
Abstract
Objectives
Hypertension is a major global health concern contributing to elevated mortality from heart attacks, strokes, and chronic kidney disease, with a growing prevalence attributed to sedentary lifestyles, poor diet, obesity, and an aging population. This trend is also noticeable in Iran, underscoring the necessity of raising awareness and changing university students’ lifestyles. The primary objective of this study was to ascertain the prevalence of hypertension among university students, with a secondary focus on the relationship between blood pressure levels and anthropometric parameters. Alongside conventional anthropometric measures, this study assessed body composition parameters derived from bioimpedance analysis—comprising extracellular water ratio, skeletal muscle mass, fat-free mass, and total body water—in a group of young Iranian university students.
Methods
This cross-sectional study involved 264 university students, including 130 males and 134 females, from Kashan University of Medical Sciences. Researchers measured blood pressure and anthropometric indicators and analyzed the collected data using SPSS software.
Results
28% of participants had high blood pressure, and 15.9% had hypertension. Men were five times more likely than women to have hypertension, indicating a significantly higher prevalence of the condition. Meaningful positive correlations were reported between blood pressure and fat-free mass, skeletal muscle mass, and total body water. Based on Logistic regression analysis, BMI, skeletal muscle mass, total body water, fat-free mass, and male sex were significant predictors of HTN.
Conclusion
These results imply that young individuals’ blood pressure status is highly correlated with anthropometric and body composition parameters.
Keywords
1. Introduction
Hypertension (HTN) represents a significant global public health issue, characterized by its considerable prevalence in both developed and developing nations. 1 Based on the 2017 ACC/AHA guideline, the diagnostic criterion for HTN has been reduced by 10 mmHg (from 140/90 mmHg to 130/80 mmHg), underscoring the increased significance and sensitivity associated with the issue of HTN. 2 Therefore, the contemporary definition of HTN, according to current diagnostic criteria, is defined as systolic BP ≥130 mmHg and/or diastolic BP ≥80 mmHg. 3
Iran is not an exception; a study conducted in 2021 by the World Health Organization (WHO) in collaboration with 184 countries, including Iran, estimated the global prevalence of HTN at about 1.2 billion people in general. The outcomes of this research indicate that the prevalence of HTN in Iran is projected to impact approximately 10 million individuals aged 30 and older, primarily due to unhealthy dietary patterns, physical inactivity, obesity, and population aging.4,5
Anthropometry assessment serves as a prevalent, cost-effective, and non-invasive method for evaluating overall nutritional status at both the individual and population levels. 6 Anthropometric indices encompass a range of measurements, encompassing weight, height, body mass index (BMI), waist circumference (WC), waist-to-hip ratio (WHR), body fat percentage (BFP), extracellular water ratio (ECWR), fat-free mass (FFM), body fat mass (BFM), soft lean mass (SLM), skeletal muscle mass (SMM), and total body water (TBW). 7 These measurements are progressively being utilized to assess cardiovascular risk factors related to obesity, particularly HTN.
A wide range of studies has demonstrated the clinical significance of anthropometric measurements. Numerous studies have shown that increases in these anthropometric measures are associated with higher odds of dyslipidemia, hyperglycemia, and particularly HTN [11].
Furthermore, the relationship between HTN and anthropometric measurements is prominently demonstrated in various studies. Previous research among university students has shown significant links between anthropometric indicators, such as BMI, WC, and WHR, and elevated BP levels.8,9 Also, markers related to obesity and male sex have been consistently related to elevated odds of HTN among young adults.10,11
Although numerous studies have explored the link between anthropometric measures and HTN, many have concentrated mainly on older populations or assessed only conventional indicators of obesity, such as BMI and WC. There is little data on how detailed body composition factors—like EWR, SMM, FFM, and TBW—relate to BP status among young Iranian adults. This study, therefore, sought to estimate the prevalence of HTN and to investigate its association with both standard anthropometric measures and body composition metrics derived from bioimpedance analysis in students at Kashan University of Medical Sciences. As HTN becomes more common among younger individuals, which is a trend linked to ‘Globesity,’ the global rise in overweight and obesity,12,13 this study’s focus on young adults could help identify cardiovascular risk factors earlier in populations typically seen as having a lower risk for HTN. Consequently, an effort was undertaken to assess the prevalence of HTN among students at Kashan University of Medical Sciences in 2024, and, secondarily, to determine the correlation between anthropometric indices and BP status. This information has the potential to inform the prioritization of health policy and service management, improve early screening strategies, reduce treatment costs, and mitigate the onset of this condition.
2. Materials & methods
2.1. Study design and participants
In order to ascertain the prevalence of HTN and assess its correlation with anthropometric indicators, this cross-sectional study was carried out in 2024 among students at Kashan University of Medical Sciences in Iran.
Students were randomly selected from the university’s official enrollment list using a digital lottery system, serving as the sampling frame. The draw included individuals from first to fourth year across different disciplines. Prior to the selection process, each student received a unique numerical code, and a computer-based random selection method was used to choose participants. The selection remained entirely random, with no stratification or grouping applied at any stage.
A minimum of 265 participants was required for the study. This number was determined using PASS software, based on prior research by Cheah WL et al., 14 which reported an 8.2% prevalence of HTN. The calculation assumed a 95% confidence level and allowed for a margin of error of ±0.07.
2.2. Exclusion and inclusion criteria and participants
The study included students aged 18 to 30 who were currently enrolled in the first through fourth years at Kashan University of Medical Sciences and agreed to take part. Eligible participants also needed to have a BMI ranging from 18.5 to 40 kg/m2.
Individuals were excluded if they had a BMI of 40 kg/m2 or higher, followed a specific diet, had chronic illnesses other than HTN, were taking medications that could influence body composition or blood pressure, or had missing anthropometric or BP measurements. Seven participants were removed from the study due to pre-existing health conditions, medication use, or a BMI exceeding 40 kg/m2. As a result, the final analysis was based on data from 264 individuals.
2.3. Anthropometric measurements
Anthropometric evaluations were conducted at both the Medical and Clinical Nutrition Center of Shahid Beheshti Hospital in Kashan, taking place daily between 8:00 AM and 12:00 PM, with around ten participants assessed per session.
Body composition was measured using an InBody bioelectrical impedance analyzer. Participants were instructed to remove footwear, detach socks, stand straight on the device’s platform, and hold the hand electrodes with their arms slightly away from their sides, following the manufacturer’s guidelines. Each measurement session lasted about 3 to 4 minutes.
The device recorded several metrics, including body weight, BMI, WHR, BFP, ECWR, FFM, BFM, SLM, SMM, and TBW.
To ensure accuracy, the InBody device was calibrated regularly each day before use, in accordance with the manufacturer’s instructions. All assessments were carried out under consistent environmental conditions by qualified staff.
2.4. Blood pressure assessment
BP was assessed using a calibrated digital sphygmomanometer accurate to within 1 mmHg. Before each measurement, participants were asked to sit quietly for several minutes. Readings were measured on the right arm while individuals were seated in a comfortable position.
Two readings each of SBP and DBP were recorded, spaced 3 to 5 minutes apart, and the average of these two values was utilized. When the difference between the initial readings exceeded 10 mmHg, a third measurement was taken. In such cases, the analysis relied on the average of the two closest values.
To ensure the digital device’s accuracy, manual BP measurements were conducted daily in a randomly selected 10% of participants using a standard sphygmomanometer. These manual results were then compared with the corresponding digital readings.
2.5. Physical activity assessment
Physical activity levels were evaluated using a validated questionnaire based on metabolic equivalent tasks (METs), which includes nine categories of activities ranging from sleeping or resting (0.9 METs) to intense physical exertion (>6 METs). This tool was initially created for use in European populations and has been validated by comparison with daily activity logs and CSA accelerometer measurements. 15
The Persian adaptation of the questionnaire has previously demonstrated acceptable validity and reliability in Iranian adolescents, as shown by Ziaee and Kelishadi et al., with strong correlations observed when compared to both the International Physical Activity Questionnaire (IPAQ) and one-week physical activity records. 16
3. Results
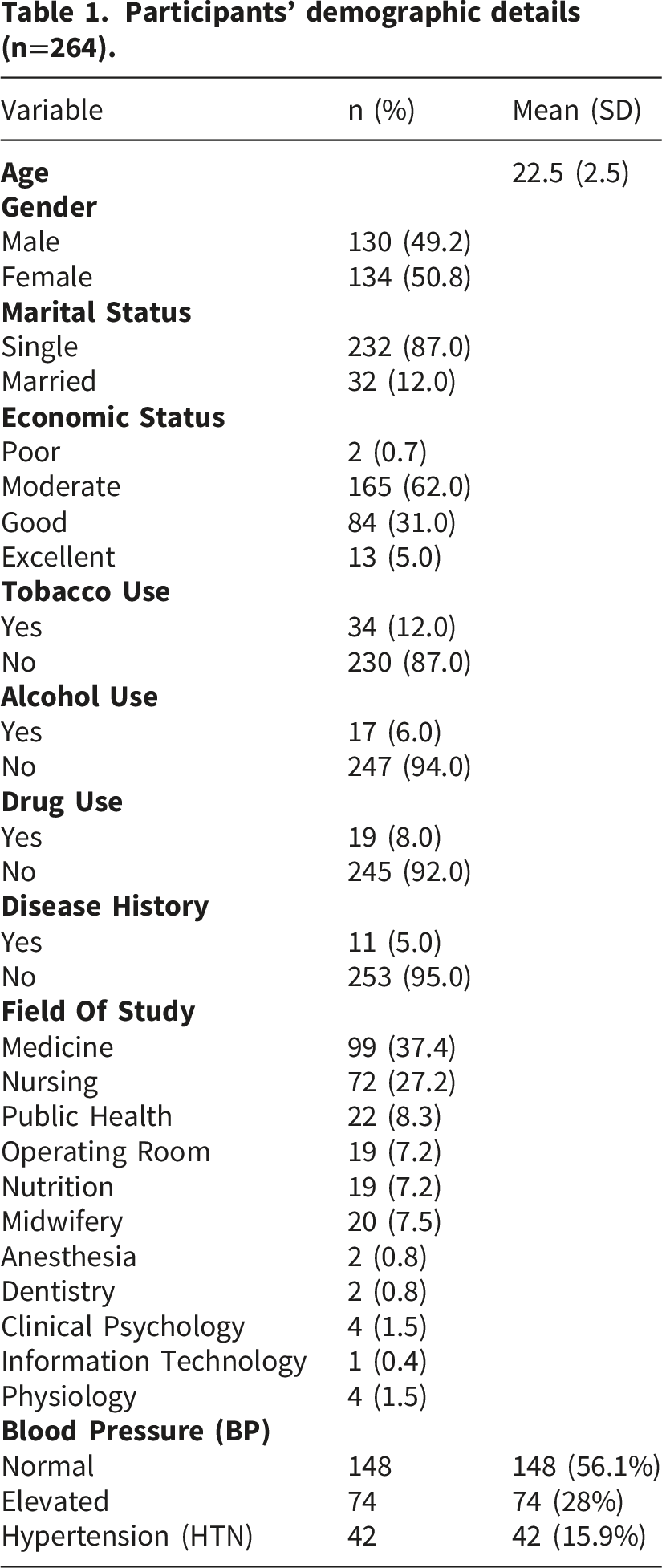
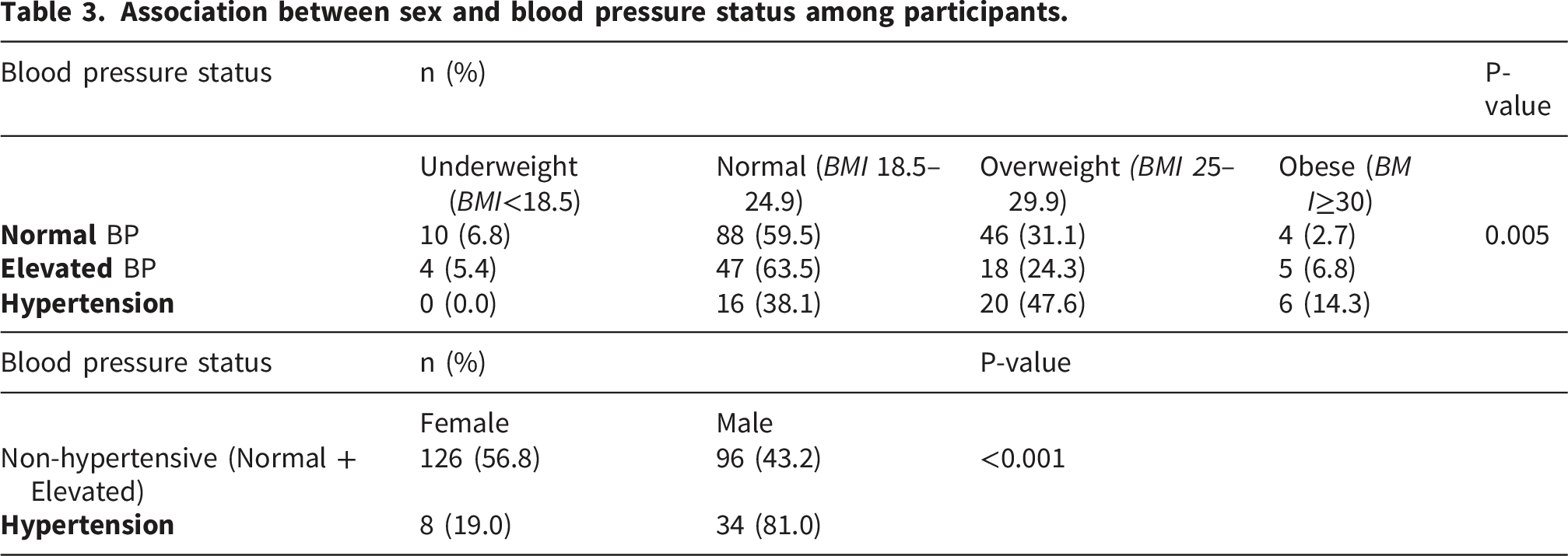
BP was also analyzed by sex. Among HTN participants, men consisted of 81%, while women accounted for 19%. In contrast, in the normal BP group, men comprised 43.2% and women 56.8%. These findings indicate a higher prevalence of HTN among male individuals, and the relationship between sex and BP status was determined to be substantially meaningful (p<0.001).
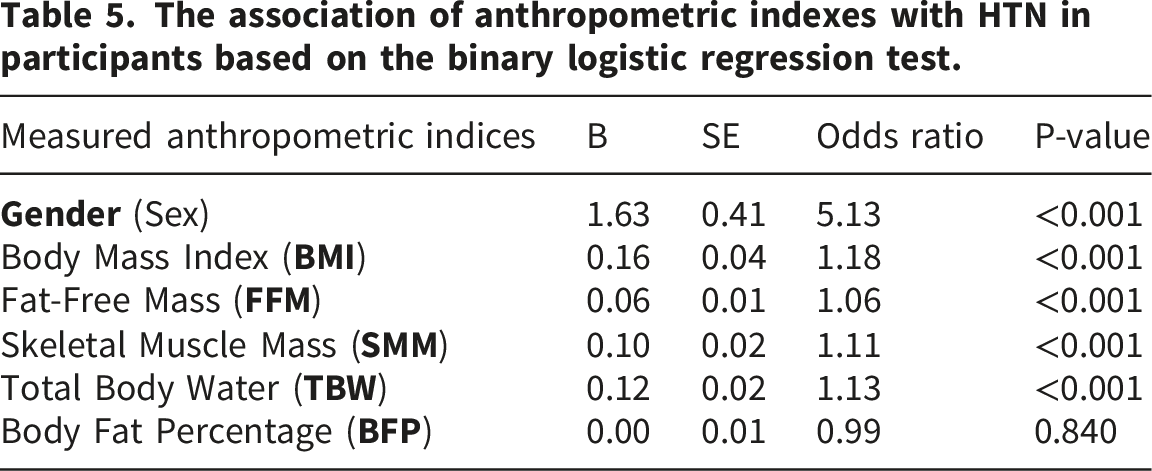
Of all the variables evaluated, FFM showed the minimum link to HTN, where every one-unit rise in FFM was associated with a 6% elevation in the odds of HTN (OR = 1.06, p < 0.001).
Additionally, men demonstrated approximately fivefold (5.13) higher odds of HTN compared with women, according to a substantial gender association with the condition (B = 1.63, OR = 5.13, p<0.001).
4. Discussion
This study not only expands on existing research by analyzing conventional anthropometric indicators, encompassing BMI, WC, and WHR, but also comprises comprehensive body composition measures obtained through bioimpedance, including ECWR, SMM, FFM, and TBW, in connection with BP levels among young Iranian adults. While previous studies in university settings have primarily focused on standard markers of obesity, our findings suggest that additional aspects of body composition may also be associated with BP status and HTN occurrence.
Moreover, the high prevalence of elevated BP observed in this young population highlights a growing concern regarding early cardiometabolic abnormalities among university students.
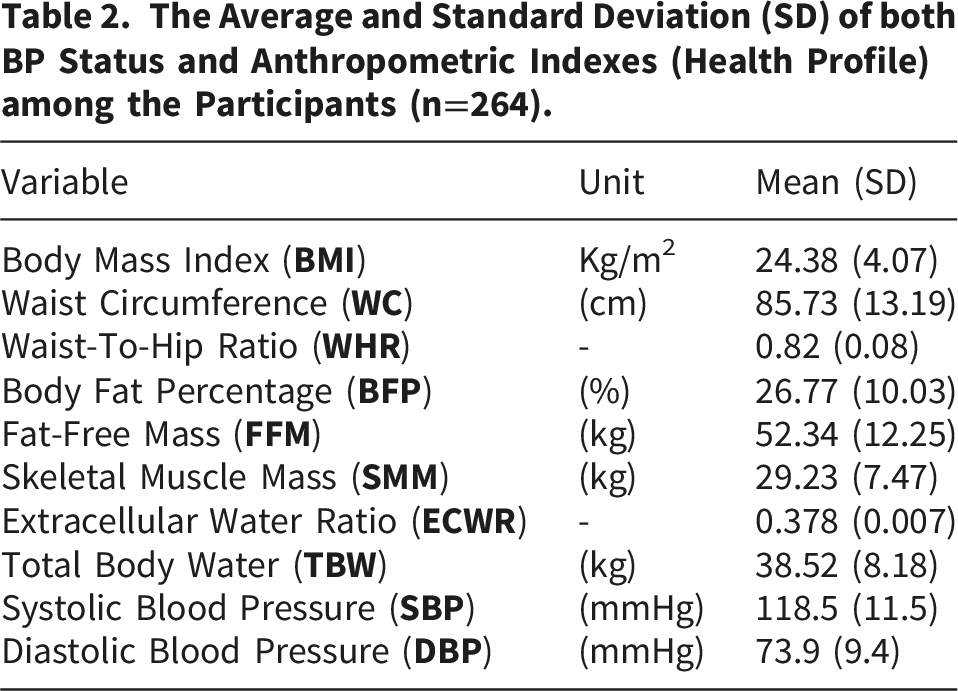
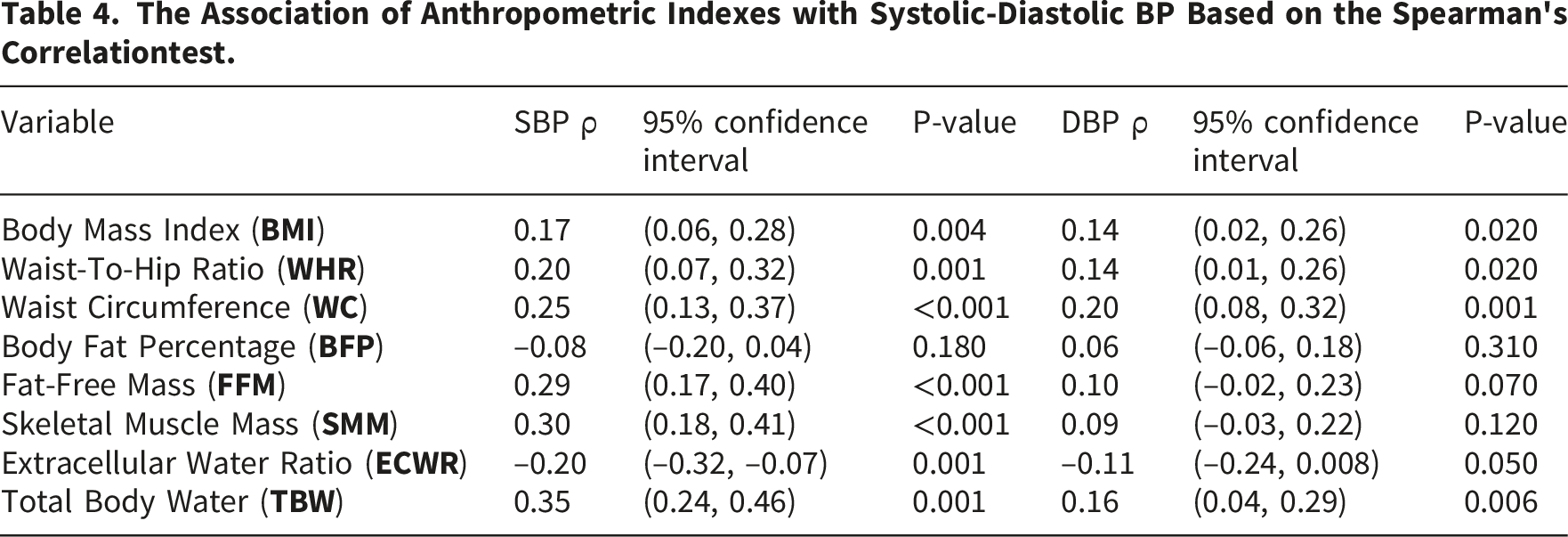
This study, which included 264 participants, found significant positive links between BMI, WC, WHR, FFM, SMM, and TBW with SBP, and between BMI, WC, WHR, and TBW with DBP; FFM and SMM were not significantly associated with DBP. In contrast, the ECWR was inversely related to BP, while BFP showed no significant association. These outcomes indicate that measures of overall body composition and abdominal obesity (WC and WHR) might have a stronger link to BP status in young adults than total BFP by itself. Higher levels of overall and lean mass metrics, along with being male, were significantly linked to increased odds of HTN when considering the evaluation of the logistic regression.
In different countries, prior research has indicated that the prevalence of HTN among students exhibits significant variation.
A study conducted in 2014 by Ibrahim NK et al. indicated that the prevalence of HTN in among medical students at King Abdulaziz University in Saudi Arabia was approximately 5 to 7%. 17 Besides, Baig M and colleagues reported that approximately one-tenth (9.3%) of medical students in Jeddah were diagnosed with HTN; 3.7% exhibited elevated SBP, and 7.9% showed elevated DBP. 18 Additionally, a 2016 study by Cheah WL et al., involving 218 pre-university students, indicated a prevalence of HTN at risk of 7.3% among pre-university students, with a notably higher incidence among males, recorded at 16.7%. Approximately 22% of the participants in the study were categorized as overweight or obese. A significant proportion of males exhibited a standard WC (75.9%), whereas nearly half of the females were classified within the unhealthy category for WC (47.0%). 9 Recent cohort studies have examined cardiometabolic health markers among university students in the United Kingdom. In 2025, Savage MJ et al. conducted a survey involving 1,299 students, revealing that 12.7% were classified as hypertensive. Additionally, the findings indicated that 34.5% of the participants were categorized as having overweight or obesity, 7.6% exhibited a ‘very high’ WC, 11.0% had a high WHR, and 25.5% presented with a high waist-to-height ratio (WHtR). 19 Furthermore, a separate study was performed involving 1719 college students in China. The findings indicated an overall prevalence of HTN of 10.59%. Male students exhibited a significantly higher occurrence of HTN at 10.24%, as well as an abnormal pulse pressure rate of 8.13%, in comparison to their female counterparts. Ultimately, the multivariable analysis revealed a significant relationship between HTN and both neck circumference (NC) and BMI, while no significant correlations were observed with the other assessed parameters. 20
The results of this study largely align with earlier international research,17–20 showing consistent associations between obesity-related anthropometric measurements and higher BP in young adults. Still, differences in reported rates of HTN across studies could stem from variations in factors such as ethnicity, lifestyle, diet, physical activity, sample composition, and the specific criteria used to define HTN.
Recently, two cross-sectional surveys were performed among children and adolescents. In their analysis of a Lithuanian sample, Stankute et al. (2024) found that WC, NC, and mid-upper arm circumference were all meaningfully correlated with HTN. 21 Similarly, Vaquero-Álvarez et al. (2020) conducted an assessment of Spanish children and adolescents, ultimately highlighting that among anthropometric variables for the detection of HTN, WC showed among the highest diagnostic accuracy for detecting hypertension among other variables. Both surveys emphasize the prospective advantages of body measurements for the timely diagnosis of cardiovascular risk, particularly HTN, among youth populations. 22
A study conducted on 622 university students in Jordan revealed varying results. The findings revealed an obesity prevalence of 15.4%, with 27.7% of participants diagnosed with pre-hypertension in the study population. 23 A study carried out by El-Ashker S and colleagues involving 284 male university students in Saudi Arabia revealed a high prevalence of elevated blood pressure, alongside rates of overweight and obesity at 16.5% and 34.9%, respectively. 24
The prevalence of HTN found in this study is comparable to that reported in some previous studies,21–24 likely due to variations in population traits, gender composition, lifestyle habits, and rates of obesity among university students across different regions.
Similarly, a limited number of studies with varying outcomes have been undertaken in Iran regarding the prevalence of HTN among students. A cross-sectional study conducted in 2004 utilized data from 3,931 students at Tehran University to examine the connection between obesity and HTN. The findings revealed that the prevalence of overweight and obesity was 13.5% and 3.2%, respectively. Of the participants, 63.9% exhibited a normal BMI, while 19.4% were classified as underweight. The link between BMI and HTN was found to be statistically significant. 25 Another study, conducted by Tabrizi et al. in 2016, aimed to assess the predictive capabilities of obesity indices, physical activity, and cardiovascular health on the development of cardiovascular disease among a cohort of 223 students at Sharif University of Technology. WC exhibited a significant positive correlation with SBP in females. 10 A distinct investigation conducted in 2015, involving 300 individuals excluding students, examined anthropometric indices and their association with coronary artery disease (CAD). This study, led by Arjmand G et al., demonstrated a strong and promising link between SBP and DBP with BMI in both populations with and without CAD. Furthermore, the correlation between DBP and BMI was found to be more pronounced. Moreover, the association between SBP and DBP with WHR was demonstrated to be significant; however, the relationship with BFP was found to be insignificant. 11
The results of this study largely align with previous findings,10,11,25 especially in confirming strong links between BMI, WC, and WHR and BP measures. At the same time, they reinforce the weaker association seen between BFP and outcomes related to HTN.
Notably, in this study, BFP showed no significant link to either SBP or DBP. One potential reason is that overall body fat levels may not adequately capture how fat is distributed, especially visceral fat, which is more strongly tied to HTN and metabolic issues. In comparison, measures like WC and WHR might more accurately reflect central fat accumulation, a pattern more directly associated with vascular problems and higher BP. Additionally, their young age could mean that the long-term health effects often tied to increased body fat have not yet emerged.
A further key finding of this study was the inverse link between ECWR and SBP. While the exact physiological basis for this connection is still uncertain, it could be related to variations in hydration levels, fluid distribution, and overall body composition in young adults. ECWR, measured via bioelectrical impedance analysis, may reflect unique physiological traits that differ from standard measures of body fat. Additionally, individuals with more favorable metabolic profiles and lower BP might have better-regulated extracellular fluid balance. However, given the current lack of consistent and comprehensive evidence regarding ECWR and HTN, further mechanistic studies from a long-term point of view are necessary to gain a clearer understanding of their connection.
5. Conclusion
This study aims to investigate the onset of HTN and its relationship with various anthropometric indices within a cohort of Iranian university students, considering the impact of Iran’s aging population, dietary habits characterized by high fat and salt intake, the emergence of obesity, and the adoption of unhealthy lifestyle practices on HTN.
The findings revealed a significant prevalence of elevated BP and HTN among students at Kashan University of Medical Sciences, with notable correlations identified between HTN and various indices, including BMI, WC, WHR, FFM, SMM, and TBW. More importantly, the outcomes of this study proposed that a substantial majority of individuals diagnosed with HTN present with a balanced BMI, whereas a noteworthy fraction is categorized as overweight. A notable correlation was identified between WC and WHR, with SBP and DBP. The male gender constitutes a remarkable risk factor for HTN. The associations highlight the importance of anthropometric measurements in early identification of individuals at risk, including those in younger populations typically considered low-risk.
Considering the accumulation of data on Gobesity and metabolic disorders within youth and university demographics, subsequent research endeavors should focus on establishing causal relationships and assessing the longitudinal predictive validity of these anthropometric indices. Furthermore, RCTs evaluating lifestyle modifications, dietary changes, and physical activity should be prioritized to identify effective strategies for the prevention of HTN within university populations.
5.1. Strengths and weaknesses
This cross-sectional study is distinguished by its comprehensive analysis of both traditional and advanced anthropometric indicators, with a specific focus on university students within a Middle Eastern context. However, it has several limitations. The cross-sectional nature of the design restricts the ability to determine causal links between anthropometric indicators and HTN, meaning the observed associations should be interpreted with caution. Additionally, the single-center approach may affect how widely the results can be applied to other groups. To build on these findings, future research should include larger samples, multiple centers, and a wider range of age groups. Moreover, it is imperative to take into account the sex-specific differences when analyzing the association between anthropometric indices and BP status.
Footnotes
Ethical considerations
This study was carried out under the Declaration of the Research Center for Biochemistry and Nutrition in Metabolic Diseases, Kashan University of Medical Sciences. It was approved by the Institutional Review Board of Shahid Beheshti Hospital on February 4th, 2024. The study has been registered with the Shahid Beheshti Hospital Medicine School trials registry, and
Author contributions
A.A. designed the research and prepared the first draft of the manuscript, and the original writing, review, and editing of the final draft. K.A.K. contributed to the investigation and supplied resources for the study’s second draft. A.Y. contributed to the manuscript’s statistical analyses and processing of SPSS data. S.J. conceptualized the study, oversaw its development, and assisted with the review and language editing of the manuscript. All authors reviewed and approved the final version of the manuscript for publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors attest to having obtained all required patient permission documents. Although full anonymity cannot be ensured, the patient agrees that his name and initials will be kept private and unpublished and that every effort will be taken to preserve his identity.
Data Availability Statement
Upon reasonable request, the corresponding author will provide the data supporting the study’s results and statistics.