
Abstract
Background
The global rise in cesarean section (CS) deliveries has raised concerns, particularly when performed without medical indications. This study aimed to estimate the prevalence of CS deliveries in both public and private healthcare facilities in Bangladesh and to explore reported non-medical correlates of CS delivery and self-reported postoperative maternal complications.
Methods
A population-based cross-sectional study was conducted between January and December 2023 across urban and rural areas of three major administrative divisions in Bangladesh. Participants were selected from a community-based multistage sampling approach based on birth registration records, and face-to-face interviews were conducted with 4,614 mothers who had given birth during the study period. Data on delivery mode, self-reported medical indications, patient preferences, healthcare provider behavior, and post-cesarean outcomes were collected and analyzed descriptively.
Results
Among all births, 61.51% were delivered via CS, with a markedly higher rate observed in private healthcare facilities (81.45%) than in public hospitals. Approximately 21.57% of respondents reported that CS delivery was performed due to previously identified medical indications, based on maternal report and available institutional information (where feasible). A considerable proportion (38.93%) of women who underwent CS births reported postoperative complications, including postoperative pain (23.02%), postpartum hemorrhage (10.85%), surgical site infections (3.63%), and venous thromboembolism (1.43%).
Conclusion
The findings reveal an alarmingly high rate of CS deliveries in Bangladesh, particularly within private healthcare settings, with many participants reporting limited or unclear medical explanations for CS delivery. The high frequency of self-reported postoperative complications suggests important maternal health concerns. Strengthening monitoring of CS practices, improving patient-provider communication, and enhancing public awareness may help optimize CS utilization and maternal healthcare outcomes in Bangladesh.
Introduction
Over the past decade, the global incidence of cesarean section (CS) deliveries has risen sharply, often without corresponding improvements in maternal or perinatal health outcomes. While CS can be a lifesaving intervention when medically indicated, unnecessary procedures are associated with up to three times increased risks of maternal morbidity and mortality than those associated with normal vaginal delivery (NVD).1–3 Additional complications linked to CS include surgical injury, neonatal respiratory distress, and reduced maternal fertility. 2 Consequently, the International Federation of Gynecology and Obstetrics (FIGO) recommends that CS be performed only when clinically justified. 4
Previous studies have suggested that physician practice patterns, institutional characteristics, and maternal preferences may be associated with increased CS delivery rates5,6; however, these relationships are complex and may vary across healthcare settings. A World Health Organization (WHO) survey across 24 countries found that nearly one-third of CS deliveries occurred without medical indication, increasing the risk of adverse outcomes.1,7 This pattern, once concentrated in middle- and high-income countries, is now a growing public health concern in low- and middle-income nations. For example, a study in Brazil reported that 84% of CS deliveries occurred before the onset of labor, most without emergency need. 8 Overuse of CS not only threatens maternal and neonatal health but also increases healthcare costs and diverts resources away from essential care in under-resourced systems.9,10
In Bangladesh, CS has become the most frequently performed surgical procedure, showing steep and uneven growth across socioeconomic groups. Affluent, urban, and educated women are disproportionately more likely to undergo CS. 11 National survey data show that CS deliveries rose from 3% in 2000 to 24% in 2014. 12 The rate in institutional settings increased from 33% in 2000 to 63% in 2014, with private hospitals reporting up to 77% of births by CS.12,13 Previous studies indicate that a significant share of these procedures lacked medical justification. 14 Although often perceived as safer, CS carries substantial risks, including infection, hemorrhage, venous thromboembolism, and delayed recovery.15,16
The persistently high and increasing CS rate in Bangladesh substantially exceeds WHO’s recommended threshold of 10–15%,12,13 warrants urgent attention. Although the WHO has historically suggested that CS rates above this level may not lead to further reductions in maternal or neonatal mortality, the relevance of this benchmark may vary across healthcare settings and population risk profiles. The present study, therefore, aimed to (i) estimate the prevalence of CS delivery in government and private healthcare facilities across selected regions, (ii) explore reported non-medical correlates, (iii) assess self-reported post-cesarean complications, and (iv) examine the employment patterns of gynecologists that may influence delivery decisions. The findings are expected to inform evidence-based policies to reduce unnecessary CS and improve maternal health outcomes.
Design and methods
Study areas
This population-based study was conducted across three administrative divisions of Bangladesh (Dhaka, Chittagong, and Rajshahi), encompassing both urban and rural settings [Supp. Figure 1]. These divisions represent distinct geographic, demographic, and socioeconomic characteristics, providing a comprehensive overview of the national context. Dhaka, the capital and most densely populated region, is centrally located and serves as the country’s primary administrative and commercial hub. 17 Chittagong, situated along the southeastern coast, is the largest division by area and includes Bangladesh’s principal seaport, contributing significantly to national trade. Rajshahi, located in the northwestern region, is comparatively less urbanized and characterized by higher levels of poverty, malnutrition, and limited access to healthcare services. 18 By including these three diverse divisions, the study aimed to capture representative insights into the prevailing patterns of birth delivery practices across varied socioeconomic and geographic landscapes in Bangladesh. Although the selected divisions represent geographically and socioeconomically diverse regions of Bangladesh, the study did not include all administrative divisions of the country. Therefore, the findings should not be interpreted as fully nationally representative.
Study design
A population-based cross-sectional study was conducted between January and December 2023 across urban and rural areas of three major administrative divisions in Bangladesh. The study was designed to provide population-level evidence from selected representative regions rather than a complete nationwide assessment. Participants were selected from government birth registration records obtained from ward offices in urban areas and union offices in rural areas across the selected divisions. Birth registration lists maintained by local administrative authorities were used to construct the sampling frame. These records were reviewed to identify mothers who had delivered within the study period and met the inclusion criteria. The study included mothers who had delivered their newborns either in healthcare facilities (NVD or CS) or at home (NVD) with the assistance of traditional birth attendants. When an eligible participant could not be contacted after repeated visits or declined participation, the next eligible participant from the same geographic area and registration list was approached to minimize data loss. To capture institutional factors influencing delivery practices, additional interviews were conducted with healthcare providers, including gynecologists and obstetricians, focusing on their employment patterns across single or multiple healthcare facilities and how these may affect delivery mode decisions.
Sample size
The number of study population required to be interviewed was estimated through a standard formula
19
This commonly used formula, known as Cochran’s formula, is used for sampling, where n denotes the minimum sample size required to estimate the population proportion (p) with a specific level of confidence (Z) and precision (E).
A total of 4,614 mothers were interviewed across the three study divisions: 1,824 from Dhaka, 1,323 from Chittagong, and 1,467 from Rajshahi. The calculated non-response rates were 20.63% (474 of 2,298) in Dhaka, 17.47% (280 of 1,603) in Chittagong, and 19.57% (357 of 1,824) in Rajshahi. Partially completed questionnaires were excluded from the final analysis and treated as non-responses. In addition to the maternal participants, a total of 273 healthcare providers were interviewed to assess factors potentially influencing delivery decisions. These included 122 providers from Dhaka (44.69%), 69 from Chittagong (25.27%), and 82 from Rajshahi (30.04%).
Data collection
Around 60% of the total population is concentrated in the Dhaka, Chattogram, and Rajshahi Divisions of Bangladesh, 20 which may reflect the national representation. Data were collected through face-to-face interviews conducted between January and December 2023 using a structured questionnaire. The instrument was initially developed based on the framework of the Bangladesh Demographic and Health Survey 2014. 21 A pilot study was conducted with 18 mothers (six from each study division) to evaluate the clarity and relevance of the preliminary questionnaire. Based on feedback from the pilot phase, the questionnaire was revised and subsequently submitted to the institutional review board for ethical approval. Recommendations from board members were incorporated into the final version of the questionnaire used for the main survey. For fieldwork, a team of 20 trained interviewers and 3 coordinators was deployed. All personnel underwent a five-day training program, which included two days of practical sessions focused on effective interviewing techniques, probing methods, and strategies to ensure complete and accurate data collection. Data entry was performed concurrently with data collection to streamline processing and ensure quality control. Information regarding the indication for cesarean delivery was obtained primarily through maternal self-report. Where applicable, collected data were cross-validated. Cross-validation was performed opportunistically for a subset of participants when hospital admission records, operating theater records, or discharge summaries were available at the time of data collection. The cross-validation process was primarily intended to improve consistency of delivery-related information rather than provide comprehensive clinical validation of all reported variables. The validation audit showed a concordance rate of more than 95%. Although approximately 4% discrepancies were identified, they did not affect the overall study conclusions. Reported postoperative complications of this study were primarily based on maternal self-report, and comprehensive clinical validation was not feasible for all participants.
A separate, specialized questionnaire was developed for healthcare providers, including gynecologists and obstetricians. This instrument underwent the same pilot testing and ethical review procedures. Healthcare providers were randomly selected from institutional rosters, with a focus on those directly involved in overseeing childbirth during the study period.
Covariates
The primary objective of this study was to estimate the current rates of NVD and CS deliveries across government and private healthcare facilities in Bangladesh. To descriptively explore potential factors associated with the mode of delivery, several covariates were included in the analysis. These included: (1) the number of children per household, (2) the educational attainment of the household head, (3) the educational level of the mother, and (4) the employment behavior of gynecologists, specifically whether they were employed in single or multiple healthcare institutions. These variables were selected based on prior evidence suggesting their influence on healthcare-seeking behavior, delivery preferences, and institutional practices.
Statistical analysis
All data were entered, processed, and analyzed using the Statistical Package for the Social Sciences (SPSS), version 14.0. Descriptive statistics were employed to summarize the present the study findings. Frequencies and percentages were calculated to describe categorical variables, including delivery modes, reasons for CS, post-operative complications, and provider employment patterns. Data were stratified by division and type of healthcare facility (government vs. private) to enable comparative analysis across geographic and institutional contexts. Binary logistic regression analysis was performed to examine associations between selected variables and CS delivery status. Variables included in the adjusted model were maternal age, residential area, educational qualification, maternal occupation, and type of healthcare facility. Adjusted odds ratios (AORs) with 95% confidence intervals (CIs) were reported. Because of the cross-sectional study design and limited availability of several clinical confounders, the regression findings should be interpreted as exploratory associations rather than causal determinants.
Results
Birth delivery locations
Birth delivery rate in home, government, and non-government hospitals/clinics.
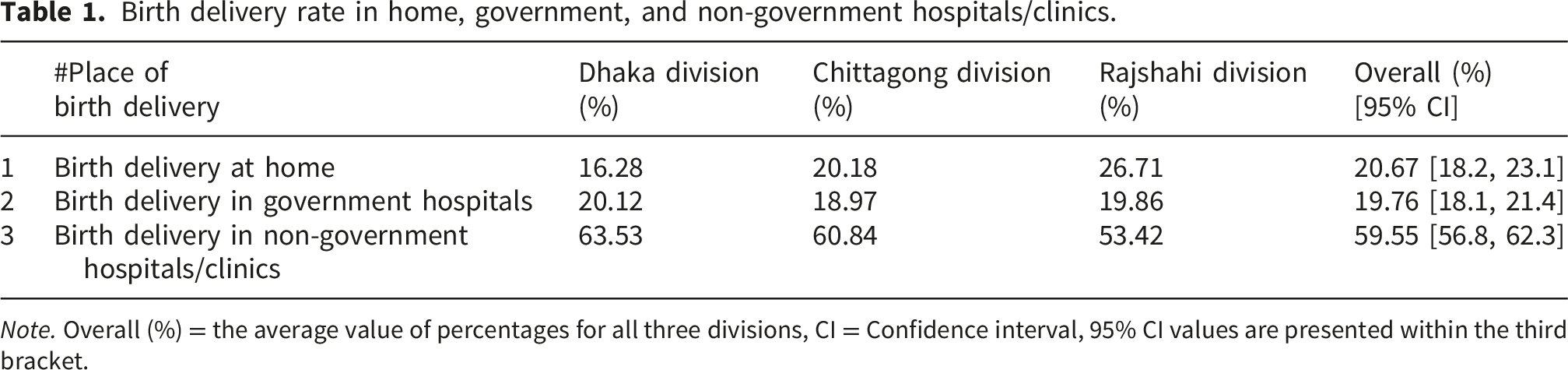
Note. Overall (%) = the average value of percentages for all three divisions, CI = Confidence interval, 95% CI values are presented within the third bracket.
Estimation of current cesarean delivery rate in study areas
The CS delivery rate was markedly high across all three divisions. Prevalence was nearly similar in Dhaka (67.21%) and Chittagong (64.63%) but lower in Rajshahi (52.69%), with an overall rate of 61.51% [Figure 1(a)]. By facility type, CS deliveries in government hospitals were high, around 66.57% in Dhaka, 65.87% in Chittagong, and 59.58% in Rajshahi [Figure 1(b)]. In contrast, private facilities reported alarmingly higher rates; 83.25% in Dhaka, 79.87% in Chittagong, and 81.24% in Rajshahi. These findings demonstrate a stark public–private disparity, with consistently higher CS intervention rates in private hospitals. Distribution of cesarean section deliveries across healthcare facilities. (a) NVD versus CS birth delivery rates in Dhaka, Chittagong, and Rajshahi divisions in Bangladesh. (b) Comparison of CS delivery rates between government and non-government health facilities. ***p ≤ 0.005; *p ≤ 0.05.
Participant-reported circumstances and perceived reasons associated with cesarean section delivery.
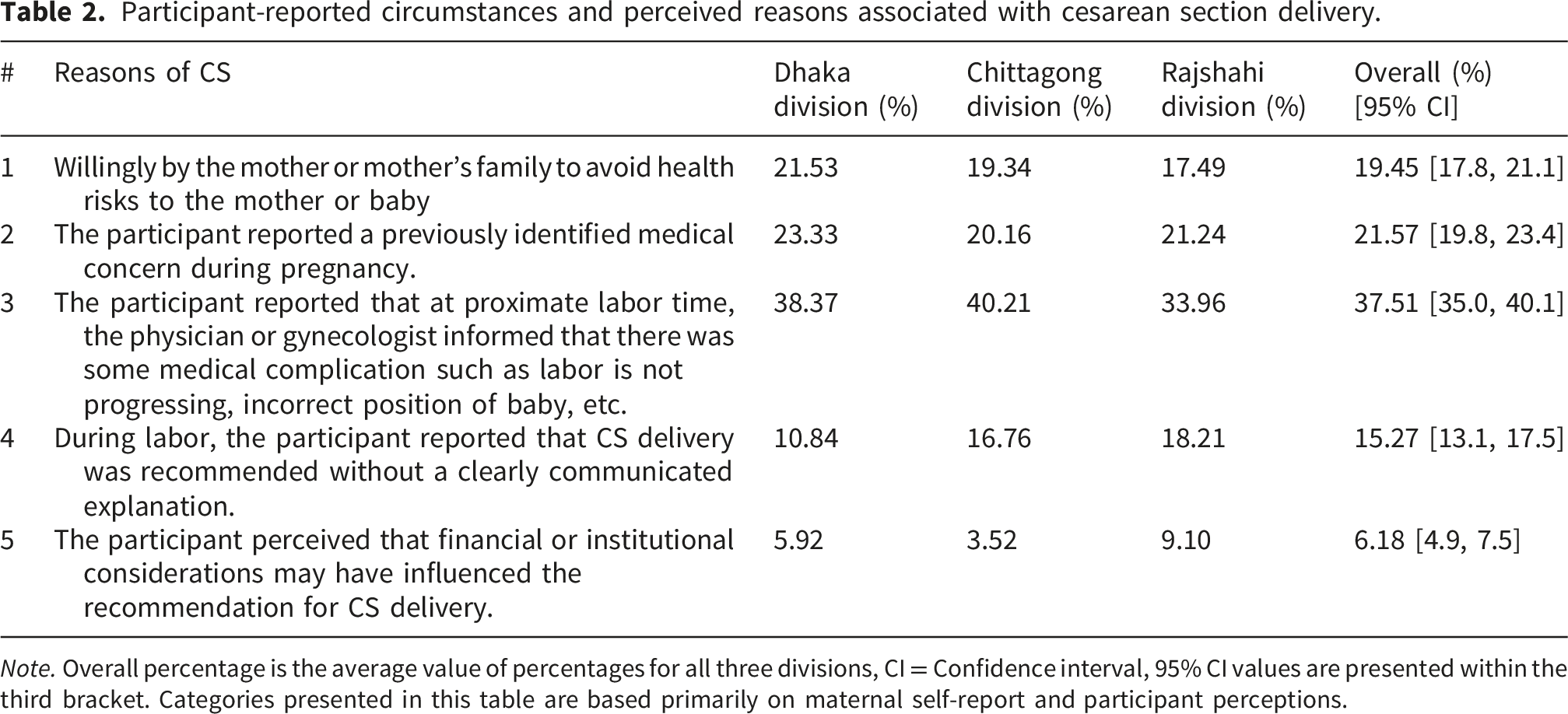
Note. Overall percentage is the average value of percentages for all three divisions, CI = Confidence interval, 95% CI values are presented within the third bracket. Categories presented in this table are based primarily on maternal self-report and participant perceptions.
The working behavior of gynecologists
The analysis revealed that a substantial proportion of gynecologists were employed simultaneously in multiple healthcare facilities. Specifically, 33.98% of gynecologists reported working at two institutions, 43.87% at three, and 8.36% at four. Only 13.52% of gynecologists were exclusively employed in a single healthcare facility [Supp. Table 1]. In the context of Bangladesh, it is common for a gynecologist to hold a full-time position at one hospital or clinic while working part-time at additional institutions. The coexistence of multiple institutional employment patterns and high CS prevalence observed in the study may reflect broader organizational or healthcare system characteristics; however, the present data do not permit conclusions regarding whether these employment arrangements directly influence clinical decision-making.
Furthermore, the majority of gynecologists (84.43%) were employed full-time in government healthcare facilities. In contrast, only 15.56% of gynecologists were employed in full-time positions in non-government (private) facilities, with the highest proportion observed in Dhaka (18.03%) and the lowest in Chittagong (11.59%) [Supp. Table 1]. These employment patterns may partially explain the high CS rates in private facilities, as many gynecologists who work part-time in these settings may prefer scheduled deliveries that align with their availability across institutions.
Post-operative complications experienced by mothers after CS delivery
Self-reported postoperative complications following cesarean section delivery.
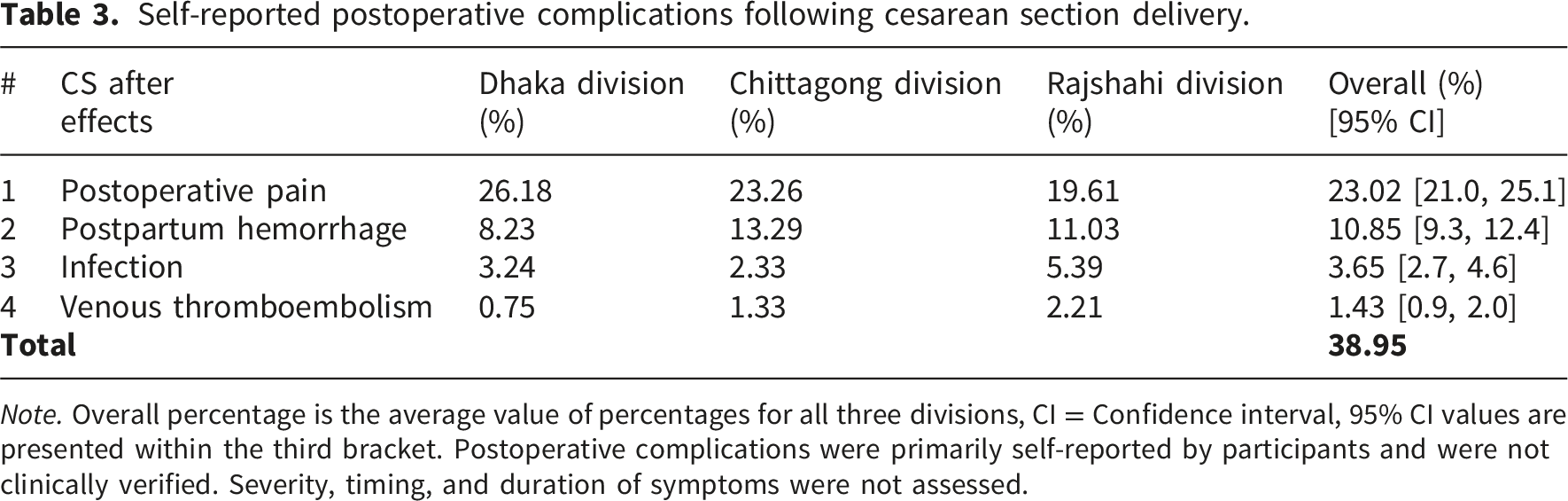
Note. Overall percentage is the average value of percentages for all three divisions, CI = Confidence interval, 95% CI values are presented within the third bracket. Postoperative complications were primarily self-reported by participants and were not clinically verified. Severity, timing, and duration of symptoms were not assessed.
Factors associated with cesarean section delivery
Binary logistic regression analysis of factors associated with cesarean section delivery in the study population.
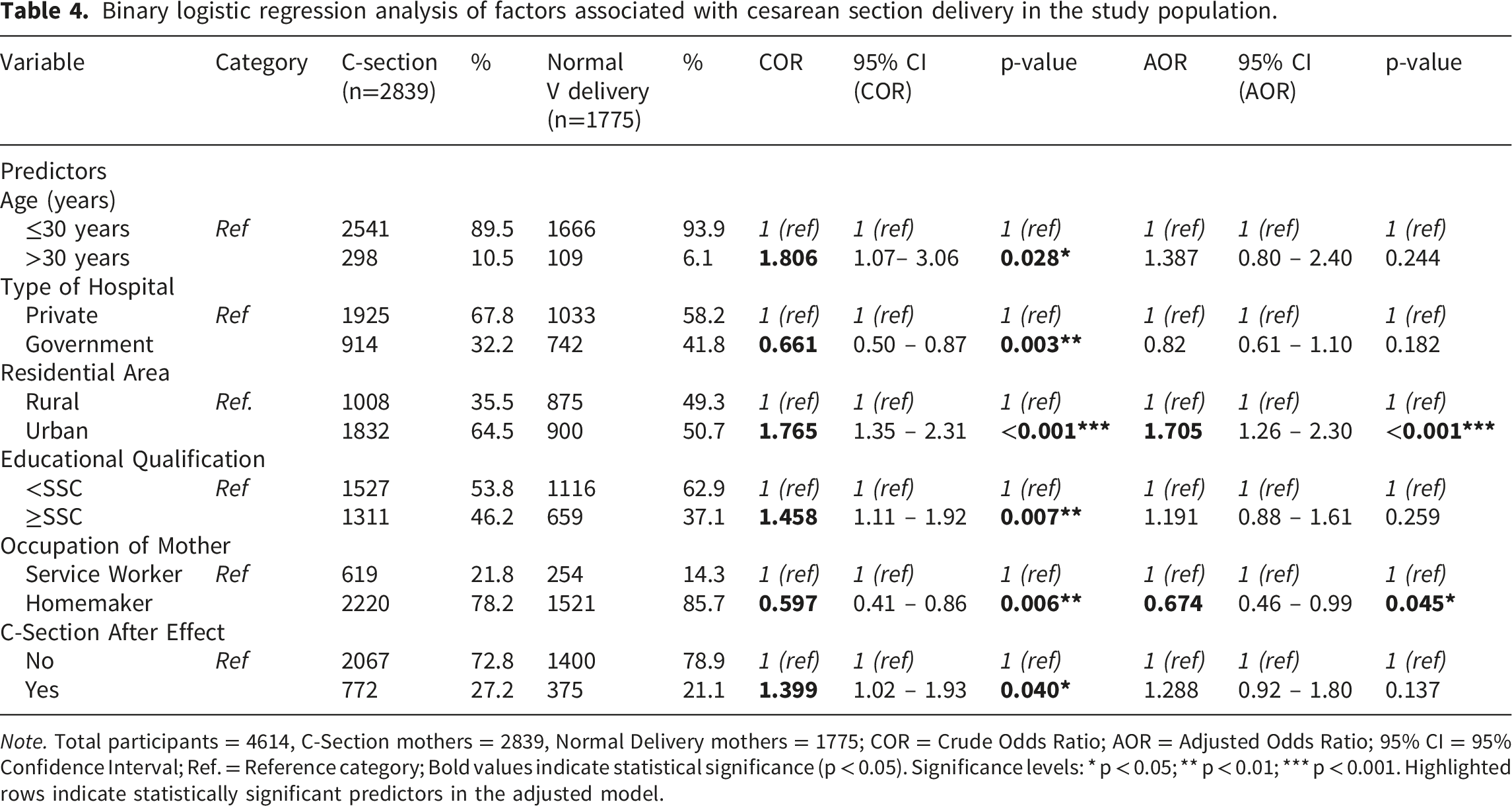
Note. Total participants = 4614, C-Section mothers = 2839, Normal Delivery mothers = 1775; COR = Crude Odds Ratio; AOR = Adjusted Odds Ratio; 95% CI = 95% Confidence Interval; Ref. = Reference category; Bold values indicate statistical significance (p < 0.05). Significance levels: * p < 0.05; ** p < 0.01; *** p < 0.001. Highlighted rows indicate statistically significant predictors in the adjusted model.
Several factors demonstrated significant crude associations that were attenuated following multivariable adjustment. Advanced maternal age (>30 years) was associated with higher odds of CS in the unadjusted analysis (COR = 1.81; 95% CI: 1.07–3.06; p = 0.028), but this effect became non-significant after controlling for confounders (AOR = 1.39; 95% CI: 0.80–2.40; p = 0.244). Birth delivery at government hospitals appeared to have a protective association in the crude analysis (COR = 0.66; 95% CI: 0.50–0.87; p = 0.003); however, the adjusted odds ratio did not reach statistical significance (AOR = 0.82; 95% CI: 0.61–1.10; p = 0.182), indicating potential confounding by other factors. Higher educational attainment (≥SSC) followed a similar pattern, demonstrated significantly higher crude odds of cesarean delivery (COR = 1.46; 95% CI: 1.11–1.92; p = 0.007), although this association was attenuated in the adjusted model (AOR = 1.19; 95% CI: 0.88–1.61; p = 0.259). On the other hand, post-cesarean complications were more frequently observed among mothers who underwent cesarean delivery, the adjusted association did not reach statistical significance (AOR = 1.288; 95% CI: 0.92–1.80; p = 0.137), despite a significant crude association (COR = 1.399; 95% CI: 1.02–1.93; p = 0.040)
Discussion
Our study found a high CS delivery rate of 61.51% across three major divisions in Bangladesh, nearly four times higher than the WHO’s recommended limit of 15%. 13 As Dhaka, Chittagong, and Rajshahi divisions are densely populated areas in Bangladesh [Supp. Figure 1], the high CS delivery rate identified in this study represents a sharp rise, and a growing public health concern. Historically, most births occurred at home; in 2007, 85% of child deliveries were performed in home assisted by traditional birth attendants, and the remaining 15% institutional deliveries assisted by skilled professionals. 22 By 2013, 42% were assisted by skilled professionals, 23 and in the present study, institutional deliveries rose to 78%. While institutional births generally improve outcomes, they have also contributed to the rapid increase in CS.
Private facilities dominate institutional childbirth services in Bangladesh. In our data, 59.55% of institutional deliveries were in private hospitals, where the CS rate was 81.45%. Similarly high CS rates in private healthcare facilities have been consistently reported in other divisions of Bangladesh and in several other countries. For example, the CS delivery rate in the private healthcare sector was also reported to be 82% in Bangladesh’s Sylhet division and 80% in Brazil.24,25 Previous studies have suggested that physician practice patterns, financial incentives, maternal preferences, the financial capacity of families, and the availability of advanced facilities may contribute to higher CS rates in private healthcare settings.5,6,26 Although our data, based on maternal self-reports, also indicated these potential contributing factors, we were unable to identify the exact reasons underlying this difference within our study population. Only 21.57% of CS procedures in our study were maternal self-reported medically indicated, while an additional 19.45% were performed at maternal request, often under the perception that CS is safer or less painful. 27 Approximately 15.27% of participants reported that CS delivery was recommended without a clearly communicated explanation, raising concerns about patient-provider communication and informed decision making. Many gynecologists are employed at multiple facilities: 43.87% worked at three, and 33.98% at two institutions. Although most were full-time employees in government hospitals, the majority of deliveries occurred in private facilities. Vaginal deliveries are unpredictable in timing, often prolonged, and may require active labor management with oxytocin and continuous monitoring, 28 while CS can be scheduled, making it more convenient for physicians managing multiple jobs. This employment structure may be associated with a greater preference for scheduled procedures such as CS delivery; however, the present study cannot establish whether these employment patterns directly influence physician decision-making.
NVD is often painful but usually followed by faster recovery and earlier return to daily activities. In contrast, CS is initially painless under anesthesia but frequently results in more persistent postoperative pain. 29 In our study, this was the most common complication, affecting 23.02% of CS mothers. Although duration was not assessed, a Finnish study reported persistent pain in 22% of mothers one year after CS, suggesting potential long-term morbidity.9,30 Postpartum hemorrhage was reported by 10.85% of mothers, notably higher than the global average of 6% for all births, 31 reflecting the greater risk associated with CS. Infection rates were also consistent with the global incidence of post-cesarean wound infection (3–15%). 32 In our data, Rajshahi recorded highest, around 5.39%, equivalent to emergency CS cases abroad. For example, Haukeland University Hospital reported a 5.4% infection rate following emergency CS and 0.4% for elective procedures. 33 In contrast, mothers in Dhaka and Chittagong divisions experienced significantly lower rates of post-cesarean infections, nearly half of those observed in Rajshahi. Participants reported venous thromboembolism was less frequently; however, it was more common in Rajshahi (2.21%) than in other divisions. All postoperative complications were self-reported by mothers rather than systematically evaluated clinically. Although limited cross-validation with hospital records was performed where feasible, comprehensive clinical confirmation was not possible for all cases. Moreover, the present study assessed the occurrence of postoperative complications but did not evaluate their clinical severity, duration, or precise timing after delivery. Therefore, the findings should be interpreted as indicative of self-reported complications rather than detailed clinical outcomes. These higher rates of infection and thromboembolism may be linked to socioeconomic disadvantages such as poverty, poor nutrition, and limited healthcare access. 18 Overall, postoperative pain was the most consistent complication associated with CS across regions, while hemorrhage, infection, and thromboembolism showed regional variation. Although some self-reported postoperative symptoms appeared broadly similar to patterns described in previous studies, caution is warranted when comparing them with clinically monitored hospital-based investigations, as the present study relied primarily on retrospective participant self-report rather than standardized clinical assessment. These findings demonstrate that CS contributes not only to maternal morbidity but also to widening health inequalities.
Healthcare providers strongly influence delivery mode decisions. 34 In Bangladesh, families often change their consulting gynecologists due to multiple reasons, including cost, distance, and perceived quality of care. In our data (Supp. Figure 2), although the majority of mothers (82.57%) reported continuing antenatal and delivery care with the same gynecologist throughout pregnancy, a proportion (17.43%) of participants changed providers during the course of care, which appeared more frequent in the Rajshahi division (22.10%). This discontinuity in care may affect clinical decision-making, particularly regarding delivery mode. Additionally, many physicians default to repeat CS for women with prior surgical births, citing safety concerns. 35 In our sample, first-, second-, and third-born infants accounted for 45.19%, 41.73%, and 11.12% of deliveries, respectively [Supp. Table 2], highlighting the role of previous birth history in influencing CS rates. In Bangladesh, cultural perceptions reinforce these trends, with some families believing that CS protects the baby or avoids the pain of labor.
Our multivariable logistic regression analysis identified urban residence as the strongest and most consistent factor associated with cesarean section (CS) delivery, with urban mothers having approximately 70% higher adjusted odds of undergoing CS compared with their rural counterparts. This association remained robust after adjustment for maternal age, hospital type, education, occupation, and postoperative complications, suggesting that urban residence may be independently associated with delivery mode beyond its correlation with socioeconomic characteristics. Similar findings have been reported in several low- and middle-income countries, where urban populations generally demonstrate higher CS utilization rates.36–38 This pattern may reflect differences in healthcare accessibility, greater concentration of private healthcare facilities, and increased availability of surgical obstetric services. Maternal occupation emerged as the second significant factor associated with CS delivery, with homemakers having 33% lower adjusted odds of CS than service workers. Although the association was modest and approached borderline statistical significance, its persistence after multivariable adjustment suggests that employment status may capture dimensions of maternal autonomy, healthcare accessibility, or socioeconomic positioning, which cannot be fully explained by education or residential status. Formally employed women may have greater financial independence and familiarity with institutional healthcare systems, which may facilitate access to private facilities where CS utilization is substantially higher.39–41 However, this interpretation should be approached cautiously, as occupational status may also reflect unmeasured factors such as household income, partner education, or intra-household decision-making dynamics.
To curb unnecessary CS, multisectoral strategies are needed. First, the government should establish model maternal healthcare facilities that strictly follow evidence-based guidelines, serving as benchmarks for both public and private institutions. The Ohio Perinatal Quality Collaborative in the United States provides a useful model, reducing early-term elective births through provider training and standardized protocols. 42 Similar interventions could be adapted to the Bangladeshi context. Second, the government should monitor the regulation of private hospitals, as the majority of institutional deliveries are carried out there. The high prevalence of CS delivery observed in private facilities may reflect a combination of institutional, structural, and patient-related factors; however, the present study was not designed to evaluate provider incentives or motivations. Given the observed association between multiple institutional employment patterns and high CS rates in private facilities, future studies should evaluate potential policy approaches, such as improving obstetric care continuity and strengthening institutional oversight. Private hospitals should be encouraged or required to employ permanent, full-time gynecologists to ensure continuity of care and reduce reliance on scheduling convenience. Third, public awareness campaigns are essential to challenge misconceptions about CS. Educational interventions should emphasize that while CS is lifesaving when medically indicated, it also carries potential maternal and neonatal risks. Mass media, including television, radio, newspapers, and social platforms, can play a central role in educating families about the relative risks and benefits of CS versus NVD.
Conclusion
The study demonstrates a high prevalence of CS delivery in the selected regions of Bangladesh, particularly within private healthcare facilities. The findings also revealed substantial regional variation in delivery practices, participant-reported reasons for CS delivery, and self-reported postoperative complications. Postoperative pain was the most commonly reported complication, whereas infection, hemorrhage, and thromboembolism were reported less frequently and showed regional variation. Several participant-reported, institutional, and healthcare-system factors were associated with CS delivery patterns. However, the study primarily provides descriptive evidence on CS practices and participant-reported post-cesarean experiences; therefore, causal interpretations should be avoided. Further clinically validated, longitudinal, and mixed-methods research is needed to better understand the mechanisms underlying these observations. Comprehensive reforms, including stricter clinical protocols, regulation CS prectices in private hospitals, provider training, and strengthening monitoring, may help reduce unnecessary CS and improve maternal health outcomes in Bangladesh.
Strengths and limitations
This study has several strengths. It was conducted across diverse regions of Bangladesh, including urban and rural areas, and involved a large sample that represented varied geographic and socioeconomic groups, enhancing generalizability. In addition, data were collected not only from mothers but also from healthcare providers, offering a broader understanding of factors influencing CS delivery rates in Bangladesh.
However, some limitations should be noted. The cross-sectional design did not permit causal inference regarding the relationships between healthcare provider behavior, institutional practices, and CS delivery decisions. Furthermore, the analyses exploring determinants of CS delivery were primarily descriptive because important clinical and socioeconomic confounders, including prior CS history, detailed obstetric risk profiles, and household economic status, were not comprehensively available. Consequently, the findings should be interpreted as exploratory and associative rather than definitive evidence of causality. The study did not cover all administrative divisions, which may restrict nationwide representativeness. Data on post-cesarean complications were self-reported by the mother rather than based on clinical records, raising the possibility of recall bias or underreporting. Although birth registration records were used to support systematic participant selection, recruitment was conducted across multiple districts, wards, and unions; therefore, some degree of geographic clustering was unavoidable during field implementation. Moreover, the duration and severity of post-cesarean complications were not assessed, hence, cannot provide a deeper understanding of long-term maternal outcomes. Despite these limitations, the findings provide important evidence on the overuse of CS and its associated factors in Bangladesh.
Supplemental material
Supplemental material - The cesarean epidemic in Bangladesh: Associated factors and maternal health risks
Supplemental material for The cesarean epidemic in Bangladesh: Associated factors and maternal health risks by Hazrat Ali, Md Imran Nur Manik, T M Fahad, Kazi Muhtasim Fuad, Shibli Rubatul Islam, Al Mamun, Md Anwarul Haque, Md Shariful Islam, Md Emtiaj Alam, Tarannum Naz, Shariful, Haque, Md Faruk Hasan, Md Rafiqul Islam Khan and Alam Khan in Journal of Public Health Research.
Footnotes
Acknowledgments
The authors would like to thank and acknowledge the participation of all the mothers in this study. We appreciate their willingness to support our study. In addition, we would like to thank and acknowledge the general physicians, gynecologists, and administrative staff of healthcare facilities who shared their information with us. We also thank our interviewers for their pleasure in working with us.
Ethical considerations
Data collection procedure of the study was reviewed and approved by Rajshahi University Ethical Council (RUEC) with approval number RUEC/2018/c-section003.
Consent to participate
Written informed consent was obtained from the majority of respondents. In the case of illiterate participants, verbal consent was taken rather than written consent, where interviewers read the same consent information to let them know. All efforts were made to maintain the privacy of the collected information.
Author contributions
HA, MINK, TMF, and AK conceived and designed the experiments. MINK, MAH, and KMF performed data collection from Dhaka division. TMF, AM, and MSI conducted data collection from the Rajshahi Division. HA, MEA, and TN collected data from the Chittagong Division. SRI, MFH, and MRIK performed data curation. SH, and AK performed statistical analysis and data interpretation. All authors read and approved the manuscript
Funding
The study was supported with special research grant of Ministry of Science and Technology, Bangladesh (grant project no.39.00.0000.009.99.024.22-901/SRG-225614, MS Group) and partly by University of Rajshahi Research fund (grant project no. A170/5/52/R.U./Science-38/22-23). The funders had no role in study design, data collection and analysis, preparation of the manuscript or publication of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used during current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.