
Abstract
Background
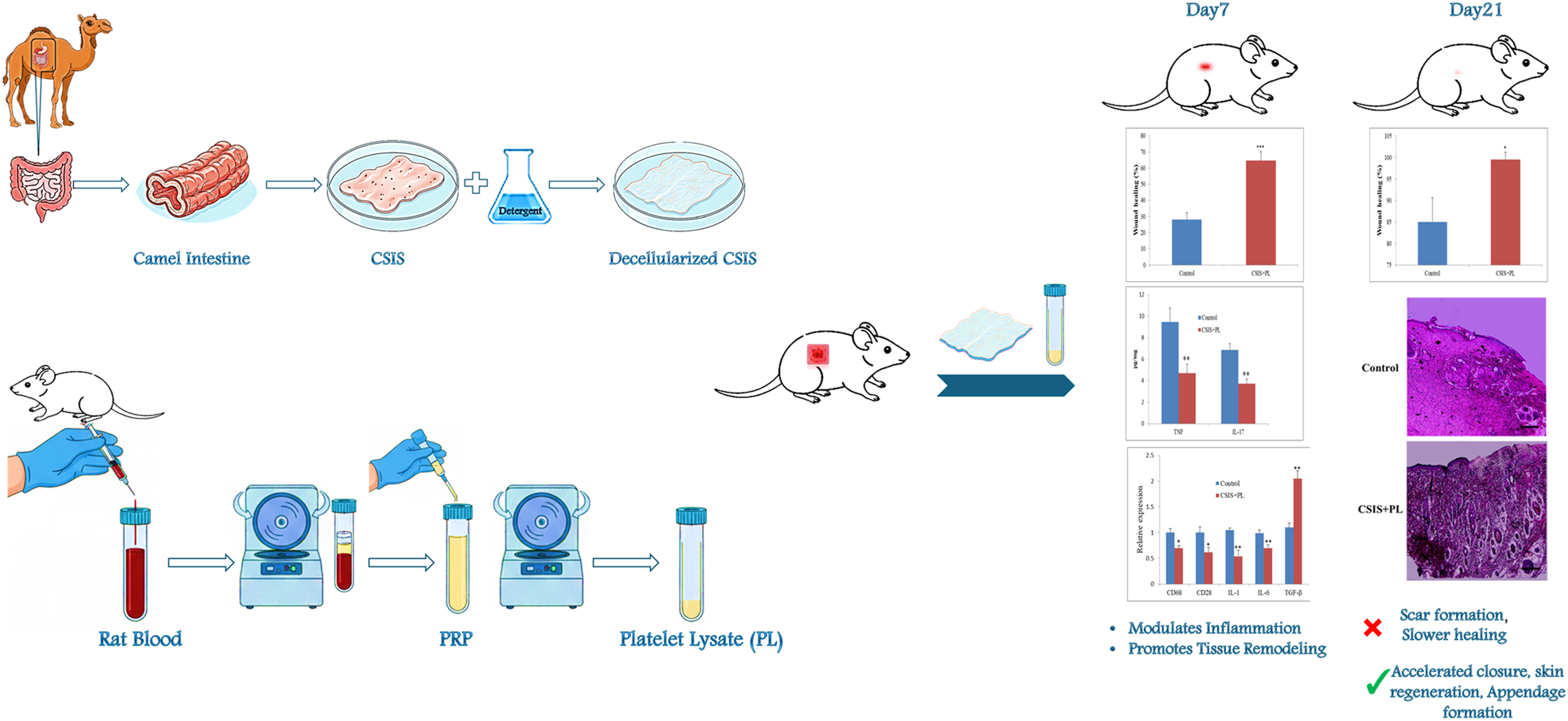
Chronic and extensive skin wounds remain a major clinical challenge requiring advanced regenerative strategies. Decellularized extracellular matrix scaffolds and platelet derivatives support tissue repair by providing essential structural and biological signals. This study evaluated decellularized camel small intestine submucosa (CSIS) alone or combined with platelet lysate (PL) for full-thickness skin wound healing in rats.
Methods
CSIS was prepared via detergent-based decellularization and characterized histologically and via DNA quantification. Following in vitro biocompatibility testing with mesenchymal stem cells (MSCs) using an MTT assay, 1.5 × 1.5 cm full-thickness dorsal wounds in male Wistar rats were randomly assigned to control, CSIS, PL, or CSIS+PL groups. Wound closure was tracked macroscopically on days 7, 14, and 21. Wound tissues were analyzed via histopathology, RT-qPCR for inflammatory genes (CD68, CD28, IL-1, IL-6, TGF-β), and ELISA for TNF-α and IL-17.
Results
Decellularization efficiently removed cellular components while preserving ECM architecture and supported good MSC viability. In vivo, all treated groups showed faster wound closure than control, with near-complete healing in the CSIS+PL group by day 21 (residual area: 1.02 ± 1.24 mm2 vs. 33.55 ± 12.45 mm2 in control, p < 0.05). Histology demonstrated thicker epidermis, more organized dermis, and reduced inflammatory infiltrate in CSIS and especially CSIS+PL wounds. At day 7, CSIS+PL significantly decreased mRNA levels of CD68, CD28, and IL-1, moderately lowered IL-6, and increased TGF-β compared with control. TNF-α and IL-17 protein levels in wound tissue were also significantly reduced (TNF-α: 4.7 ± 0.9 pg/mg; IL-17: 3.7 ± 0.5 pg/mg in CSIS+PL vs. control, p < 0.01).
Conclusion
CSIS is a biocompatible scaffold that supports skin regeneration, and its combination with PL enhances wound healing by modulating inflammation and promoting tissue remodeling. This strategy may represent a promising approach for the treatment of complex cutaneous defects.
Keywords
Highlights
Camel SIS is a novel, biocompatible scaffold for skin tissue engineering. CSIS+PL synergy significantly accelerates macroscopic wound closure in rats. Treatment induces regeneration of hair follicles and sebaceous glands by day 21. Scaffold reduces pro-inflammatory TNF-α and IL-17 protein levels in wounds. CSIS+PL suppresses inflammatory genes while upregulating TGF-β expression.
Introduction
Skin wounds that extend through the full-thickness of the dermis often heal slowly and may result in scar formation, infection, or chronic non-healing lesions.1,2 Such wounds are common after trauma, burns, cancer surgery, or complications of diabetes and vascular disease.2,3 Conventional dressings mainly provide protection and moisture balance, but they do not actively stimulate regeneration of normal skin structure. 4 More advanced strategies, including tissue-engineered skin substitutes and 3D-printed bioinks containing living cells, are being explored for chronic and complex wound management. 5
Wound healing is a dynamic and overlapping process including hemostasis, inflammation, proliferation, and remodeling. 6 Successful repair requires a well-regulated interaction between cells, extracellular matrix (ECM), cytokines and growth factors. 7 When this balance is disturbed by persistent inflammation, healing is delayed, leading to chronicity. 1
Tissue engineering approaches try to restore this balance using biomaterial scaffolds and bioactive molecules.7–9 Decellularized ECM scaffolds derived from different tissues provide a complex mixture of structural proteins and signaling cues while lacking cells that could induce immune rejection. 7 Small intestine submucosa (SIS) is one of the most widely studied ECM materials and has been used clinically for different soft tissue reconstructions.10,11 While porcine and bovine SIS have been extensively characterized, camel-derived SIS offers distinct potential advantages: regional abundance in Middle Eastern and North African markets, and a thicker submucosal collagen network that may provide enhanced mechanical resilience, as previously demonstrated for decellularized camel pericardium. 12 Additionally, camels host fewer zoonotic viruses (approximately 15 species) compared to pigs and cattle (approximately 31 species), potentially lowering cross-species pathogen transmission risk. 13 Histomorphometric studies have detailed the well-defined and robust collagen-rich architecture of the camel jejunum, including its prominent submucosal layer. 14 Despite these potential benefits, camel SIS remains underexplored compared to conventional livestock sources. Establishing its biocompatibility and regenerative efficacy is essential to expand the biomaterial repertoire for regionally adaptable wound care.
Platelet derivatives such as platelet-rich plasma (PRP) and platelet lysate (PL) contain high concentrations of growth factors, cytokines, and extracellular vesicles that can accelerate tissue repair and modulate inflammation. 15 Several studies have shown that platelet products improve healing in bone, cartilage, skin, and other tissues.16,17 Combination of ECM scaffolds with platelet derivatives may therefore provide both structural support and strong biological stimulation. 18
In the present study, we prepared decellularized camel SIS (CSIS) and evaluated its effect on full-thickness skin wound healing in rats, either alone or combined with PL. We hypothesized that CSIS would serve as a biocompatible scaffold and that addition of PL would enhance its regenerative potential by reducing inflammatory responses and promoting tissue remodeling. To test this hypothesis, we analyzed macroscopic wound closure, histopathological changes, inflammatory gene expression, and local cytokine levels at different time points after injury.
Materials and methods
Preparation and decellularization of camel SIS
Small intestines were obtained from adult male Camelus dromedarius (age 4–6 years, weight 350–450 kg), certified disease-free by a veterinary-controlled slaughterhouse in Kerman Province, Iran. Tissues were transported in cold phosphate-buffered saline (PBS; Shellmax, China) within 2 h post-sacrifice. After washing with PBS, the small intestines were cut longitudinally into 10 cm pieces. The submucosal layer was obtained by removing the tunica serosa (outermost layer). The external tunica muscularis and serosa layers were then carefully removed using a surgical scalpel blade. 19
Decellularization was performed using a detergent-based protocol
19
(Figure 1). To determine the optimal treatment parameters, a preliminary optimization step evaluating various concentrations of sodium dodecyl sulfate (SDS; 0.01%, 0.1%, and 0.5%) was conducted. For the definitive protocol, tissues were incubated in the optimized concentration of 0.1% SDS (Merck, Germany) at 37 °C for 3 h under gentle agitation, followed by exposure to 1% Triton X-100 (Merck, Germany) at room temperature for 1 h. After extensive rinsing in distilled water for 90 min, the acellular scaffolds were sterilized by sequential immersion in 70% ethanol (10 min), 90% ethanol (10 min), and PBS containing 3% penicillin-streptomycin (Shellmax, China; 30 min). Scaffolds were subjected to three final 10-min PBS rinses to eliminate residual solvents. Finally, the resulting discs were equilibrated in complete culture medium for 2 h at 37 °C prior to MSC seeding. Decellularization process of camel small intestinal submucosa (CSIS). The left panel shows intact camel submucosa. The middle panel displays the removal of superficial layers. The right panel shows the decellularized CSIS after SDS and Triton X-100 treatment, with the cellular structure largely removed but extracellular matrix preserved.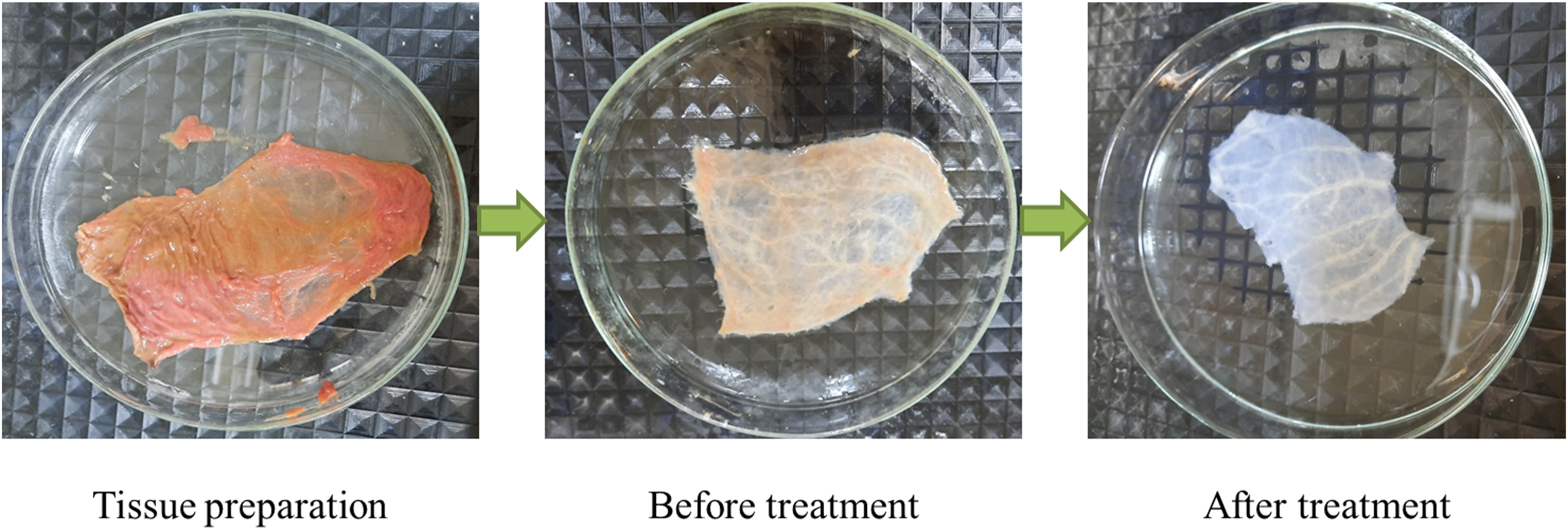
Evaluation of decellularization
To assess the decellularization efficiency, samples were fixed in 10% formalin, embedded in paraffin, sectioned at 5 μm and stained with hematoxylin and eosin (H&E). A pathologist scored nuclear basophilia (cell removal) and architectural preservation on a 5-point scale as previously described. 20 Total DNA was extracted from dried tissue and measured using a NanoDrop spectrophotometry to quantify residual DNA.
Biocompatibility assay
Rat bone marrow–derived mesenchymal stem cells (MSCs) were seeded onto CSIS discs (punched into uniform 8 mm diameters using a sterile biopsy punch to ensure consistent fit within 96-well plates) placed in 96-well plates at 1 × 104 cells/well and cultured in standard medium at 37 °C with 5% CO2. Cell viability at 72 h was evaluated using MTT assay. Absorbance at 570 nm was compared between CSIS and plastic control wells.
Preparation of platelet lysate
Platelet lysate was prepared from pooled citrated whole blood of adult Wistar rats according to a two-step centrifugation protocol. Briefly, blood was centrifuged at 250 g for 15 min to obtain plasma, followed by 1500 g for 15 min to collect PRP. The PRP underwent several freeze–thaw cycles at −80 °C and 37 °C to lyse platelets. The resulting PL, adjusted to approximately 2 × 109 platelets/mL, was aliquoted and stored at −80 °C until use.
Platelet concentration was determined using a Neubauer hemocytometer after the second centrifugation step, with counts verified in triplicate prior to aliquoting. Batch-to-batch consistency was ensured by pooling blood from 6–8 donor rats per preparation. While multiplex profiling of key growth factors (e.g., PDGF-BB, TGF-β1, VEGF) was not performed in this study, published PL preparations at comparable concentrations typically contain 15–40 ng/mL TGF-β1, 5–15 ng/mL PDGF-BB, and 1–5 ng/mL VEGF.21,22 The biological efficacy of the PL used here was functionally validated via accelerated in vivo wound closure and cytokine modulation.
Animal experiment and wound model
All procedures were approved by the institutional Animal Care and Use Committee. Male Wistar rats (8–12 weeks, 180–250 g) were anesthetized with ketamine (50 mg/kg) and xylazine (5 mg/kg). After shaving and disinfecting the dorsal skin, a full-thickness rectangular wound (1.5 × 1.5 cm) was created down to the panniculus carnosus.
Rats were randomly divided into four groups (n = 8 per group initially). Sample size was determined by an a priori power analysis using G*Power software (version 3.1.9.7). 23 Assuming an effect size of 1.5 (derived from pilot data), an α of 0.05, and a desired power of 0.80, the calculation indicated a minimum of 6 animals per group. To account for potential attrition due to post-operative grooming-related scaffold displacement, 8 animals were initially included per group. For macroscopic tracking, all 8 animals per group were followed longitudinally. For histological, molecular, and ELISA analyses, 6 animals per group per timepoint were euthanized (2 animals were excluded due to scaffold displacement, resulting in n = 6 for endpoint analyses).
Wound measurement
Digital photographs were taken immediately after surgery (day 0) and on days 7, 14, and 21. Wound area was quantified via digital planimetry using ImageJ software (v1.54f, NIH, USA) with the “Analyze Particles” plugin to trace wound margins and eliminate geometric approximation errors. The wound healing rate (%) was calculated as follows: wound healing rate = 100 × (original wound area − wound area on day X)/original wound area. 24
Histology
At each time point, rats were euthanized and full-thickness wound tissue with a rim of normal skin was excised and fixed in 10% formalin. Paraffin sections were stained with H&E to evaluate epithelialization, inflammation, fibroplasia and neovascularization using a semi-quantitative scoring system. Scoring was performed by a blinded pathologist using a 5-point scale (0 = absent, 4 = severe) for epithelial thickness, inflammatory infiltrate density, collagen organization, and neovascularization.
Real-time PCR
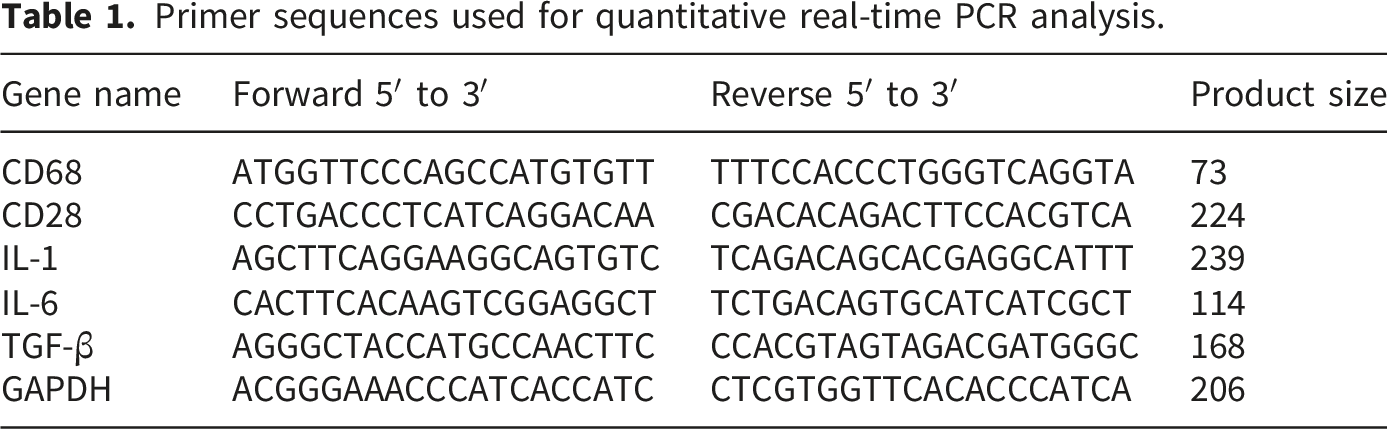
Primer sequences used for quantitative real-time PCR analysis.
ELISA
At day 7, a portion of wound tissue was homogenized in lysis buffer, and supernatants were collected after centrifugation. Concentrations of TNF-α and IL-17 were measured using commercial ELISA kits according to the manufacturer’s instructions (Karmania Pars Gene Company, Kerman, Iran). Cytokine concentrations were normalized to total protein content and expressed as pg/mg total protein.
Statistical analysis
Data are presented as mean ± standard deviation. Differences between multiple groups were analyzed by one-way ANOVA followed by Tukey’s post-hoc test for pairwise comparisons. For within-group comparisons between day 14 and day 21, a paired t-test was used. A p-value < 0.05 was considered statistically significant. As Tukey’s post-hoc test inherently controls the family-wise error rate for pairwise comparisons, no additional correction for multiple testing was applied, aligning with current standards for reporting inflammatory markers in wound healing research.25,26
Results
Properties of decellularized CSIS
H&E staining of native SIS showed abundant nuclei in mucosal and submucosal layers (Figure 2), whereas decellularized CSIS was almost completely devoid of cells, with preserved collagen architecture. Nuclear basophilia score significantly decreased after decellularization, while architectural score remained high (p < 0.01). Residual DNA content was reduced to less than 50 ng/mg dry weight, indicating efficient cell removal. Microscopic H&E staining of camel small intestinal submucosa before and after decellularization (magnification 100×, Scale bars: 150 μm). The top-left panel shows untreated submucosa. The top-right panel shows treatment with 0.01% SDS, with insufficient decellularization. The bottom-left panel (0.1% SDS) shows optimal balance of cell removal and matrix preservation. The bottom-right panel (0.5% SDS) shows disruption of extracellular matrix architecture.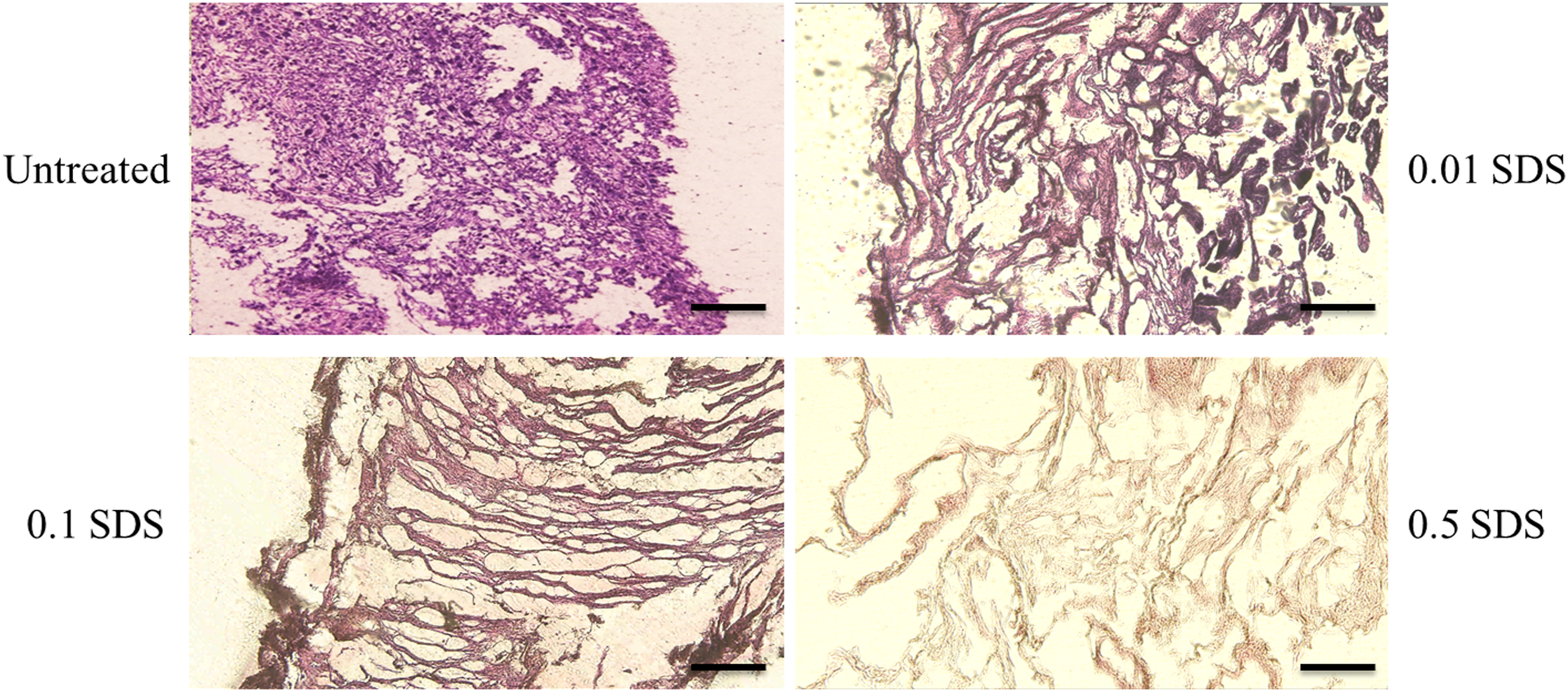
MSCs seeded on CSIS remained viable and spread on the scaffold surface. MTT assay showed no significant difference in cell metabolic activity between CSIS and plastic control wells at 72 h, confirming good biocompatibility (Figure 3). Biocompatibility of CSIS with mesenchymal stem cells. MTT assay showing comparable metabolic activity of MSCs on CSIS and tissue-culture plastic. Data are mean ± SD.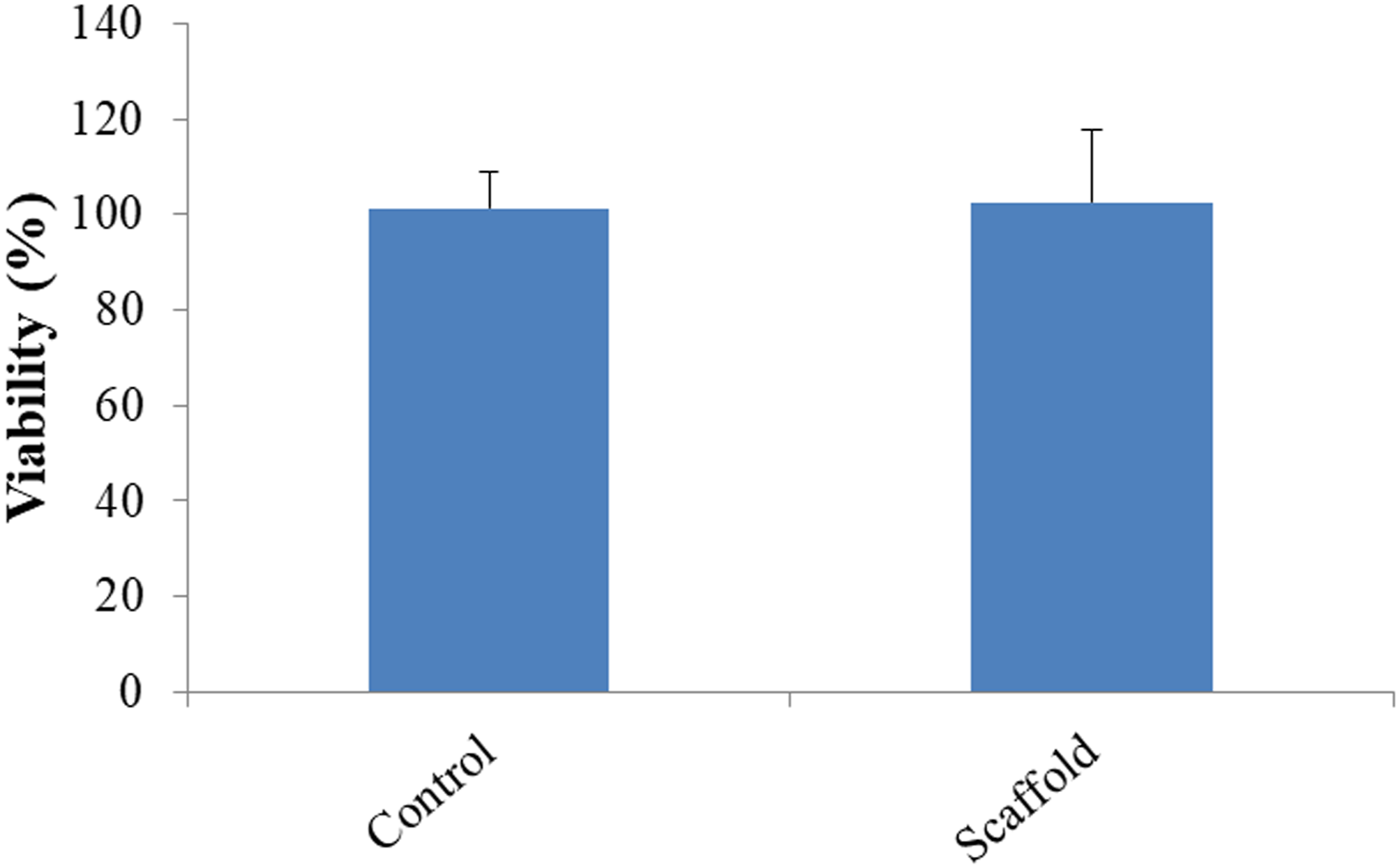
Macroscopic wound healing
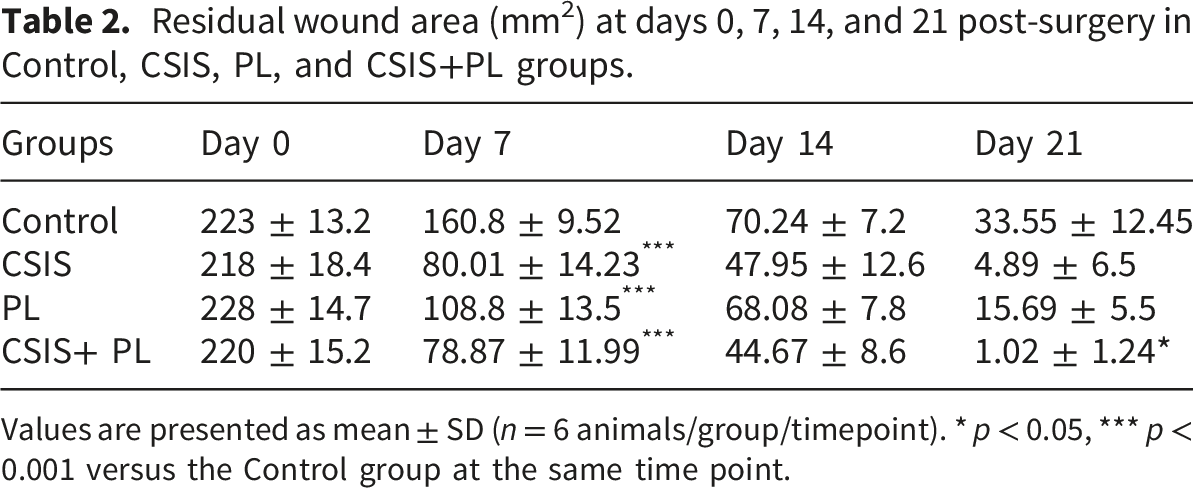
All treated groups showed faster wound contraction than the control at all time points (Figure 4(a)). On day 7, healing rates were significantly higher in CSIS, PL and CSIS+PL groups compared with the control (p < 0.001) (Figure 4(b)). By day 21, the CSIS+PL group reached almost complete closure with the smallest residual wound area, significantly lower than control (1.02 ± 1.24 mm2 vs. 33.55 ± 12.45 mm2; p < 0.05), representing 99.5% wound closure, while CSIS and PL groups showed intermediate values (Table 2). Macroscopic wound healing. (a) Representative images of full-thickness dorsal wounds at Days 0, 7, 14 and 21 in Control, CSIS, PL and CSIS+PL groups. (b) Quantitative wound healing rate over time. Data are mean ± SD. *p < 0.05, ***p < 0.001 versus control. Residual wound area (mm2) at days 0, 7, 14, and 21 post-surgery in Control, CSIS, PL, and CSIS+PL groups. Values are presented as mean ± SD (n = 6 animals/group/timepoint). * p < 0.05, *** p < 0.001 versus the Control group at the same time point.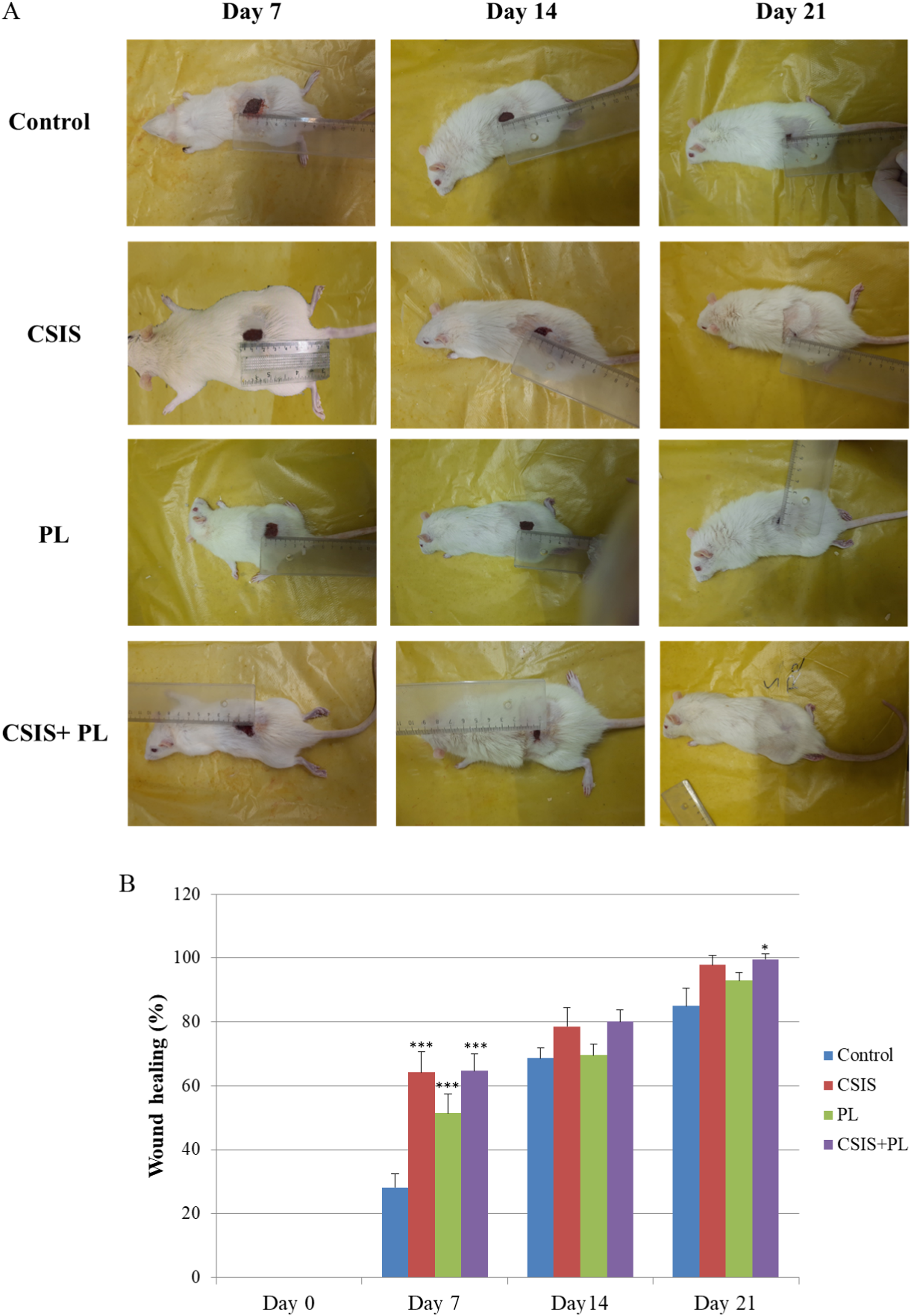
Histological findings
At Day 14, control wounds exhibited an incomplete, thin epithelium and a dense inflammatory cell infiltrate composed mainly of neutrophil- and macrophage-like cells within loose granulation tissue. CSIS wounds showed a thicker, more continuous epithelium and a better-organized dermis with moderate inflammation. PL wounds demonstrated continuous epithelial coverage and marked neovascularization, although dermal organization was less uniform. CSIS+PL wounds displayed the most advanced healing pattern, with an almost complete epidermal layer, a compact dermis, reduced numbers of neutrophil-like cells, and early formation of hair follicle- and sebaceous gland-like structures.
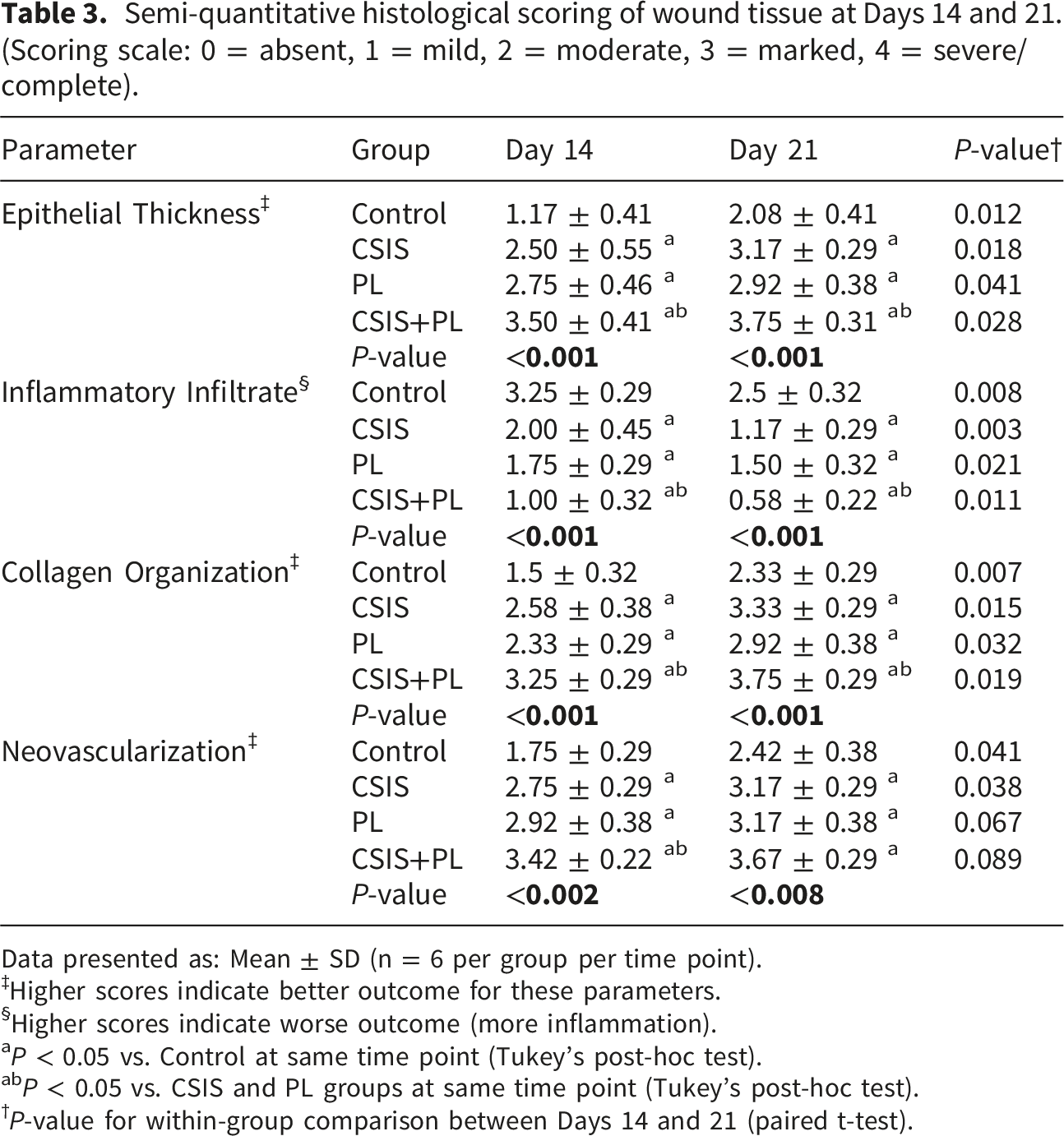
By Day 21, control wounds retained discontinuous epithelium and persistent inflammation. Both CSIS and PL groups achieved near-complete epithelialization; however, dermal reorganization and appendage formation were more pronounced in the CSIS group. The CSIS+PL group most closely approximated normal skin architecture, exhibiting a fully stratified epidermis, dense organized dermis, developing hair follicles and sebaceous gland-like structures, and minimal inflammatory cells (Figure 5 and Table 3). Histological evaluation of wound healing. Representative H&E-stained sections from Day 14 and Day 21 wounds (magnification 100×, Scale bars: 150 μm). CSIS+PL treatment shows accelerated re-epithelialization, improved dermal organization and reduced inflammatory infiltration compared with the control and single-treatment groups. Semi-quantitative histological scoring of wound tissue at Days 14 and 21. (Scoring scale: 0 = absent, 1 = mild, 2 = moderate, 3 = marked, 4 = severe/complete). Data presented as: Mean ± SD (n = 6 per group per time point). ‡Higher scores indicate better outcome for these parameters. §Higher scores indicate worse outcome (more inflammation). aP < 0.05 vs. Control at same time point (Tukey’s post-hoc test). abP < 0.05 vs. CSIS and PL groups at same time point (Tukey’s post-hoc test). †P-value for within-group comparison between Days 14 and 21 (paired t-test).
Gene expression analysis
CD68 is a canonical marker of macrophage infiltration, and CD28 is a key co-stimulatory receptor driving early pro-inflammatory T-cell responses. 27 The pro-inflammatory cytokines IL-1, IL-6, and TNF-α amplify leukocyte recruitment and fibroblast activation, 28 while IL-17 sustains neutrophilic inflammation and can delay resolution. 29 Conversely, TGF-β orchestrates extracellular matrix deposition, myofibroblast differentiation, and the transition from the inflammatory to the proliferative phase. 30
At day 7, qPCR (Figure 6) showed that CD68 and CD28 mRNA levels were significantly reduced in the CSIS+PL group compared with control (p < 0.05), indicating decreased macrophage and T cell activation. CSIS and PL alone showed moderate but non-significant reductions (Figure 6(a)). Gene expression analysis of wound tissue at Day 7. Relative mRNA expression of inflammatory (CD68, CD28, IL-1, IL-6) and remodeling-associated (TGF-β) markers measured by qPCR and normalized to GAPDH. Data are expressed as fold change versus control (mean ± SD). *p < 0.05, **p < 0.01 versus control.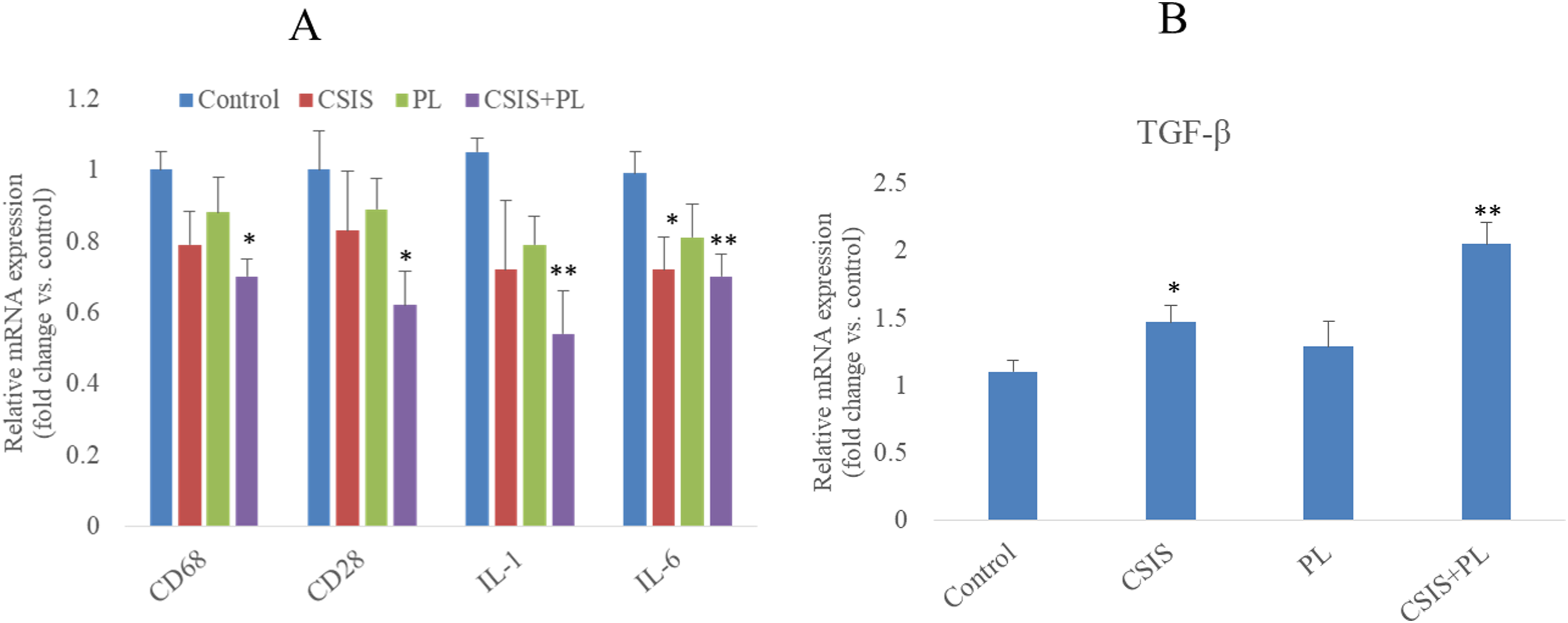
The pro-inflammatory cytokine IL-1 was significantly downregulated in CSIS+PL wounds (p < 0.01), whereas CSIS and PL produced smaller decreases. IL-6 expression showed a mild reduction in CSIS and CSIS+PL groups, while PL was closer to control. TGF-β expression (Figure 6(b)), in contrast, was significantly increased in CSIS and CSIS+PL groups compared with the control (p < 0.05), reflecting enhanced matrix remodeling activity.
Cytokine levels by ELISA
Consistent with qPCR data and as shown in Figure 7, TNF-α and IL-17 concentrations in wound tissue at day 7 were highest in the control group. CSIS and PL treatments significantly reduced both cytokines (p < 0.05), and the CSIS+PL group showed the greatest decrease (p < 0.01 vs control). Inflammatory cytokine levels in wound tissue. TNF-α and IL-17 protein concentrations measured by ELISA at Day 7. CSIS and PL treatments reduce cytokine levels, with greatest reduction in the CSIS+PL group. Data are mean ± SD. *p < 0.05, **p < 0.01 versus control.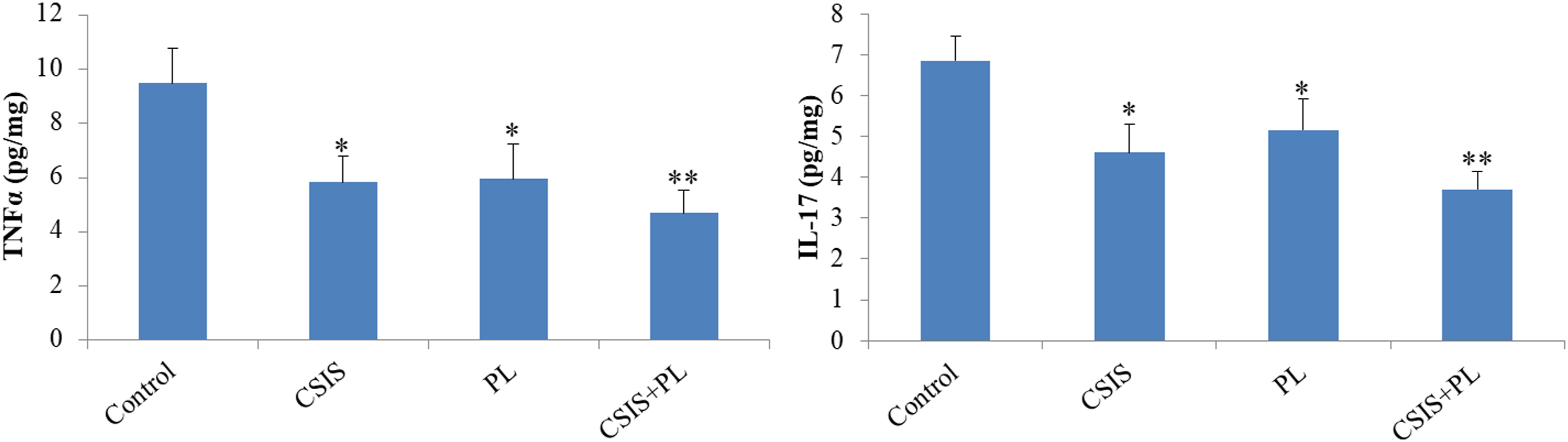
Discussion
The present study demonstrates that decellularized camel small intestine submucosa (CSIS) is a biocompatible extracellular matrix scaffold capable of accelerating full-thickness skin wound healing, with substantially superior regenerative outcomes when combined with platelet lysate (PL). This work contributes to a growing body of evidence that composite biomaterial strategies pairing structurally intact native ECM with concentrated bioactive factors establish a pro-regenerative microenvironment distinct from traditional repair-focused approaches.
Decellularization and ECM architecture as a foundation
The preservation of native ECM architecture alongside efficient cellular elimination is foundational to CSIS efficacy. Our findings align with contemporary frameworks for decellularized tissue characterization: nuclear basophilia reduction below established immunogenicity thresholds (DNA <50 ng/mg dry weight) coupled with maintained collagen and proteoglycan organization. Recent comparative work on dECM-based composite scaffolds demonstrates that intact ECM composition, particularly the retention of tissue-specific signaling cues and mechanical properties drives superior outcomes compared to synthetic alternatives lacking these biochemical and structural templates. The biocompatibility confirmed by MSC viability assays extends recent observations that decellularized tissues, through mechanisms not yet fully elucidated, provide permissive microenvironments for fibroblast recruitment, migration, and ECM deposition without triggering robust immune rejection. Critically, the architectural integrity of CSIS likely preserves mechanosensitive elements integrin-binding sites, growth factor sequestration domains, and collagen-based topography that mechanically literate cells, including macrophages, can interrogate to guide phenotypic responses independent of cytokine signaling alone.31,32
Platelet lysate as a growth factor amplifier
Platelet lysate delivers concentrated growth factors (PDGF, TGF-β, VEGF, EGF) at supraphysiological concentrations. 17 Recent mechanistic work demonstrates that PL-mediated healing occurs through direct STAT3 activation in dermal fibroblasts and endothelial cells, suppressing pro-inflammatory IL-6 while simultaneously upregulating collagen I synthesis and promoting the angiogenic transcriptional program. 33 The JAK2/STAT3 pathway, activated by IL-10 secreted by M2 macrophages and reinforced by PL-derived growth factors, emerges as a critical molecular axis regulating the transition from inflammatory to pro-regenerative phenotypes.33,34 This finding extends classical understanding of PL in wound healing: beyond providing passive growth factor support, PL actively reprograms cellular signaling cascades toward tissue repair outcomes. 35 When impregnated into CSIS, these factors undergo spatially regulated release within a collagen-rich matrix, creating sustained bioavailability throughout the critical proliferative window a spatial organization that likely exceeds the efficacy of soluble factor administration alone.33,35,36
Immune modulation through coordinated macrophage polarization
The significant reductions in CD68 and CD28 mRNA, coupled with suppressed TNF-α and IL-17 protein, indicate that CSIS+PL dampens the canonical pro-inflammatory immune response without eliminating it entirely. This selective immune modulation characterized by reduced M1 macrophage infiltration and pro-inflammatory cytokine production reflects a growing appreciation for the temporal dynamics of macrophage plasticity in wound healing. Recent epigenetic and transcriptomic analyses reveal that macrophage polarization is not a binary M1/M2 transition but rather a tunable continuum, with distinct gene expression subprograms responding independently to environmental signals.37–39 In the present study, the maintained or modestly reduced IL-6 expression alongside robust TGF-β upregulation is consistent with selective suppression of early pro-inflammatory signaling while preserving cytokines essential for fibroblast recruitment and matrix synthesis. This kinetic profile aligns with optimal immune resolution pathways in which transient inflammation is necessary for debris clearance but must be rapidly suppressed to avoid pathological persistence.28,40
Proposed mechanistic framework & limitations
While our data demonstrate accelerated closure and cytokine modulation with CSIS+PL, direct molecular validation of macrophage polarization (e.g., via phospho-flow cytometry for CD206/CD86 or STAT3/STAT6 activation kinetics) and MMP/TIMP dynamics was beyond the scope of this study. However, the observed cytokine shifts and histological outcomes align with literature suggesting that dECM scaffolds combined with platelet derivatives promote a pro-regenerative microenvironment through growth factor-mediated signaling and macrophage phenotype modulation.14,21,22,28,33,37,39,40 At the molecular level, STAT3 and STAT6 transcription factors, activated downstream of IL-4, IL-13, and IL-10 signaling, are known to coordinate M2 macrophage differentiation and maintain anti-inflammatory gene expression programs.14,21,22 The elevated TGF-β in CSIS+PL wounds likely amplifies this polarization circuit, while the progressive stiffening of the ECM may provide negative feedback to limit excessive macrophage-driven inflammation.25,26,41,42 These mechanisms remain a working hypothesis warranting direct experimental validation. Additionally, the absence of a heterologous SIS control (e.g., porcine) limits definitive attribution of camel-specific ECM advantages. Furthermore, while the MTT assay confirmed metabolic viability, the absence of high-resolution morphological assessments (e.g., scanning electron microscopy or confocal live/dead staining) limits the evaluation of 3D cell-scaffold spatial interactions, which will be incorporated in our immediate future studies. Finally, because the study concludes at day 21, longer-term assessment (60–90 days) is required to confirm true skin appendage regeneration versus transient structures, and to evaluate long-term scar quality and tensile strength.
Synergistic effects on tissue architecture and regeneration
The presence of hair follicles, sebaceous glands, and densely organized dermal collagen in CSIS+PL-treated wounds by day 21 is remarkable and biologically significant. Spontaneous regeneration of skin appendages in adult full-thickness wounds is exceptionally rare outside specialized experimental contexts or during fetal development, where a different inflammatory trajectory and delayed ECM deposition favor scar-free healing. The appearance of appendage structures suggests that CSIS+PL created permissive conditions for not merely wound closure or scar formation, but for restoration of tissue complexity and architectural fidelity. This regenerative rather than reparative phenotype likely reflects both the intact ECM template (which preserves spatial organization cues for epithelial-mesenchymal interactions) and the growth factor milieu sustained by PL, particularly TGF-β-mediated fibroblast-keratinocyte crosstalk and VEGF-driven angiogenesis that re-establishes vascular supports for long-term tissue viability. 43 While other bioactive skin patches, including collagen hydrogels with fibroblast-conditioned medium or PRP-based constructs, have improved wound closure and epidermal differentiation in ovine full-thickness wounds, they generally rely on freshly harvested cells and more complex preparation than our acellular CSIS+PL dressing. 44
Histologically, the maturation of collagen fiber organization transitioning from disorganized granulation tissue toward bundled, aligned type I collagen with preserved elastin indicates active remodeling orchestrated by myofibroblasts and regulated by the MMP/TIMP balance. The modest IL-6 reduction in CSIS+PL wounds alongside increased TGF-β supports this interpretation: IL-6 can bias matrix deposition toward type III collagen and immature fibrosis, while TGF-β promotes both myofibroblast differentiation and the shift from type III to type I collagen, enhancing tissue tensile strength and mechanical durability.
Clinical translation and future directions
Despite these methodological constraints, the results suggest a clear translational pathway. CSIS is a renewable, regionally abundant biomaterial with demonstrated biocompatibility and cost-effectiveness relative to acellular dermal matrices derived from cadaveric human skin or animal-derived products. The combination with PL already in routine clinical use across orthopedic and wound care specialties circumvents the need for novel biomolecule development or complex manufacturing. Compared with commercially available products, CSIS offers advantages: unlike human-derived acellular dermal matrices (AlloDerm®), CSIS can be produced in unlimited quantities from an abundant animal source; compared with porcine SIS products (Oasis®), CSIS may have different degradation kinetics, though direct comparative studies are needed. Regulatory pathways for decellularized tissue products are increasingly established, facilitating preclinical-to-clinical translation. Future investigations should encompass: (1) single-cell RNA sequencing to resolve macrophage heterogeneity and state transitions during healing; (2) phospho-flow cytometry for STAT3/STAT6 activation kinetics; (3) biomechanical testing to assess tissue integrity and scar minimization; (4) dose-response and optimization studies of PL loading and CSIS thickness; (5) evaluation in clinically relevant comorbidity models (diabetic, immunocompromised, aged animals); and (6) mechanism studies examining integrin-independent mechanosensing in wound macrophages using genetic models and mechanotransduction inhibitors. The potential synergy between CSIS and PL, a composite that pairs durable structural support with sustained bioactive signaling warrants investigation in other tissue repair contexts, including orthopedic, cardiac, and mucosal applications.
Conclusion
This work demonstrates that decellularized camel small intestine submucosa, when loaded with platelet lysate, establishes a pro-regenerative microenvironment capable of accelerating full-thickness skin wound healing through coordinated modulation of inflammation, macrophage polarization, and tissue remodeling. The proposed mechanistic basis involves synergistic contributions from intact ECM architecture (providing structural templating and mechanosensing cues), growth factor bioavailability (potentially activating STAT3/STAT6 and downstream regenerative pathways), and selective immune suppression (favoring M2 macrophage phenotypes and anti-inflammatory mediator release). These findings support further investigation of CSIS+PL as a therapeutic strategy for complex cutaneous defects and establish a biological rationale for combining native biomaterials with concentrated growth factor preparations in tissue engineering.
Footnotes
Acknowledgments
The authors would like to acknowledge RUMS’s support and contributions for providing financial assistance for this research. Additionally, they express their gratitude to the Immunology of Infectious Diseases Research Center for providing the necessary facilities and resources for conducting the experiments.
Ethical considerations
The ethical review board of Rafsanjan University of Medical Sciences approved this study (Ethics Code: IR. RUMS.REC.1398.155).
Consent for publication
Authors have given their consent for publication.
Author contributions
Aliakbar Yousefi-Ahmadipour: Conceptualization, Methodology, Investigation, Formal analysis, Writing – Original Draft, Writing – Review & Editing, Supervision, Funding Acquisition. Afsaneh Mirzahosseini-Pourranjbar: Investigation, Data Curation, Formal analysis, Writing – Original Draft. Fatemeh Asadi: Methodology, Validation, Investigation, Resources. Morteza Khademolhosseini: Methodology, Project Administration, Resources. Mohammad Kazemi Arababadi: Conceptualization, Methodology, Resources. Mohammad Reza Mirzaei: Methodology, Investigation, Resources. Manira Maarof: Validation, Writing – Review & Editing, Supervision.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Rafsanjan University of Medical Sciences funded this project (Funding No. 98101).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting this study’s findings are available upon request from the corresponding author.