
Abstract
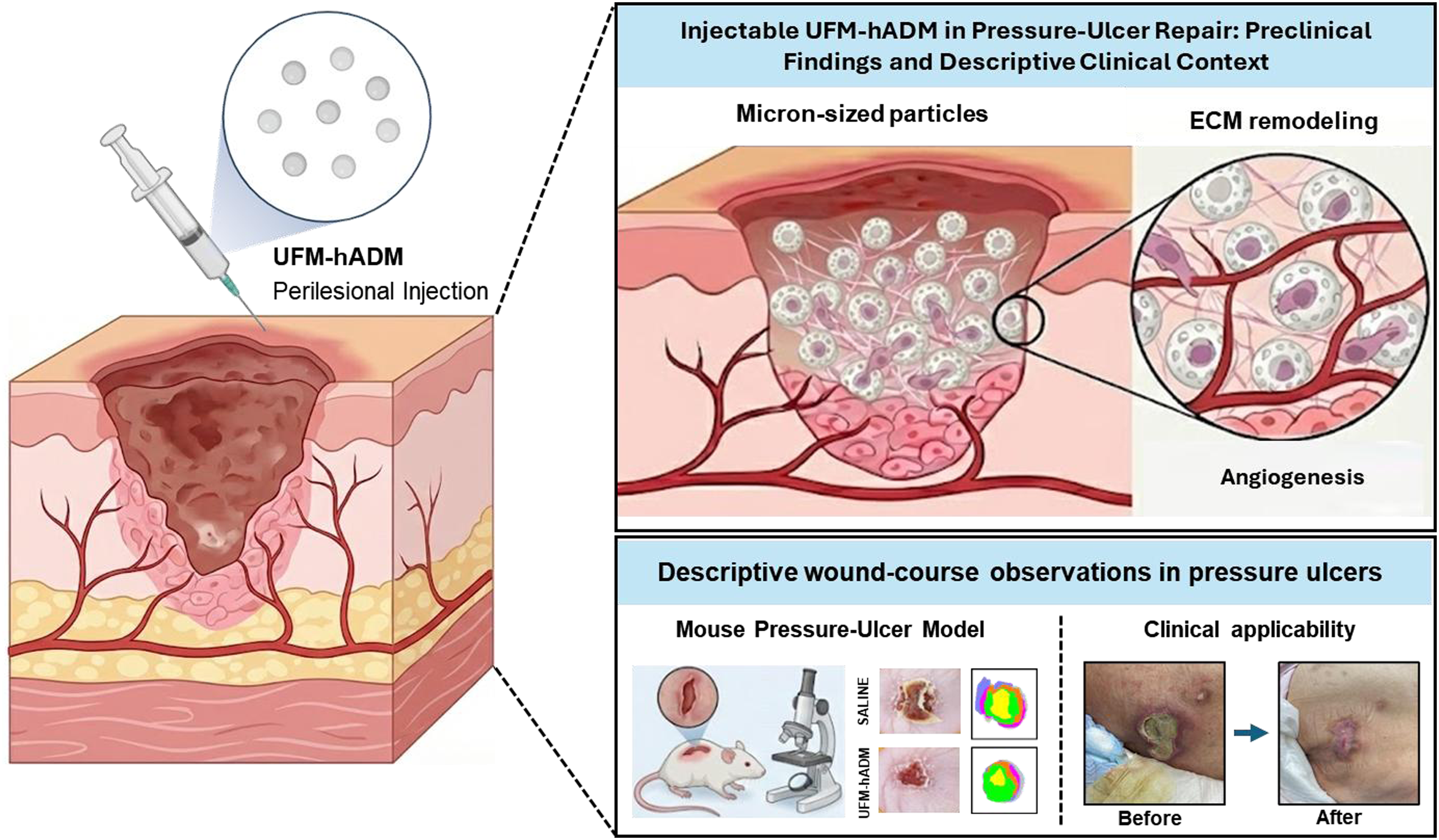
Chronic pressure ulcers persist within a self-sustaining microenvironment marked by unresolved inflammation, inadequate neovascularization, and excessive extracellular-matrix (ECM) degradation, highlighting the need for injectable bioactive scaffolds that can be delivered precisely to reprogram compromised tissue. The ultra-fine micronized human acellular dermal matrix (UFM-hADM; ∼70 μm) is designed to remain suspendable and pass through narrow-gauge injection, enabling uniform distribution along irregular wound margins and undermined tissue planes where sheet-type matrices may have limited contact and conformability. Here, we evaluated perilesional injection of an UFM-hADM (∼70 μm) as an injectable ECM scaffold in a murine cyclic ischemia–reperfusion pressure-ulcer model. Compared to saline, UFM-hADM accelerated early wound closure and improved quality of healing at Day 7, with enhanced re-epithelialization and dermal regeneration accompanied by increased collagen deposition. Mechanistically, UFM-hADM shifted the wound milieu toward a pro-healing program by attenuating pro-inflammatory cytokines (TNF-α and IL-6) while increasing IL-10, promoting neovascularization and vascular maturation (upregulated VEGF, increased CD31 and α-SMA), and restoring balanced ECM remodeling (elevated COL1A1 and COL3A1 with suppression of MMP1 and MMP3). These coordinated molecular changes opposed inflammatory, protease-rich transcriptional signatures identified in human pressure ulcers through public transcriptomic reanalysis. In addition, exploratory observational use of Ministry of Food and Drug Safety (MFDS)-approved UFM-hADM for pressure ulcers, undertaken with patient consent as part of routine clinician-directed care, suggested acceptable tolerability and a favorable healing course during follow-up. Collectively, these findings provide mechanistic support for the adjunctive clinical use of UFM-hADM as a minimally invasive, human-derived injectable ECM adjunct that may facilitate pressure-ulcer healing through coordinated modulation of immune, vascular, and matrix responses.
Keywords
● Perilesional microinjection of ultra-fine micronized hADM (UFM-hADM) enables conformal extracellular matrix (ECM) delivery to irregular pressure-ulcer geometry. ● In a mouse ischemia–reperfusion pressure-ulcer model, UFM-hADM accelerates repair by coordinating inflammation control, angiogenesis, and constructive ECM remodeling. ● During follow-up after treatment, acceptable tolerability and a favorable wound-healing course were observed.
Introduction
Pressure ulcers remain a persistent and costly complication across acute care, long term care, and community settings, disproportionately affecting older adults and patients with immobility, neurologic impairment, or critical illness.1,2 Contemporary meta analyses report substantial prevalence in hospitalized populations, while long term care settings show wide variability that reflects differences in case mix, surveillance intensity, and prevention resources. 2 At a population level, global burden analyses indicate that pressure ulcer incidence and disability have continued to rise alongside demographic aging and the expansion of complex chronic disease, reinforcing pressure injuries as a major, growing challenge for health systems. 3 Collectively, these data underscore a major unmet need for therapies that extend beyond coverage and instead target the biological barriers that lock pressure injuries into chronic, non-healing trajectories.
The etiology of pressure injury is multifactorial, with sustained mechanical loading over bony prominences leading to tissue deformation and compromised perfusion, often compounded by shear, moisture, nutritional deficiency, and systemic inflammation.4,5 Mechanistic frameworks emphasize two interacting pathways: direct deformation induced cellular damage and ischemic injury with subsequent reperfusion, both of which contribute to deep tissue injury and progressive cutaneous breakdown.6,7 Accordingly, mouse models applying cyclic compression via magnets or controlled devices have been used to recapitulate clinically relevant ischemia reperfusion patterns and to interrogate associated inflammatory and microvascular dynamics.8,9 Importantly, even after pressure relief and optimization of standard measures, established pressure injuries frequently persist, reflecting a failure to transition from early inflammation to coordinated proliferation and remodeling.10–12 Chronic wounds are characterized by sustained infiltration of neutrophils and predominance of classically activated pro-inflammatory macrophages (M1)with elevated tumor necrosis factor alpha (TNF-α) and interleukin (IL)-6, coupled with protease antiprotease imbalance that increases matrix metalloproteinase (MMP) activity and accelerates extracellular matrix (ECM) breakdown, thereby limiting pro-healing signaling.13,14 Among the cytokines most relevant to non-resolving wound inflammation, TNF-α and IL-6 are major pro-inflammatory mediators that amplify leukocyte activation, matrix degradation, and impaired tissue repair, whereas IL-10 is a key anti-inflammatory and pro-resolving cytokine that helps suppress excessive inflammation and supports the transition toward tissue repair.15–17 These hostile inflammatory and proteolytic conditions impair angiogenesis and granulation, perpetuate hypoxia-associated stress and stalled re-epithelialization, and leave the wound bed matrix-depleted and protease-rich, making durable closure unlikely without targeted biologic intervention. 18
Decellularized ECM therapies are mechanistically well suited to chronic pressure injuries, as the dermal ECM provides adhesive and mechanical cues and regulates growth factor signaling required for repair.14,19 By restoring fragmented matrix architecture, ECM biomaterials can modulate innate immunity, promote constructive remodeling and neovascularization, and bias early macrophage polarization toward a pro-regenerative phenotype.20–22 In addition, ECM-associated proteoglycans and glycosaminoglycans can sequester and protect heparan sulfate-binding growth factors (e.g., VEGF, FGF), thereby preserving bioavailability in protease-rich wound environments and supporting vascular ingrowth and maturation.19,23
Within this therapeutic class, human acellular dermal matrix (hADM) has a long clinical history as a biologic scaffold and has evolved from sheet grafts to micronized or paste type formats that better conform to irregular cavities, undermined edges, and tunneling wounds.24–26 Clinical studies in chronic wounds, including randomized trials in diabetic foot ulcers and multicenter trials of paste type ADM for complex defects, support that dermal matrix scaffolds can accelerate granulation, enhance epithelialization, and improve healing outcomes when added to standard care.26,27 However, conventional sheet grafts may be limited by handling constraints and inadequate filling of dead space, while some particulate products face challenges in injectability and homogeneous dispersion, particularly when narrow gauge needle delivery is desired.
Ultra-fine micronized human acellular dermal matrix (UFM-hADM; mean particle size ∼70 µm; extensively decellularized) was investigated as an injectable extracellular matrix scaffold designed to support minimally invasive delivery and stable suspension. In this study, we evaluated UFM-hADM in a mouse pressure injury model that captures cyclic ischemia and reperfusion injury, and we interrogated mechanistic endpoints aligned to core chronic wound barriers, including inflammatory cytokine signaling, neovascularization markers, and matrix remodeling signatures. We additionally examined public transcriptomic data comparing chronic pressure-ulcer tissue with healing skin and retrospectively summarized two descriptive routine-care patient observations in which UFM-hADM had been used for refractory stage 3 pressure injuries.
Materials and methods
Animals
All experiments in this study were conducted using female SKH-1 hairless mouse (8–10 weeks old, 20–25 g body weight), obtained from RaonBio (Yongin, Korea). The mouse were housed under standard laboratory conditions with controlled temperature and humidity, with ad libitum access to water and food. All animal procedures adhered to institutional and national guidelines and were approved by the Institutional Animal Care and Use Committee (IACUC) of Hulux (Approval No. Hulux-2025-02-001). The mouse were acclimatized for at least 7 days before randomization to Control (Saline) and hADM groups (n = 5/group).
Pressure-ulcer model
Pressure ulcers were induced on the shaved dorsum using a cyclical ischemia–reperfusion (I/R) model with opposing neodymium magnets. 9 Under isoflurane anesthesia (DaonPharm, Seongnam, Korea), the dorsal skin was gently lifted and sandwiched between two circular neodymium magnets (diameter 12 mm, thickness 3 mm, mass 2.51 g; surface flux density ≈ 2,800 G) for 12 h, followed by a 12-h release. This 24-h cycle was repeated three times (total 72 h), and the day of the final release was defined as Day 0, at which point a single full-thickness circular ulcer was present. On Days 0, 1, and 3, ultra-fine micronized human acellular dermal matrix (UFM-hADM) or saline was administered as ten perilesional intradermal/subcutaneous microinjections (10 µL per site; 100 µL per wound) using a 31-gauge needle. The injection was distributed evenly around the wound margin in a sterile vehicle. For analysis of skin recovery, wounds were photographed using a digital camera at the indicated time points and measured using ImageJ software.
Ultra-fine micronized human acellular dermal matrix (SESALO®)
SESALO® (LCI Bio Co., Ltd., Namyangju, Korea) is an ultra-fine micronized human acellular dermal matrix (UFM-hADM) supplied as an injectable suspension. This product has been approved by the Ministry of Food and Drug Safety (MFDS) in Korea. The manufacturer reports a mean particle size of approximately 70 µm and exhaustive decellularization to minimize residual cellular components and improve safety and suspension stability.
Imaging and planimetry
On Days 0, 1, 3, 4, and 7, standardized images were captured at a fixed distance and lighting with a scale marker. The wound area was traced in ImageJ by a blinded researcher. Percent closure = [(A_Day 0 – A_Day x)/A_Day 0] × 100.
Hematoxylin-eosin (H&E) staining
On Day 7, wounds along with 2-3 mm margins were excised, fixed in 4% paraformaldehyde, paraffin-embedded, and sectioned (5 μm). The skin tissue was stained with H&E (G1120, Solarbio) and observed under an NSS-6 digital slide scanner (Nexcope, China). Quantitative histomorphometry was performed on wound-center sections using calibrated NSS-6 software by blinded observers. Residual wound width was defined as the maximal horizontal distance between the advancing epithelial margins. Epidermal thickness was measured as the vertical distance from the stratum basale to the stratum granulosum at 5-10 predefined non-overlapping points per section and expressed in micrometers (μm), and the mean value per section was used for analysis. Hair-follicle counts were recorded within the regenerated wound bed. Five sections per group were analyzed.
Masson’s trichrome (MT) staining
After the mice were euthanized, the skin was harvested and fixed in 4% paraformaldehyde and processed routinely for paraffin embedding. Subsequently, the skin tissue was sectioned at 5 μm and stained with MT (G1340, Solarbio) to evaluate collagen/ECM. Collagen deposition was quantified as the MT-positive area fraction (%) within a standardized wound-bed region of interest using threshold-based ImageJ segmentation under identical image-acquisition settings. The measured collagen-positive area was normalized to the total region-of-interest area. Five independent non-overlapping sections per group were analyzed. Images were acquired with an NSS-6 digital slide scanner (Nexcope, China).
Immunohistochemistry
Paraffin-embedded skin sections were deparaffinized in xylene and rehydrated through graded ethanol. Following heat-induced epitope retrieval in Tris-EDTA buffer at pH 9.0 for 20 min, sections were blocked and incubated overnight at 4 °C with anti-CD31 (EPR17259, Abcam, 1:2000) and anti-α-smooth muscle actin (α-SMA; myofibroblasts/perivascular cells; 34105, Cell Signaling, 1:500). Signals were visualized using HRP-conjugated secondary antibodies and DAB (GK500710, Gene Tech), followed by hematoxylin counterstaining. Images were captured with the NSS-6 digital slide scanner (Nexcope, China). Quantification was performed by blinded observers using two independent tissue sections per sample and three randomly selected high-power fields (HPFs) per section with Nikon NIS-Elements AR 64-bit version 5.30 software. CD31-positive microvessels were defined as discrete DAB-positive endothelial structures within the granulation tissue and were counted per HPF. α-SMA staining was quantified as the percentage of DAB-positive area within the same field after normalization to total tissue area. Representative negative and positive control staining data for CD31 and α-SMA immunohistochemistry are shown in Supplementary Figure S1. For each sample, the mean value across the analyzed fields was used as one biological replicate for statistical analysis.
Quantitative reverse transcription-polymerase chain reaction (qRT-PCR)
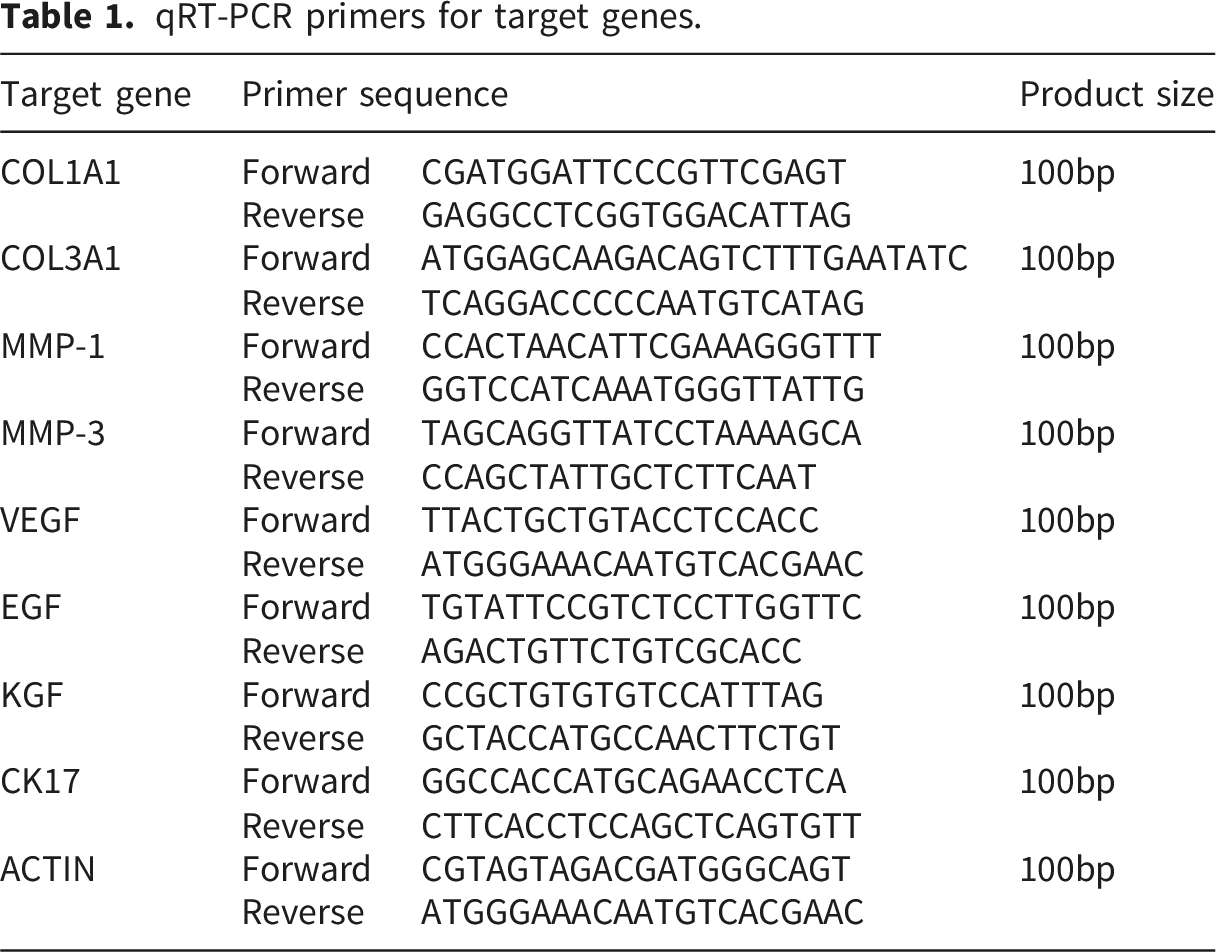
qRT-PCR primers for target genes.
Cytokine enzyme-linked immunosorbent assay (ELISA)
Wound tissue homogenates were analyzed for cytokine levels of TNF-α, IL-6, and IL-10 using commercial ELISA kits (ab108910, ab108870, ab100713, Abcam, Cambridge, MA, USA) according to the manufacturer’s protocols. Absorbance was measured at 450 nm using a microplate reader. Cytokine concentrations were normalized to the total protein content, determined via a bicinchoninic acid (BCA) protein assay. All measurements were performed in duplicate.
Transcriptomic dataset reanalysis
The bulk RNA-seq dataset GSE137897 was retrieved from the NCBI Gene Expression Omnibus and analyzed in R using the Seurat framework. Differential-expression analyses between conditions were performed with multiple-testing correction, and functional enrichment analyses (GO and KEGG) were conducted in R.
Statistical analysis
All statistical analyses were performed using GraphPad Prism (version 11.0; GraphPad Software, USA), unless otherwise stated. Data are presented as mean ± SD, with individual points representing biological replicates (n = 5/group unless otherwise specified). Wound-closure kinetics were analyzed using two-way repeated-measures analysis of variance (ANOVA) with Geisser-Greenhouse correction, followed by Sidak’s multiple-comparisons test. Single-endpoint comparisons between the saline and UFM-hADM groups, including histomorphometric parameters (residual wound width, epidermal thickness, hair-follicle counts, and collagen density), immunohistochemical quantification (CD31-positive microvessels per high-power field and α-SMA-positive area), qRT-PCR data, and ELISA data, were analyzed using an unpaired two-tailed t-test when normality and homogeneity of variance assumptions were satisfied; otherwise, the Mann-Whitney U test was applied. Transcriptomic dataset reanalysis was performed in R as described above. The two clinical cases were summarized descriptively and were not subjected to inferential statistical analysis. A p value < 0.05 was considered statistically significant.
Preliminary clinical application and methods
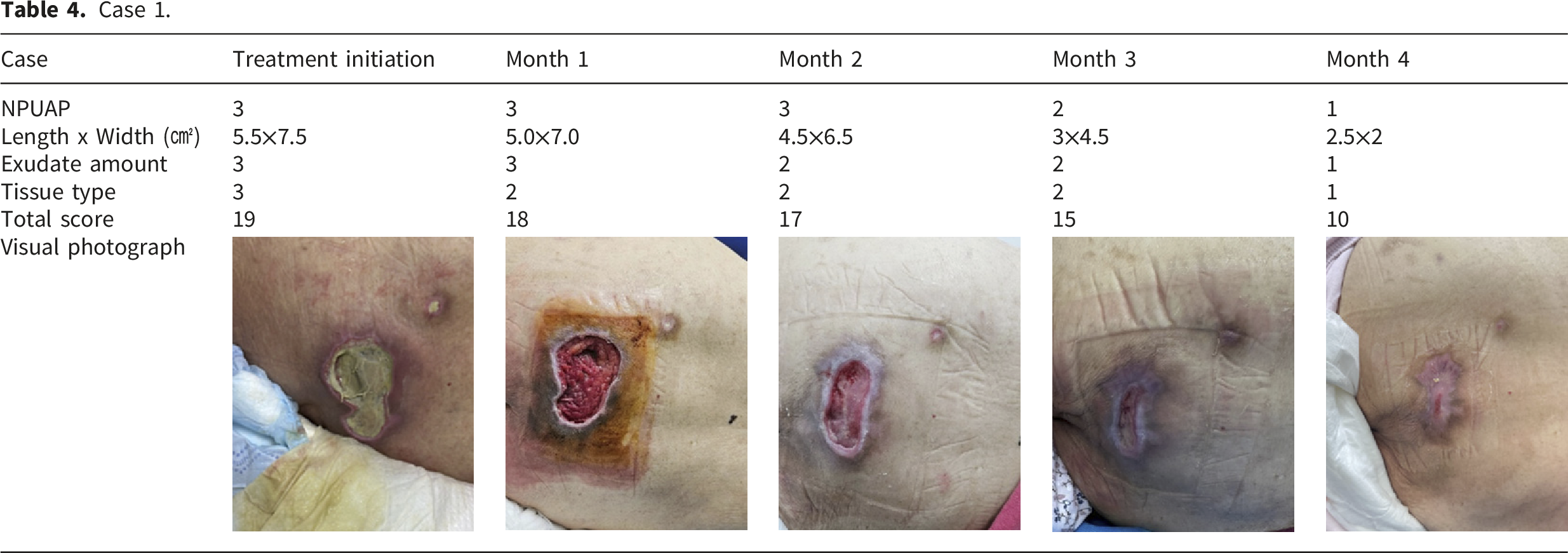
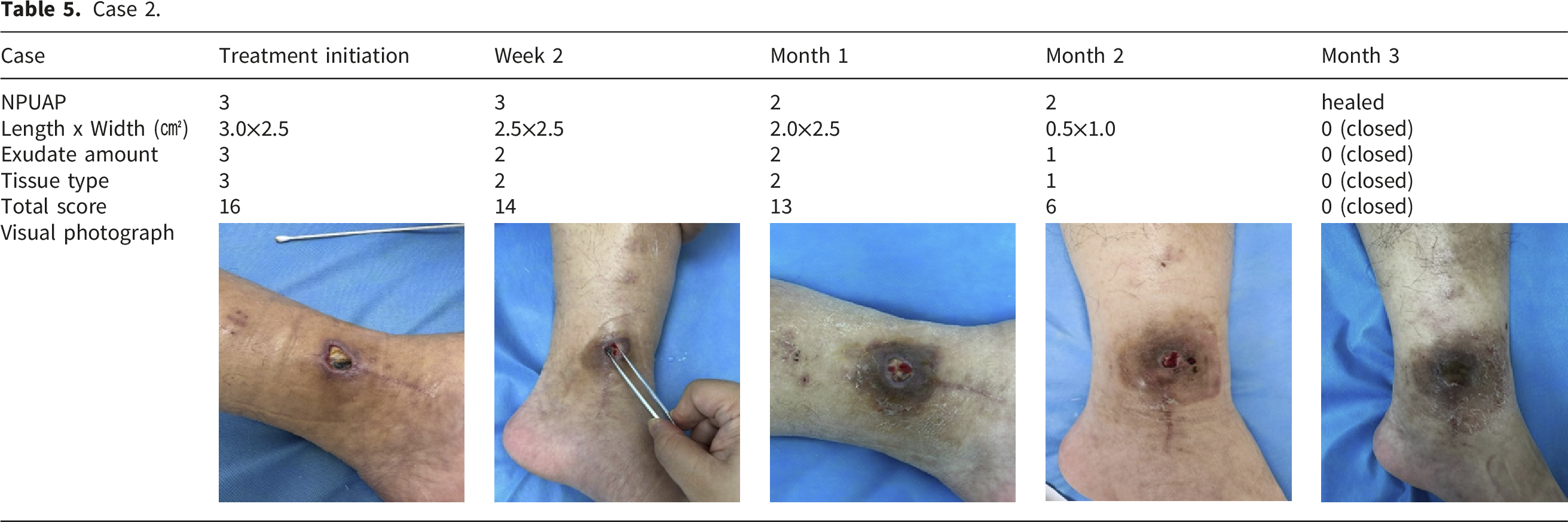
• Case 1: A 97-year-old immobile patient with trauma, dementia, and general debilitation, presenting with a worsening sacral pressure ulcer. • Case 2: A 78-year-old male patient with a chronic, treatment-refractory stage 3 pressure ulcer located on the ankle.
The national pressure ulcer advisory panel pressure ulcer (NPUAP) Stages/Categories (2007).
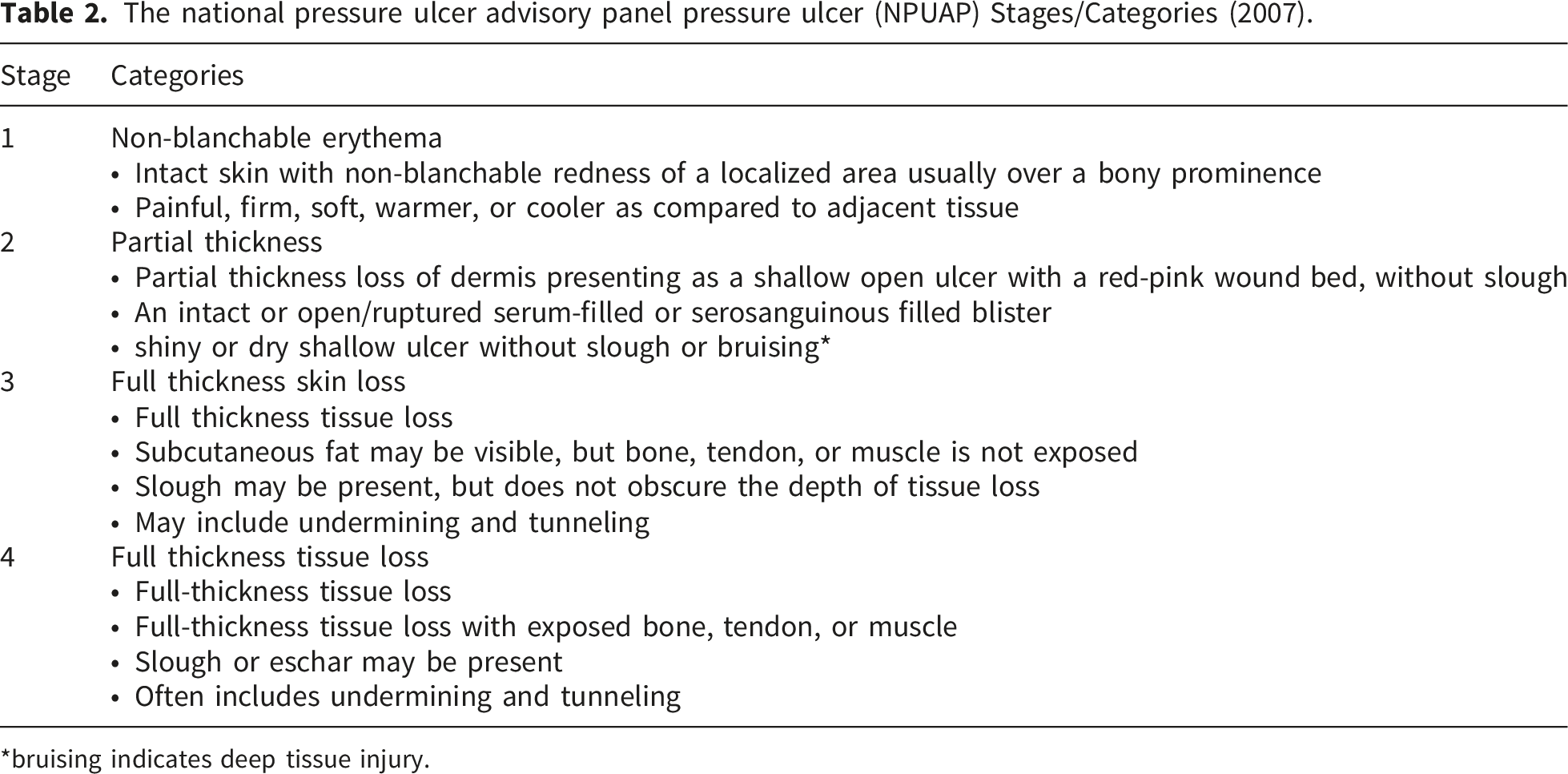
*bruising indicates deep tissue injury.
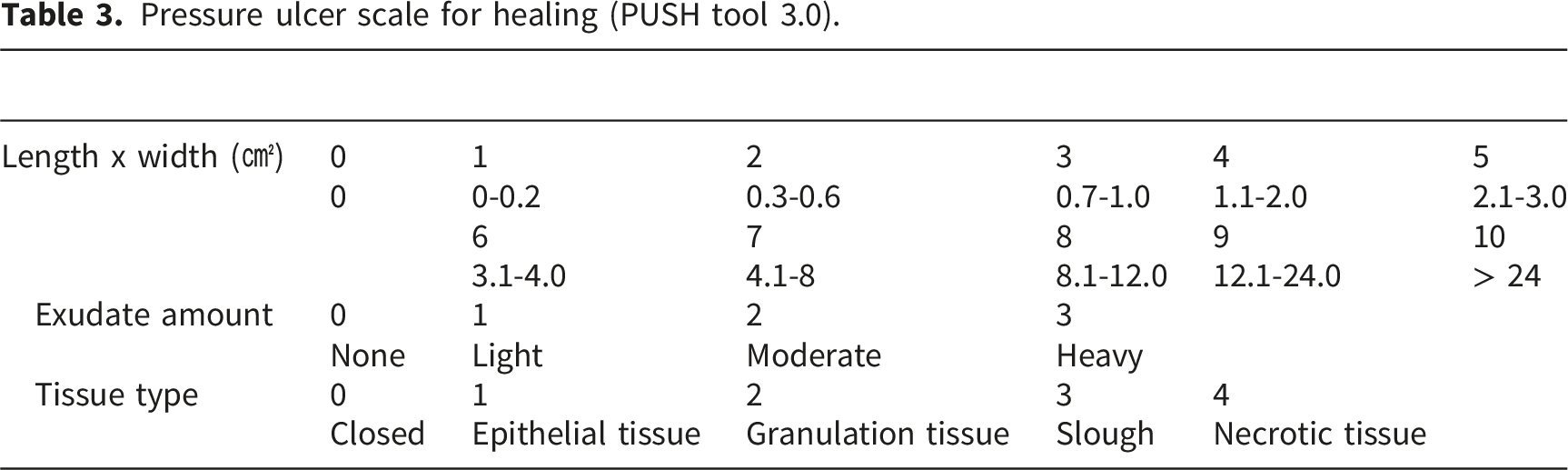
Pressure ulcer scale for healing (PUSH tool 3.0).
Results
UFM-hADM accelerates wound closure in a cyclic ischemia/reperfusion pressure-ulcer mouse model
We evaluated whether perilesional UFM-hADM improves early healing of pressure ulcers. Mouse underwent three standardized dorsal ischemia and reperfusion cycles to generate ulcers, followed by perilesional intradermal and subcutaneous injections of UFM-hADM or saline on Day 1 and Day 3, with macroscopic tracking through Day 7 (Figure 1(A)). Serial photography and planimetric contouring provided quantitative measurement of closure (Figure 1(B) and (C)). Across the time course, UFM-hADM treated wounds closed significantly faster than saline controls, with the separation most pronounced on Day 4 and Day 7. Taken together, these data indicate that perilesional UFM-hADM accelerates early macroscopic healing after ischemia and reperfusion injury. Study design and macroscopic assessment of wound closure in a murine pressure-ulcer model. (A) Experimental timeline. After a 7-day acclimation, dorsal pressure ulcers were induced by three ischemia/reperfusion cycles (12 h ischemia and 12 h reperfusion per cycle) using neodymium magnets (12 mm × 3 mm, 2800 Gauss). Perilesional intradermal/subcutaneous injections of UFM-hADM or saline were performed on Day 1 and Day 3 (10 μL per site, 10 sites). Biopsies were collected on Day 7. (B) Representative serial wound photographs acquired on Days 1, 3, 4, and 7. Right panels show planimetric contour overlays of wound boundaries across time points. Scale bars, 10 mm.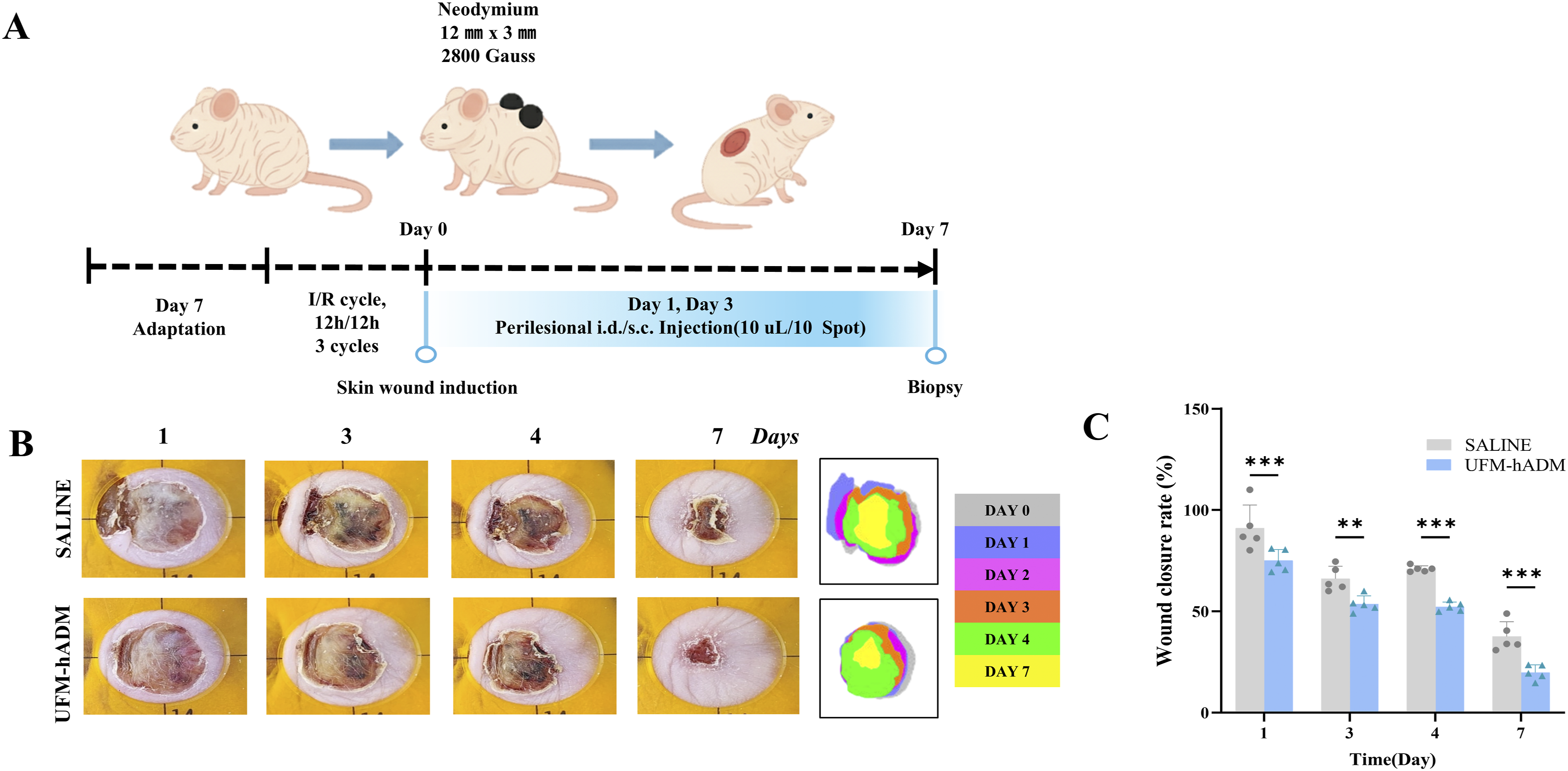
We next examined tissue-level regeneration on Day 7 by histology. Hematoxylin and eosin staining showed a narrower residual wound gap and more advanced re-epithelialization in UFM-hADM compared with saline, accompanied by a visibly thicker neo-epidermis and restoration of adnexal structures within the wound bed (Figure 2(A)). Masson’s trichrome staining revealed denser and more organized collagen in UFM-hADM-treated tissue. Quantitative morphometry confirmed these observations: residual wound width was reduced, epidermal thickness increased, the number of hair follicles within the wound bed was higher, and collagen-positive area was greater in the UFM-hADM group (Figure 2(B)). Together, these data indicate that UFM-hADM improves the quality of repair by advancing epithelial coverage and promoting dermal regeneration with robust collagen deposition. Histology and quantitative morphometry of wound repair on Day 7. (A)Representative hematoxylin and eosin (H&E) and Masson’s trichrome (MT) images of wound sites from saline and UFM-hADM groups on Day 7. Insets show higher magnification of the boxed regions. Scale bars: 2 mm (overview) and 400 μm (high magnification). (B) Quantitative morphometry in ImageJ. Metrics included residual wound width (μm), epidermal thickness (μm), hair-follicle counts within the wound bed (arrows indicate hair follicles in the high-magnification panels), and collagen density expressed as MT-positive area. Bars indicate mean ± SD. Each dot represents one animal. Statistics: two-tailed unpaired t-test for two-group comparisons. * p < 0.05; ** p < 0.01; **** p < 0.001.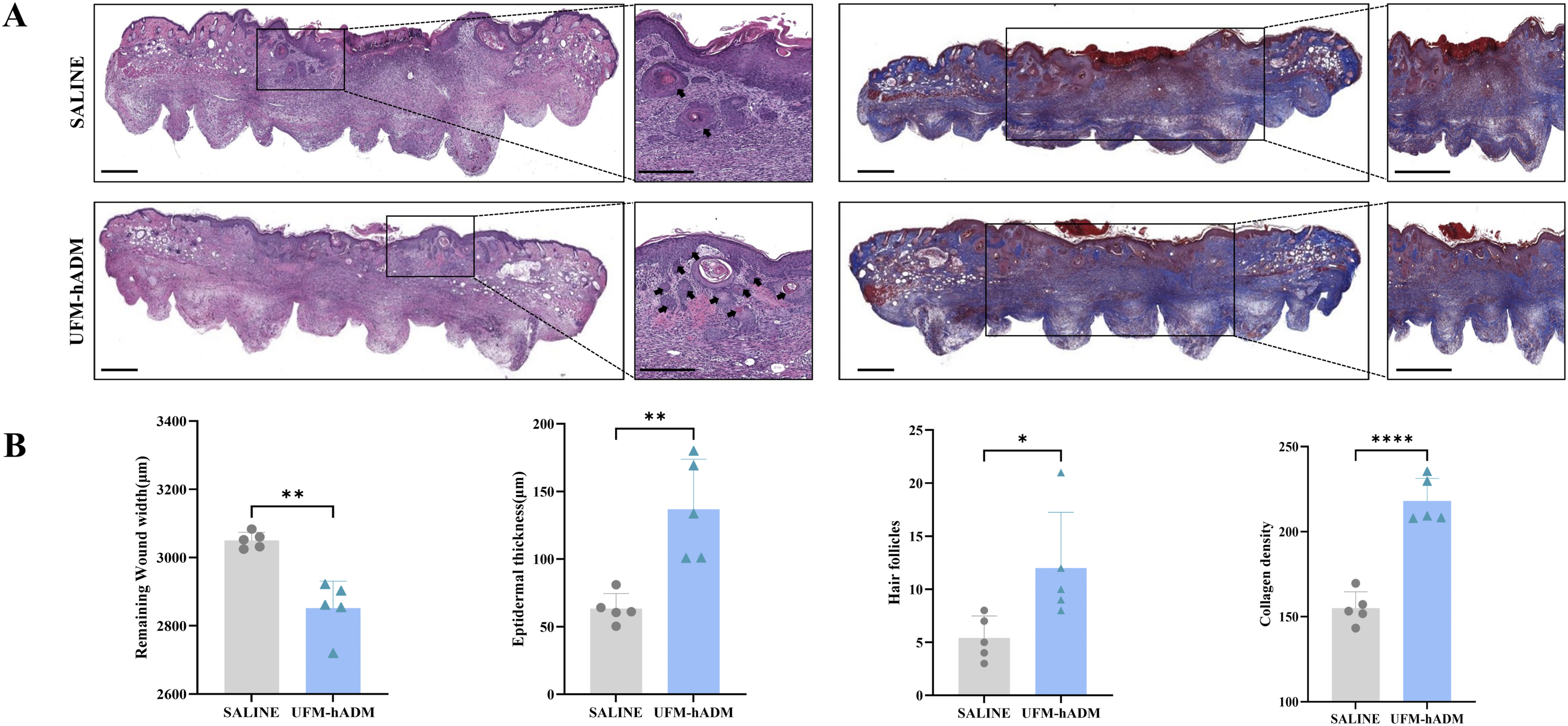
Chronic pressure ulcers exhibit a pro-inflammatory, ECM-Degradative gene signature
To characterize the transcriptional signatures underlying pressure ulcer pathology, we reanalyzedintact skin, acute wounds, and pressure ulcers, we reanalyzed the public human pressure-ulcer single-cell transcriptomic dataset (GSE137897) by aggregating single-cell profiles into group matrices for Skin, Acute wound, and Pressure ulcer and then performed differential expression and enrichment analyses. The heat map shows clear group separation, with pressure ulcers enriched for inflammatory and stress-keratin programs and skin enriched for structural and extracellular matrix transcripts (Figure 3(A)). In the Skin versus Pressure Ulcer contrast, panel B displays the top 20 differentially expressed genes ranked by absolute log2 fold change among genes with adjusted P less than 0.05. Ulcer samples showed higher expression of S100A8, S100A9, SERPINB family members, MMP1, MMP3, and stress keratins KRT6 and KRT16, whereas intact skin showed higher levels of extracellular matrix and barrier related genes including POSTN and LAMB4 (Figure 3(B)). Panel C visualizes GO Cellular Component cnet relationships generated from the top 50 genes, emphasizing cornified envelope and keratin filament nodes alongside a collagen-containing extracellular matrix node connecting ECM genes (Figure 3(C)). Panel D maps the top 50 genes onto KEGG pathways that capture protease activity and IL-17 associated inflammation together with cytoskeletal remodeling and energy metabolism modules (Figure 3(D)). Summarizes GO-CC enrichment, ranking collagen-containing extracellular matrix, basement membrane, and organelle lumen among the top terms, with high gene ratios and low adjusted P values (Figure 3(E)) Taken together, our data highlights a distinct pressure-ulcer transcriptional program characterized by heightened inflammation and protease activity alongside attenuated structural ECM synthesis relative to intact skin. Grouped transcriptomic profiling and tissue qRT-PCR. (A) Heat map of group-aggregated expression for Skin, Acute wound, and Pressure Ulcer from GSE137897. Highly variable genes were normalized and scaled to z-scores. (B) Top 20 differentially expressed genes for the Skin versus Pressure Ulcer comparison, ranked by absolute log2 fold change among genes with Benjamini–Hochberg adjusted P < 0.05. Gene symbols are labeled. (C) GO Cellular Component cnet network generated from the top 50 differentially expressed genes from the Skin versus Pressure Ulcer comparison. Nodes represent terms linked to member genes. Node size indicates term gene counts. Node color encodes gene-level fold change. (D) KEGG pathway cnet network generated from the top 50 differentially expressed genes from the same comparison. Size and color conventions match panel C. (E) GO Cellular Component dot plot summarizing enriched terms obtained from the top 50 gene set. Dot size indicates the number of mapped genes. (F) Day 7 wound-tissue qRT-PCR for COL1A1, COL3A1, MMP1, and MMP3. Expression normalized to ACTIN; each dot represents one animal. (G) Day 7 wound-tissue qRT-PCR for VEGF, EGF, CK17, and KGF (FGF7). Expression normalized to ACTIN; each dot represents one animal. Statistics: two-tailed unpaired t test for two-group comparisons. * p < 0.05; ** p < 0.01; *** p < 0.005.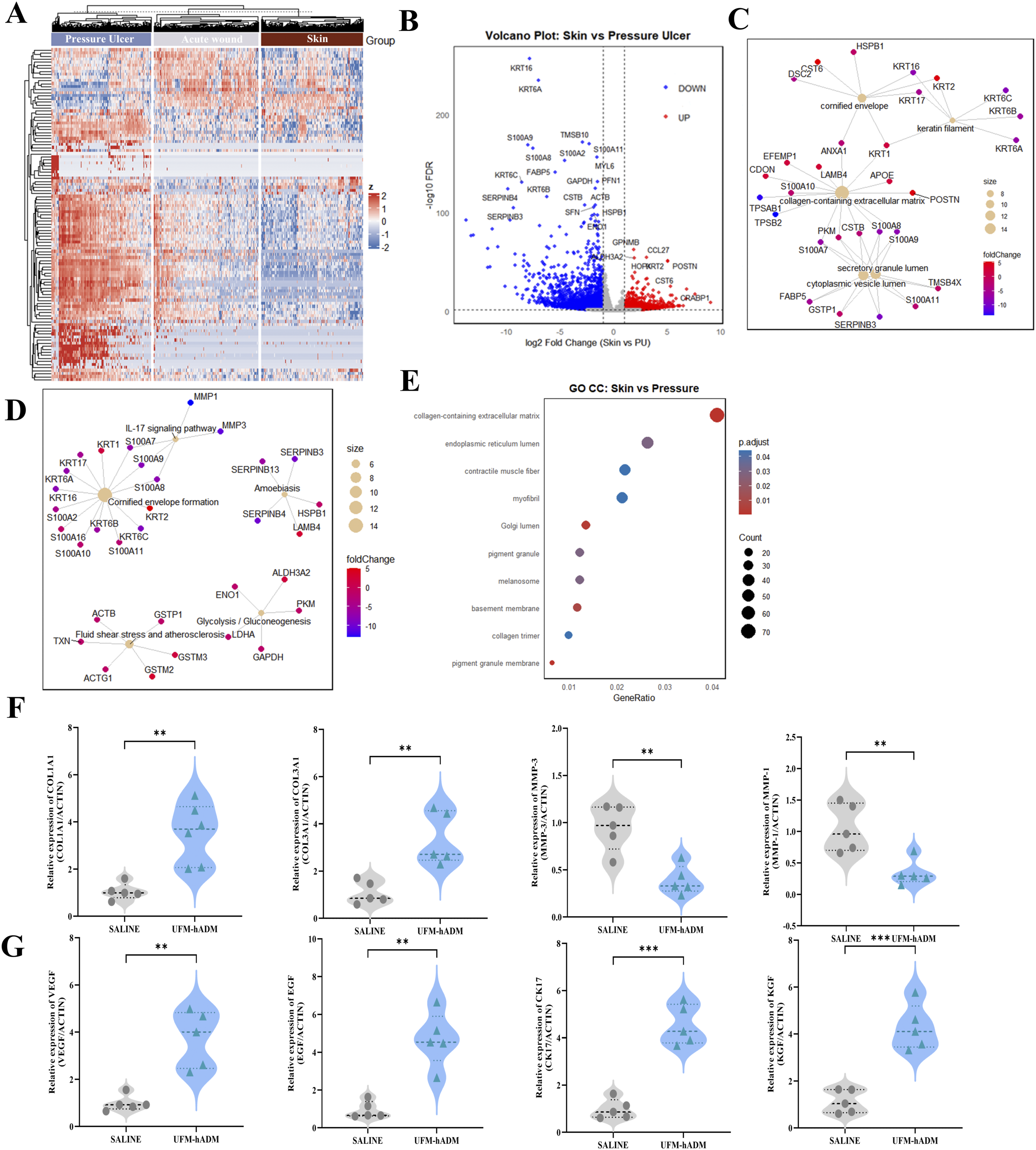
To determine whether UFM-hADM could therapeutically reverse this pathological signature in vivo, we quantified the expression of key marker genes in Day 7 mouse wound tissue… Relative to saline, UFM-hADM increased COL1A1 and COL3A1 and decreased MMP1 and MMP3, indicating reduced proteolysis with greater matrix deposition, and it elevated regenerative and epithelial–angiogenic markers VEGF, EGF, CK17, and KGF (FGF7) (Figure 3(F)–(G)). These findings corroborate the relevance of the human transcriptomic signatures and demonstrate that UFM-hADM actively redirects the wound microenvironment from a chronic, degradative state toward an ECM-rebuilding, pro-healing profile.
UFM-hADM shifts the wound cytokine milieu toward an anti-inflammatory profile
To investigate the inflammatory microenvironment at the protein level, consistent with the observed histological and molecular shifts, we quantified key cytokines in Day 7 wound homogenates using ELISA (Figure 4(A)). Compared with saline, UFM-hADM showed significantly lower TNF-α and IL-6 and higher IL-10 (Figure 4(B)). These measurements indicate attenuation of the inflammatory state and promotion of a pro-resolving profile in treated wounds. Workflow and ELISA of inflammatory cytokines in Day 7 wound tissue. (A) Sample processing schematic. Wound tissue was collected on Day 7, homogenized, and clarified for cytokine assays. (B) ELISA of TNF-α, IL-6, and IL-10 in wound homogenates from saline and UFM-hADM groups. Data are shown per animal with mean ± SD. Statistics: two-tailed unpaired t test. **** p < 0.001.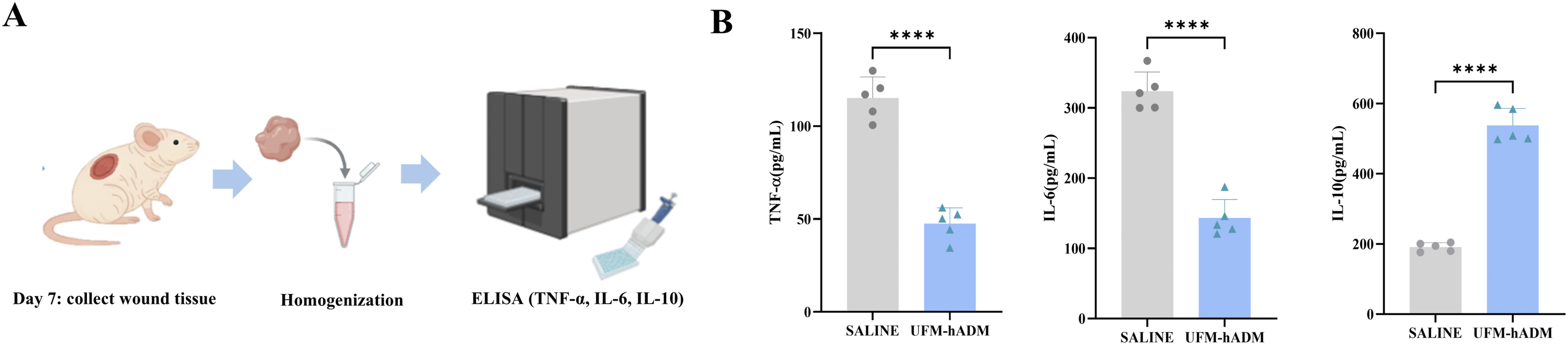
UFM-hADM enhances microvascular density and smooth-muscle investment in granulation tissue
We next evaluated the extent of tissue regeneration by analyzing neovascularization and stromal maturation. On Day 7, immunostaining for the endothelial marker CD31 revealed a significantly denser capillary plexus in UFM-hADM-treated wounds compared to saline controls. Specifically, capillaries in the treated group appeared more continuous beneath the neo-epidermis and extended deeper into the granulation bed, displaying fewer avascular gaps. Quantitative analysis confirmed this robust angiogenic response, showing an approximately 2- to 3-fold increase in the number of CD31-positive microvessels per high-power field in the UFM-hADM group (Figure 5(A) and (B)). Regarding stromal remodeling and maturation-associated features, α-SMA staining demonstrated broader perivascular coverage and an expanded population of interstitial myofibroblasts within the wound bed in the UFM-hADM group. Consistent with these observations, the α-SMA–positive area was approximately doubled relative to saline group (Figure 5(A) and (C)). Collectively, these findings indicate not only enhanced capillary formation but also features consistent with improved maturation and stabilization of neovessels within the regenerating tissue. Immunohistochemistry for microvessels and smooth-muscle markers in Day 7 wound tissue. (A) Representative sections stained for CD31 and α-SMA from saline and UFM-hADM groups, imaged at 40× objective. Scale bars, 100 μm. (B) Quantification of CD31-positive microvessels per high-power field. (C) Quantification of α-SMA-positive area, expressed as percent of tissue area. Bars indicate mean ± SD; each dot represents one animal. Statistics: two-tailed unpaired t test. * p < 0.05; *** p < 0.005.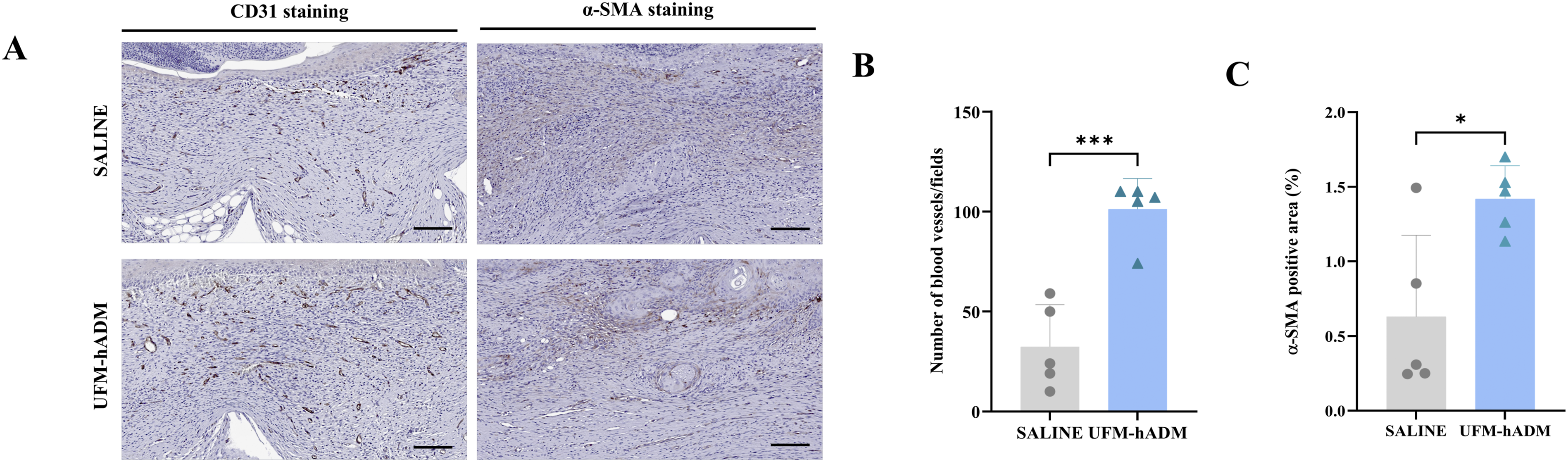
Wound-healing course in pressure-ulcer patients treated with adjunctive UFM-hADM
Case 1.
Case 2.
Discussion
This study supports UFM-hADM as an injectable, biologically active ECM scaffold that can accelerate pressure-ulcer repair by coordinating three interdependent processes that commonly fail in chronic wounds: inflammation resolution, neovascular restoration, and constructive matrix rebuilding. Rather than improving a single axis in isolation, UFM-hADM produced a convergent signature across cytokines, vascular markers, and ECM remodeling readouts, which strengthens biological plausibility because these processes are mechanistically coupled during cutaneous repair and typically collapse together in chronic ulcer state.27–29 Importantly, the cyclic ischemia-reperfusion framework used here is widely accepted to capture a key component of pressure-ulcer pathogenesis and has been repeatedly leveraged to evaluate therapeutic efficacy in preclinical settings.30,31 Within that context, the consistent macroscopic and histologic improvements at Day 7, together with multi-layer molecular shifts, argue against a purely nonspecific dressing-like effect and instead support a microenvironment-modifying mechanism.
Chronic pressure ulcers are characterized by excessive proteolytic activity that degrades newly deposited extracellular matrix faster than it can be restored, thereby undermining tissue structural integrity and growth factor retention required for stable granulation tissue formation and re-epithelialization. 32 In our study, UFM-hADM lowered MMP1 and MMP3 while increasing COL1A1 and COL3A1, with histologic evidence of more robust collagen deposition, consistent with rebalancing from degradative turnover toward constructive remodeling. This directionality aligns with wound-bed preparation principles that emphasize shifting from persistent proteolysis to a migration-permissive matrix supporting stable granulation during entry into the proliferative phase, and our transcriptomic contextual analysis likewise identified an inflammatory, protease-associated program typical of chronic pressure-ulcer tissue, supporting that the remodeling markers altered by UFM-hADM are disease-relevant rather than arbitrary endpoints.4,28
The immunomodulatory effect of UFM-hADM provides a mechanistically linked explanation for improved matrix rebuilding and angiogenesis in chronic ulcers, where persistent pro-inflammatory signaling (including TNF-α and IL-6) impairs fibroblast function, disrupts vascularization, and perpetuates tissue damage.10,33 UFM-hADM reduced TNF-α and IL-6 while increasing IL-10, consistent with inflammation-resolution programs and with the concept that decellularized extracellular matrix scaffolds can actively modulate innate immunity toward constructive remodeling. Because angiogenesis requires a permissive extracellular matrix, controlled proteolysis, and balanced pro-angiogenic cues, the observed increases in VEGF, CD31-positive microvessel density, and α-SMA-positive structures are biologically plausible and may be supported by extracellular matrix proteoglycans and glycosaminoglycans that regulate heparan sulfate-interacting growth factor bioavailability in protease-rich wound beds. 34 Together, these coordinated changes across inflammatory, vascular, and matrix markers support restoration of wound-bed competence rather than isolated, unrelated effects.
Perilesional injection is particularly relevant for Stage 3–4 pressure ulcers, where undermining tunnels and irregular dead space can reduce the contact and retention achieved by sheet materials or topical agents.4,28 However, clinical application of injectable ECM scaffolds has been constrained by both source availability and processing challenges. Xenogeneic matrices offer scalable supply but can retain residual species-specific immunogenicity, including the alpha-gal epitope, which can elicit anti-Gal immune recognition and, in some settings, contribute to persistent inflammation or suboptimal remodeling.35,36 Conversely, although human-derived ADM provides species-matched biocompatibility, dense dermal tissue is technically difficult to convert into consistently fine, flowable particles without compromising biological activity, and earlier formulations often relied on coarser particles or viscous pastes requiring larger-bore delivery. 37 Reported micronized human ADM injectables show broad particle-size distributions (e.g., micronized AlloDerm, Cymetra; median 123 µm with 68% spanning 58–593 µm), whereas paste-type micronized ADM used clinically for chronic wounds has been described with substantially larger mean particle sizes (e.g., 664.2 ± 389.9 µm).34,37 A finer and more flowable particulate design can facilitate delivery through narrower-gauge needles and promote more uniform infiltration of undermined planes, thereby increasing matrix–tissue contact and the opportunity for cell–matrix engagement in anatomically complex ulcer.26,38 Micronized paste-type human ADM has therefore been positioned as an ECM micro-scaffold that supports host-cell infiltration and subsequent constructive remodeling, providing a mechanistic backdrop for injectable hADM platforms.39,40 Accordingly, an ultra-fine, flowable ECM format offers a practical means to increase ECM contact within undermined planes that are poorly served by topical retention. 41
In the present ischemia-reperfusion pressure-injury model, perilesional UFM-hADM produced concordant improvements across inflammatory cytokine signaling, angiogenic markers, and ECM remodeling indices, supporting the premise that an injectable ECM scaffold can address multiple, co-dependent barriers that commonly sustain pressure-ulcer chronicity. 42 Because chronic pressure ulcers often fail through coupled deficits in inflammation resolution, neovascular restoration, and matrix rebuilding, the observed convergence across these domains is biologically persuasive and argues against a purely nonspecific space-filling effect. 30 Growth-factor based strategies are mechanistically justified, yet their effectiveness can be attenuated in protease-rich wound environments that limit ligand stability and signaling persistence, and they typically target a narrower biological axis than ECM-based approach.43,44 Moreover, ECM scaffolds can couple structural support with growth factor-binding capacity and immunomodulatory cues, which may be advantageous in protease-rich wound environments where narrowly targeted biologics, including growth-factor based strategies, can show attenuated durability.41,45 Collectively, the present findings show that perilesional administration of UFM-hADM induces coordinated biological responses and improves wound healing in a controlled murine pressure-ulcer model, supporting its rationale as a minimally invasive, human-derived injectable ECM approach. The mechanistic and efficacy-related interpretations of this study are based on the murine model, whereas the two human cases obtained during routine clinical care provide descriptive clinical context regarding the wound course after UFM-hADM treatment. As the present study focused on elucidating the mechanism of action and therapeutic efficacy of UFM-hADM in a controlled pressure-ulcer model, direct comparison with standard therapeutic agents or currently used scaffold-based products was beyond its scope. Given the broad clinical use and diverse application potential of ADM-based materials, further comparative studies will be required to more clearly define the durability, applicability, and relative therapeutic position of UFM-hADM. Collectively, the convergent improvements observed across inflammation resolution, neovascular restoration, and matrix remodeling provide compelling evidence supporting UFM-hADM as a rational, minimally invasive, human-derived injectable ECM therapy for chronic pressure ulcers.
Supplemental material
Supplemental material - Ultra-fine micronized human dermal matrix reprograms the chronic pressure-ulcer microenvironment to accelerate healing
Supplemental material for Ultra-fine micronized human dermal matrix reprograms the chronic pressure-ulcer microenvironment to accelerate healing by Hao Jin, Binna Shin, Daseul Kim, Yeji Seo, Yong Jin Lee, Sang-Myoeng Lee in Journal of Applied Biomaterials & Functional Materials
Footnotes
Acknowledgement
The authors gratefully acknowledge Dr.Jin Young Kim of Kyung Hee University Medical Center Chamjoeun Hospital for his valuable advice on the interpretation of clinical data.
Ethical considerations
The animal study was approved and overseen by Hulux’s Internal Ethics Committee (IACUC) of Hulux-2025-02-001. The two human cases are presented as retrospective descriptive observations derived from routine clinician-directed care using MFDS-approved UFM-hADM. Written informed consent for publication of de-identified clinical information and photographs was obtained directly from each patient.
Author contributions
Conceptualization: [Y.J.L., B.N.S.]; Methodology: [D.S.K, Y.J.S.]; Investigation: [B.N.S., H.J.]; Formal analysis: [D.S.K.]; Resources: [B.N.S.]; Writing: original draft: [B.N.S., H.J., Y.J.L., S.-M.L.]; Writing: review & editing: [H.J., S.-M.L.]; Visualization: [B.N.S., D.S.K.]; Supervision: [Y.J.L., S.-M.L.].
Funding
This work was supported by the Technology Innovation Program (RS-2025-02311948, Development of Multi-Organ Chip Culture Automation and Multimodal Analysis System for Non-Clinical Drug Evaluation) funded by the Ministry of Trade, Industry & Resources(MOTIR, Korea)
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data supporting the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.