
Abstract
Ultrasound-guided transvaginal ethanol sclerotherapy is one of the methods for ovarian endometrioma treatment. It involves aspiration of the cyst content and subsequent administration of some fibrosis agent. This minimally invasive procedure does not reduce ovarian reserve hence, it is addressed to patients with fertility plans. To date, there have been no reports of this method being used in patients with advanced disease stages. Therefore, we present a case of a patient with advanced deep infiltrating endometriosis who underwent this treatment procedure for endometrioma. Our patient had a history of two extensive laparotomies for deep infiltrating endometriosis. A follow-up MRI examination revealed the presence of ovarian endometrioma and disturbed anatomy of the pelvis. The patient was referred to our center and deemed a suitable candidate for ultrasound-guided transvaginal ethanol sclerotherapy for endometrioma. The procedure was successfully performed. After 8 months of follow-up, no recurrences were observed, and the patient reported significant alleviation of pain symptoms. The high efficacy of sclerotherapy in managing advanced endometriosis phenotypes is encouraging. However, further research is needed.
Introduction
Regardless of the severity of endometriosis, co-occurrence of different disease subtypes including ovarian cysts (endometriomas), lesions located on the peritoneal surface, or foci of the disease deeply infiltrated pelvic cavity organs is commonly observed.1,2
For this reason, endometriosis is challenging to treat. Treatment of endometriomas primarily includes pharmacotherapy and surgical cystectomy. Nevertheless, a single optimal treatment method is difficult to indicate, as it depends on the dominant symptoms and disease advancement. 3
In addition to using the methods mentioned above, endometriomas can also be effectively resolved with sclerotherapy, a minimally invasive treatment method. This procedure involves the aspiration of fluid from the endometriotic cyst, followed by the injection of a sclerosing agent, which induces fibrosis and occlusion. 4 It is mainly performed from transvaginal access under ultrasound guidance,5,6 and high-percentage ethanol is the most commonly used sclerosing agent. 4 A recent meta-analysis emphasized the particular utility of this method in women with reproductive intentions, due to its negligible impact on ovarian reserve. Thus, sclerotherapy is primarily indicated for this target group of patients. 7 Although sclerotherapy for endometriomas has been known for over twenty years, the indications for the procedure have not been entirely specified. 8 To the best of our knowledge, there are no reports describing the use of sclerotherapy in patients with advanced endometriosis so far.
Therefore, we present a case of a 37-year-old patient diagnosed with deep infiltrating endometriosis with a co-occurred ovarian endometrioma who successfully underwent the procedure of transvaginal ultrasound-guided ethanol sclerotherapy.
Case description
A 35-year-old woman with a history of painful menstruation, but no known chronic medical conditions, presented to the emergency department with severe abdominal pain, nausea, and constipation. Given the suspicion of paralytic ileus, the patient underwent an emergency laparotomy. During the surgery, a hard 4-cm whitish tumor, which caused complete bowel obstruction, was found in the mesentery of the distal sigmoid. A sigmoidectomy with a temporary end-on colostomy was performed. During the surgery, the presence of deep infiltrating endometriosis was suspected, which was further confirmed in the histopathological examination.
Postoperatively, the patient received dienogest therapy. Between 2 and 5 months post-surgery, she underwent computed tomography (CT) and magnetic resonance imaging (MRI) scans. Their results revealed endometriotic infiltration involving the Douglas pouch and the rectum and endometriomas in the right and left ovaries measuring 17 mm × 30 mm and 12 mm × 25 mm, respectively.
Eight months after primary surgery, the patient underwent an elective laparotomy. Before the surgery, the serum level of Ca-125 was greatly increased and measured at 103 U/mL. During the surgery, a colo-anal anastomosis and a cystectomy for endometriomas were performed.
Following the second surgery, the patient continued hormonal therapy. Despite amenorrhea, she continued to experience abdominal pain. The follow-up Ca-125 level examined 1 month after the procedure decreased to 22.70 U/mL. Moreover, the HE-4 value was 47.70 pmol/L and the AMH value was 3.14 ng/mL.
A follow-up MRI scan performed a year and a half after the second surgery described an endometrioma of the left ovary and multiple foci of peritoneal endometriosis.
Six months after this imaging study, the patient was referred to our center, where she underwent an ultrasound (US) examination. The occurrence of endometrioma measuring 41 mm × 35 mm in the left ovary was revealed. US examination did not find any suspicious signs of malignancy. Consequently, the patient was qualified for the ultrasound-guided transvaginal ethanol sclerotherapy for the endometrioma, after providing informed consent.
The procedure was performed under general anesthesia (midazolam and propofol), with the patient in the lithotomy position. Following aseptic preparation of the vagina, 20 mL of dark viscous fluid was aspirated from the cyst using a 16-G needle under ultrasound guidance. The aspirated fluid was submitted for cytological examination. Subsequently, the cyst cavity was flushed with saline several times until the fluid was clear. About 12 mL of 96% ethanol was then instilled in the lesion cavity and aspirated after 10 min of dwell time. The procedure was completed without complications. The results of the cytological examination were typical for endometriomas. Figures 1a and 1b illustrate the ultrasound scans before and immediately after sclerotherapy, respectively.
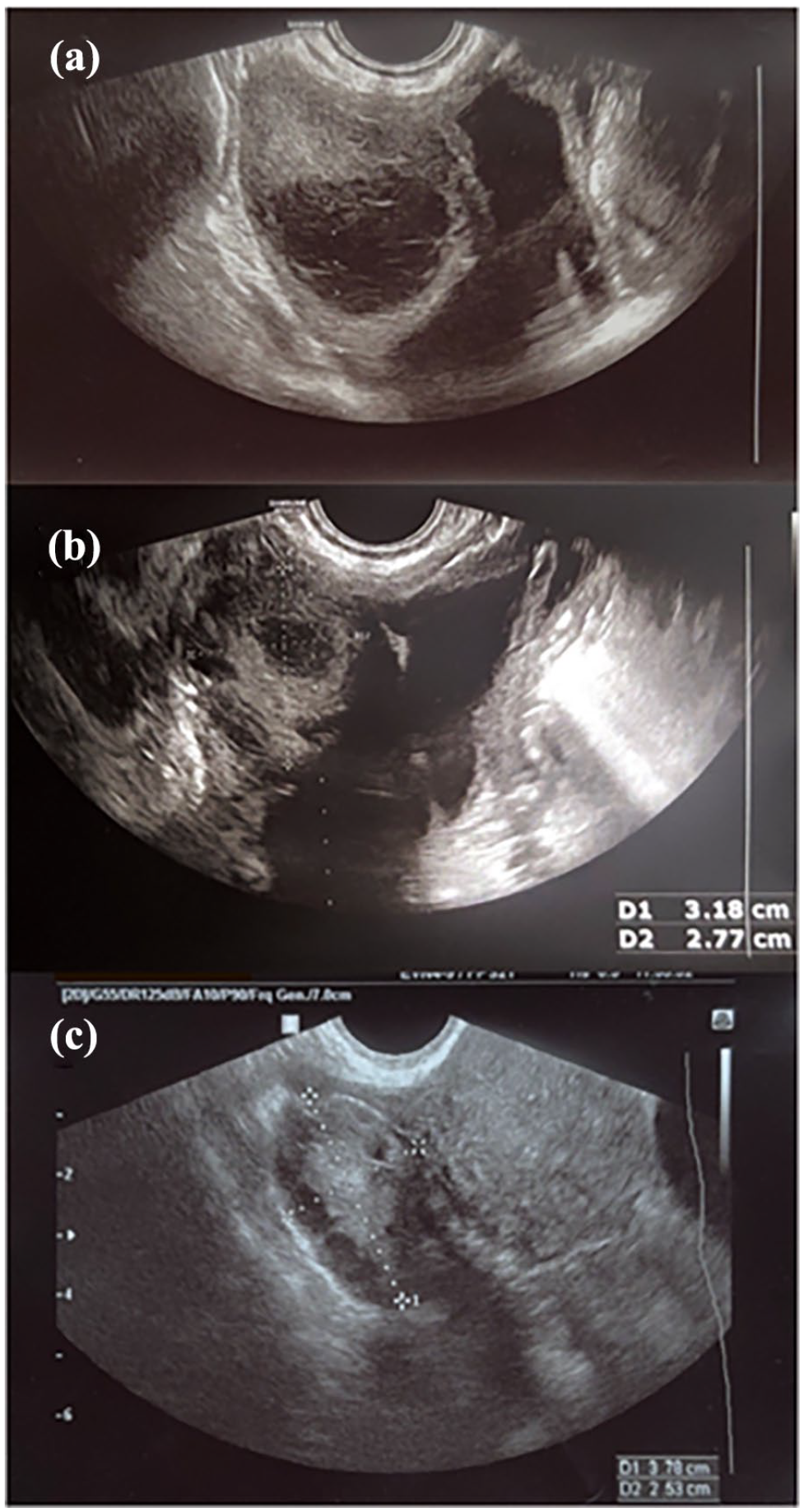
Ultrasound image of the left ovary: (a) before (cyst measuring 41 mm × 35 mm), (b) immediately after (32 mm × 28 mm), and (c) 8 weeks after sclerotherapy.
At the 8-week follow-up examination, the patient reported no symptoms, and no abnormalities were found in the ultrasound (Figure 1c).
Pre- and 3 months post-procedure, at the second follow-up visit, pain assessments were conducted using a 10-point visual analog scale (VAS) for menstrual pain, dyspareunia, and chronic pelvic pain. The ratings for each parameter decreased after sclerotherapy. Menstrual pain decreased from 5 to 2, dyspareunia from 2 to 1, and chronic pelvic pain from 5 to 2. Six months post-procedure, AMH was measured at 3.10 ng/mL.
Conclusions
Sclerotherapy, a minimally invasive approach for endometriomas, has been shown not to affect ovarian reserve, making it suitable for women with reproductive plans.9,10 Moreover, this treatment efficiently alleviates pain symptoms, 10 likely due to reduced local inflammation and oxidative stress following cyst aspiration.11,12
Despite its advantages, sclerotherapy is not without limitations. Although imaging examinations are used to assess suitability, the definite diagnosis of a non-endometriotic cyst can only be confirmed histopathologically. 9
Additionally, some studies suggest a higher recurrence rate compared to laparoscopic cystectomy. 7 Minor adverse events, including fever, mild abdominal pain, and the appearance of an abscess or alcohol intoxication, may occur. 7 Minimizing the risk of infection is essential, particularly in sclerotherapy performed from transvaginal access. A sterile vaginal swab and prophylactic antibiotics before the procedure may be considered, as suggested by Miquel et al. 9 While ethanol leakage is a rare complication, affecting only 0.3% of patients according to Kim et al., 10 steps can be taken to further reduce its risk. 4 These include immobilization of the patient, partial volume injection of ethanol, and limiting the number of cyst punctures. 4
The described case had a positive outcome, as a significant post-procedural pain reduction was noticed. Moreover, AMH concentration did not decrease 6 months post- procedure, and endometrioma did not recur 8 months after the sclerotherapy.
Patient’s history of extensive endometriosis-related surgeries, according to the imaging scans, had substantially altered pelvic anatomy. Therefore, further intervention could have led to severe complications and surgical failure. Additionally, the patient’s desire to undergo sclerotherapy was motivated by a deteriorated quality of life after two serious surgeries.
It is worth emphasizing that in this case, while sclerotherapy offered a less invasive approach, it was not without risk, as transvaginal access could have been compromised by the patient’s altered pelvic anatomy. Nevertheless, a preoperative US examination indicated that a safe cyst puncture was feasible, making sclerotherapy a viable option.
Previous studies have demonstrated the efficacy of sclerotherapy in treating large-diameter endometriomas 13 or abdominal wall endometriosis. 14 However, these cases did not involve deep infiltrating endometriosis. While there were also several studies in which ethanol sclerotherapy was used for endometriomas in patients with deep infiltrating endometriotic lesions, the lesions were not advanced.15 –17
To the best of our knowledge, this case report represents the first ultrasound-guided transvaginal ethanol sclerotherapy being used successfully in a patient with advanced deep infiltrating endometriosis phenotype.
In conclusion, ethanol sclerotherapy can be a viable option for patients with advanced endometriosis, particularly when another surgical intervention carries high risk of complications. Interestingly, in our patient, sclerotherapy resulted in a significant reduction of pain despite the presence of deep infiltrating endometriotic lesions. In addition, we hope that this approach has preserved ovarian function and increased likelihood of future fertility.
Footnotes
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the Medical University of Lublin.