
Abstract
Objective
Furcal perforations are iatrogenic complications which compromise the biological and mechanical integrity of endodontically treated teeth. Although calcium silicate-based materials are widely used for perforation repair, their ability to restore fracture resistance remains unclear. This study aimed to evaluate the fracture strength of mandibular molars with simulated furcal perforations repaired using Bio MTA+ or calcium-enriched mixture (CEM).
Method
Seventy-six extracted human mandibular molars were randomly allocated into four groups (n = 19): negative control (no perforation), positive control (perforation without repair), Bio MTA+ (perforation repaired with Bio MTA+) and CEM (perforation repaired with CEM). Standardised root canal treatments were performed on all specimens, followed by perforation and repair procedures where applicable. Fracture strength was measured using a universal testing machine at a crosshead speed of 1 mm/min. The data were analysed using one-way ANOVA and Tukey’s HSD test.
Results
A statistically significant difference was observed among the groups (F(3,72) = 52.362, p < 0.001). The negative control group exhibited the highest fracture strength values, whereas the positive control group presented the lowest. Both Bio MTA+ and CEM groups demonstrated significantly higher fracture strength than the positive control group (p < 0.05), but significantly lower values than the negative control group (p < 0.05). No statistically significant difference was found between Bio MTA+ and CEM (p = 0.773).
Conclusion
Furcal perforations significantly reduce the fracture resistance of endodontically treated teeth. Repair with calcium silicate–based materials improves mechanical strength but does not restore it to the level of endodontically treated teeth without perforation. Bio MTA+ and CEM demonstrated comparable performance and may be considered suitable options for furcal perforation repair.
Keywords
Introduction
The formation of mechanical or pathological communication between the root canal system and the external root surface is defined as perforation. 1 Furcal perforations are iatrogenic complications that may occur during access cavity preparation, particularly when canal orifices are difficult to localise, during retreatment procedures or during post-space preparation following endodontic treatment.2,3 Such complications are clinically significant, as perforated teeth are generally associated with a poorer prognosis, 4 particularly given that a previous study reported that mandibular molars are involved in more than half of all perforation cases. 5 The presence of a perforation increases the risk of microbial contamination, which may lead to inflammation and subsequent bone loss. In addition to biological consequences, perforations may compromise the structural integrity of the tooth. Compromised tissue integrity may alter the distribution of functional forces; consequently, the susceptibility to fracture may increase due to tissue loss, potentially resulting in tooth extraction. 6 The location and size of the perforation, as well as the duration of exposure to the oral environment, are critical factors affecting long-term survival. Therefore, early detection and prompt management are essential, involving the sealing of the perforation site, the timely completion of root canal treatment and definitive restoration to minimise microbial contamination and mechanical weakening. 3
Endodontically treated teeth are known to exhibit reduced fracture resistance due to the loss of tooth structure during access cavity preparation, canal instrumentation and restorative procedures. In such teeth, the remaining dentine is subjected to altered stress distribution, making them more susceptible to fracture under functional loading.7,8 Furcal perforations may further exacerbate this condition by creating areas of stress concentration and structural discontinuity within the tooth. Consequently, the selection of an appropriate repair material plays a critical role in restoring the mechanical integrity of the compromised tooth structure. 1
The mechanical performance of repair materials is closely related to their ability to interact with dentine and to influence stress distribution within the tooth structure. Ideally, a repair material should possess mechanical properties, particularly elastic modulus, similar to those of dentine to allow more uniform stress transfer under functional loading.3,6,9 Materials with significantly different mechanical properties may lead to stress concentration at the interface, increasing the risk of structural failure. A previous finite element study 9 reported that materials with dentin-like elastic moduli may improve the homogeneity of stress distribution and fracture resistance by promoting a more unified biomechanical behaviour of the restored tooth, whereas materials with markedly different elastic moduli, such as gutta-percha, have been associated with less favourable stress distribution patterns. Mineral trioxide aggregate (MTA) has been extensively investigated and has become a widely accepted material for perforation repair. It possesses several advantageous properties, including high alkalinity, antibacterial activity, dimensional stability and excellent sealing ability. However, its clinical use has been limited by certain drawbacks, such as a prolonged setting time and the potential for tooth discolouration. 10 Calcium silicate-based materials have also been suggested to contribute to the reinforcement of a weakened tooth structure due to their bioactive nature and favourable mechanical characteristics.6,9 However, the extent to which these materials can restore the fracture resistance of teeth with structural defects, such as furcal perforations, remains unclear.
Bio MTA+ is a bioceramic repair material characterised by a relatively rapid setting time, potentially overcoming the clinical limitations of traditional MTA. Its powder comprises of calcium carbonate, silicon dioxide, aluminium oxide and a calcium–zirconium complex, and distilled water is used as the mixing liquid. Once set, Bio MTA+ exhibits an alkaline pH, adequate radiopacity and low solubility. 11
Calcium-enriched mixture (CEM) is another calcium silicate-based material that can be used for indications similar to those of MTA. Although its chemical composition differs, it demonstrates comparable physical and biological properties.10,12 In addition, its cost-effectiveness has contributed to its increasing use in clinical practice. CEM powder contains calcium oxide, sulphur trioxide, phosphorus pentoxide, silicon dioxide, trace amounts of sodium oxide, magnesium oxide and chloride. It is mixed with a water-based solution.10,13
Previous studies have focused on the sealing ability, microleakage, bond strength and biological responses associated with these materials when used for perforation repair.14–16 However, limited information is available regarding their influence on the fracture resistance of teeth with furcal perforations. Considering the importance of mechanical integrity for the long-term survival of endodontically treated teeth, evaluating the reinforcing potential of these materials is of substantial clinical relevance. To the best of our knowledge, no previous study has directly compared the effect of Bio MTA+ and CEM on the fracture resistance of mandibular molars with furcal perforations. Therefore, the present study provides novel information regarding the reinforcing potential of these contemporary calcium silicate–based biomaterials in a clinically relevant perforation model.
Accordingly, the aim of this study was to compare the fracture strength of endodontically treated mandibular molars with simulated furcal perforations repaired using Bio MTA+ or CEM. The null hypothesis was that there would be no significant difference in fracture strength among the experimental and control groups.
Materials and methods
Study design and sample size calculation
This in-vitro study is reported in accordance with the Preferred Reporting Items for Laboratory Studies in Endodontology (PRILE) guidelines. 17 The required sample size was determined through a power analysis using the G*Power 3.1.9.2 software (Heinrich Heine University, Dusseldorf, Germany). To determine a difference at a medium effect size (f = 0.40) with a power of 80% at a 0.05 error level (α = 0.05) across four groups, 76 teeth were included in the study, with equal specimens in each group (n = 19).
Specimen selection and preparation
In this study, the preparation of the samples and the applied tests were performed by a single experienced operator. Seventy-six extracted human mandibular molars were obtained from patients who underwent tooth extraction for non-research therapeutic reasons. The teeth were immersed in 5.25% sodium hypochlorite (NaOCl) to remove soft tissue remnants and for debridement. Subsequently, they were stored in thymol solution for 48 h for disinfection and in 4°C distilled water until use. The teeth were examined using a stereomicroscope, and periapical radiographs were taken from the buccolingual and mesiodistal angles. Teeth were included if they had no root canal treatment; no internal or external resorption; no calcified root canals; no caries, cracks or fractures; no fused or extra roots; complete root development and root canal curvatures of less than 10 degrees. To enhance dimensional standardisation, the mesiodistal and buccolingual widths of the teeth were measured at the cemento–enamel junction level using a digital calliper. Teeth with average mesiodistal and buccolingual dimensions of approximately 9 mm–10 mm were included in the study. Specimens with substantially smaller dimensions were excluded to minimise the possibility of including second or third molars and to reduce anatomical variability among the samples.
Root canal preparation and obturation
The crowns of the teeth were removed to a level of 4 ± 1 mm from the cemento–enamel junction to the furcation area so the distances to the furcation were standardised. The access cavity was prepared with diamond burs. The working length of the canals was determined so the tip of a #10 K-type file was 0.5 mm shorter than the length observed at the apex of the root. The root ends were coated with wax to create a closed-end system. Using the Protaper Next rotary file system (Dentsply Maillefer, Ballaigues, Switzerland), the mesial canals were enlarged to X2 and the distal canals to X3. Two millilitres of 2.5% NaOCl irrigation were used for irrigation between each file using 30-gauge side-perforated needles (Ultradent Products, Inc., South Jordan, UT, USA). In accordance with the manufacturer’s recommendations, a new file system was used after every four preparations. After drying with paper points, the canals were filled using the single-cone technique with corresponding X2 and X3 gutta-percha cones (Dentsply Sirona, Charlotte, NC, USA) and AH Plus sealer (Dentsply De Trey GmbH, Konstanz, Germany). After removing excess gutta-percha, the access cavity was covered with temporary filling material (Cavit G, 3M Deutschland GmbH, Seefeld, Germany) and kept in a 100% humid environment at 37°C for 24 h to allow the sealer to set.
Experimental groups and perforation procedure
The teeth were randomly allocated into four groups (n = 19) using a computer-generated randomisation method: Group 1: No further intervention Group 2: Furcal perforation, no repair Group 3: Furcal perforation, repair with Bio MTA+ (Cerkamed, Stalowa Wola, Poland) Group 4: Furcal perforation, repair with CEM (Bionique Dent, Tehran, Iran)
Composition and key characteristics of the tested biomaterials.
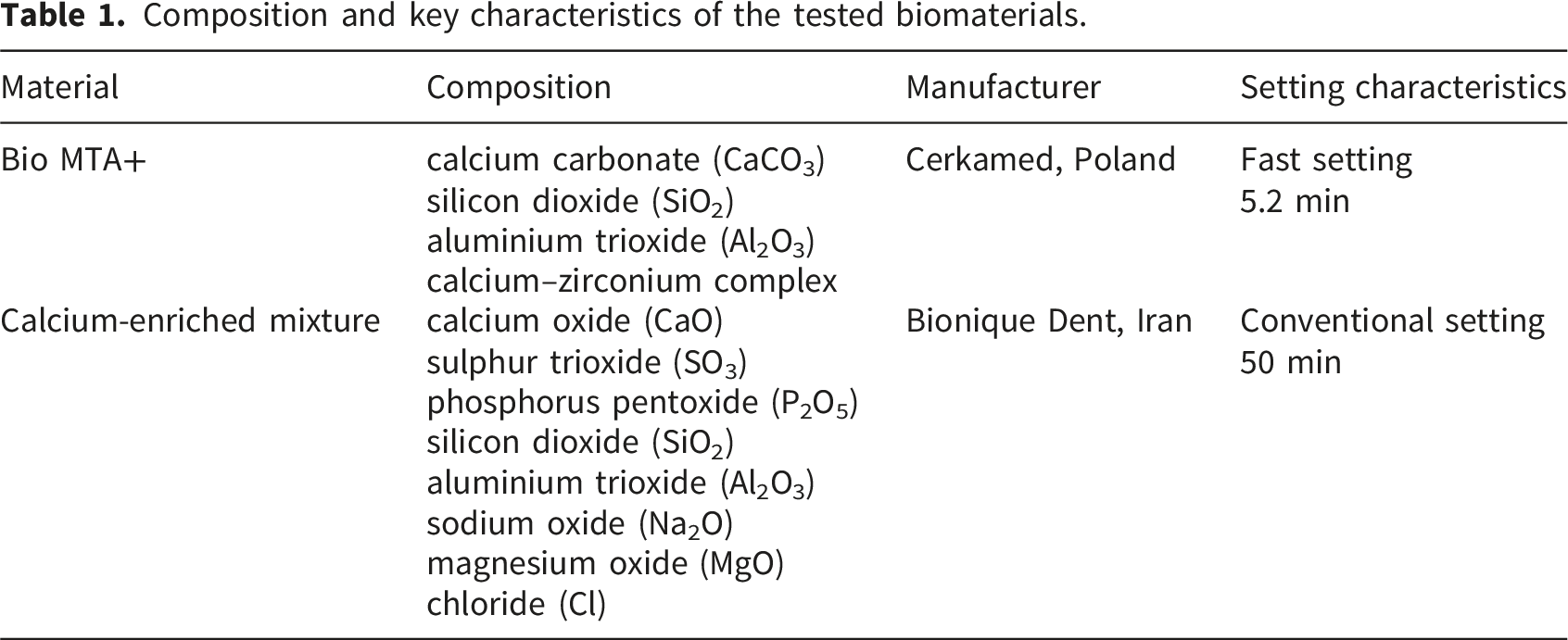
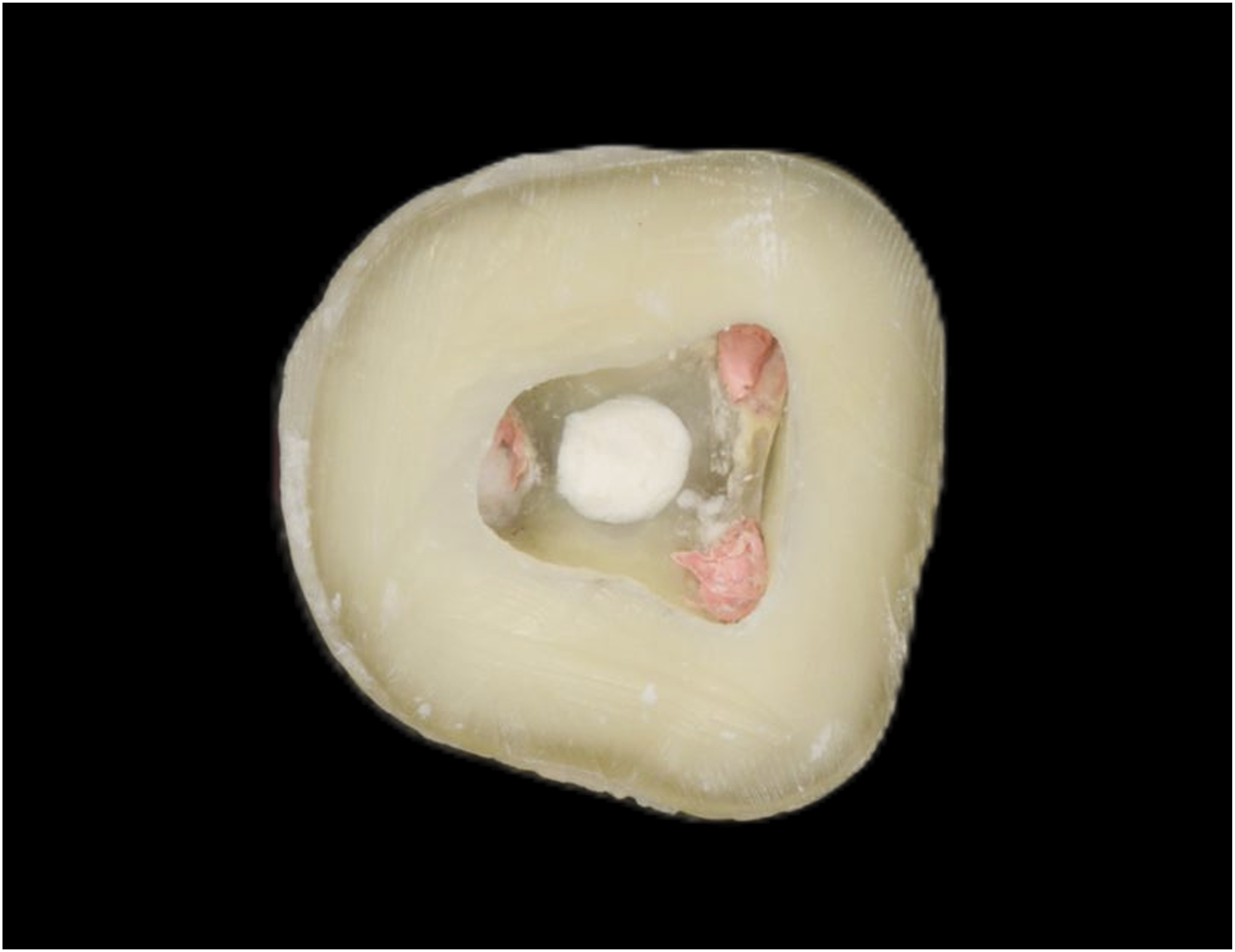
Representative image showing the creation of a furcal perforation and its repair using calcium silicate-based biomaterials.

Radiographic image confirming the integrity of the furcal perforation repair, root canal treatment, and coronal restoration.
Simulation of periodontal ligament and embedding
A condensation polysiloxane impression material (Oranwash VL; Zhermack, Badia Polesine, Italy) was applied to the root surface of each tooth to mimic the periodontal ligament and better approximate clinical conditions. The samples were embedded in acrylic blocks (Imicryl, Konya, Turkey) up to 1 mm apical to the cementoenamel junction, leaving the furcation region slightly exposed.
Fracture strength testing
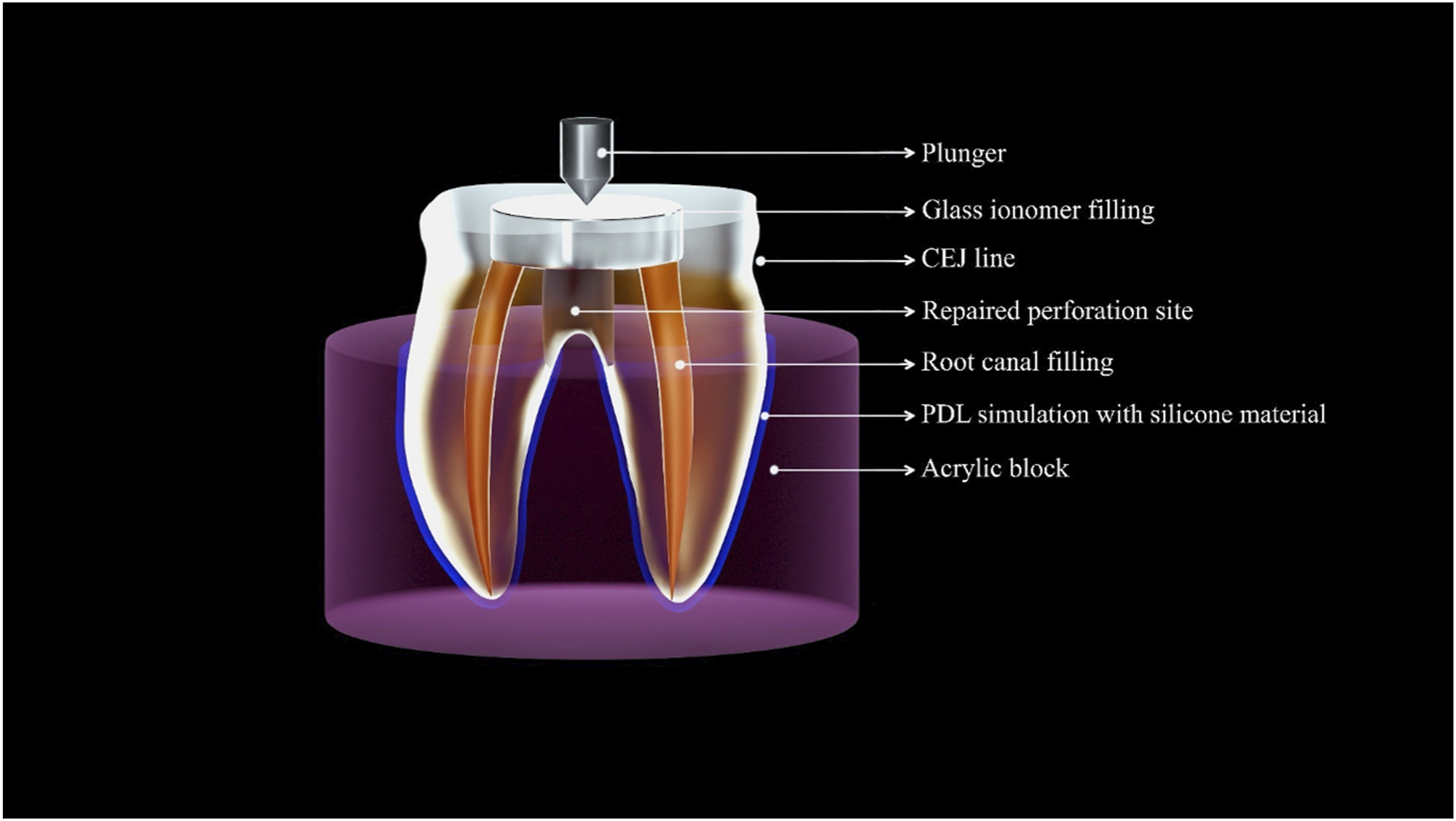
Fracture strength was measured using a universal testing machine (Lloyd Instruments LR50K; AMETEK, Inc., FL, USA) (Figure 3) by applying force to the centre of the occlusal surface of each sample at a crosshead speed of 1 mm/min, using a round-ended cylinder with a diameter of 5 mm. Figure 4 schematically illustrates the experimental setup. The amount of force displayed on the screen at the moment that the fracture occurred was recorded. The operator performing the fracture strength testing was blinded to the group allocation. Mounted samples on universal testing machine. Schematic illustration of the experimental setup used for the fracture strength testing of repaired furcal perforations.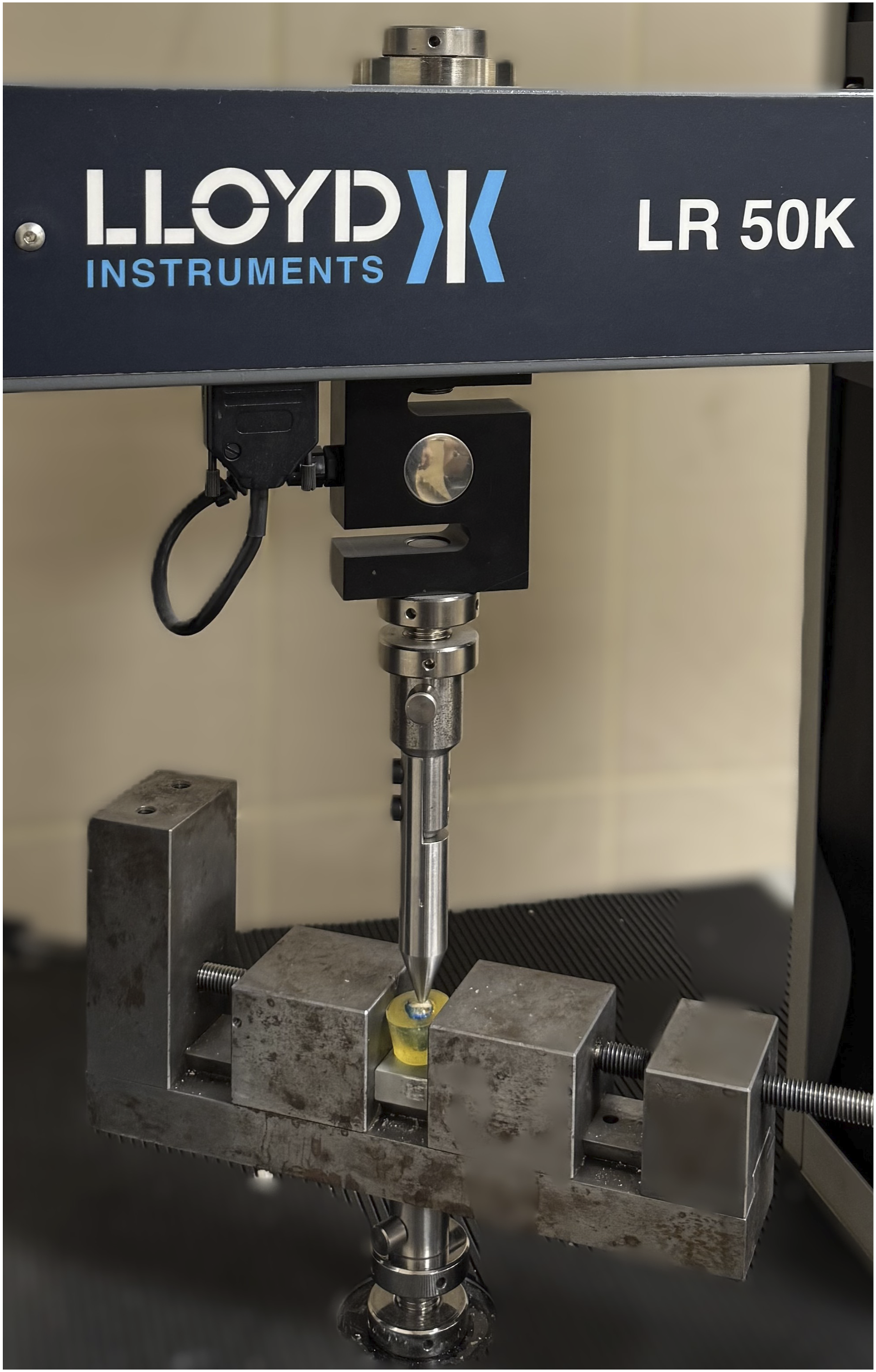
Statistical analysis
Statistical analyses were performed using SPSS software (IBM Corp., Armonk, NY, USA). Mean, standard deviation, median, minimum and maximum values were used as descriptive statistical data. The conformity of the data to normal distribution was assessed using the Shapiro–Wilk test. Comparisons between groups were performed using a one-way analysis of variance (ANOVA). The group from which the difference originated was evaluated using Tukey’s HSD test. The level of statistical significance was set at p < 0.05.
Results
Descriptive statistical data of the fracture strength (in newtons) values for the tested groups.
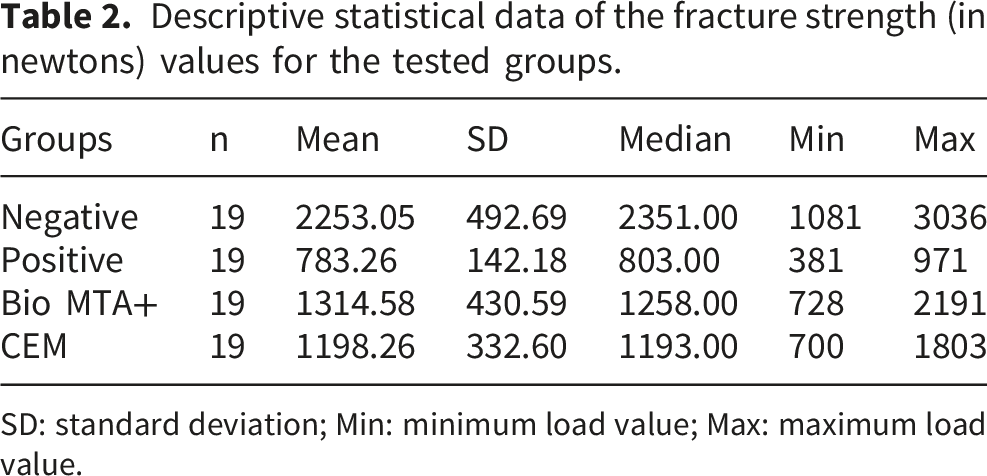
SD: standard deviation; Min: minimum load value; Max: maximum load value.
Multiple comparison test results of the fracture strength (in newtons) values among groups.
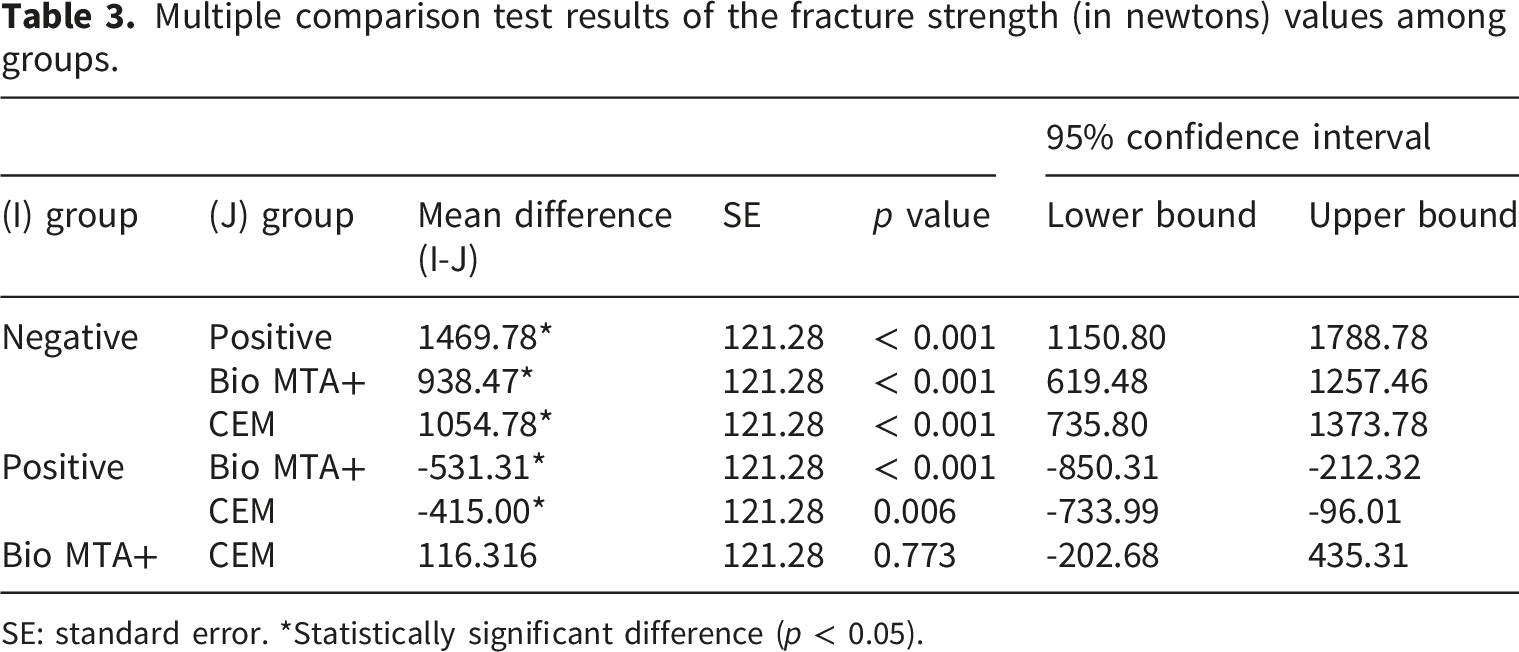
SE: standard error. *Statistically significant difference (p < 0.05).
No statistically significant difference was observed between the Bio MTA+ and CEM groups (p = 0.773). Both repair material groups demonstrated significantly higher fracture strength values than the positive control group, indicating better mechanical resistance following perforation repair. However, the fracture strength values in these groups remained significantly lower than those of the negative control group.
The distribution of fracture strength values among the groups is illustrated in Figure 5. The boxplot conveys a clear separation between the positive control group and the other groups, with the negative control group showing higher values and a wider distribution. The Bio MTA+ and CEM groups exhibited overlapping interquartile ranges, reflecting the absence of a statistically significant difference between these two materials. Boxplot illustrating the distribution of fracture strength values (N) among the experimental groups.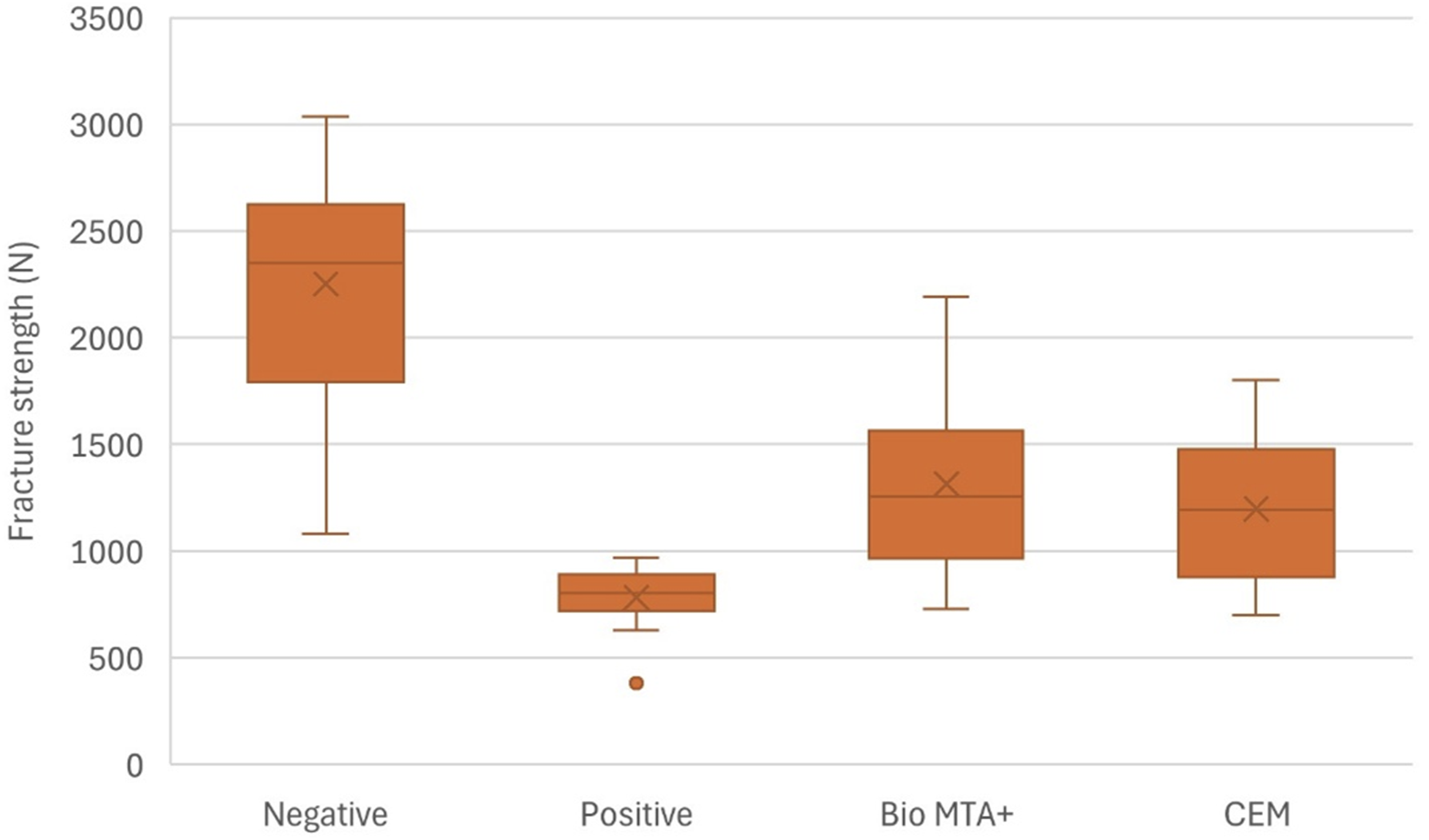
Discussion
The present study evaluated the fracture strength of endodontically treated mandibular molars with simulated furcal perforations repaired using two calcium silicate-based biomaterials, Bio MTA+ and CEM. The results found that unrepaired perforations significantly reduced fracture resistance, whereas the use of both repair materials augmented mechanical strength compared with the positive control group. However, neither material restored fracture resistance to the level observed in the negative control group. The results demonstrated that while repair improved strength, neither material restored it to the negative control level; therefore, the null hypothesis was partially rejected.
The standardisation of the experimental conditions was prioritised to minimise confounding factors. Mandibular molar teeth were selected for this study because a substantial portion of clinical perforations occur in this tooth type, 5 making standardised experimental conditions here particularly relevant. A substantial portion of the crown was removed to reduce the variability related to the coronal anatomy and restorative procedures. Although the complex multidirectional forces encountered in the oral environment cannot be fully replicated in vitro, applying a vertical load at 90° allowed consistent and reproducible comparisons across all samples. 18 Moreover, composite restorations on the crown part of the teeth may disperse functional stresses through the dentine–bond interface, which may affect fracture strength values.19,20 Additionally, centrally located perforations were selected because a previous finite element analysis has demonstrated that defects located in the central region of the pulpal floor are associated with greater stress concentration and a higher risk of fracture than more peripheral defects. 3 The simulation of the periodontal ligament using a silicone-based impression material was performed to better approximate clinical conditions and to reduce the potential effects of acrylic polymerisation on root structures. 13 In addition, a 7-day storage period was selected to allow the complete setting and maturation of the calcium silicate-based repair materials before fracture testing. The relatively lower variability observed in the positive control group may be related to the standardised perforation procedure, which consistently reduced structural integrity among the specimens. In contrast, the negative control group may have been more influenced by natural anatomical variations in the tooth structure.
This study found that unrepaired furcal perforations significantly compromise fracture resistance, whereas repair with calcium silicate-based materials partially restores mechanical strength. The positive control group presented the lowest fracture strength values, confirming the detrimental mechanical effects of unsealed perforations. These defects may act as areas of structural discontinuity, leading to stress concentrations under functional loading. Aside from the possible negative biological consequences of untreated furcal perforations, 4 higher stress accumulation in empty cavities was demonstrated in the finite element analysis studies by Aslan et al. 21 Therefore, it is important to repair the perforated area with materials that can share the stress load and distribution with the remaining hard tissue, preferably those with an elastic modulus closer to that of dentine.6,9 The elastic modulus values of Bio MTA+ and CEM are unknown. However, it is known that Portland cement, a precursor to MTA, reaches an elastic modulus of 15–30 GPa upon hardening. 22 Considering that the elastic modulus of dentine ranges from 14.0–18.6 GPa, bioceramic materials contribute to stress distribution and may protect teeth from fracturing.3,6,22 Despite this improvement, fracture strength values in the repaired groups remained significantly lower than those of the negative control group, indicating that complete mechanical restoration was not achieved. This is particularly important for calcium silicate cement-based materials. Elwazan et al. 9 compared Biodentine, which is marketed as a dentine-substitute, and Portland cement in the repair of mid-root perforations in premolar teeth and reported that teeth repaired with Biodentine were as fracture resistant as intact teeth. The method of preparing the materials may have caused such a difference. Biodentine is a produced in capsule form and is mechanically mixed in a standard way using an amalgamator. In the present study, however, Bio MTA+ and CEM were prepared manually by hand mixing. The compressive strength of materials prepared with an amalgamator is reportedly higher than those prepared manually, 23 which may explain why complete mechanical restoration was not achieved here. Furthermore, achieving a void-free filling in the repair of furcal perforations is difficult. 24 The presence of interfacial gaps or voids, even at a microscopic level, may limit the reinforcing potential of these materials and prevent the complete recovery of mechanical integrity.
In the present study, no statistically significant difference was observed between Bio MTA+ and CEM in terms of fracture strength. Although these materials differ in chemical composition, they are both classified as calcium silicate-based biomaterials and share similar clinical indications. However, the long-term performance of the materials may vary. Biodentine has been reported to have a greater increase in compressive strength after 1 month compared to traditional MTA. 25 In the present study, fracture strength testing was performed 1 week after repair procedures. The long-term effects of Bio MTA+, a newer formulation, on fracture strength could be the subject of further studies. Although no statistically significant difference was observed between Bio MTA+ and CEM, the Bio MTA+ group displayed numerically higher fracture strength values. Compared with unrepaired perforations, fracture resistance increased by approximately 68% in the Bio MTA+ group and 53% in the CEM group. These findings suggest that both calcium silicate-based materials provide a substantial mechanical benefit following perforation repair. However, the relatively large variability within the repair groups and the absence of a statistically significant difference indicate that these numerical differences should be interpreted with caution. From a clinical perspective, both repair materials substantially improved fracture resistance compared to unrepaired perforations. Although neither material restored fracture strength to the level of the negative control group, the magnitude of improvement observed in the Bio MTA+ and CEM groups highlighted the mechanical value of perforation repair.
Previous studies comparing CEM and traditional MTA have reported inconsistent findings depending on the experimental design and outcome measures. While some studies have demonstrated comparable performance between these materials in terms of fracture resistance,19,26–28 others have reported distinctions under specific conditions.13,14,16,29 For example, in Kabtoleh et al.’s study, 13 the fracture strength of MTA was found to be better than that of CEM in strip perforation repair. In Sheykhrezae et al.’s study, 14 the bond strength of MTA in furcal perforations was better than that of CEM. Moazami et al. 29 reported that MTA reduced the flexural strength of bovine dentine more than CEM in the long term. Sahebi et al.’s fluid filtration study 16 reported that CEM showed better sealing properties than MTA. These discrepancies may be explained by variations in defect configuration, loading protocols, sample preparation methods and evaluation techniques.
The current study has several limitations inherent to in-vitro designs. The complex biomechanical and biological conditions of the oral environment, including cyclic loading, thermal fluctuations and periodontal responses, cannot be fully simulated. In addition, the structural variability of dentine among teeth and regions may have influenced the results.3,6 Furthermore, the long-term behaviour of calcium silicate-based materials and their interaction with dentine over time were not assessed. 29 Moreover, the fracture patterns and microstructural characteristics of the fractured specimens were not evaluated. Future studies incorporating microscopic analyses of fracture surfaces and material–dentin interfaces, dynamic loading conditions, long-term evaluation and different repair timings may provide further insight into the mechanical behaviour and clinical performance of perforation repair materials.
Within the limitations of this in-vitro study, furcal perforations significantly reduced the fracture resistance of endodontically treated teeth compared to those without structural defects. Repair with calcium silicate-based materials, such as Bio MTA+ or CEM, improves mechanical strength but does not restore it to the level of endodontically treated teeth without perforation. Bio MTA+ and CEM demonstrated comparable performance and may be considered suitable options for furcal perforation repair from a mechanical standpoint. While repair provides a significant mechanical benefit compared to no treatment, the treated tooth remains more susceptible to fracturing than its non-perforated counterpart.
Footnotes
Ethical considerations
This study was approved by the Baskent University Institutional Review Board and Non-Interventional Clinical Research Ethics Committee, in accordance with the Declaration of Helsinki (project no: D-DA25/02).
Consent to participate
Informed verbal and written consent was obtained from all patients whose extracted teeth were used in this study.
Author contributions
B.O.: Conceptualization, Resources, Investigation; T.O.: Writing – Original draft, Investigation, Visualization; D.I.: Project administration, Investigation, Data curation; D.R.: Resources, Formal analysis. K.G.: Supervision; Writing – Review & Editing. All authors reviewed and approved the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Baskent University Research Fund (Project no: D-DA25/02).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analysed during the current study are uploaded as research data.