
Abstract
This study evaluated the effect of calcium-rich nanohydroxyapatite (nano-HA) as an intracanal medicament on root fracture resistance compared with calcium hydroxide (CH). Forty-eight caries-free maxillary central incisors were instrumented and randomly assigned to a two-factor design (two medicaments × two sealers), yielding four experimental groups (n = 12/group): CH + resin-based sealer, CH + bioceramic-based sealer, nano-HA + resin-based sealer, and nano-HA + bioceramic-based sealer. The medicaments were applied and stored in simulated body fluid at 37 °C and 100% humidity for 10 days. After removal, the canals were obturated with heated gutta-percha using either a resin-based or a bioceramic-based sealer, and were then stored for an additional 28 days. Vertical fracture resistance was measured using an Instron Universal Testing Machine. Data were analyzed using two-way ANOVA (p < 0.05). The nano-HA groups showed a higher mean fracture resistance (924.04 N) than the CH groups (818.54 N). The highest fracture resistance was observed in the nano-HA + bioceramic-based sealer group (1020.38 N), whereas the lowest was observed in the CH + resin-based sealer group (665.83 N). The main effect of sealer type was statistically significant (p < 0.001), while no significant interaction between medicament and sealer type was detected. Within the limitations of this in vitro study using static vertical loading, sealer type had a large, statistically significant effect on fracture resistance, with the bioceramic-based sealer yielding higher values than the resin-based sealer. Although the nano-HA groups exhibited numerically higher fracture resistance than calcium hydroxide, the main effect of intracanal medicament did not reach statistical significance. These findings are limited to laboratory conditions and should not be directly extrapolated to long-term clinical performance.
Keywords
Introduction
Root canal treatment can be completed in single or multiple visits. In some cases with questionable or unfavorable prognoses, using an intracanal medicament dressing after adequate biomechanical preparation, including irrigation, offers a clinical advantage.1,2 Interim intracanal medication is used when root canal obturation cannot be completed in a single visit to prevent bacterial growth and provide additional disinfection.2,3
After the application interval for intracanal medicaments, root canal treatment can be completed using a combination of endodontic root canal sealers and gutta-percha to fill voids and irregularities in the root canals and reduce bacterial remnants. A wide range of root canal sealers have been used, including formulations such as epoxy resin, calcium hydroxide, silicone, and bioceramics. 4 Although epoxy-resin-based ones are still considered the gold standard, bioceramic formulations have gained increasing attention in endodontic practice due to their tissue compatibility, bioactivity, and ability to bond to dentin, which are considered key factors in reinforcing dentin structure.4–7
Calcium hydroxide (CH) is widely used in endodontics as an interim dressing agent and supports hard tissue formation by promoting active mineralization.2,4,6,8,9 However, a key limitation of intracanal interim CH application is its potential to increase the risk of vertical root fractures. This occurs due to significant collagen degradation in the superficial root dentin, which compromises the structural integrity and durability of the hard tissue.10–13
Hydroxyapatite (HA) has attracted attention recently for its broad range of applications in tissue engineering and dentistry, which are quite similar to those of the main inorganic constituent of tooth.14–16 Nanohydroxyapatite (nano-HA) is a widely studied nanobiomaterial in restorative dentistry, as evidenced by the literature.17–19 While its inorganic components support hard tissue regeneration, its biocompatibility and effects on microorganisms and biofilms make it a candidate to be considered in the development of endodontic biomaterials.20–26 Nano-HA refers to HA particles, the size of which ranges from 1 to 200 nm.14,27 This nanomaterial can be integrated into the enamel structure and infiltrate the native collagen of demineralized dentin without causing collagen degradation, which may compromise the structural integrity of the root; therefore, the remineralization of dentin and enamel by nano-HA has been widely used in previous research work.12,23,24,27,28 Additionally, nano-HA modulates osteoblast differentiation by mediating autophagy, 22 stimulates the adhesion and odontogenic potential of HDPCs, 20 promotes the growth of odontoblast-like MDPC-23 cells, 21 and inhibits bacterial growth and reduces bacterial biofilm formation.15,25,26
Previous studies have primarily focused on incorporating nano-HA into sealers and restorative materials, demonstrating improved bioactivity, remineralization potential, and mechanical properties.17,29,30 Although experimental studies have yielded promising results, scientific evidence on the potential benefits remains limited. In addition, to the best of our knowledge, limited data are available regarding the use of nano-HA as an intracanal medicament. In contrast, it can be hypothesized that nano-HA, due to its biomimetic and remineralizing properties, may counteract dentinal collagen degradation and contribute to the preservation or enhancement of dentin mechanical integrity. However, despite this biological rationale, the actual effect of nano-HA as an intracanal medicament on root fracture resistance remains unclear and requires systematic investigation under controlled conditions.
In this context, this study aimed to evaluate the effect of calcium-rich nano-HA, as an interim intracanal medicament, on root canal fracture resistance compared with conventional CH before obturation, with various types of sealers. The null hypotheses were that neither the type of intracanal medicament nor the sealer type, nor their interaction, would have a significant effect on root fracture resistance.
Materials and methods
The ethics committee’s approval for the study was obtained from the local Non-Interventional Ethics Committee in compliance with the Helsinki Declaration (2024/9.9 project no: 2024/1892). The experimental setup for this laboratory study was developed and conducted in accordance with the Preferred Reporting Items for Laboratory Studies in Endodontology (PRILE) 2021 guidelines.
Sample size calculation, sample selection, and eligibility
The sample size was calculated using G*Power software (version 3.1; Heinrich-Heine University, Düsseldorf, Germany). The effect size was derived from previously reported fracture resistance differences in a comparable in vitro study. 31 An a priori power analysis for a two-way ANOVA was performed assuming a medium effect size (Cohen’s f = 0.30), an alpha error probability of 0.05, and a power (1 − β) of 0.90, resulting in a minimum sample size of 12 specimens/group.
Forty-eight caries-free maxillary central incisors, extracted from patients aged 35–55 years due to advanced periodontal disease and severe mobility, were collected. The inclusion criteria were as follows: closed root apices, a single straight root canal, similar root structure shapes, and consistent dentinal thickness. The calculus and tissue remnants were removed. A single root canal and apical foramen were confirmed by a periapical radiography at different angles and under an operation microscope at various magnifications (Carl Zeiss Meditec AG, Oberkochen, Germany). The exclusion criteria were curved root formation, external or internal resorption, anatomical variations, cracks, craze or fracture lines, or incomplete apical formations. The same length of 13 mm was obtained for samples by occlusal reduction to a 2 mm cemento-enamel junction. Roots with buccal and lingual thicknesses at the coronal part of the root dentin of 1.5–2 mm were selected for standardization. Buccolingual dentin thickness was measured using a digital caliper with 0.01 mm accuracy. All the roots were carefully examined under an operating microscope, and with the help of fiber-optic lighting to detect any craze lines or cracks on the root surfaces.
Preparation of root canals, allocation of groups, and experimental design
The apical patency was checked via a #15 K-type stainless steel hand file. The working length was determined to be 12 mm by subtracting 1 mm from the apical opening. The root canals were instrumented with an M-Wire nickel-titanium rotational file system up to 40/.06v (ProTaper Next; Dentsply Maillefer, Ballaigues, Switzerland). During the instrumentation, the root canals were irrigated with 1 mL of 2.5% sodium hypochlorite between each instrument. After the shaping procedure before dressing, the last irrigation was performed with 2 mL of sodium hypochlorite and 2 mL of distilled water. All the samples were labeled numerically (1–48) and kept in a saline solution throughout the experimental period before being dressed with various intracanal medicaments.
The instrumented roots were allocated into two main groups randomly according to the use of various non-setting medicaments (CH/nano-HA) and four subgroups (n = 12; Figure 1), according to the sealer used for obturation (resin-based/bioceramic-based) via a computer-assisted randomization program (Research Randomiser Program, v4.0, available at http://www.randomiser.org) by a blind operator.

Group allocation and representative periapical radiographs with the materials used.
Preparation of interim medicaments and dressing of the root canals
To prepare homogeneous agents and avoid human error, distilled water and pure glycerin were mixed using a magnetic stirrer at 300 rpm and 55 °C to form a base at 20% concentration. Carboxymethyl cellulose (CMC) was added to obtain a viscous hydrogel after 60 min. The interim materials were composed of conventional CH (Kalsin; Spot Dental Products, İzmir, Türkiye) powder and HA nanopowder (Sigma–Aldrich, Saint Louis, MO, USA) added to the same vehicle prepared as a hydrogel at a ratio of 1:2 (powder/liquid ratio (wt.%)) and mixed at 150 rpm for 60 min (Table 1). The homogeneity of the hydrogel mixtures was verified visually and by ensuring consistent viscosity and absence of particle aggregation throughout the mixing process. Additionally, standardized magnetic stirring conditions were maintained for all preparations to ensure uniform particle distribution.
The components of the prepared interim medicaments and simulated body fluid.
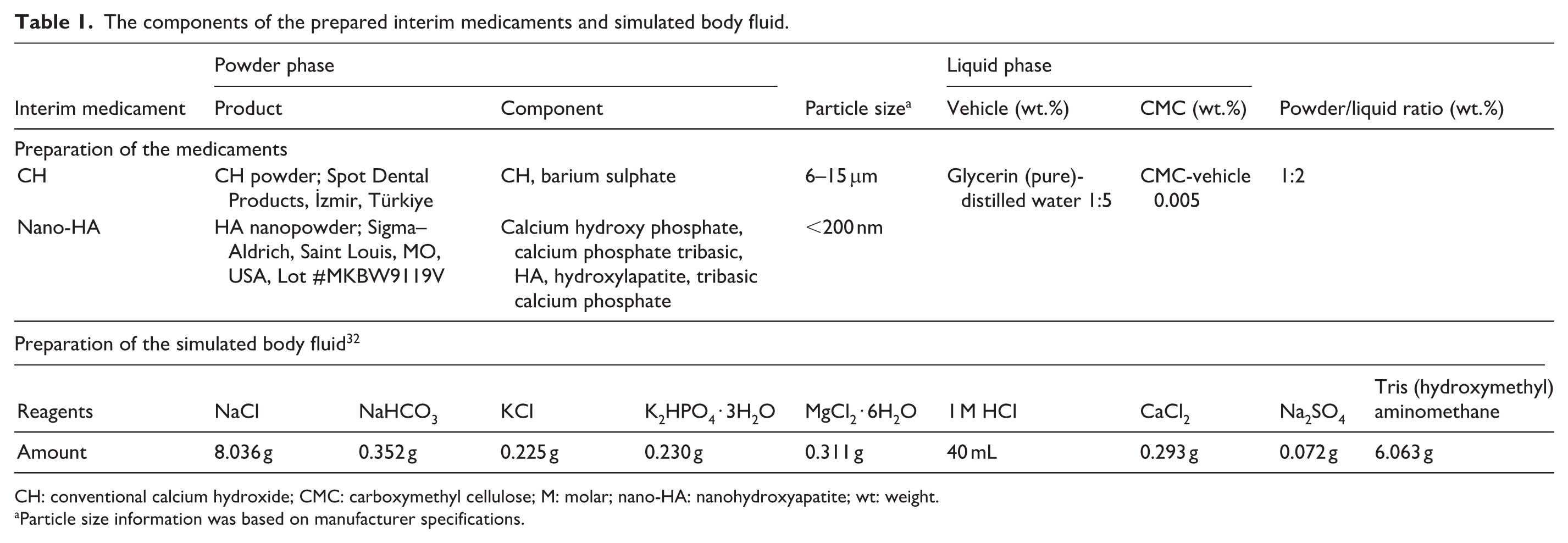
CH: conventional calcium hydroxide; CMC: carboxymethyl cellulose; M: molar; nano-HA: nanohydroxyapatite; wt: weight.
Particle size information was based on manufacturer specifications.
After the root canals were dried with absorbent tapered paper points (40/.06, Diadent; Diamond Dental Industrial, Chongiu City, Korea), the interim medicaments were applied to the root canal system in a standardized manner using syringes equipped with application tips. Standardization of medicament placement was verified by comparing pre- and post-medication periapical radiographs taken at multiple angulations (buccolingual and mesiodistal), confirming uniform canal filling in terms of length and density (Figure 1). The coronal entrance of the roots was sealed with a temporary sealing material (Cavit™; 3M ESPE, Seefeld, Germany).
Simulated body fluid (SBF) absorbed media were designed using a sponge formwork to mimic the tooth socket and clinical conditions. The chemical composition of freshly prepared SBF is presented in Table 1. 32 The samples were stored in the specially produced bodymimetic media in an incubator (37 °C, 100% humidity) for 10 days. 33 The SBF-soaked sponge was periodically monitored (every 2–3 days), and replenished with fresh SBF to maintain stable moisture levels and ionic availability throughout the 10-day medicament period.
Removal of dressing and obturation
The root canals were irrigated with 17% EDTA and activated using EDDY (VDW, Munich, Germany). The activation period included five cycles of replenishment and activation for EDTA, each lasting 1 min, with 30 s of conventional needle irrigation followed by 30 s of EDDY activation, and 1 mL of irrigation solution was used per minute. 13 Finally, the root canals were flushed with two cycles of 2.5% sodium hypochlorite (2 mL) replenishment and activation, followed in a similar manner. All the root canals were dried with absorbent tapered paper points to proceed with the obturation phase.
The tug-back feeling was controlled with a resin- or bioceramic-based sealer (AH Plus Jet®, AH Plus® Bioceramic Sealer; Dentsply Sirona, Ballaigues, Switzerland) coated on a master cone 40/.06 (Endoart; Inci Dental, Istanbul, Türkiye) following the working length. For obturation, the continuous-wave technique was used across all groups. Using the Fast Pack device (Eighteeth Medical, Chang-Zhou, China), the gutta-percha was down-packed with a medium tip (50/00.5) to 3–4 mm from the working length. Then, the root canals were obturated with a backfill device (Eighteeth Medical, Chang-Zhou, China) via a large tip (23 Ga) cartridge-dispensed warm gutta-percha to the cementoenamel junction. The fillings of root canals were checked with periapical radiographs (Figure 1). The cleaned cavity was bonded (G-Premio Universal Bond; GC, Tokyo, Japan) and sealed with light-cured flowable composite (Fusion Flo; Prevest DenPro, Jammu, India). The samples were stored in similar SBF-absorbed body mimic media in an adjustable incubator (100% humidity at 37 °C) for 28 days to allow the obturation materials to harden entirely and the bioceramic sealer to present bioactivity.32,34
All clinical procedures (preparation of root canals to the obturation phase) were conducted by an experienced endodontic specialist (S.K.) to avoid human error parameters. Besides, the steps were controlled via periapical radiography by another experienced endodontist (O.Ö.).
Preparation of the models and fracture strength testing
All the roots were immersed in molten wax (8 mm from the apex) to obtain a 0.2–0.3 mm thick layer, which was subsequently embedded in autopolymerizing acrylic resin. After polymerization, the root samples and the wax were removed. Then, the samples were covered with a second type of silicon impression material (Zetaplus, Zhermack, Italy) and mounted in pre-spaced acrylic resin to simulate the periodontal ligament.
Each sample was mounted individually on a computer-controlled testing machine (Instron Universal Testing Device, Instron 4411; Instron Corporation, Canton, MA, USA). A steel conical tip with an apical diameter of 0.8 mm, tapered at a 60° angle, was affixed to the testing machine. A compressive right-angle load was applied at the center of the coronal surface using a 60° conical steel tip (0.8 mm diameter), aligned parallel to the long axis of the specimen, at a crosshead speed of 1 mm/min until fracture occurred. Readings were recorded using computer-assisted software (Instron Bluehill Lite Software; Instron Corporation, Canton, MA, USA). The force at the time of fracture was recorded in Newtons (N). Fracture testing was performed by an operator blinded to group allocation.
Statistical analysis
Statistical analyses were performed with R-Project Software for MacOS (www.R-project.org; R Foundation for Statistical Computing, Vienna, Austria). Data are presented as mean ± standard deviation (SD). Normality was assessed using the Shapiro–Wilk test. A two-way analysis of variance (ANOVA) was performed to evaluate the main effects of intracanal medicament and sealer type, as well as their interaction, on vertical fracture resistance. The ANOVA results included F statistics, p values, and eta-squared (η2) effect sizes. When overall differences among groups were identified, pairwise comparisons were conducted using Tukey’s honestly significant difference (HSD) post hoc test. Statistical significance was set at p < 0.05.
Results
In this study, which aimed to evaluate the effect of calcium-rich nano-HA as an interim intracanal medicament on the fracture resistance of root canals, compared with conventional CH, the mean fracture resistance was 924.04 N in the nano-HA groups and 818.54 N in the CH groups. The highest mean value for the group and root canal sealer interaction was obtained with nano-HA + bioceramic-based, at 1020.38 N. The CH + resin-based sealer had the lowest interaction with 665.83 N. The main effect of sealer type on vertical fracture resistance was statistically significant (F = 22.432, p < 0.001, η2 = 0.338), with roots obturated using the bioceramic-based sealer demonstrating significantly higher resistance than those filled with the resin-based sealer (Table 2). The large effect size observed for sealer type (η2 = 0.338) indicates that a substantial proportion of the variance in fracture resistance was attributable to the filling material rather than the intracanal medicament. The model explained ~38% of the variance, moderate explanatory power, in fracture resistance, indicating that additional structural and biomechanical variables contribute to fracture resistance beyond the tested factors. Figure 2 presents the representative loading values at the time of fracture measured by the universal test device. Compressive forces were recorded as negative values by the testing software; however, for clarity, absolute values were considered for statistical analysis and reporting. Figure 3 shows the average vertical fracture resistance values according to the interim medicament and root canal sealer.
Vertical fracture resistance values (N) according to the interim medicament and root canal sealer.
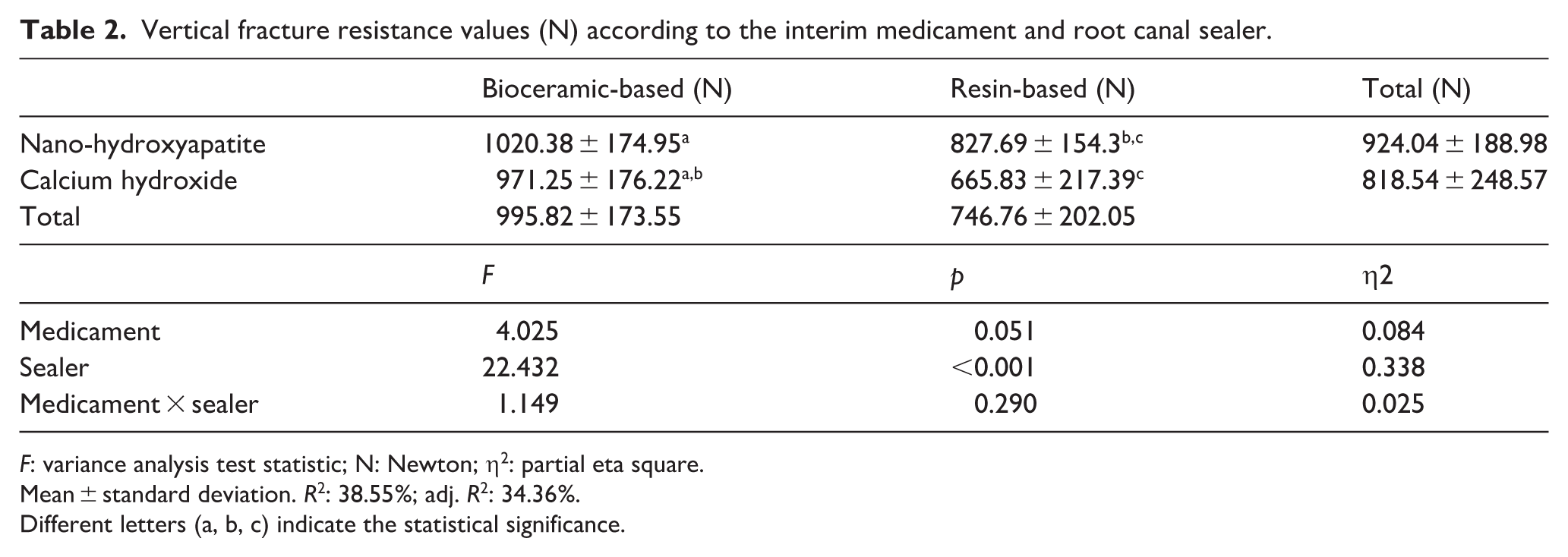
F: variance analysis test statistic; N: Newton; η2: partial eta square.
Mean ± standard deviation. R2: 38.55%; adj. R2: 34.36%.
Different letters (a, b, c) indicate the statistical significance.

Representative loading values at the time of fracture measured by the universal test device.

Average vertical fracture resistance values (N) according to the interim medicament and root canal sealers (vertical column values indicate recordings in Newton).
Discussion
Microcracks, cracks, or vertical root fractures are critical in endodontics, and since they are challenging to diagnose, there are many questions and uncertainties about their management. Additionally, fractures of roots that have been endodontically treated are common in clinical practice. 35 Even though the predisposing factors have not been fully defined, 36 root canal treatment is a critical etiological factor for vertical root fracture.35,37–39 The main factor is the loss of healthy pulp tissue, which is highly relevant because of its biochemical effects on dentin–pulp complex adherence, which provides a natural monoblock structure of the tooth. Although the loss of connective tissue is considered the leading risk factor, the root canal treatment stages, such as access cavity preparation by the removal of extensive hard tissue, especially from pericervical dentin, as well as extended shaping for instrumentation, dentin exposure to medication agents, irrigation solutions, and dentinal collagen degradation, are other factors contributing to the development of craze lines, microcracks, and structural distortions that may predispose the root to fracture.13,36,38,40
Various cavity designs, minimally invasive approaches, and coronal restorative application recommendations to protect an endodontically treated tooth from mechanical distortions are available to sustain the prognosis.41,42 However, considering the loss of connective tissue such as dental pulp and dentin–pulp adhesion, these approaches remain palliative, as vertical root fracture reports in the literature support this situation.38,39,43–45 More advanced intraroot strengthening strategies are needed in clinical practice to prevent their formation. In this context, although the superiority in long-term clinical success over resin-based root canal sealers is still controversial, it is crucial to benefit from biomaterials to strengthen the dentin in the root canal, which are more compatible with the biological characteristics of tissues, support dentin microhardness with bioactive properties, and prevent collagen degradation, which would not cause loss of elasticity in the tooth.4,46 Biologically characterized root canal filling materials present promising mechanical reinforcement efficiency.47–49 In recent years, bioceramic-based intracanal medicaments have been introduced; however, research has focused on physicochemical characterization, cytocompatibility, and antibiofilm activity.50,51 There is a lack of evidence to improve dentinal hard tissue structure for root strengthening, a key issue that should be addressed, given the effects of CH on dentin.
This study compared nano-HA and CH as interim intracanal medicaments with respect to their effects on root fracture resistance. The comprehensive methodology ensured a controlled environment for standardized mechanical testing. A factorial design was preferred to evaluate not only the independent effects of medicament and sealer type but also their potential interaction under standardized conditions. The null hypotheses regarding medicament type and interaction were not rejected, whereas the null hypothesis related to sealer type was rejected, because the main effect of intracanal medicament did not reach statistical significance (p = 0.051), and no significant interaction between medicament and sealer type was observed.
Although the nano-HA + bioceramic group exhibited the highest mean values, this difference was not statistically significant in terms of interaction. The superior performance of the bioceramic-based sealer may be related to its chemical bonding potential with dentin and its ability to form interfacial mineral deposition zones, which have been associated with improved stress distribution under compressive loading conditions.
Reported maximum bite forces and occlusal loads vary considerably depending on tooth type and functional conditions, with anterior teeth generally subjected to lower forces than posterior teeth. 52 Since the present study was conducted using maxillary central incisors, the fracture resistance values obtained should be interpreted within the context of anterior teeth. In contrast, posterior teeth are exposed to higher and more complex occlusal forces, which may result in different mechanical behavior and clinical outcomes. Therefore, direct extrapolation of these findings to posterior teeth should be approached with caution.
In addition to fracture resistance values, fracture pattern has been reported as an important parameter for evaluating the clinical relevance of in vitro loading tests. Previous studies have classified fractures as favorable (restorable) or catastrophic (non-restorable), emphasizing that the location and direction of crack propagation may influence clinical prognosis rather than fracture load alone.53,54 Materials that increase fracture resistance do not necessarily alter the distribution of fracture modes. Clinically, unfavorable (catastrophic) fractures often necessitate extraction or complex surgical interventions, whereas favorable fractures may allow for restorative options. 55 Classification of fracture patterns in vitro can therefore better approximate the clinical prognosis associated with each material combination. Although fracture patterns were not systematically evaluated in the present study, it can be speculated that materials promoting dentin reinforcement and more homogeneous stress distribution, such as bioceramic sealers and potentially nano-HA, may be associated with more favorable fracture modes. However, this assumption remains hypothetical and should be confirmed in future studies incorporating detailed fracture pattern analysis.
Given that ~62% of the variance remained unexplained, factors such as variability in dentin microstructure, residual stress patterns, and loading configuration may have influenced fracture outcomes in the present study. The absence of a statistically significant interaction suggests that the mechanical contribution of the sealer was independent of the type of medicament previously applied. This finding may indicate that the structural reinforcement provided by the obturation material outweighs potential modifications induced by short-term intracanal dressing by long-term bioactivity.
The bioactivity characteristics of biomaterials that increase tooth fracture resistance and enable hard tissue regeneration in dentin may be explained by ion exchange in the environment, the accumulation of HA within the material’s porous structure, and the contact with the dentin surface. 34 The nano-HA particles, which are already components of the inorganic matrix that needs to be formed, can penetrate dentin tubules, act as a scaffold during precipitation, and promote the integrity and growth of apatite crystals. The potential reinforcing effect of nano-HA may be attributed to its ability to penetrate dentinal tubules, act as a nucleation site for mineral deposition, and promote intrafibrillar remineralization of collagen. These mechanisms may contribute to improved structural integrity and resistance to crack propagation.
For these types of materials to exhibit bioactive properties, they should come into contact with biological environments via biological fluids.32,34 Biomaterials with a setting-by-hydration mechanism require body fluids not only to harden but also to exhibit their bioactive properties. Therefore, under in vitro conditions, the moisturizing and clinical simulation methods using these materials should not rely solely on humidity; instead, they should use ionized solutions that mimic body fluids. Typically, the samples are kept at 37 °C and 90%–100% humidity for vertical fracture tests to mimic clinical conditions.13,42,43,56–58 However, the authors believe that only humidity would be limited in reflecting the actual behavior of the biomaterials. SBF has been widely used in bioactivity testing to promote apatite precipitation and to evaluate material–fluid interactions under ionic conditions.32,34 In this context, the storage intervals of the dressing and after the obturation phase were determined in specially designed SBF-absorbing media via sponge formwork. Its use in the present study aimed to provide a more biologically relevant environment than humidity alone.
The removal of CH should be performed effectively; thus, residual medicament may compromise the sealing ability of sealers and allow the entry of materials into dentinal walls. Kolunsağ et al. reported that a sonically activated EDTA application duration increases the fracture resistance of roots by up to 5 min. 13 Although prolonged EDTA exposure may influence dentin microhardness, 59 the same irrigation protocol was applied to all groups to standardize the procedure and minimize confounding effects, which may influence the bonding behavior of sealers. On the basis of this evidence, the methodology of this study employed 5 min of sonically activated EDTA irrigation before sodium hypochlorite activation to remove the medicaments. 13 On the other hand, since hydroxyapatite is a mineral phase expected to form as a result of bioactivity within the root canal dentin structure, residual nano-HA is unlikely to adversely affect obturation, particularly when bioceramic sealers are used. In contrast to the potential negative impact of residual calcium hydroxide on resin-based sealers, nano-HA residues may be more compatible with bioactive materials. Therefore, the combination of a bioactive intracanal medicament such as nano-HA with bioceramic sealers may create a more favorable environment for mineral deposition and structural reinforcement, which could partly explain the numerically higher fracture resistance values observed in the nano-HA groups.
The vehicle of interim medicaments used to apply the root canal system is an essential component, so various types of vehicles have been used for effectiveness. 60 A viscous hydrogel was prepared by mixing glycerin and CMC to achieve homogeneous and standardized medicaments. This hydrogel formation allowed the agent to be placed in the root canal to achieve compact and controllable consistency. Therefore, the materials remained stable in the root canal throughout the storage interval.
It is essential to standardize all the parameters possible when conducting a laboratory-based study, except for the variable that will be the focus of the evaluation. A no-medicament control group was not included because the primary objective was to compare two intracanal medicaments under standardized conditions. The use of crown removal for standardization was one of the limitations of this study. Even though this process was performed to standardize the samples, the residual structure of the tooth, pericervical dentin thickness, coronal restoration, and parafunctional/occlusal habits should not be ignored, as dentin elasticity affects the fracture strength of endodontically treated teeth.36,37 However, this research focused on the root strength, so this methodology excluded the mentioned variability. Therefore, cyclic or dynamic loading was not applied. The applied load was static and delivered in a single vertical direction. In clinical conditions, anterior and posterior teeth are exposed to multidirectional and dynamic occlusal forces rather than a single perpendicular load. However, vertical static loading is widely used in in vitro fracture resistance studies because it provides a standardized and reproducible method for comparing the mechanical performance of different materials under controlled conditions.43,56–58 Therefore, the fracture resistance values obtained in this experimental model may not fully replicate the complex biomechanical stresses encountered intraorally.
Additionally, since the study was carried out under in vitro conditions, it could not fully reflect the intraoral environment, although the samples were stored in SBF-containing media. Since vertical root fracture is multifactorial, it is recommended that experimental designs be conducted to evaluate the correlation between other factors. One of the other limitations is that nano-HA does not have any radiopacity. However, although this situation constitutes a disadvantage in controlling the hermetic placement of the material, this limitation was minimized by comparing pre- and post-medication radiographs of the prepared but unmedicated roots with the contrast difference and following the apical overflow of the agent placed by coronal injection. In addition, since the hydrogels were prepared via a magnetic stirrer, the possibility of any air bubbles was also eliminated. Besides, although nano-HA has demonstrated antimicrobial potential in previous studies, 61 antimicrobial properties were not evaluated in the present investigation and therefore cannot be directly correlated with the mechanical findings. Although the difference between bioceramic and resin-based sealers was ~250 N, the direct clinical translation of this mechanical advantage remains uncertain due to the multifactorial nature of vertical root fracture. Under these conditions and within these limitations, further studies are needed to comprehensively understand the behavior and achievements of nano-HA dressings and the clinical impact of the results.
Nanobiomaterials have been increasingly investigated across multiple biomedical disciplines; since nanoscale materials are smaller and have better controllable properties than traditional materials do, they make it possible to develop new and more effective treatments in the fields of dentistry and endodontics.14,62,63 These findings suggest that incorporating nano-HA into endodontic treatments with the use of bioceramic sealer may represent a promising biomaterial approach; however, further studies including fatigue testing and clinical evaluation are required before any inference regarding long-term performance can be made. To the best of our knowledge, there are limited data regarding the use of nano-HA as an intracanal medicament. Future perspectives related to the study of calcium-rich nano-HA versus conventional CH for interim intracanal medication include the following: conducting extensive clinical trials to validate the in vitro findings and assess the long-term clinical outcomes, investigating the detailed mechanisms that enhance fracture resistance, exploring the optimization of nano-HA formulations to improve the bioactivity, and antimicrobial properties, comparative studies with other emerging biomaterials and medicaments were performed to establish a comprehensive understanding of the relative advantages and limitations, developing radiopaque formulations. These future perspectives aim to build on the promising findings of the study and facilitate the translation of nano-HA into routine clinical practice, ultimately improving patient outcomes in endodontics.
Conclusion
Within the limitations of this in vitro study, sealer type demonstrated a statistically significant and large effect on fracture resistance, with the bioceramic-based sealer showing higher resistance values than the resin-based sealer.
Although the main effect of intracanal medicament did not reach statistical significance, the nano-HA groups exhibited numerically higher fracture resistance values compared with CH. Notably, the highest mean fracture resistance was observed in the nano-HA combined with the bioceramic-based sealer group.
While no significant interaction between medicament and sealer type was detected, the favorable mechanical performance observed in the nano-HA + bioceramic combination suggests that this novel medicament warrants further investigation in studies with larger sample sizes and additional mechanical and clinical parameters.
These findings are limited to static fracture resistance measured under laboratory conditions and cannot be directly extrapolated to long-term clinical outcomes.
Footnotes
Ethical considerations
The ethics committee’s approval for the study was obtained from the Karabük University Non-Interventional Ethics Committee (KBÜ-2024/9.9 project no: 2024/1892).
Author contributions
Conceptualization: O.Ö., T.K. Data curation: O.Ö. S.K. Formal analysis: O.Ö., S.K. Methodology: S.K., E.Ş. Supervision: O.Ö. Validation: O.Ö., T.K. Writing—original draft: O.Ö. Writing—review and editing: T.K. and O.Ö.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data related to this study’s findings are available from the corresponding author upon reasonable request.