
Abstract
Introduction:
Endometriosis affects around 10% of women of reproductive age with symptoms of pelvic pain, dysmenorrhoea, dyspareunia, dyschezia, and infertility. Current research highlights a possible relationship between endometriosis and poor sleep quality. The aim of this study was to assess the relationship between sleep quality and endometriosis. Outcomes measured included sleep quality and quality of life and pain score.
Methods:
Thirty women with a histological diagnosis of endometriosis and 30 control patients completed an online questionnaire that assessed sleep quality (Pittsburgh Sleep Quality Index) and quality of life (WHO-QOL-BREF). Pain scores within the endometriosis group were evaluated using a visual analogue scale.
Results:
Women with endometriosis had significantly poorer sleep quality (80% vs 50%, p = 0.015) and lower quality of life scores when compared to the control group. Within the endometriosis group, there were trends between poor sleep, a reduced quality of life, and higher pain scores; however, these did not reach statistical significance.
Discussion:
Sleep quality and quality of life were significantly reduced in women with endometriosis when compared to controls.
Introduction
Endometriosis is defined as the presence of endometrial glands and stroma outside of the uterine cavity and remains the most common cause of chronic pelvic pain in women. 1 It affects around 10% of women of reproductive age 2 with the prevalence increasing to 30%–40% in women undergoing gynecological surgery for pelvic pain or infertility. 3 Other symptoms include dysmenorrhoea, dyspareunia, dyschezia, and infertility. Despite a multitude of studies, the pathophysiology and ideal treatment of endometriosis remains unclear, but the role of estrogen in the disease progression is well documented. Many studies have shown endometriosis to be associated with a reduced quality of life (QOL)4,5 and a reduced quality of sex life. 5 The disease is associated with a high economic burden, and studies have shown that QOL scores can be utilized to predict the extent of these costs.4,6 In addition, the prevalence of depression and anxiety7–9 is higher in women with endometriosis, with recent studies suggesting multi-professional group intervention combined with conventional treatments as an ideal multidisciplinary approach to the management of the disease. 10
Interestingly, studies have shown that the level of pain reported by women with endometriosis is not correlated to the stage of disease,11,12 suggesting factors other than the primary lesions to be responsible for the degree of pain experienced. It has also been demonstrated that a lower pain threshold exists in women with endometriosis,13–15 suggesting instead a central sensitization process in the neurological pain pathways of these women. 16
The pain associated with endometriosis begins with the activation of peripheral nerve receptors at the site of the lesions when the nerves are compressed or infiltrated. 17 This pain is a result of tissue injury and release of various local inflammatory mediators such prostanoids, substance P, nitric oxide (NO), chemokines, and cytokines. Over time, these act to lower the threshold of pain receptors, leading to a heightened pain sensitivity in the area of damage (primary hyperalgesia) and also in surrounding regions as a result of central sensitization (secondary hyperalgesia). Nerve growth factor and brain-derived neurotrophic factor (BDNF) in lesions have been shown to be neuromodulators and contributors to this secondary hyperalgesia. 18 With continuous noxious input into the central nervous system (CNS), alterations in gene transcription and expression of neurotransmitters results in a hypersensitive state well beyond the area of initial noxious input.
Sleep is one modifiable lifestyle factor that can influence several components of the pain pathway. Pain and sleep are closely related; however, the direction of causality remains unknown. Lack of sleep leads to hypersensitivity to pain19,20 and interference with the activity of pain medications; 21 and also increased pain can directly result in interrupted sleep cycles. In a study of women with fibromyalgia, a lack of sleep engendered significantly more pain the following day while a painful day culminated in a poor night’s sleep, indicating a bidirectional relationship. 22
Alterations in mood and attention toward pain following sleep deprivation might also account for the association with pain perception. 23 Studies with healthy people as well as clinical studies with chronic pain women showed lowered pain thresholds after sleep deprivation.19,20,24,25 This association is attributed to the shared brain structures for sleep generation and pain maintenance and modulation pathways, including the thalamus and mesencephalic periaqueductal gray matter.26–29 Neurochemical changes due to sleep deprivation may also provide an explanation for lower pain thresholds. It has been found that sleep deprivation affects 5-hydroxytryptamine (5-HT) receptor functioning, reducing the pain inhibitory effects of serotonin. 21
The association between sleep and endometriosis has only recently become a research focus. Women with endometriosis have been found to have a higher incidence of sleep disorders when compared to women without the disease 30 with investigators finding sleep disorders in 72% of women with chronic pain. 31 There is also evidence of a unique sleep disorder in this population, with another study finding women with chronic pain to have reduced rapid eye movement (REM) sleep and sleep-onset latencies. 32
A study from South America found reduced sleep quality in women with endometriosis, with an association found between better sleep quality and higher pain thresholds and also between higher pain scores and reduced sleep quality. 33 Following on from this, an Italian study found the prevalence of poor sleep quality to be significantly higher in women with endometriosis (64.8%) compared to controls (12.9%); in turn, poor sleep was associated with increased pelvic pain and reduced QOL. 34
Given poor sleep quality is associated with a reduced QOL and/or worse pain scores in women with endometriosis, this highlights a significant modifiable lifestyle factor to target for treatment. Interventions to improve sleep quality could be considered as part of a holistic approach to pain management in this complex patient cohort. Sleep disorders can be improved by simple interventions such as regular physical activity and sleep education. 35 Moreover, melatonin has shown to be a novel potential treatment for endometriosis.
Melatonin increases sleep quality, while also acting as an analgesic and anti-inflammatory agent, in those with endometriosis. 36 In addition, multiple animal experiments have shown that exogenous melatonin can suppress endometriosis lesions. 37 Melatonin not only acts as sleep inducer but is also an anti-oxidant, free-radical scavenger, anti-inflammatory agent, anti-carcinogenic factor, and potential immunoregulator and, therefore, could play a very important role in this population of women suffering from endometriosis.
Considering all the current available literature, this study aimed to explore the relationship between sleep quality and endometriosis, in an Australian population. This was achieved by comparing sleep quality between a group of women with a histological diagnosis of endometriosis and a control group of women (with no diagnosis or symptoms of endometriosis). Secondary outcomes included the effects of poor sleep on QOL and pain scores and the correlation between pain scores and QOL.
Materials and methods
This study was conducted at a large Australian tertiary Hospital. The project was approved by the local Human Research Ethics Committee (HREC/16/QGC/112).
Subjects were recruited from the hospitals outpatient gynecology clinics. Participants in the group of interest (endometriosis, n = 30) were recruited from the gynecological surgical waiting list (awaiting a diagnostic laparoscopy), completed the questionnaire pre-operatively and were included if they had a histological diagnosis of endometriosis. Control participants (controls, n = 30) were recruited from the gynecological colposcopy clinic. A total of 160 participants (77 endometriosis group and 73 control group) were invited to take part in the study. Thirty declined to participate (6 from endometriosis group and 24 from control, giving a response rate of 81.25%), 23 were excluded when there was no endometriosis found at their diagnostic laparoscopy, 23 excluded due to incomplete questionnaires (19 endometriosis group and 4 control), and 24 excluded based on other exclusion criteria (9 from the endometriosis group and 15 from the control group).
Inclusion criteria for the endometriosis group included a histological diagnosis of endometriosis. For both groups, it included ability to provide informed consent, age over 18 years, and currently attending the gynecology outpatient department of a large tertiary hospital. Exclusion criteria for the control group included any previous diagnosis or symptoms of endometriosis (dysmenorrhoea, dyschezia, dyspareunia, infertility, and chronic pelvic pain). For both groups, exclusion criteria included pregnancy, GnRH analogues, 38 illicit drugs, previous hysterectomy/oophorectomy, severe medical co-morbidities, and night shift work. These exclusion criteria were elicited through questions within the demographics section of the questionnaire.
Data were collected in the form of a collation of multiple validated questionnaires; a link was emailed to participants for the online Survey Monkey questionnaire. The complete survey included consent, demographics, the World Health Organisation Quality of Life-BREF questionnaire (WHO-QOL-BREF), the Pittsburgh Sleep Quality Index (PSQI) for sleep quality and a visual analogue scale (VAS) for pain scores (only for the endometriosis group, as the control group participants all reported no pelvic pain within the last month).
Statistical analysis
The PSQI and WHO-QOL-BREF were calculated according to the provided instructions. The WHO-QOL-BREF outcomes were also converted to the Trans scale by transforming each raw scale to a 0–100 scale. Descriptives were presented with frequency (%) for categorical variables, mean (SD) for normally distributed continuous variables, and median (interquartile range (IQR)) for skewed variables. Chi-square and Fisher’s exact tests were used for comparing categorical data. T-tests were used for comparing normally distributed continuous variables between groups and Mann–Whitney U-tests were used for skewed data. Correlations were used to assess for any linear associations between the variables. SPSS, version 22, was used for analysis. 39 Statistical significance was defined as p < 0.05.
Results
The final study included 60 participants; 30 in the endometriosis group and 30 in the control group.
Demographics
Descriptives of the demographic data for all 60 participants are shown in Table 1. The mean (SD) age was 30.4 (7.47) for women in the endometriosis group and 39.5 (10.91) in the control group (p < 0.001). Most participants were Caucasian (78.3%). The median (IQR) body mass index (BMI) was 24.0 (21.2–28.3) with no statistically significant difference between the two groups. There were, however, some significant differences between the two groups. The control group had higher rates of gravidity, parity, and use of contraception. The endometriosis group had a significantly higher proportion of women who had experienced difficulty conceiving for more than a year (p = 0.015).
Descriptives of demographics.
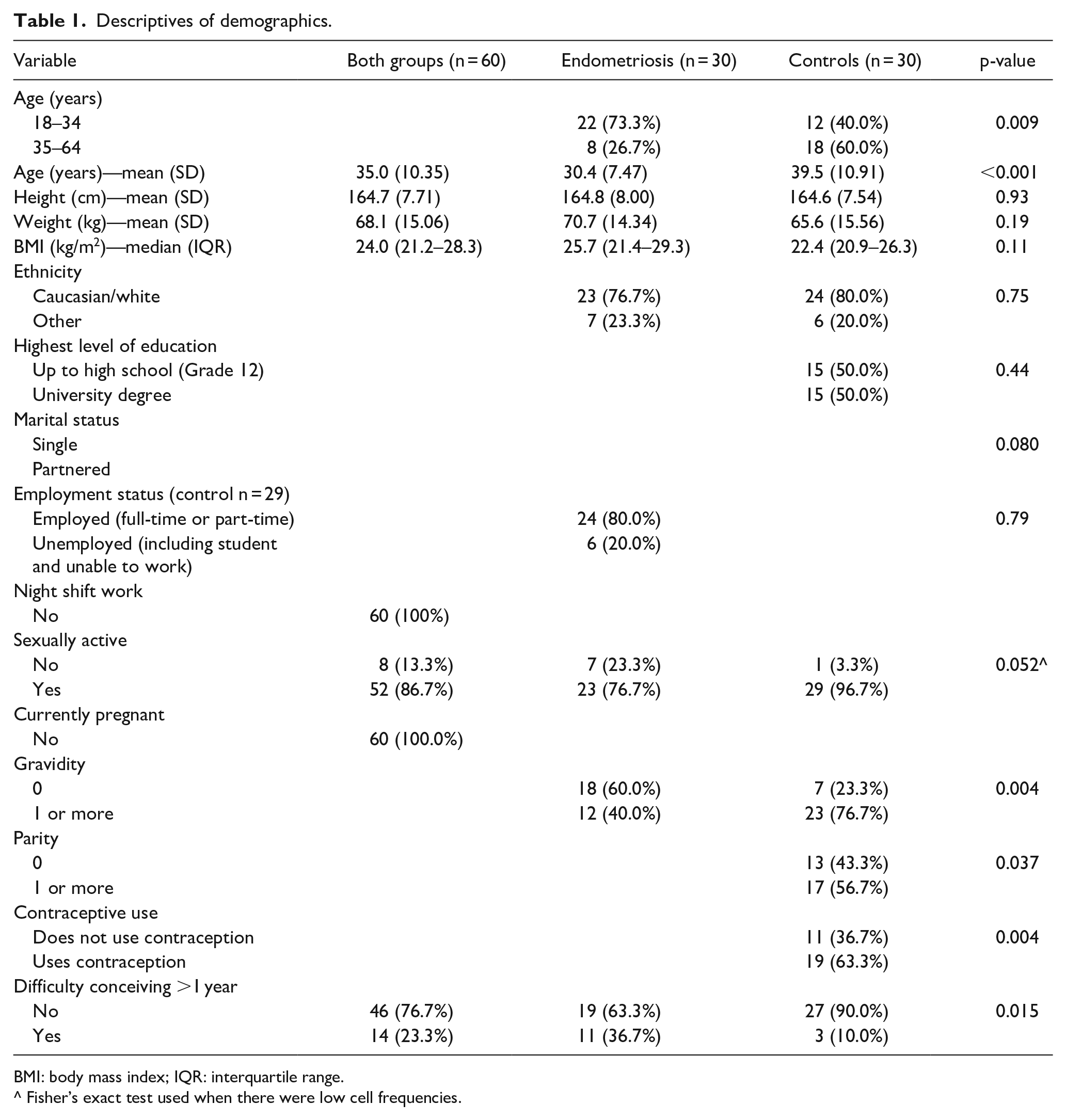
BMI: body mass index; IQR: interquartile range.
^ Fisher’s exact test used when there were low cell frequencies.
Sleep Scores (PSQI)
Participants in the endometriosis group were more likely to have poor sleep quality than those in the control group (80% vs 50%, p = 0.015) as shown in Table 2.
Comparison of sleep quality and QOL between the groups.
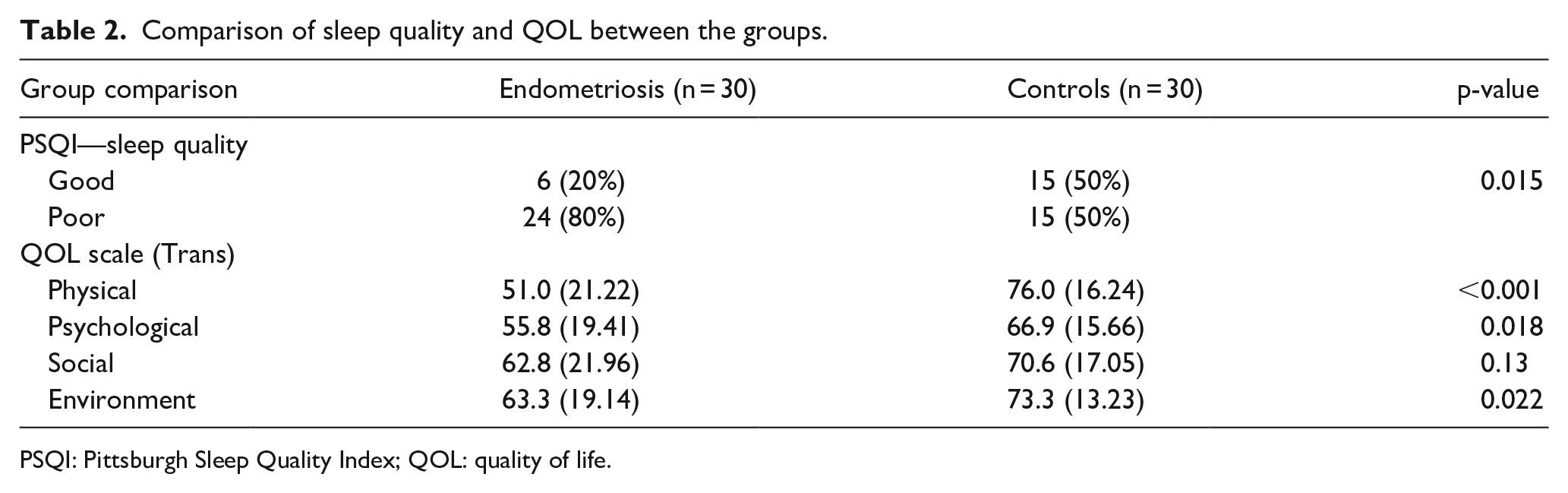
PSQI: Pittsburgh Sleep Quality Index; QOL: quality of life.
QOL (WHO-QOL-BREF)
Table 2 also shows the comparison of QOL scores between the endometriosis and control group. Physical, psychological, and environment quality of life scores were significantly lower for the endometriosis group when compared to controls (p < 0.05).
VAS pain scores
VAS pain scores were recorded by the participants within the endometriosis group and were reported as median (IQR). Pain score over the last 4 weeks was 6.5 out of 10 (4–8), dyspareunia 3.5 (0–5), dyschezia 3.5 (2–7) and pain when not menstruating 4 (0–6). Highest pain levels were recorded for “menstruation pain” with a median score of 8 (IQR: 5–9).
Sleep quality and QOL within the endometriosis group
The correlation between sleep quality and QOL for the endometriosis group is presented in Table 3. While the average QOL score was higher for the good sleep quality category in all QOL sub-scales, none of the differences were found to be significant at p < 0.05.
Association between QOL and sleep quality for the endometriosis group.
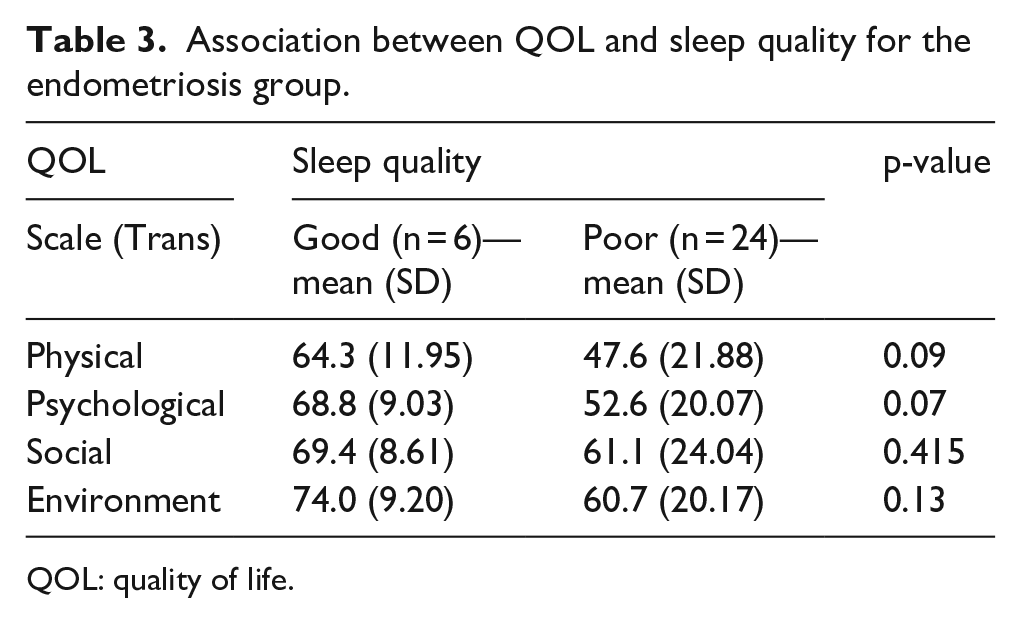
QOL: quality of life.
Sleep quality and pain scores within the endometriosis group
Participants with poor sleep quality generally had higher pain scores, except in the case of pain when the participant is not menstruating, however again these differences were not found to be significant (Table 4).
Association between sleep quality and pain levels for each pain type.
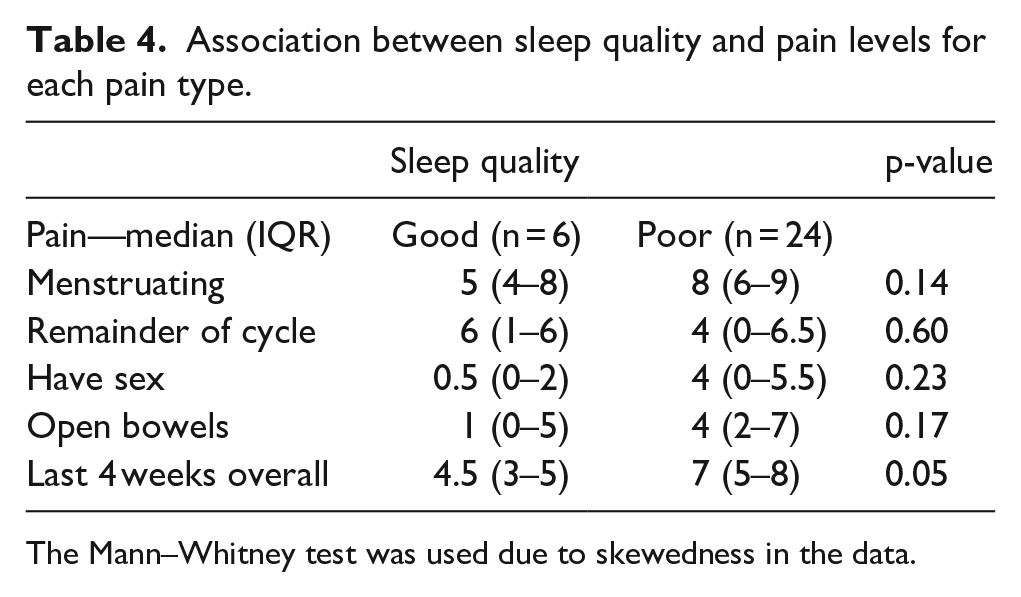
The Mann–Whitney test was used due to skewedness in the data.
Pain and QOL within the endometriosis group
Within the endometriosis group, the correlation between pain score and QOL measurement was negative within each domain, indicating that as one increases, the other decreases (Table 5). However, none of the correlations were strong. The correlation with the largest magnitude was that between physical QOL and overall pain in the last 4 weeks, r = −0.54 (p = 0.002).
Correlations between pain levels and quality of life scores.
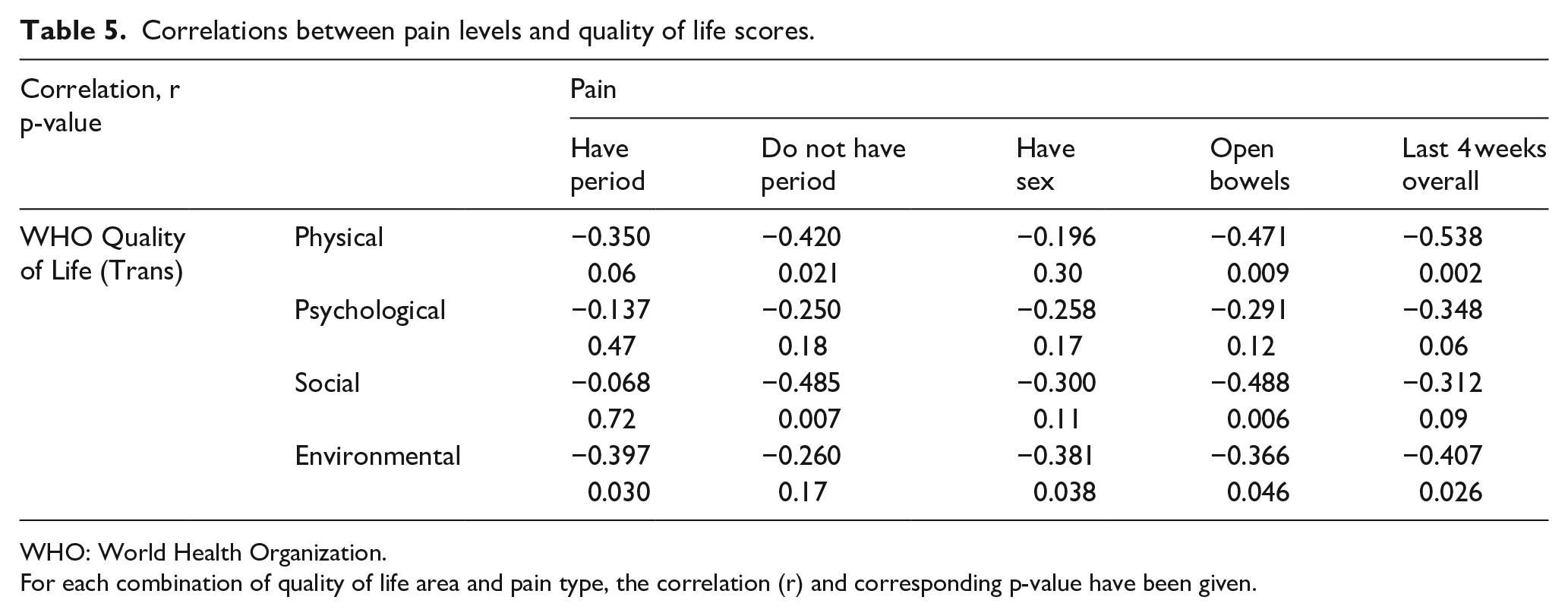
WHO: World Health Organization.
For each combination of quality of life area and pain type, the correlation (r) and corresponding p-value have been given.
Effect of age on outcomes
The effect of age on the outcomes was explored to investigate the effect of the unbalanced age between groups. Those with good sleep in the study population were older with a mean (SD) age of 37.8 (10.14), while those with poor quality of sleep had a mean (SD) age of 33.4 (10.27); however, this was found to be not statistically significant (p = 0.12). Pearson’s correlations were calculated between the continuous age measure and the WHO-QOL outcomes (for both groups) and the VAS pain scale outcomes (for the endometriosis group only). All correlations in both tables were small (r < 0.3) and non-significant. When the WHO-QOL was investigated for each domain separately, the correlations were also small and non-significant.
Discussion
Women with endometriosis had poorer sleep quality when compared to controls. They also had significantly lower QOL scores, in three of the four assessed areas. The results of this study are consistent with the small number of available studies. This however is the first study of its kind in an Australian population. VAS Pain scales highlighted that endometriosis women experience pain at all times, with worse pain occurring at the time of menstruation.
Within the endometriosis group, the average QOL score was higher for all sub-scales for those with good sleep quality, compared to those with poor sleep. The endometriosis participants with poor sleep also generally had higher pain scores in comparison to those with good sleep. Finally, there was a consistent negative correlation between pain scores and QOL within all domains within the endometriosis group, with higher pain scores associated with reduced QOL scores. These all suggested and highlighted important clinical relationships, but the magnitude of the correlations was too small to provide strong evidence. A larger sample size in future studies may be able to provide more evidence.
Within the demographics, there were some significant differences between the two groups. Women with endometriosis were more likely to have experienced difficulty conceiving for more than a year and less likely to have ever been pregnant or have given birth (Table 1). This would be consistent with the known association between endometriosis and infertility. Within the endometriosis group only 26.7% of participants used some form of contraception (3.3% mirena, 13.3% oral contraceptive pill, and 10% other (condoms and copper IUD) which was an interesting observation, given hormonal contraceptives are the usual first-line treatment for endometriosis. Endometriosis women (76.6%) used analgesia on a regular basis (paracetamol, ibuprofen, naprogesic, or endone) again highlighting the amount of pain experienced by this population. There was a significant difference in age between the endometriosis and control group. However, this was taken into account and explored further during analysis and no significant association was found between age and the outcomes (sleep quality, QOL, and pain scores).
This study found that women with endometriosis had significantly poorer sleep and QOL, when compared to healthy controls. Limitations of the study included the small sample size and the statistically significant difference in age between the two groups. Larger, aged-matched, case-control studies are required to further investigate the relationship between sleep quality and endometriosis in an Australian population. Furthermore, while exclusion criteria ensured the control group experienced no symptoms of endometriosis, in future studies, ultrasonography should be utilized to confirm this. This study, like previous similar studies, compared women with endometriosis to healthy controls, to highlight the presence of impaired sleep quality in this group of women. Therefore, this study is unable to identify whether the poor sleep in the study group was caused directly by the endometriotic pathology or due to their chronic pain. Future studies could compare sleep quality between women with endometriosis and women with other forms of chronic pain, to determine if endometriosis has an independent, significant, effect on sleep. This study represents a gateway to future research to explore sleep-related interventions, including the use of melatonin, in women diagnosed with endometriosis.
Footnotes
Acknowledgements
The authors would like to thank all the women who participated in the study.
Author contribution
S.D. and Y.H. conceived and designed the study and performed the data collection. S.D., L.W., and A.A.A. participated in analysis and interpretation of data and wrote the manuscript. A.A.A. critically revised and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The project was approved by the Gold Coast University Hospital Human Research Ethics Committee (HREC/16/QGC/112).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent to Participate
Written informed consent was obtained from all subjects before the study.
Informed Consent to Publish
Written informed consent was obtained from the patient(s) for their anonymised information to be published in this article.