initial identification was based on colony morphology and Gram staining. Final identification was performed using the Vitek 2 Compact automated system (bioMérieux, Marcy-l'Étoile, France) using GN (Gram-negative) and GP (Gram-positive) cards.
Antimicrobial Susceptibility Testing (AST): AST was performed using the Vitek 2 system with appropriate cards (e.g., AST-N281 for GN and AST-P633 for GP). The Minimum Inhibitory Concentrations (MICs) were determined and interpreted as Susceptible (S), Intermediate (I), or Resistant (R) according to the Clinical and Laboratory Standards Institute (CLSI) M100 guidelines current at the time of the study.
In cases of polymicrobial infections, each distinct morphotype was isolated, identified, and tested for antibiotic susceptibility independently. For clinical correlation analysis, patients harboring at least one MDR strain were classified into the MDR group.
2.4. MDR bacteria definition
MDR bacteria, as proposed by international experts in 2012, were approved by the European Centre for Disease Prevention and Control and the Centers for Disease Control and Prevention in the United States: Bacteria resistant to at least one antibiotic in a group of antibiotics and resistant to three or more groups of antibiotics. 12 Crucially, the Magiorakos framework defines MDR utilizing species-specific antimicrobial categories tailored to major public health pathogen groups, including Enterococcus spp., MRSA, Pseudomonas aeruginosa, Acinetobacter baumannii, and Enterobacterales. To determine Multidrug-resistance (MDR), we evaluated the susceptibility of isolates against 9 different antimicrobial categories for GN or GP including: Carbapenems (Meropenem), Extended-spectrum cephalosporins (Ceftriaxone), Glycopeptides (Vancomycin), Aminoglycosides, Penicillins, Fluoroquinolones, Oxazolidinones, Tetracyclines, and Nitroimidazoles.
2.5. Data analysis
Data from archived clinical records, direct examination at clinical wards were collected for analysis. The clinical, laboratory, and microbiological variables evaluated in this study—including patient demographics, glycemic markers, inflammatory indices, and ulcer characteristics—were selected based on established risk factors highlighted in prior diabetic foot infection literature. There were no missing data for the clinical, laboratory, or microbiological variables evaluated in this study. All 51 patients had complete records for the analyzed parameters. Statistical analysis was performed using STATA version 15. Continuous variables obtained from the clinical characteristics were expressed as the mean ± standard deviation and were compared using the student T-test. The Chi-squared test or Fisher’s exact test depending on the number of events for evaluated variables, was used for determining associated factors.
2.6. Ethical approval
The research complied with the requirements and regulations for biomedical research review of the Ethical Council with decision No.889/HDYD-DHYD on 22 Nov 2022.
3. Results
Patients’ characteristics at hospital admission (n=51).
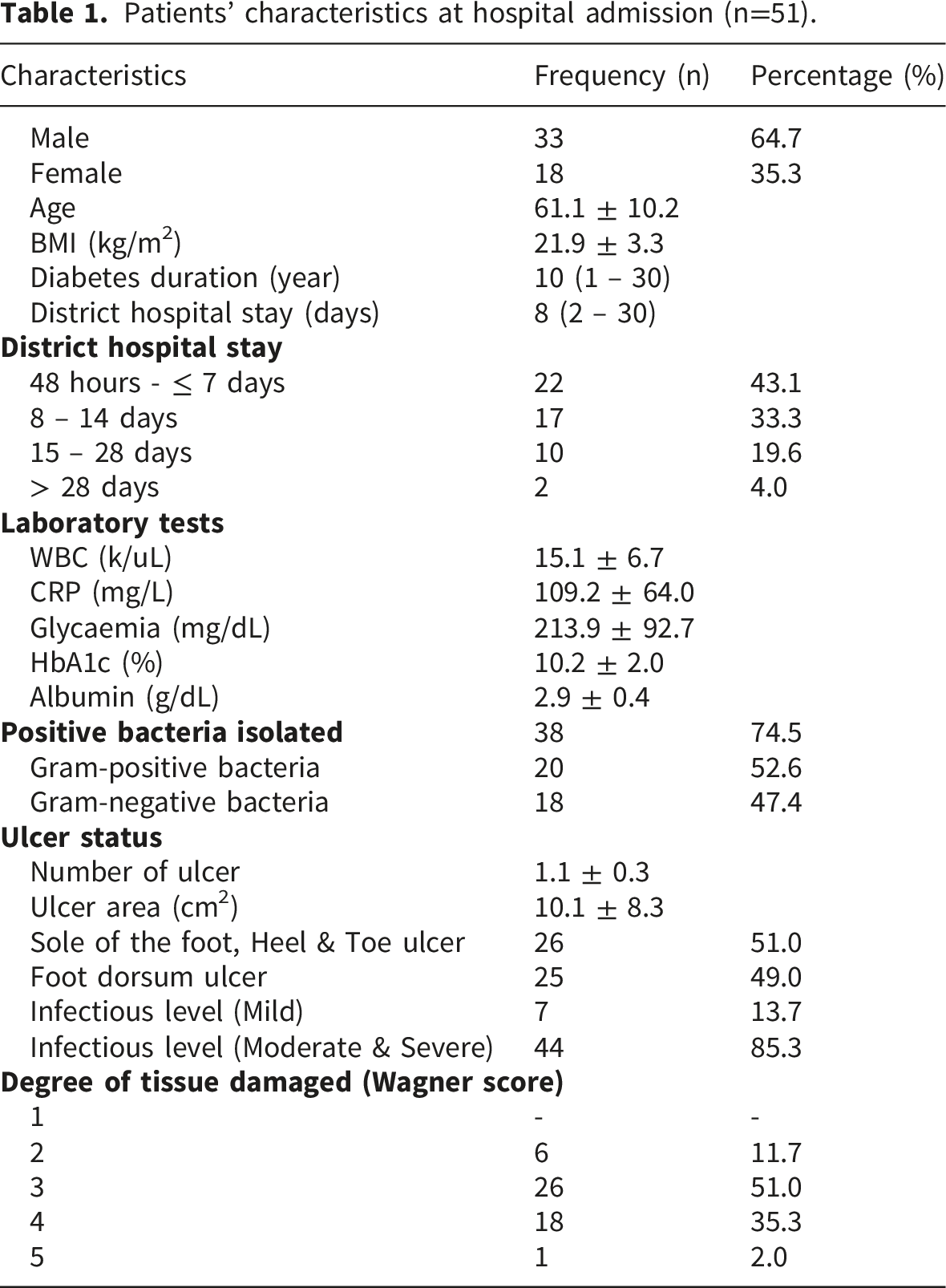
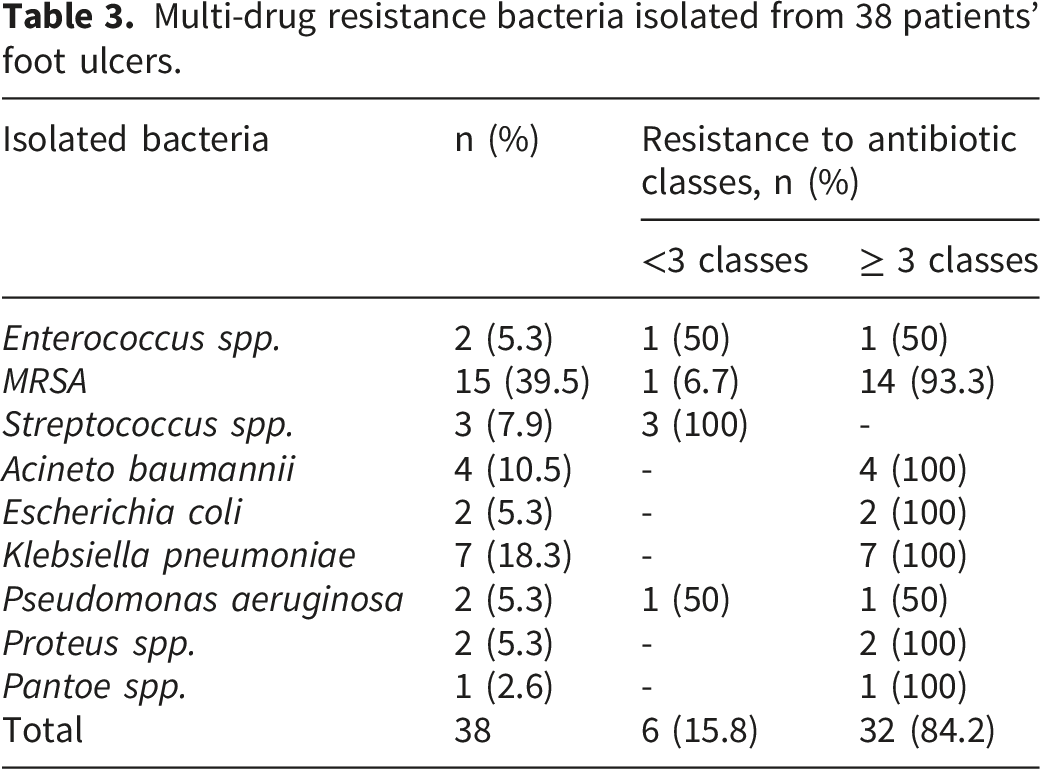
Regarding the microbial composition, all 38 positive cultures in this study yielded monomicrobial growth (100%), with each patient harboring a single isolated pathogen. Among these 38 isolates, 6 (15.8%) were fully susceptible to all tested antimicrobial categories, while the remaining 32 (84.2%) were classified as multidrug-resistant (MDR). The absence of polymicrobial infections in our study population is a notable finding, likely reflecting the selective pressure of prior antibiotic therapy.
3.1. Low rate of resistance to exposed or current administered antibiotics
Resistance to exposed or current administered antibiotics.
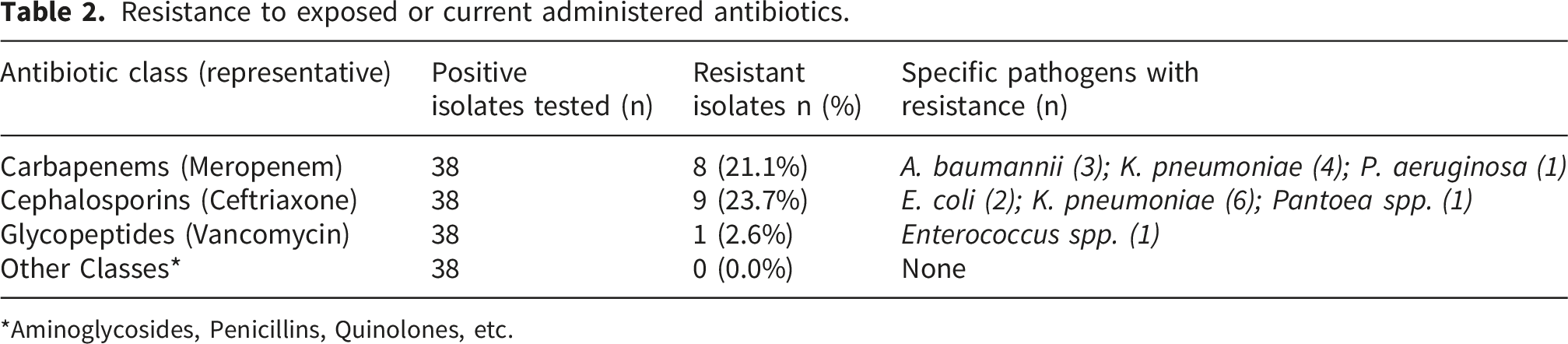
*Aminoglycosides, Penicillins, Quinolones, etc.
3.2. High rate of multi-drug resistance in 38 isolates
Multi-drug resistance bacteria isolated from 38 patients’ foot ulcers.
Patients’ clinical factors (n=38) associated to antibiotic resistance.
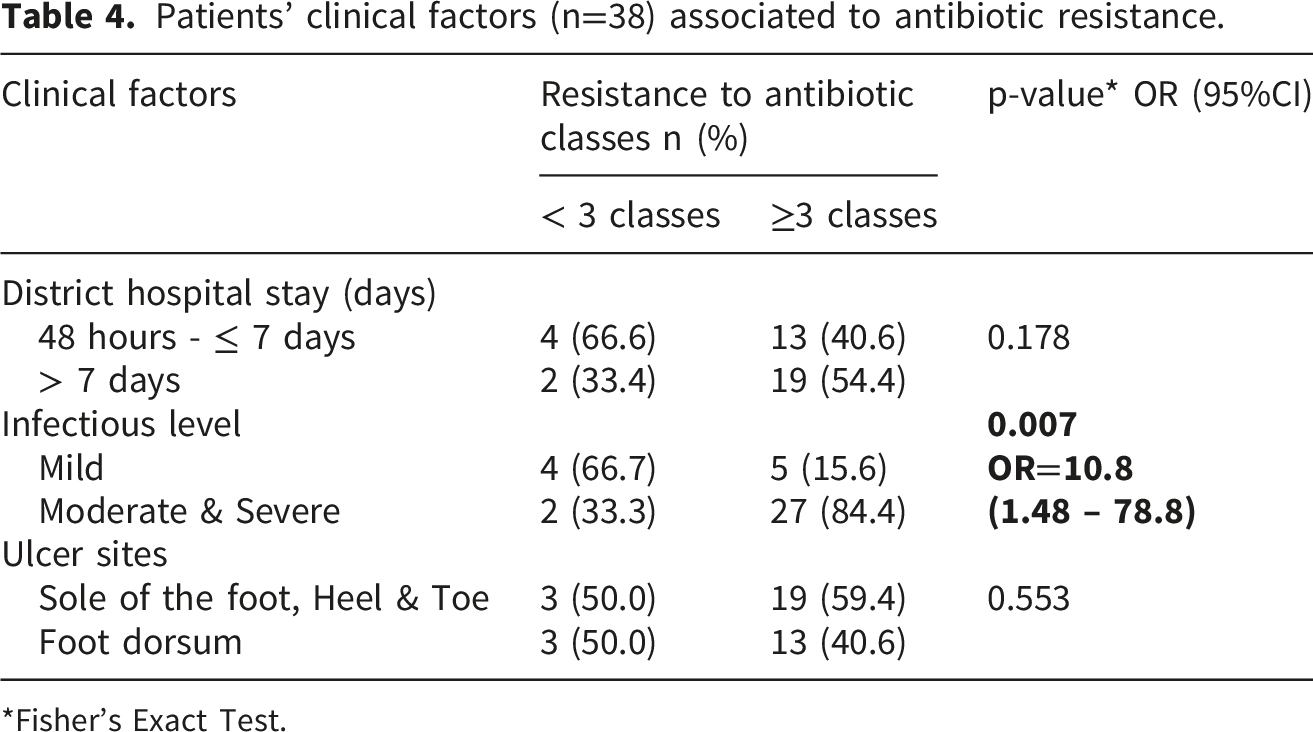
*Fisher’s Exact Test.
3. Discussion
Our cross-sectional study involved 51 T2PDs with DFI, predominantly male (64.7%), with an average age of 61.1 years. The median duration of diabetes was 10 years, and patients experienced significant clinical variability, as indicated by a median district hospital stay of 8 days. The study found a high rate positive culture positive of 74.5% with 38 bacterial isolates. This indicated that antibiotic treatment in the primary care setting was not effective, likely due to inappropriate antibiotic selection or bacterial resistance to the antibiotics used in the primary care. As a result, the culture results showed a high prevalence of bacterial growth, even after a median of 8 days of antibiotic use. Notably, 18 isolates exhibited high resistance levels, with significant concerns regarding carbapenem and cephalosporin resistance among gram-negative bacteria. Multi-drug resistance was noted in 84.2% of isolates, particularly among MRSA and several gram-negative strains. Patients with DFI caused by MDR bacteria had a significantly higher rate of severe infectious level ulcers compared to those infected with non-MDR bacteria, with an OR of 10.8 and a p-value of 0.007.
Generally, T2DPs are old and with a long duration of diabetes that highlight their susceptibility to complication associated with DFU. In our patients, the mean age was 61.1 years (±10.2), and the history of diabetes was more than 10 years, which aligns with the demographic trend of Type 2 diabetes patients with DFU typically being aged 50 years and older. This observation is consistent with findings from our previous study at Cho Ray Hospital 22 and other studies.3,23
The clinical parameters provided valuable insights into the infection status and tissue damage associated with DFI. Key indicators such as WBC count, CRP levels, and glycaemia play crucial roles in managing DFI. An elevated WBC count exceeding 11,000 k/uL indicates an infection, with clear distinctions observed between infected and non-infected groups 24 In our patients, the WBC count was 15,100 k/uL, indicating an ongoing infection. Similarly, CRP levels above 5 mg/L are correlated with infections and demonstrate high sensitivity and specificity in diagnosing DFI 24 Our patients exhibited an exceptionally high CRP level of 109.2 mg/L. Furthermore, poor glycemic control, as reflected in elevated glycaemia and HbA1c levels, is associated with increased ulcer severity and a heightened risk of infection. 11 Consistent with this, our patients showed high glycaemia and HbA1c levels of 213.9 mg/dL and 10.2%, respectively.
In our study, severe infectious levels were observed in 29.4% of patients despite undergoing antibiotic treatment, with a positive culture rate of 74.5%. Of the pathogens isolated, Gram-positive bacteria accounted for 52.6%, while Gram-negative bacteria constituted 47.4%. In comparison, other studies examining positive cultures following antibiotic administration reported a lower positive culture rate of 52.2%, with the proportion of Gram-negative bacilli rising to 68.9%. 25 and 65% were gram-negative bacteria, dominated by Escherichia coli (30%). Gram-positive bacteria were found in 35%, with Staphylococcus aureus (18%) as the most, 26 we observed a higher rate of positive cultures, characterized by a greater proportion of Gram-positive isolates (52.6% vs. 35%), while the rate of Gram-negative isolates was lower (47.4% vs. 65% or 68.9%). The prevalence of MRSA isolates was 39.5%, which surpasses the average rate reported in a meta-analysis encompassing 40 studies with 12,924 patients across 20 countries, where the overall prevalence of MRSA in DFI was found to be 17%, with an increase to 20% in low-income countries. 27 Our findings are similar to data from Poland, where research from 2014 to 2019 indicated MRSA isolation rates of 36.0%, 35.8%, 34.4%, 32.2%, 30.9%, and 30.2%, respectively. 28
While diabetic foot infections are often polymicrobial, our study exclusively identified monomicrobial growth in all positive samples. This observation can be attributed to the specific inclusion criteria of our study, where all participants had undergone a minimum of 48 hours of antibiotic treatment prior to sampling. It is highly probable that this pre-admission antibiotic exposure effectively eliminated more susceptible commensal and pathogenic bacteria, leaving behind only the single most resistant or dominant strain. This ‘filtering effect’ not only explains the monomicrobial nature of our samples but also accounts for the exceptionally high prevalence of MDR strains (84.2%) observed in our findings. The positive culture rate in our patients is influenced by bacterial resistance to current antibiotic regimens. Importantly, the resistance to antibiotics previously administered was found to be relatively low. Regarding the treatment of Gram-positive bacteria, glycopeptides, particularly vancomycin, exhibited a resistance rate of only 2.0% among Enterococcus spp., and all MRSA isolates remained susceptible. In contrast, the treatment of Gram-negative bacteria presented alarming resistance rates; carbapenems, specifically meropenem, showed a resistance rate of 15.7%, while cephalosporins, particularly ceftriaxone, displayed an even higher resistance rate of 17.6%. This highlights concerns regarding the efficacy of cephalosporins in managing infections caused by these pathogens. Furthermore, we evaluated antibiotic resistance across different classes to determine the rate of MDR, defining MDR as resistance to three or more classes of antibiotics. Among Gram-positive bacteria, MRSA demonstrated a significant antibiotic resistance rate of 93.3% to more than three classes. The increasing resistance of MRSA continues to pose a considerable challenge, complicating treatment options., 29 among the 112 MRSA isolates, 92.9% were classified MDR bacteria, exhibiting resistance to erythromycin, clindamycin, ciprofloxacin, and levofloxacin. 28 The alarmingly high MDR rate of 84.2% observed in our study must be interpreted in light of several methodological factors. First, the referral bias inherent in a tertiary care setting like Cho Ray Hospital means our study population consists primarily of patients with treatment-refractory infections. This is compounded by the prior use of antibiotics in 100% of the subjects, which likely eliminated susceptible strains and favored the persistence of MDR pathogens such as MRSA and carbapenem-resistant Gram-negative bacilli.
Among Gram-negative bacteria, certain strains, including Acinetobacter baumannii, Escherichia coli, and Klebsiella pneumoniae, exhibited complete (100%) multi-drug resistance. This finding aligns with previous research indicating that Acinetobacter baumannii and Klebsiella pneumoniae demonstrate concerning resistance profiles, particularly with respect to carbapenems.30–32
Bacteria exhibits antibiotic resistance predominantly through three mechanisms: intrinsic resistance to at least one class of antibiotics, acquired resistance via genetic mutations and the transfer of resistance genes from other bacteria. 33 The prevalence of MDR is highly complex and is associated with multiple factors beyond prior antibiotic exposure, including recurrent hospitalizations—a common occurrence in Vietnamese diabetic patients due to high re-ulceration rates. 22 Furthermore, the high background prevalence of carbapenem-resistant organisms in Vietnamese healthcare settings 32 and clinical factors such as ulcer duration 34 create a complex environment for resistance development. Consequently, factors such as diminished immune function, significant tissue damage, delayed wound healing, extended hospitalizations, and prolonged antibiotic use elevate the risk of MDR bacteria. This phenomenon is reflected in our study, where approximately two-thirds of the population demonstrated MDR. This finding is consistent with the study conducted by Yang, which identified several contributing factors, including a history of hospitalization and prior antibiotic use, that were significantly associated with MDR. 15 The study conducted by Liu, which employed the same diagnostic criteria as Yang’s research, identified several factors associated with multidrug resistance. These factors included a history of hospitalization, wound size greater than 4 cm2, the requirement for surgical treatment, and elevated CRP levels. 34 Noor’s study also reported that prior antibiotic use, low BMI, and HbA1c levels were associated with MDR. Conversely, the duration of diabetes and Wagner grade were not found to be significant factors, which is consistent with our findings. 35 Yan’s study similarly found that factors such as prior antibiotic use, body mass index (BMI), HbA1c levels, and wound size were significantly associated with multidrug-resistant bacteria. In contrast, the Wagner grade was not found to be a significant factor. 23 Zubair’s research indicated that, in addition to the duration of hospitalization, a wound size greater than 4 cm2 was significantly associated with MDR. 36 We found that factors such as the duration of diabetes greater than 10 years, HbA1c levels, Wagner grade, and wound size were not significantly associated with multidrug-resistant bacteria. This may be attributable to the similar distribution of these factors between the multidrug-resistant and non-multidrug-resistant groups. Furthermore, the reliance on the Wagner classification without objective vascular data (e.g., ABI) limits our ability to account for the impact of ischemia on treatment failure. Future studies should employ multidimensional systems like WIfI to better characterize the interplay between vascular status and microbial resistance. Despite these limitations, the strong association found between MDR and severe clinical outcomes (OR=10.8, p=0.007) underscores the urgent need for stricter antibiotic stewardship at the primary care level.
Our study has several limitations that warrant consideration. First, the research was conducted at a single national tertiary referral hospital, introducing a significant referral bias. Our patient population primarily consists of patients who had already failed initial antibiotic therapy at lower care levels; thus, the high MDR rate (84.2%) and infection severity reported may not be representative of the broader diabetic population in Vietnam, limiting the external validity of our findings. Second, we relied on superficial wound swabs rather than tissue biopsies. Although performed after rigorous cleaning according to IDSA/IWGDF principles, this method may capture colonizing flora rather than deep-seated pathogens, and we did not perform molecular testing for resistance mutations. Additionally, although nine broad antimicrobial categories were evaluated in this study, not all categories are clinically applicable or routinely tested for every specific bacterial species. Because the Magiorakos criteria rely on species-specific panels, evaluating a standardized set of categories without universal biological applicability across all isolates may have caused us to inadvertently underestimate the true resistance burden in certain species. Additionally, our assessment of ulcer severity relied solely on the Wagner classification, which lacks objective vascular assessments (e.g., ABI or Doppler). The absence of more comprehensive systems like the WIfI classification may limit the clinical characterization of ischemia in our population. Finally, the association found between MDR and infection severity (OR=10.8) should be interpreted with caution. Because severe infection is frequently a downstream consequence of treatment failure driven by resistant pathogens, these two variables likely lie within the same causal pathway. Due to our small sample size, we could not perform multivariable adjustment to account for potential confounders or collinearity, such as prolonged hospital stays or poor glycaemic control. While our results provide a critical reflection of the resistance challenges in specialized facilities, future large-scale studies with robust statistical modeling and tissue biopsies are required to confirm these exploratory findings.
5. Conclusion
Our study identified a notable prevalence of MDR bacteria (84.2%) among referred patients with diabetic foot infections at a tertiary center. These findings suggest a potential association between prior antibiotic exposure and the presence of highly resistant pathogens, which often coincided with more severe clinical presentations in our patients. While limited by the exploratory and single-center nature of the research, these observations underscore the importance of considering antimicrobial stewardship and continuous resistance monitoring within referral networks.
Supplemental material
Supplemental material - Supplemental material for High prevalence of multidrug-resistant bacteria in diabetic patients with foot ulcers: A descriptive analysis of patients referred to a tertiary care hospital in Vietnam
Supplemental material for High prevalence of multidrug-resistant bacteria in diabetic patients with foot ulcers: A descriptive analysis of patients referred to a tertiary care hospital in Vietnam by Tan Dat Huynh, Manh Nguyen Nguyen and Chi Thanh Tran in Journal of Public Health Research.
Footnotes
Acknowledgments
We would like to thank Cho Ray Hospital for supporting our research.
Ethical considerations
The research complied with the requirements and regulations for biomedical research review of the Ethical Council of the University of Medicine and Pharmacy of Ho Chi Minh City. The study was approved by the Ethics Committee in Biomedical Research at the University of Medicine and Pharmacy of Ho Chi Minh City under Decision No.889/HDYD-DHYD on 22 Nov 2022. And the study was also approved by the Cho Ray Hospital’s Board of Directors to carry out the project.
Author contributions
Huynh Tan Dat: Contributed to conception, design, data acquisition and interpretation, critically revised the manuscript. Nguyen Manh Nguyen: Contributed to conception, data acquisition and interpretation, drafted the manuscript. Tran Chi Thanh: Contributed to conception, design, data acquisition and interpretation, critically revised the manuscript. All authors gave their final approval and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article. This research was self-funded by research group.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.