
Abstract
Background
Vision impairment remains a major global public health concern, with persistent gender disparities in access to eye care services, particularly in low- and middle-income countries. Evidence from Nepal suggests inequities in service utilization despite expanded outreach programs. This study aimed to examine gender-specific patterns of eye care service utilization in outreach settings.
Design and Methods
This retrospective cross-sectional study analyzed secondary data from 43,848 individuals screened at diagnostic, screening, and treatment (DST) and surgical outreach camps organized by 23 Nepal Netra Jyoti Sangh hospitals across all seven provinces of Nepal between 2020-2024. Demographic, clinical, and service-utilization data were summarized descriptively, and associations were tested using chi-square analysis (SPSS v23; p<0.05).
Results
Women accounted for 53.1% (n=23,290) of service users, with slightly higher outreach participation than men (75.6% vs. 74.5%). However, women’s participation declined with age, from 78.9% in those under 60 years to 60.5% in those aged ≥80 years. Cataract was the predominant diagnosis (n=42,239; 96.3%), more frequent among women (52.8%), while trauma-related surgeries were more common in men (78.6%). Follow-up rates were higher among patients treated by female surgeons (60.4%) compared to male surgeons (49.1%) (p<0.001). In multivariable analysis, patient gender showed a minimal association with follow up (AOR= 1.04, 95%CI: 1.00 -1.08). In contrast, patient treated by female surgeon was independently associated with higher odds of follow up (AOR:1.45, 95%CI: 1.39 -1.51). Significant provincial variation in follow-up attendance was observed, with significantly higher odds in most provinces compared to Sudurpaschim Province. Patient received service though surgical camp had the highest likelihood of follow up compared to walk-in patients (AOR=3.79).
Conclusion
The finding highlights eye care service utilization varied by gender, age, patient residence, outreach modality in Nepal. Follow up was more influenced by surgeon gender and outreach modalities than by patient gender alone. Targeted, gender-responsive strategies are needed to improve equitable access and strengthen continuity of care, particularly for older women.
What we already know
• Nepal is developing country with low health literacy with difficult access to health care and pattern as well as burden of visual impairment, ocular diseases vary with demographic profile of the population. • Female patients exhibit varied pattern of service utilization due to barrier like limited access, lack of awareness, social stigma, fear and financial constraints • Women carry two third of blindness in Nepal, but persistent gender inequity has marginalized women from accessing eye care services.
What this article adds
• Women comprised 53.1% of total service consumers and showed higher participation in outreach programs (75.6%) than men (74.5%), but female outreach utilization declined with age—from 78.9% under 60 years to 60.5% over 80 years. • There was a significant association (p < 0.001) between patient follow-up status and the gender of surgeons, highlighting critical gaps in understanding gender-specific service utilization patterns at diagnostic, screening, and treatment camps in Nepal. • Periodic, well-managed eye camps in rural areas are needed to effectively reach underserved populations, alongside government efforts to improve accessibility to specialized healthcare facilities for those unable to afford treatment costs.
Introduction
Globally, vision impairment remains a major public health concern with one billion cases such as cataract and refractive error which are preventable or treatable. The World Report on Vision (2019) highlights that women with moderate to severe distance vision impairment outnumber men by around 7%. 1 In 1999, the World Health Organization (WHO) and the International Agency for the Prevention of Blindness (IAPB) launched VISION 2020: The Right to Sight, a global initiative aimed at eliminating avoidable blindness by improving access to quality eye care. 2 The Lancet Global Health Commission on Global Eye Health reports that over 90% of vision impairment cases can be prevented or treated through cost-effective interventions. 3
Despite global progress, significant disparities persist mostly in low middle income countries, particularly among women, marginalized populations, due to a combination of biological factors and socio-cultural barriers, including financial dependency, restricted mobility, limited decision-making power. 1 In such settings, barriers to accessing education, economic opportunities, and social inclusion further hinder the achievement of the Sustainable Development Goals and equitable eye health services for all. 4
Nepal exists as a example in the evolving landscape of eye care and conducting regular national blindness surveys, Nepal’s first survey in 1981 reported a blindness prevalence of 0.84%, prompting the establishment and expansion of national eye care services. 5 Subsequent surveys using the Rapid Assessment of Avoidable Blindness (RAAB) methodology between 2006 and 2010 estimated a prevalence of 2.5% among individuals aged 50 years and above, with an extrapolated overall prevalence of 0.35% reflecting an approximate 60% reduction from 1981 levels.5,6
The most recent RAAB survey (2018–2021), conducted across seven provinces, reported a national blindness prevalence of 1.1% among those aged 50 years and older, with an extrapolated overall prevalence of 0.28%. Women were more affected (1.3%) than men (0.9%).7,8 Cataract remained the leading cause of blindness, with approximately two-thirds of cases occurring in women, who frequently face barriers.7,8
Gender disparities have also been documented in refractive error services. A study on presbyopia reported higher prevalence among younger women compared to men; however, service utilization was greater among men. 9 Furthermore, differences in corrective lens distribution (52.29% for men versus 47.71% for women) suggest greater attendance of older men at outreach health camps. 9 In rural areas, untreated cataract disproportionately affects women from low-income households, underscoring the need for targeted interventions such as expanded outreach services, increased screening programs, improved referral systems, and health financing mechanisms to enhance surgical uptake.
This study aims to address critical gaps in understanding gender-specific patterns of service utilization at diagnostic, screening, and treatment (DST) camps in Nepal. By analyzing demographic, clinical, and outreach-related characteristics, the research seeks to identify trends and inform targeted strategies to reduce gender disparities in eye care—ultimately contributing to more equitable health outcomes.
Design and Methods
Study design and setting
This retrospective cross-sectional study analyzed data from surgical camps and Diagnostic, Screening, and Treatment (DST) eye camps supported by the DAK Foundation, conducted between 2020 and 2024 in 23 eye hospitals operated by Nepal Netra Jyoti Sangh (NNJS) across all seven provinces of Nepal.
Sample size and sampling techniques
The study included all walk-in patients at hospitals, as well as individuals attending DST and surgical eye camps. In total, 43,848 participants of all age groups were screened in community-based camps and, when indicated, transported to base hospitals for cataract surgery.
Ophthalmic evaluation and data collection
Camps were organized with active community engagement, involving local organizations and volunteers. A trained team—comprising ophthalmologists, optometrists, ophthalmic assistants, opticians, and eye health workers—conducted community-based eye examinations. The primary focus was on detecting operable cataract cases and arranging transportation for surgical management. Ophthalmic assistants and eye health workers collected detailed patient histories including gender, age, address, diagnosis of ocular condition, RE/LE, pre operated VA and follow ups VA and recorded presenting complaints, while ophthalmologists performed comprehensive eye examinations, including visual acuity testing with Snellen’s charts and handheld slit-lamp evaluations to detect cataracts, refractive errors, conjunctivitis, retinal disorders, and other ocular pathologies. Minor conditions such as conjunctivitis and refractive errors were treated on-site, while complex cases were referred to tertiary facilities or specialized surgical camps.
At the base hospitals, cataract surgeries were primarily performed using Small Incision Cataract Surgery (SICS) with intraocular lens (IOL) implantation, adhering to standard clinical protocols. Postoperative assessments included first-day visual acuity testing, followed by discharge with topical antibiotics and corticosteroids. Patients with complications were retained for further management. All surgical patients were counselled and scheduled for a six-week follow-up to assess visual outcomes. All individuals who attended the outreach camp were registered for service delivery and received appropriate interventions, including medications and spectacles, as required. Participants who required surgical intervention and were referred to surgical or DST camps constituted the primary study population. For data analysis, only patient records containing complete demographic information, clinical history, diagnosis, treatment details, and follow-up data were included. Records with incomplete or missing information were excluded from the analysis.
Data management and statistical analysis
Visual outcomes were categorized according to WHO guidelines: good outcome (6/6–6/18), borderline outcome (6/24–6/60), and poor outcome (<6/60). Blindness was defined as presenting visual acuity (PVA) of ≤3/60, and visual impairment as PVA <6/12. 10 Data were extracted from camp and hospital medical records, including pre- and postoperative visual acuity, and entered into Microsoft Excel before analysis in SPSS Version 23 (SPSS Inc., Chicago, IL, USA). Descriptive statistics were generated as frequencies and percentages, presented in tables and graphs. Associations between categorical variables were assessed using the chi-square test, with p<0.05 considered statistically significant. A multivariate analysis was performed to identify factors associated with follow up utilization, adjusting for potential confounders. Adjusted odds ratios (AOR) with 95% confidence interval were reported.
Ethical consideration
Ethical approval was obtained from the Institutional Review Committee of NNJS (Reg. no. 38/2024). The study adhered to the principles of the Declaration of Helsinki. As this was a retrospective review of existing camp and hospital records, informed consent was not required. Data collection and reporting followed the STROBE Statement guidelines.
Results
Demographic characteristics of service utilization by gender
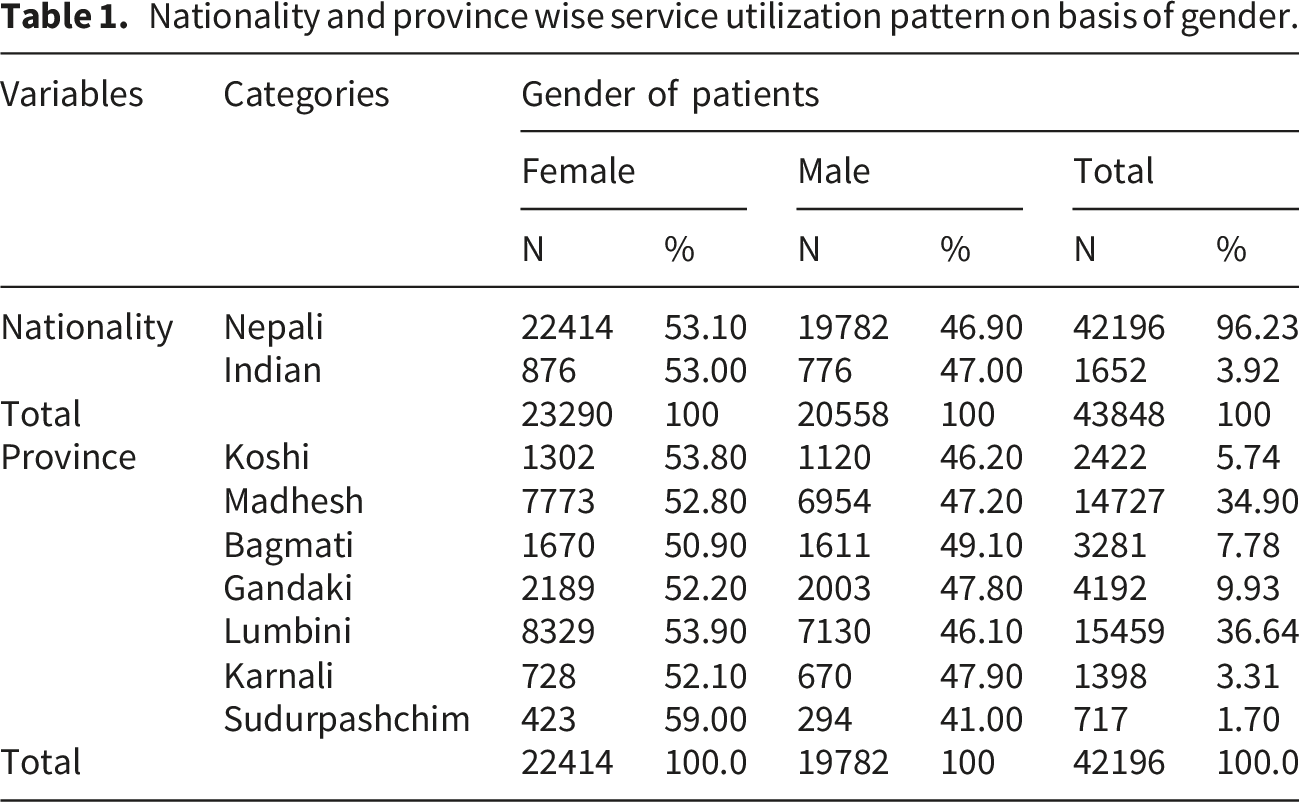
Nationality and province-wise service utilization
Nationality and province wise service utilization pattern on basis of gender.
Age groups and surgeon’s gender wise service utilization
Analysis by age group revealed distinct patterns in gender distribution. Among patients below 60 years, females predominated 5,800 (58.5%) compared to males 4,115 (41.5%), constituting 22.6% of the overall cohort. In the 60–69 years group, females comprised 9,517 (53.8%) and males 8,180 (46,2%), representing 40.4% of the total. In the 70–79 years category, the distribution was nearly equal, with females at 6,433 (50.3%) and males at 6,357 (49.7%). However, among those aged 80 years and above, males 1,906 (55.3%) outnumbered females 1,540 (44.7%), suggesting that older women may face additional barriers to accessing care.
Regarding the gender of the surgeons, both male and female providers contributed substantially to service delivery. Male surgeons performed procedures on 25,860 patients 13,671 females (52.9%) and 12,189 males (47.1%) accounting for 59.0% of the cases. In contrast, female surgeons operated on 17,988 patients 9,619 females (53.5%) and 8,369 males (46.5%) representing 41.0% of the total (Supplemental table 1).
Mode of DST service utilization by gender and age group
Outreach services were the predominant mode of eye care utilization across all age groups for both genders, accounting for approximately three-quarters of total use (female: 75.6% of 23290, male: 74.5% of 20558). Females consistently showed slightly higher utilization of outreach services than males across most age groups (e.g., below 60 years: 78.9% vs 76.6%; 60–69 years: 79.0% vs 77.8%). However, with increasing age, reliance on outreach services declined for both genders (e.g., ≥80 years: female 60.5%, male 61.9%), accompanied by a rise in surgical camp utilization (female: 11.0% to 31.8%; male: 13.3% to 30.6%). Walk-in service utilization remained low and relatively stable across all age groups (female: 7.7–10.1%, male: 7.1–10.0%). Overall, gender differences were modest, although males showed slightly higher use of surgical camps (17.6% vs 16.1%). This suggests that outreach activities are the primary access point for most patients, especially women and younger age groups, while older individuals rely more on surgical camps (Supplemental table 2).
Clinical characteristics of service utilization by gender
Diagnosed cases according to gender
Cataract was the predominant diagnosis, accounting for 42,239 cases (96.3%). Among these, 22,289 cases (52.8%) were in females and 19,950 cases (47.2%) in males. Eyelid and lacrimal system conditions were diagnosed in 164 patients, with a higher frequency in females (111 cases; 67.7%) compared to males (53 cases; 32.3%). Conjunctival and ocular surface conditions were identified in 94 patients, with 72 cases (76.6%) in females and 22 cases (23.4%) in males. Pterygium was diagnosed in 1,024 patients, with females accounting for 655 cases (64.0%) and males 369 cases (36.0%). In contrast, corneal conditions were observed predominantly in males (11 cases; 73.3%) versus 4 cases (26.7%) in females, and glaucoma-related conditions were also more frequent among males (6 cases; 60.0%) than females (4 cases; 40.0%). Diagnoses of pseudophakia, post-surgery trauma, retinal and optic nerve conditions, and other disorders were recorded in smaller proportions (Supplemental table 3).
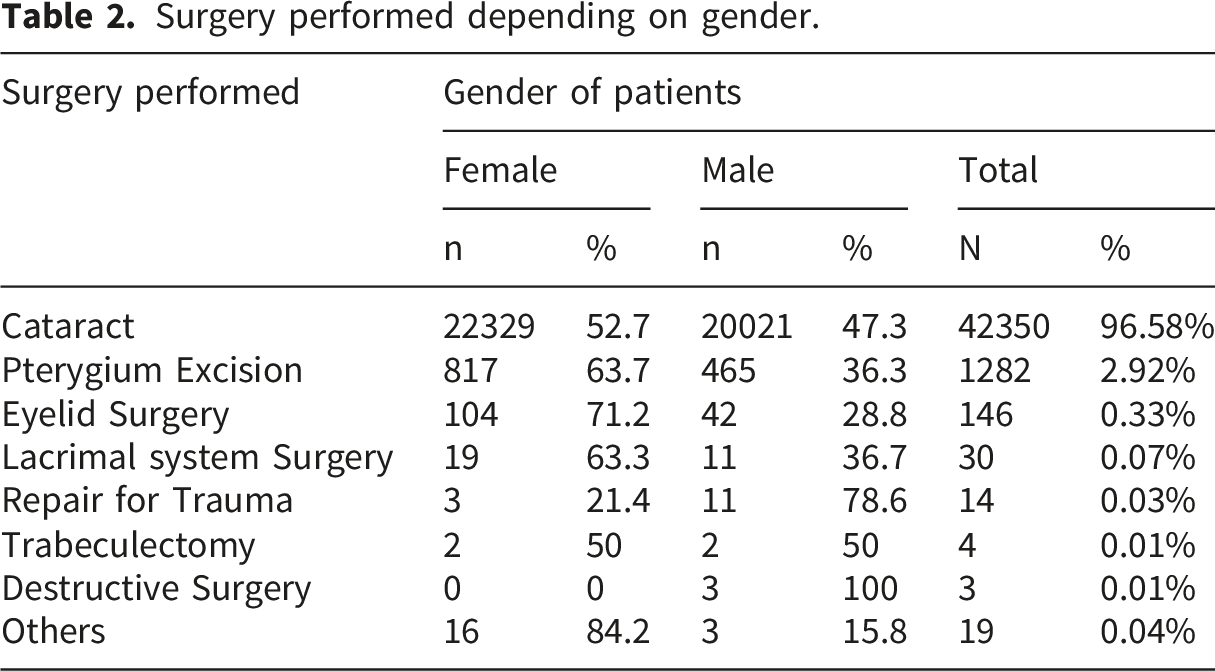
Surgeries performed depending on gender
Surgery performed depending on gender.
Follow-up status of patients by gender of patient and surgeon
Follow-up status of patients by gender of patient and surgeon.

*The Chi-square statistics are significant at the .05 level.
Association of follow-up status with independent covariates: Multivariable logistic regression analysis
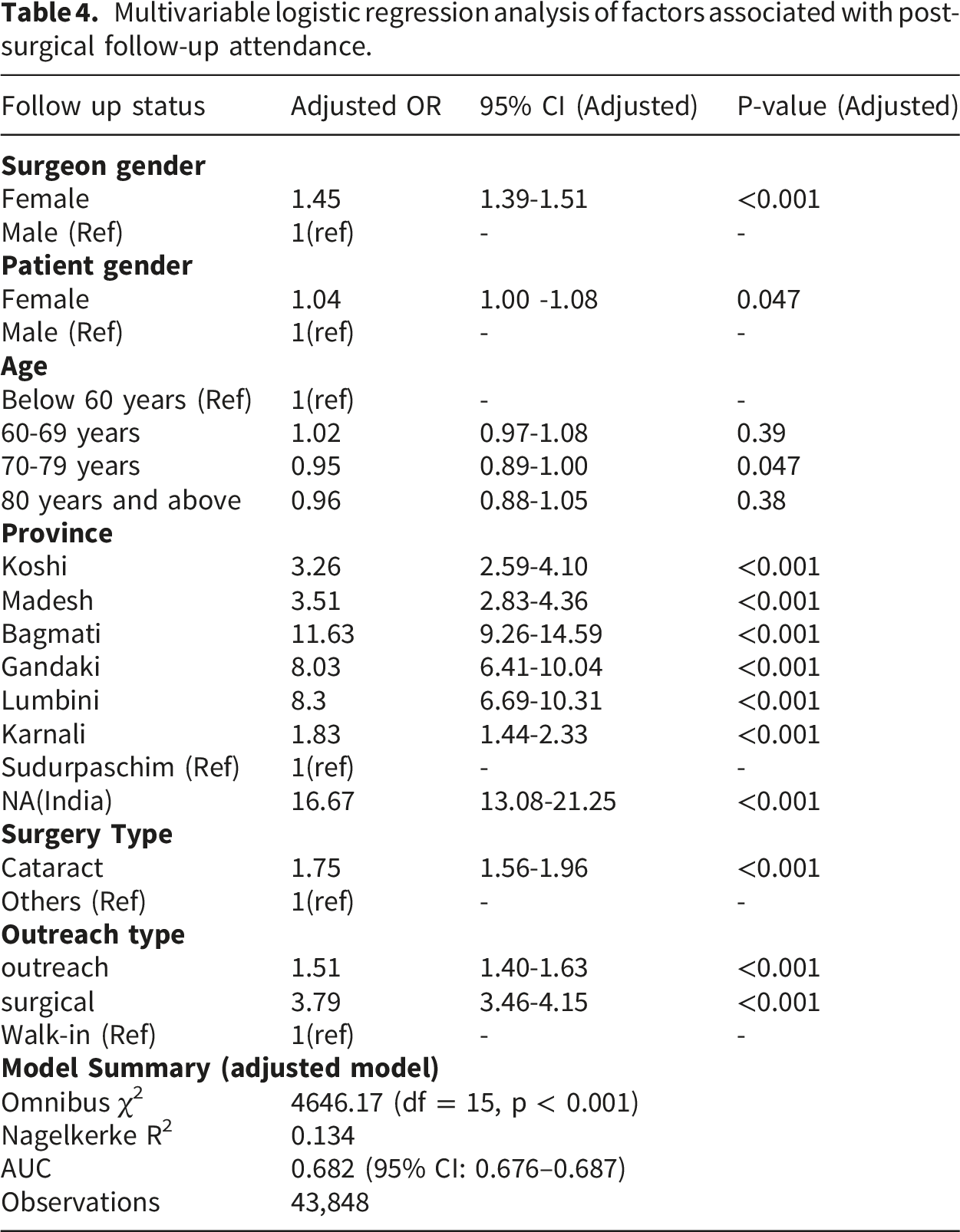
Multivariable logistic regression was performed to identify factors independently associated with post-surgical follow-up attendance, after adjusting for potential confounders. The overall model was statistically significant (Omnibus χ2 = 4646.17, df = 15, p < 0.001), indicating that the predictors collectively explained follow-up attendance beyond chance. The model demonstrated modest discriminative ability, with an Area under the ROC Curve (AUC) of 0.682 (95% CI: 0.676–0.687) and explained 13.4% of the variance in follow-up status (Nagelkerke R2 = 0.134), consistent with the multifactorial nature of health service utilization behavior.
After adjustment, Female patients had marginally but significantly higher odds of attending follow-up compared to male patients (AOR = 1.04, 95% CI: 1.00–1.08, p = 0.047), suggesting a modest independent gender effect on follow-up behavior. Patients aged 70–79 years had slightly lower odds of follow-up compared to those below 60 years (AOR = 0.94, 95% CI: 0.89–0.99, p = 0.047). The 60–69 years and 80 years and above age groups did not differ significantly from the reference category (p > 0.05).
A strong independent association was observed with surgeon gender. Patient treated by female surgeons has significantly higher odds of follow up compared to those treated by male surgeon (AOR= 1.45, 95%CI: 1.39-1.51). Significant provincial variation in follow-up attendance was observed, with Sudurpaschim as the reference category. Patients from NA (India) had the highest odds of follow-up attendance (AOR = 16.67, 95% CI: 13.08–21.25), followed by Bagmati (AOR = 11.63, 95% CI: 9.26–14.59), Lumbini (AOR = 8.30, 95% CI: 6.69–10.31), and Gandaki (AOR = 8.03, 95% CI: 6.41–10.04). Koshi (AOR = 3.26), Madesh (AOR = 3.51), and Karnali (AOR = 1.83) also showed significantly higher odds of follow-up compared to Sudurpaschim (all p < 0.001), indicating that patients from Sudurpaschim had the lowest follow-up rates across all provinces.
Multivariable logistic regression analysis of factors associated with post-surgical follow-up attendance.
Discussion
This retrospective study highlights persistent gender-based disparities in eye care service utilization in Nepal, underscoring the urgency of targeted strategies to promote equitable healthcare access. Analyzing demographic trends, regional patterns, and outreach program effectiveness, the findings reveal both critical gaps and promising opportunities to strengthen Nepal’s eye care delivery system.
Among the service recipients, 96.2% were Nepali nationals, with females representing a consistent majority 53.1% among Nepali and 53% among Indian nationals. This higher utilization among women mirrors global trends that reflect women’s disproportionately greater burden of vision impairment, driven by both biological and socio-cultural determinants.11,12 Comparable findings have also been reported in previous Nepali studies. 13 Notably, more women accessed services through rural outreach clinics, likely due to the free provision of care. Evidence suggests that no-cost healthcare initiatives such as community eye centers and free surgical eye camps substantially enhance service uptake, particularly among underserved groups including women, children, and the elderly. 14 However, a recent school-based study observed higher utilization by male students, although this difference was not statistically significant. 15
Despite the overall higher participation of women, significant challenges persist in meeting their eye care needs. Women continue to face barriers such as financial dependency, illiteracy, and restricted social mobility. 16 Interestingly, women below the age of 60 were more frequently represented (58.5%), whereas utilization declined with age, with males constituting the majority in the 80+ group. This trend may be attributed to mobility limitations, insufficient communication with providers, a lack of elderly-friendly services, and affordability concerns. However, studies have also identified family support as a crucial enabler in overcoming such barriers, particularly among older adults. 17 While the latter study affirms the influence of age on healthcare utilization, it does not offer a gender-specific breakdown of access challenges. 18
Gender disparities were also observed across Nepal’s diverse ecological regions, with the most pronounced gaps in the Terai region. 13 In this study, Lumbini Province recorded the highest number of users (n = 15,459), of whom 53.9% were women. Sudurpashchim Province had the highest female proportion at 59%. These regional differences point to the importance of developing locally tailored strategies to address specific contextual barriers.
Cataracts emerged as the most common diagnosis, accounting for 96.33% of cases, with a slightly higher prevalence in women (52.8%). This finding aligns with global evidence indicating a higher cataract risk among females.19,20 In this study trauma-related surgeries were more common among males potentially reflecting occupational exposure and risks. While women generally experience a higher burden of visual impairment, men may face distinct vulnerabilities particularly in conflict zones or high-risk workplaces. 21
Outreach initiatives were found to be particularly effective in enhancing service access for women. Over 75% of female participants utilized outreach services, indicating a strong dependence on proactive, community-based models. These programs have proven to be both impactful and cost-effective, particularly in resource-constrained settings like Nepal. When properly scaled, outreach services not only broaden rural coverage but also support sustainability across social, economic, and environmental dimensions. 22
After adjustment, the multivariable analysis showed that follow up utilization was influenced by service delivery modality and surgeons’ gender than by patient demographics characteristics, particularly, patient gender and age. Although the model was statistically significant, the low pseudo R2 suggests that additional unmeasured factors also contribute to follow up utilizations. Patient treated by female surgeons had higher likelihood of follow up, indicating that provider-patient interaction and communication may play an important role in continuity of care. Similarly, service modality through surgical camps was significantly associated with better follow up compared to walk-in services, suggesting that structured outreach models enhance continuity. Geographical variation remained significant even after adjustment, highlighting persistent regional difference in access and health system performance. In contrast, patient gender showed only a minimal effect, suggesting that although descriptive patterns indicate gender disparities in service utilization, follow up utilization may be more strongly shaped by health system and service delivery factors than by gender alone.
A difference of nearly 10% in follow-up visits was observed, indicating that patients treated by female surgeons were more likely to adhere to follow-up recommendations compared to those treated by male surgeons. While the underlying mechanisms cannot be directly examined using the available data, several plausible explanations may account for this association. Evidence suggests that female healthcare providers are more likely to adopt patient-centered communication styles, characterized by greater empathy and attentiveness, and may be preferred by patients for more sensitive and personalized care. 23 Effective clinician–patient communication has been consistently linked to improved treatment adherence and continuity of care. The World Health Organization World Report on Vision 2019 further highlights that the acceptability of eye care services—shaped by characteristics of the health workforce such as gender, language, culture, and age—plays a critical role in service utilization and outcome. 1 Additionally, gender concordance between provider and patient has been associated with enhanced patient experience and satisfaction. 24 These dynamics may be particularly relevant in sociocultural contexts like Nepal, where gender norms can influence healthcare interactions. However, these interpretations should be considered exploratory, as the study design does not allow direct assessment of these mechanisms, and this remains an important area for future research.
Four day screening of eye disease in rural areas of Nepal shows out of 250 patients (54.80% males and 45.20% females), Cataract was the commonest ocular disease (29.6%) among the screened population and 24% (60 patients) of them required cataract surgery (57% male and 43% female). 25 Comparative study performed in the hospital like Tilganga Institute of Ophthalmology, females accounted for 50.8% of patients receiving outpatient care and 48.3% of patients receiving surgical care. In rural outreach clinics, females accounted for 56.1% of clinic patients and 51.5% of patients undergoing surgery. 26 Similar to our study utilization of eye care services in an underserved community in Enugu State, Nigeria shows majority (65.6%) of services utilizations were females. Utilization of eye care services was associated with age, religion, occupation, marital status, monthly income, education, family history, and history of ocular disease. The major barrier to the utilization of eye care services was cost (30%), distance (22.6%), and bad road infrastructure. 27 Similar study results was seen in study of our neighboring country India which shows almost 55% of surgeries were on female eyes, and this proportion grew slightly over the time window. The mean age of male patients at the time of surgery was 62.4 years while that of female patients was 60.3 years. The median ages were 63 years for male patients and 60 years for female patients. 28 In study of eye care services utilization in South Ethiopia shows study respondents was 48 (±10) years and 52.7% were females and the proportion of eye care services utilization among older population was found to be low which is comparable to our study. 29
This study has few limitations. First, the retrospective design and reliance on secondary programmatic data restricted the availability of detailed socio-cultural and economic variables. Important factors such as education level, household income, decision-making autonomy, and prevailing gender norms—which are known to influence healthcare-seeking behavior—were not captured in the dataset. As a result, the study could not comprehensively assess the underlying drivers of the observed gender disparities in eye care utilization. Therefore, findings should be interpreted with caution, and future studies incorporating primary data collection are recommended to better understand these contextual determinants. Second, this study did not capture intersectional socio-demographic characteristics such as socioeconomic status, disability status, caste/ethnicity, or other forms of marginalization. These factors may interact with gender to shape access to eye care services in complex ways. The absence of such variables limits our ability to fully understand compounded inequalities and may underestimate disparities among the most vulnerable populations. Future research should adopt an intersectional approach to better elucidate how overlapping social identities influence eye care utilization in Nepal. Additionally, the absence of qualitative data hinders a comprehensive understanding of the socio-cultural dynamics, stigma, financial dependency, cultural norms shaping access to eye care. Therefore, it is suggested to conduct mixed methods of studies in future to address such gaps. Sample size calculation was not undertaken, as the study included all eligible cases with complete records available during the study period. Thus, a complete enumeration approach was adopted.
Conclusion
This study underscores the need to routinely collect gender-disaggregated data and monitor male-to-female service utilization ratios in Nepal’s eye care sector. Implementing gender-sensitive, evidence-based approaches is essential to reducing access disparities. Expanding community-based outreach, enhancing primary eye care infrastructure, subsidizing treatment costs, and developing targeted interventions for elderly women are critical steps toward more equitable service delivery.
The study further demonstrates that continuity of care is more influenced not only by patient gender, but also by service delivery and provided related factors, particularly surgeon gender and outreach modality. Future research should deepen the analysis of gender and eye care access, incorporating intersectional perspectives to inform inclusive policies. By addressing current service gaps and systemic barriers, Nepal can move meaningfully toward a more equitable and inclusive eye care system—one that ensures access for all, regardless of gender, age, or geographic location.
Supplemental material
Supplemental material - Utilization patterns of eye care services among women in outreach camps: A retrospective study from Nepal
Supplemental material for Utilization patterns of eye care services among women in outreach camps: A retrospective study from Nepal by Ranjan Shah, Alina Sapkota, Sabina Shrestha, Sailesh Kumar Mishra, Manish Gautam, Anil Paudel, Anup Subedi, Nisha Jha, Sanju Maharjan, Reena Yadav, Suruchi Shahi, Chet Raj Pant, Bharat Bahadur Chand, Amrit Poudel and Krishna Khadka in Journal of Public Health Researc.
Supplemental material
Supplemental material - Utilization patterns of eye care services among women in outreach camps: A retrospective study from Nepal
Supplemental material for Utilization patterns of eye care services among women in outreach camps: A retrospective study from Nepal by Ranjan Shah, Alina Sapkota, Sabina Shrestha, Sailesh Kumar Mishra, Manish Gautam, Anil Paudel, Anup Subedi, Nisha Jha, Sanju Maharjan, Reena Yadav, Suruchi Shahi, Chet Raj Pant, Bharat Bahadur Chand, Amrit Poudel and Krishna Khadka in Journal of Public Health Researc.
Footnotes
Acknowledgements
We want to acknowledge the entirely ophthalmic and administrative personnel from all the eye hospitals who contributed to the survey and conducting the camps. We are grateful to the Institutional Review Committee of Nepal Netra Jyoti Sangh for granting ethical approval for the survey.
Ethical considerations
Ethical issues (Including Plagiarism, Data Fabrication, Double Publication) have been completely observed by authors.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author (Mr. Ranjan Shah, ranjan_shah@nnjs.org.np) upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.