
Abstract
Introduction:
Chronic pelvic pain (CPP) is a common and variable condition often without standardised or effective treatment. A hysterectomy and/or oophorectomies alleviates CPP long term in some patients. Gonadotrophin releasing hormone analogues (GnRHa) induce a pseudo-menopausal state, mimicking some outcomes of these surgical procedures. This study aims to examine whether the use of pre-operative GnRHa can predict the pain outcome of patients undergoing hysterectomy and/or oophorectomies for CPP.
Methods:
This is a retrospective cohort study at a tertiary university-affiliated hospital between 2010 and 2019 inclusive. Of 647 patients screened, 56 met the inclusion criteria of (i) pre-operative GnRHa prescription for pain management and (ii) proceeding to hysterectomy and/or oophorectomies. A positive pain response was considered either partial or complete pain relief.
Results:
All patients (N = 16) who had complete pain relief with GnRHa had complete pain resolution after surgery. Of the 25 patients who had partial resolution of pain with GnRHa, 22 (88.0%) had a positive pain response post-surgery. One patient reported no pain relief with either intervention. Pre-operative GnRHa had a sensitivity of 90.5% and specificity of 100% in predicting pain outcomes post hysterectomy and/or oophorectomies in this study.
Conclusion:
Pre-operative GnRHa may be useful in patients with CPP to predict pain outcome after hysterectomy and/or oophorectomies.
Introduction
Chronic pelvic pain (CPP) is a common and debilitating condition that affects up to 26% of women of reproductive age worldwide.1–6 CPP accounts for up to20% of visits to gynaecologists, 40% of laparoscopies and 10%–12% of hysterectomies,3,4,6 even though the origin of CPP is not gynaecologic in 80% of patients.1,2 Despite increasing awareness of its prevalence, CPP remains a complex medical issue presenting both diagnostic and therapeutic challenges due to the varied underlying causes that include both organic and functional pain syndromes. 5
Available treatment options for patients with CPP involve medical and surgical interventions.6–9 Medical treatments include hormonal suppression of the menstrual cycle, analgesics, physical therapy and cognitive-behavioural therapy.7–9 Surgical treatments include diagnostic laparoscopy, laparoscopic treatment of endometriosis, neuroablative procedures and resection of pelvic organs including the uterus and/or ovaries.7–9
While laparoscopic excision of endometriosis reduces pain for up to 80% of patients, 10 long-term pain reduction remains an ongoing issue with up to 50% experiencing a recurrence by 5 years post-operatively 11 and over 60% of patients having a repeat laparoscopy. 12 However, patients who have a hysterectomy and/or oophorectomies achieve significantly better long-term pain reduction. More than 80% of patients who have a hysterectomy alone have long term pain reduction11,13,14 while up to 90% achieve long term pain reduction with a hysterectomy and bilateral oophorectomies. 13 However, in patients with a higher degree of central sensitisation, there was a less than 50% improvements in pelvic pain 6 months after hysterectomy. 15 Therefore, careful patient selection is necessary
Current management comprises of a combination of hormonal manipulation and surgeries.15,16 At present there is no clear consensus regarding the management of CPP. 16 Often reversible and less invasive treatment options are tried first and if unsuccessful, then therapies that are more invasive and irreversible are undertaken. Besides the immediate surgical risks, long-term sequelae of these decisions, such as surgical menopause in patients undergoing bilateral oophorectomies, must be considered as well. Surgical menopause can cause sudden and severe onset of menopausal symptoms, loss of bone density, reduced libido, irreversible loss of fertility and increased risk of cardiovascular disease.17–20
To aid in patient selection, the use of GnRHa had been suggested by Carey and Slack. 21 GnRHa induces a hypo-oestrogenic state and endometrial quiescence, simulating surgical menopause and to a lesser extent the post-hysterectomy experience.22,23 In a RCT by Tang et al., 24 women with stage III & IV endometriosis, surgery combined with GnRHa relieved the degree of dysmenorrhoea. 23 This might have a role in predicting the degree of pain relief that could be achieved with surgical removal of the uterus, ovaries or both.
Thus, the aim of this study is to examine the use of GnRHa as a predictive tool to identify patients who are more likely to achieve long term pain relief with hysterectomy, oophorectomies or both. The use of GnRHa to identify chronic pelvic pain patients who are likely to achieve long term pain relief with definitive surgery is novel, with no recent studies since 1996 to examine this relationship.
Materials and methods
Research aims
The primary aim of this study was to examine whether the use of pre-operative GnRHa can predict the pain outcome of patients undergoing hysterectomy and/or oophorectomies for CPP.
The secondary aim was to assess the correlation between pain reduction with GnRHa and the presence of intra-operative findings of diagnoses known to cause CPP, including endometriosis, adenomyosis and/or endometriomas, which are described as hormonally mediated intra-operative findings, as well as adhesions. Grading of adhesions were based on the Peritoneal Adhesion Index.
Study setting and study population
This is a retrospective cohort study of patients treated at a tertiary university-affiliated hospital over a 10-year period from 2010 to 2019 inclusive. Patients were identified from pharmacy dispensing records for goserelin and naferelin. Inclusion criteria were (i) that the prescription for GnRHa was for pain management and (ii) that the use of GnRHa was prior to the patient undergoing one of the following procedures: hysterectomy, hysterectomy and unilateral/bilateral salpingo-oophorectomy (USO/BSO) or salpingo-oophorectomy of residual ovary/ovaries. Based on these criteria, of the 647 patients prescribed GnRHa during this time period, 56 patients were included.
Description of intervention
Goserelin and naferelin are the two prescribed GnRHa agents used at this institution. The dose of goserelin and naferelin were 3.6 mg subdermal implant every 28 days and 2 mg/mL intranasal spray twice daily respectively. The choice of GnRHa and the decision regarding surgical procedures were based on shared decision making between clinician and patient. The duration of GnRHa use was not explicitly defined but rather guided by symptomatic relief of pain. GnRHa was typically used for a minimum of 3 months to assess impact on symptoms. The patient stopped GnRHa if symptoms were unacceptable.
All surgeries were performed within the gynaecology units of our hospital. All surgeons had attained accreditation by the Australasian Gynaecological Endoscopy & Surgery Society (AGES) as levels 4–6. All surgeries were undertaken with the aim to treat all visible endometriosis and to remove the uterus and/or ovaries as per pre-operative counselling and patient consent. Surgeries performed did not include removal of other organs affected by endometriosis such as segmental of disc resection.
Due to the retrospective nature of the study, no standardised scoring system was used between clinicians. Pain resolution was based on qualitative data from clinician notes. Pain resolution after GnRHa and surgery were categorised into ‘complete relief’, ‘significant but not complete relief, ‘partial relief’ or ‘no relief. All outcomes were assessed by a single author (MP). A positive response to GnRHa was any reduction in pain during the course of GnRHa while a positive pain response to surgery was any reduction in pain at the 6-week post-operative visit. Intra-operative findings were not documented based on rASRM findings due to the retrospective nature of this paper. Thus, not consistently documented. All intra-operative findings collected include a combination of surgical and histological findings. Long term relief post-surgery was considered attained when no further presentations to the hospital’s emergency or outpatient department for pelvic pain were documented. As patients in the cohort may have attended other health services for pain management, reported long term relief may be artificially high.
Data collection
Patient information was obtained from pharmacy dispensing records, hospital medical records (electronic and paper) and pathology results. Demographic characteristics collected for each patient included age, body mass index (BMI), smoking status, associated diagnosed pain syndromes including bladder pain syndrome (BPS), irritable bowel syndrome (IBS) and fibromyalgia. Previous gynaecological history including a previous diagnosis of endometriosis or adenomyosis as well as previous gynaecological surgeries were also collected. History of previous treatments for pain management within this pain population was not available due to the retrospective nature of this study with paper-based medical records being unavailable. Ultrasounds were not utilised to assess burden of disease after GnRHa as this is not current practice in this health service. Data was then entered in a spreadsheet.
Statistical analysis
Statistical analysis was performed using Microsoft Excel and Stata 16 (StataCorp 2019). Summary analysis and confidence intervals were calculated for the diagnostic accuracy of the primary outcome. 24 A generalised ordered logistic regression analysis was performed to assess the association between the categorical degree of pain response to GnRHa and to surgery. Categorical variables in this paper are presented as counts and proportions Continuous variables are summarised as mean and the associated standard deviation. Due to the small sample size, further analysis was descriptive only.
Results
There were 56 patients included in the analysis. Table 1 demonstrates the collated patient characteristics. The mean age of this cohort was 39 years (SD 6.31) while the mean BMI was 30 kg/m2 (SD = 8.71). Ten patients had associated diagnosed pain syndromes which included BPS, IBS and fibromyalgia. Ninety-five percent (53/56) of patients had previously undergone gynaecological surgery with 21% (11/53) within this group having had a hysterectomy. A previous diagnosis of endometriosis has been made in 71% (40/56) either through histology or a tertiary level ultrasound demonstrating deeply infiltrating endometriosis (DIE).
Patient characteristics.
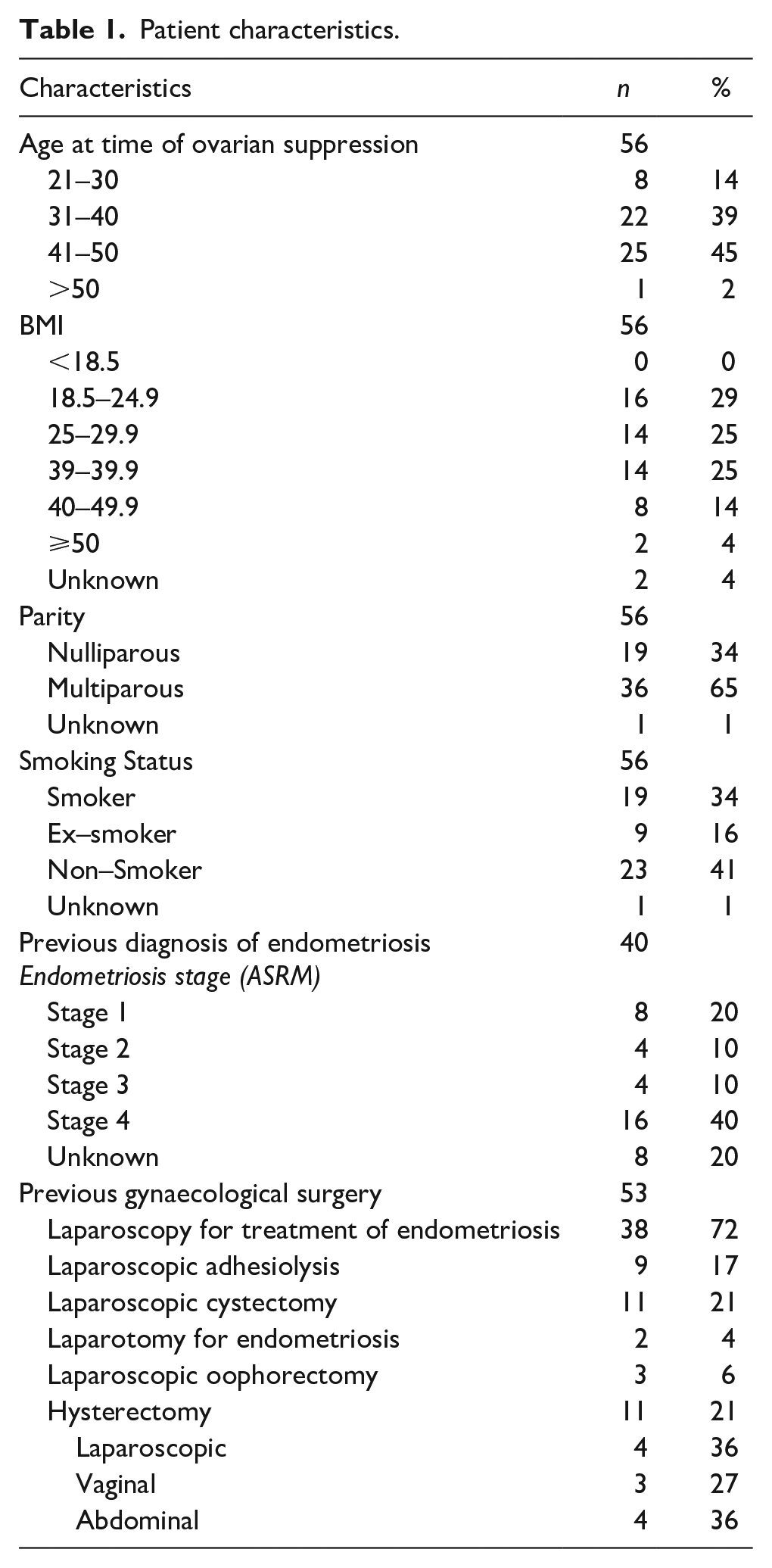
Naferelin was prescribed in 68% (38/56), 23% (13/56) were prescribed goserelin and 9% (5/56) were prescribed both. The mean duration of ovarian suppression was 4.0 ± 2.9 months. Side effects were reported by 45% (25/56) of patients using GnRHa, with 80% (20/25) experiencing vasomotor symptoms, 16% (4/25) experiencing mood disturbances and 12% (3/25) experiencing vaginal dryness. Other side effects described were poor sleep, decreased libido, headaches or migraines, hair loss as well as allergic skin reactions. Eight patients received add-back oestrogen replacements in this cohort. The mean time between starting ovarian suppression and surgery was 7.9 ± 7.6 months and the median time was 5 months.
Primary outcome
The pain responses are summarised in Table 2. Complete data was available for 43 patients in relation to pain response to GnRHa and surgery documented in their hospital medical records while 13 patients did not have their pain response documented to either GnRHa, surgery or both and were not included in the table. Within the documented cohort, 77% (33/43) were prescribed naferelin, 21% (9/43) had goserelin and 9% (4/43) had both agents.
Pain response to GnRHa and subsequent surgery with associated intra-operative findings.
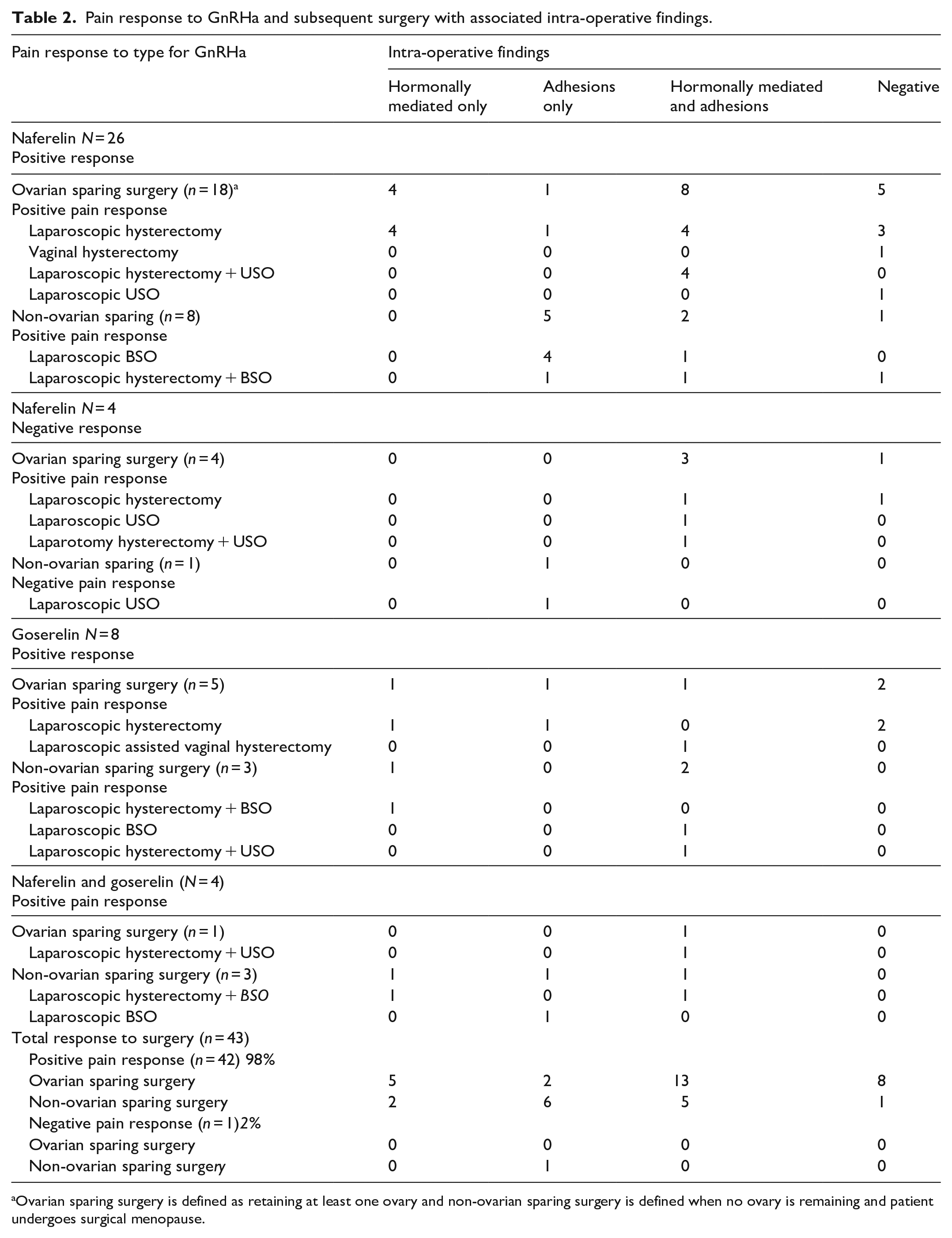
Ovarian sparing surgery is defined as retaining at least one ovary and non-ovarian sparing surgery is defined when no ovary is remaining and patient undergoes surgical menopause.
In this cohort, any positive pain response with GnRHa predicted any positive pain response following surgery with a sensitivity of 90.5% (CI = 77.4%–97.3%), a specificity of 100% (CI = 2.5%–100%), a positive predictive value (PPV) of 100% (CI = 90.7%–100%) and a negative predictive value (NPV) of 20% (CI = 0.5%–71.6%). Comparing the two agents, the sensitivity of naferelin was 100% (CI = 86.8%–100%) with a specificity of 20% (CI = 0.5%–71.6%) while the sensitivity for goserelin was100% (CI = 63.1%–100%). No specificity could be calculated for goserelin as there were no patients who had a negative response.
All 38 women who had a positive pain response with GnRHa had a positive response with surgery. Of these 38 patients, 68% (26/38) had naferelin, 21% (8/38) had goserelin and 10% (4/38) had both. Within this group, 66% (25/38) had ovarian sparing surgery that included 72% (18/25) having a hysterectomy alone, 24% (6/25) had a hysterectomy and USO while 4% (1/25) had a USO only. Of the 34% (13/38) who had non-ovarian sparing surgery, 46% (6/13) had a hysterectomy and BSO while 54% (7/13) had a USO only for a residual ovary.
There were five patients who had no pain improvement with GnRHa with all five having had naferelin. Within this group 80%(4/5) had a positive pain response with ovarian sparing surgery and 20% (1/5) had no relief with non-ovarian sparing surgery. The patient who had no pain improvement with GnRHa or surgery had a laparoscopic USO for a residual ovary.
The rate of recurrence of pain was 21% (12/56) documented as re-presentations to the health service. Within those who represented, 67% (8/12) had reported initial pain reduction post-surgery, two patients had no pain reduction post-surgery and two patients had an unknown pain response post-surgery.
Out of the eight patients who reported an initial positive pain response, seven had an ovarian-sparing hysterectomy while one patient had a bilateral salpingo-oophorectomy after having had a hysterectomy previously. Presentations were to ED by three patients, clinic by eight patients and a private gynaecologist by one patient.
The single patient who had no relief with GnRHa or surgery did not have any documented representations to the health service.
Secondary outcomes
Table 2 summarises the interaction between pain response to GnRHa and positive intra-operative findings. Positive intra-operative findings include endometriosis, adenomyosis, endometriomas and adhesions. All the findings were based on both surgical information and histological information. Within the cohort of patients who had pain reduction with GnRHa 82% (31/38) had positive intra-operative findings while 18% (7/38) did not. Out of the patients who had pain reduction with GnRHa and had positive intra-operative findings, 66% (21/32) had naferelin,19% (6/32) had goserelin and 13% (4/32) had both. This resulted in a sensitivity of 84.2% (CI = 68.8%–94.0%%), specificity of 20.0% (CI = 0.51%–71.6%), PPV 88.9%% (CI = 83.5%–92.7%) and NPV 14.3% (CI = 2.4%–52.7%) for a positive pain response with pre-operative GnRHa predicting intra-operative pathology findings.
Discussion
CPP is a complex issue with multiple potential causes. While there are various causes for CPP, common conditions associated with CPP can be influenced by sex hormones (endometriosis, adenomyosis, ovarian remnant syndrome) and non-hormonal conditions such as pelvic adhesive disease, BPS, pelvic floor dysfunction, central sensitisation and pudendal neuralgia.5,8,26,27 Psychological conditions (depression and anxiety) or a history of sexual and physical trauma are also commonly associate with CPP.7–9,26,27 As a result, individualised management of CPP is essential and the ability to predict likely patient outcomes prior to performing invasive and irreversible procedures could aid in better patient selection and pre-operative counselling.
In our study, we have demonstrated that GnRHa might play a role in selecting patients who would gain from hysterectomy and/or oophorectomy. At present, there have not been many studies looking at the use of pre-operative GnRHa to predict surgical outcomes in women with chronic pelvic pain in particular, All patients who had a positive pain response to GnRHa had a positive pain response resulting in a PPV of 100%. This is also supported by a small observational study that demonstrated that all patients who a had a positive pain response to GnRHa had a positive response with surgery. 21 However, whilst the current study demonstrates a strong correlation between pain reduction with GnRHa and pain reduction with surgery, 80% (4/5) patients who did not achieve pain relief with GnRHa still achieved pain relief with surgery. This is consistent with other studies that quote an expected rate of pain reduction of over 80% with a hysterectomy alone.11,28,29 and up to 90% with a hysterectomy and bilateral oophorectomies.13,29 All patients in our study who did not achieve pain reduction had naferelin, whilst all patients who had goserelin or goserelin and naferelin achieved pain reduction. Due to the small cohort of this study and lack of randomisation, the true efficacy cannot be commented on. The Cochrane review by Brown et al., 29 found no specific GnRHa that can be recommended over another in relieving endometriosis-associated pain. However, there is no documented review when treating chronic pelvic pain. Due to the paucity of literature within the last 10 years that examine the role of GnRHa in patients with CPP, more up to date comparisons cannot be made. Hence, the purpose of conducting this study.
While the use of GnRHa appears promising with the high initial rate of pain reduction post-surgery in patients who had a positive pain response with GnRHa, the rate of long-term pain reduction is unclear. In this study, 19% (8/43) of patients who initially reported pain relief post-surgery, re-presented through the emergency department or gynaecology outpatient clinic with a recurrence of pelvic pain. All these patients had ovarian sparing surgery. This is consistent with previous studies that have demonstrated up to 40% of patients reporting ongoing CPP post hysterectomy.14,30–32 Therefore, while most patients achieved good short term pain reduction with ovarian sparing surgery, it may be the rate of recurrence of pain is relatively increased in this population compared to patients who are rendered menopausal with surgery.
Despite the predicted mechanism of action that GnRHa is thought to have, pre-operative pain response to GnRHa poorly predicted the presence of pathological intra-operative findings of endometriosis, adenomyosis or endometriomas in this study. This is reflected in the 30% of patients who had no abnormal intra-operative findings, not dissimilar to that of other studies with up to 35% of patients having negative intra-operative pathology. 33 However, it is important to note that the use of GnRHa can result in regression of endometriosis or change in the activity of the endometriosis. 34 This may result in false over-representation of negative hormonally mediated intra-operative findings.
While this study’s findings are promising, we recognise its limitations. The retrospective nature of this research lends itself to bias in case selection and data collection, which was not blinded. This study was conducted in a tertiary unit specialising in laparoscopic surgery and pelvic pain that uses GnRHa response as a component of the clinical decision to proceed with surgery. Some of those who did not respond to GnRHa may not have proceeded to surgery, thus creating a selection bias. The small sample size also poses a significant limitation, especially given the small numbers of patients who did not respond to GnRHa and the single patient who did not improve after surgery. This results in wide confidence intervals limiting applications of our findings to clinical care
The patient population is heterogenous and included patients who had different treatment time frames with GnRHa, different types of GnRHa and different types of surgery – those that resulted in surgical menopause and those that were ovarian-sparing. The choice of GnRHa, length of treatment and type of surgery were based on clinician discretion and patient preference and therefore varied.
Another limitation of this study is the lack of both consistent reporting and lack of use of standardised pain rating score such as the visual analogue scale. Pain outcomes were based on qualitative descriptions to determine if a degree of pain relief was achieved which may not have been a true representation of a patient’s pain response.
There was complete data for the short follow-up period (6-week post-operative review). However, this may not accurately reflect longer term outcomes. Our use of re-presentation to our health service as a longer-term follow up measure, is likely to underestimate the true incidence as presentations to other health services were not captured. Despite these limitations, to our knowledge, this is the largest study looking into this topic.
Conclusion
In conclusion, assessment of the pain response to GnRHa may be of value in identifying patients who are more likely to benefit from hysterectomy and/or oophorectomies for CPP. Clinicians may utilise pre-operative GnRHa to aid in patient selection and counselling prior to exploring surgical interventions, but other pain conditions should be considered along with a multidisciplinary approach. To further evaluate the usefulness of GnRHa in predicting effectiveness of surgery in the treatment of CPP, a larger prospective cohort study with standardised interventions and documentation as well as long-term follow-up is needed.
Footnotes
Acknowledgements
None.
Author contributions
MP researched literature performed data collection, data analysis and wrote the first draft of the manuscript. CY conceived the study and gained ethical approval. MP and CY were involved in protocol development and patient recruitment. All authors reviewed and edited the manuscript. All authors approved the final version of the manuscript.
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analysed during the current study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Australasian Gynaecological Endoscopy and Surgery Society (AGES), Grant number 8927.
Ethical approval
Ethical approval for this study was obtained from the The Royal Women’s Hospital (Victoria) Research Committee and The Royal Women’s Hospital (Victoria) Human Research Ethics Committee (AQA20/13). The study (AQA20/13) meets the National Health and Medical Research Council requirement and has been endorsed by the local Institutional Review Board.
Consent to participate
Not applicable.
Consent for Publication
Not applicable.
Trial registration
Not applicable.