
Abstract
Objectives:
We describe an approach to reanimation of complete, prolonged facial paralysis using minimally invasive temporalis tendon transfer (MIT3) by the melolabial or transoral approach. Objective outcome measures are evaluated based on symmetry, and grading of preoperative/post-operative results and the scar at the melolabial fold.
Study Design:
Retrospective cohort study.
Methods:
Twenty-five patients undergoing the MIT3 technique were studied. Photographic analysis was used to determine the percentage of difference between the 2 sides (symmetry). Using the Delphi method to achieve consensus, a panel of experts graded pre/post-operative photos using the Terzis’ Facial Grading System and a 1 to 10 Likert-type scale and the melolabial scar using the Beausang Scar Scale.
Results:
Percentage of difference (symmetry) with smiling improved from 18.6% ± 1.5% (mean ± standard error of the mean [SEM]) preoperatively to 5.0 ± 0.9% (mean ± SEM) post-operatively. Expert grading by the Terzis system showed improvement post-operatively (mean 3.7/5; median 3.6/5) versus preoperatively (mean 1.5/5; median 1.2/5). Perceived improvement was also largely favourable (mean 8.1/10; median 8.0/10). Melolabial scar grading was favourable in terms of colour (mean 1.53/4), surface character (mean 1.05/2), contour (mean 1.60/4), and distortion (mean 1.74/4).
Conclusions:
The MIT3 technique offers immediate, predictable, and symmetrical return of smile function. Objective symmetry analysis and favourable expert grading of both pre-/post-operative photographs and the scar at the melolabial fold demonstrate applicability for facial reanimation in patients where other procedures have failed, or when a direct return to function is desired. Both the melolabial approach and transoral approach were found to be acceptable and effective, although applicability varies.
Introduction
Facial paralysis poses a challenge for reconstructive surgeons, as no single procedure provides complete aesthetic and functional correction. The primary goals of facial reanimation procedures are to restore symmetry and function. In the lower face, this primarily relates to oral competence and the ability to smile symmetrically. Treatment options are determined by both cause of paralysis and its duration. For new-onset facial paralysis, procedures that restore function to the native musculature, when possible, provide the best possible outcome. 1,2 This may involve reinnervation techniques such as cable nerve grafts, cross-facial nerve grafts, and hypoglossal or masseteric nerve transfers. 3 However, these techniques become ineffective in cases of long-standing complete facial paralysis as motor end plate atrophy and fibrosis occur. 1,4 In these cases, options to restore dynamic function in the lower face include free tissue or regional muscle transfer. 3,5
The gold standard for smile restoration remains free tissue transfer with cross-face grafts, offering the possibility of a spontaneous and symmetric smile in many patients. Drawbacks include the need for inpatient surgery, delayed recovery as nerve regeneration occurs, and variability in outcomes. Regional muscle transfer offers a less invasive alternative with a quicker recovery. 6,7 The temporalis sling described by Gillies involves transfer of the origin of the temporalis muscle over the zygomatic arch to the oral commissure. 8 The disadvantages of this technique include the requirement of both a temporal incision for muscle mobilization and the melolabial or a transoral incision for insetting, bulk over the zygomatic arch due to folding down of the temporalis muscle belly, lack of orthodromic contraction limiting temporalis excursion, and the resulting temporal fossa donor site defect. 3 In contrast, temporalis tendon transfer is an orthodromic procedure in which the muscle insertion is transferred to the oral commissure. This may be performed with a temporal incision to allow muscle mobilization 9 or via a single incision at the site of insertion (melolabial or transoral). 10 The temporalis tendon transfer provides essentially immediate correction of long-standing facial paralysis by orthodromic transfer of the temporalis muscle tendon. Proposed advantages include a better vector of pull, greater motor force, stronger attachment due to suturing of tendon rather than fascia, no temporal depression in the donor site, and no tissue protrusion over the zygomatic arch. 3
Herein, we describe an approach to temporalis tendon transposition, the minimally invasive temporalis tendon transfer (MIT3), which can be performed through either the melolabial or the transoral approach. Objective outcome measures are evaluated including the degree of correction achieved, symmetry, oral commissure excursion, and for grading of the scar at the melolabial fold.
Materials and Methods
Patients
From 2003 to 2010, 44 consecutive patients with complete facial paralysis underwent temporalis tendon transposition at our center. Of these, 25 patients had photographs available to satisfy inclusion in our study. Procedures studied included our previously used preauricular/melolabial approach (7 patients) or our MIT3 technique via a melolabial (16 patients) or transoral (2 patients) approach. Approval was obtained from the Johns Hopkins institutional review board. Only patients who had both preoperative and post-operative photos available were studied. Patient age ranged from 23.4 to 80.9 years (mean standard deviation [SD], 53.7 (13.9) years). Table 1 provides a description of the patient population, cause of paralysis, paralyzed side, duration of paralysis, assigned House-Brackmann grade, 11 surgical approach utilized, concurrent procedures performed, and follow-up photo time.
Summary of Patient Characteristics.

Abbreviations: F, female; FT, follow-up time; L, left; M, male; N, nasolabial only (MIT3); PD, paralysis duration; R, right; T, transoral; P/N, preauricular/nasolabial.
Surgical Technique
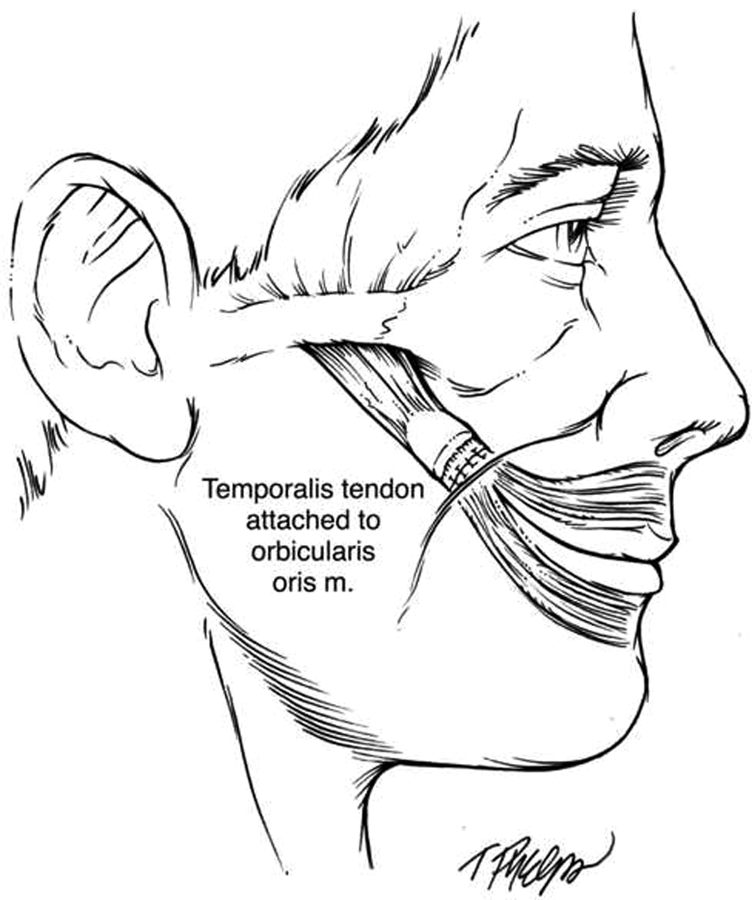
Our group previously described an approach to the temporalis tendon through both a temporal and a melolabial incision involving segmental removal of the zygomatic arch and mobilization of the temporalis muscle origin. 12 We subsequently found this temporal dissection and removal of the zygomatic arch unnecessary, gaining adequate tendon length by subperiosteal dissection toward the buccinator ridge (Figure 1) and oblique osteotomy of the coronoid process (Figure 2). We developed a minimally invasive approach that can be performed via a single melolabial incision that leaves a faint scar in the melolabial fold (Figure 3A) or a transoral approach that leaves no melolabial scar (Figure 3B). 10 The MIT3 procedure via the transoral approach is a modification of McLaughlin’s technique, 9 with the temporalis tendon being directly attached to the oral commissure, typically without the use of fascia lata (Figure 4). The MIT3 procedure through the melolabial approach requires an incision in the melolabial fold to approach the temporalis muscle tendon’s insertion on the coronoid (Figure 5). 10 In both approaches, the patient’s preoperative smile pattern is first determined to choose a proper point of attachment to achieve optimal symmetry. Simple neuromuscular retraining exercises essential to achieving a symmetric smile are initiated preoperatively and are resumed 1 week following surgery. 3
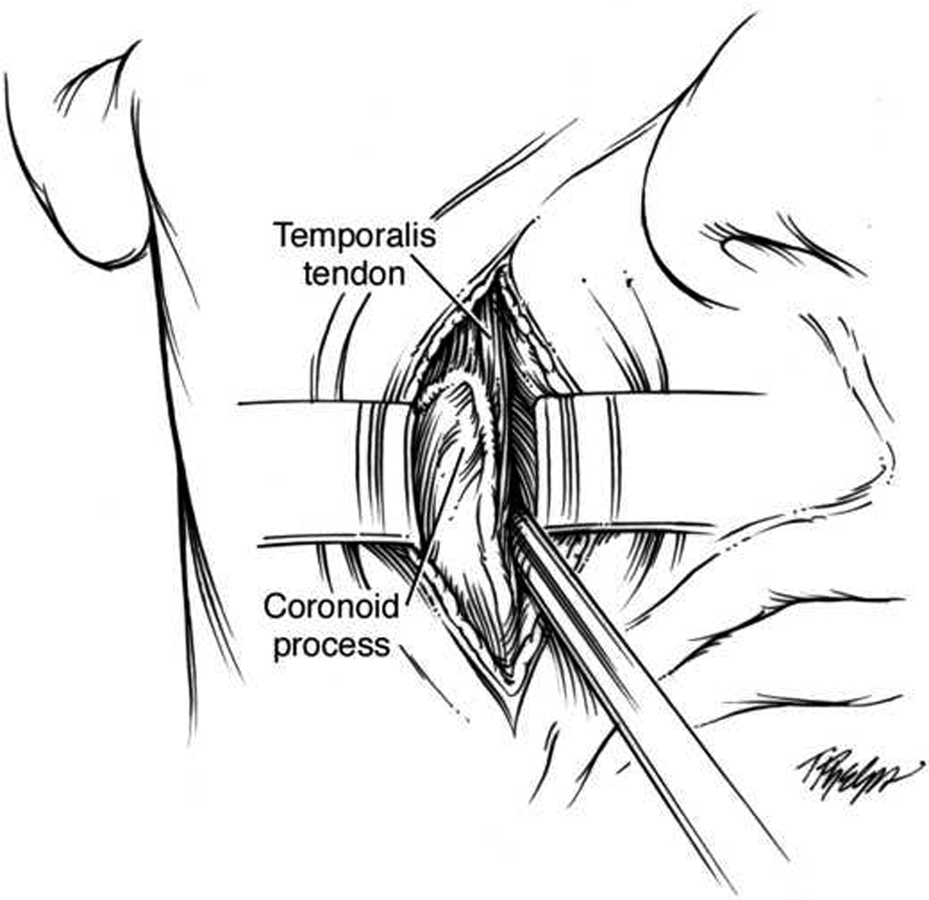
The temporalis tendon wraps around the coronoid process but has an extension along the mandibular ramus down to the buccinators ridge. To gain adequate tendon length, subperiosteal tendon dissection should be carried out towards the buccinator’s ridge.
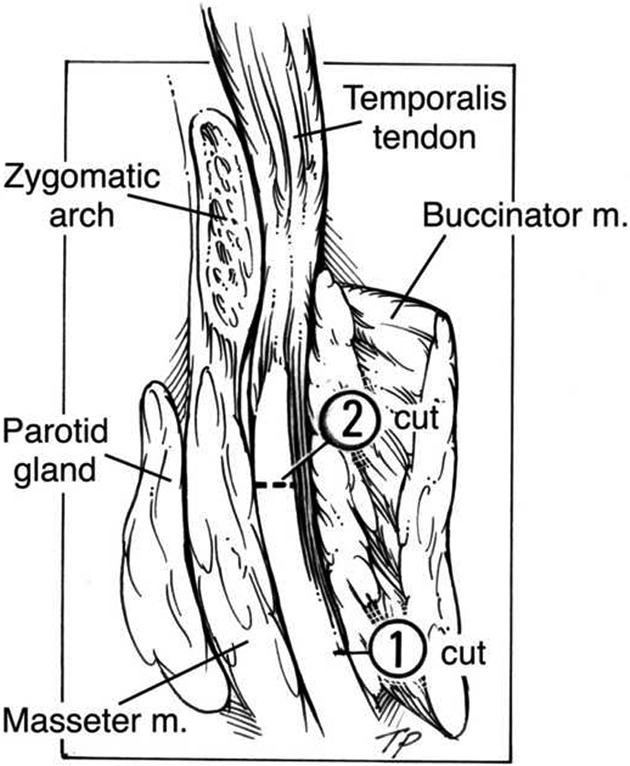
An oblique osteotomy, carried out at the neck of the coronoid process, allows mobilization of the temporalis tendon while preserving the bulk of the tendon’s length.
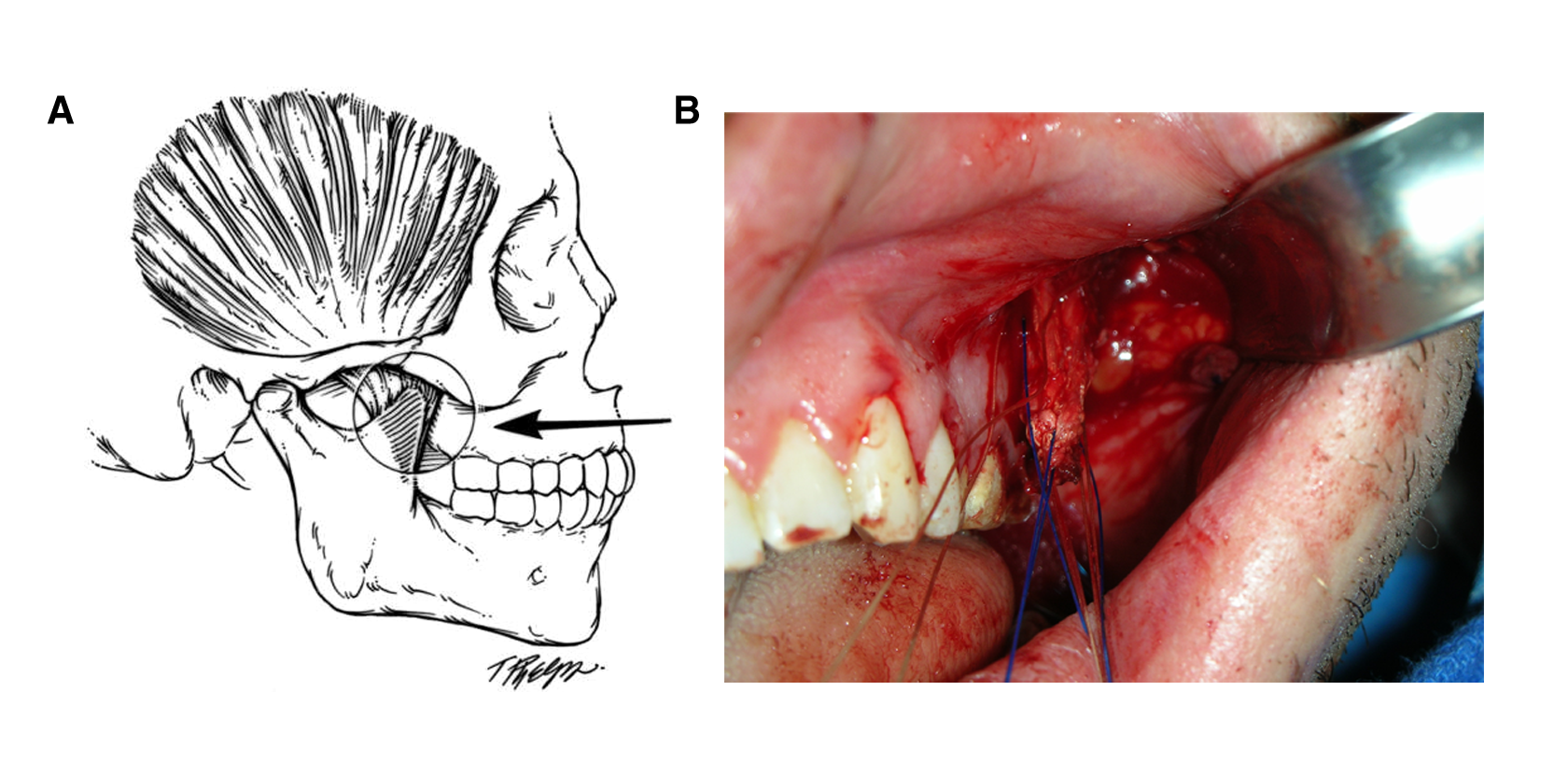
A, Transbuccal dissection through the melolabial fold provides direct access to the mandibular ramus and coronoid process. B, Intra-operative view of the minimally invasive temporalis tendon transfer (MIT3) procedure performed through the transoral approach, showing the detached temporalis tendon.
The temporalis tendon is transposed through the buccal space and fixated at the modiolus based on the smile position on the contralateral side as determined preoperatively.

Intra-operative view of the minimally invasive temporalis tendon transfer (MIT3) procedure using the melolabial approach, showing the temporalis tendon still attached to the coronoid process.
Outcome Measures
Photographic analysis using imaging software (Mirror; Canfield Scientific Inc, Fairfield, New Jersey) was conducted to measure the vertical position of the oral commissure bilaterally preoperatively and post-operatively, at rest, and with smiling. A line drawn between the medial canthi, the intercanthal distance (din), served as a measurement scale and was multiplied by an average din (35.0 mm) to present practical results. 13 This was felt to be accurate, as there are no reports of facial paralysis affecting din. 1,14 -16 The vertical position of the oral commissure was determined trigonometrically by measuring distance from the bisected intercanthal line to the oral commissure and the corresponding angle formed (Figure 6). Computing the percentage of difference in the vertical position of the oral commissure between the paralyzed and the unaffected sides allowed us to determine symmetry.
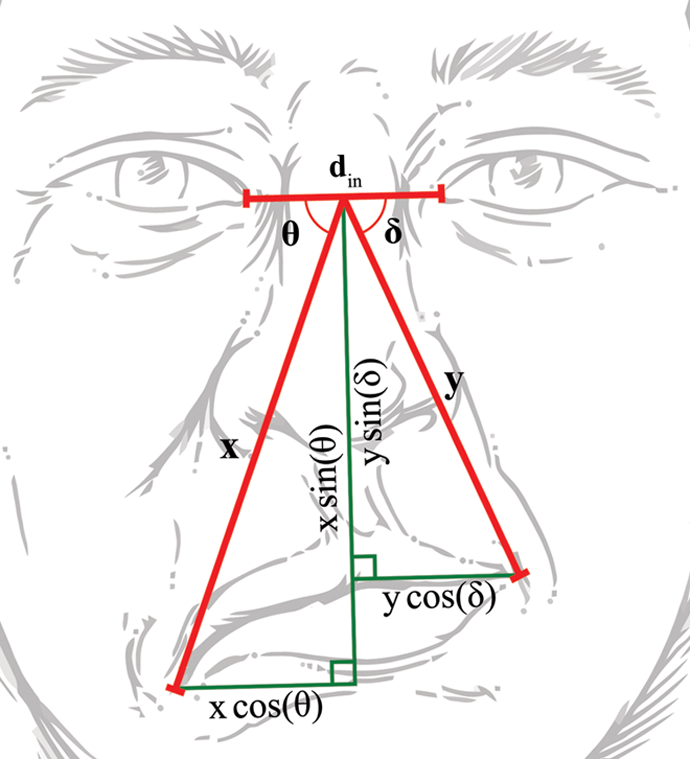
A line drawn from the bisected intercanthal distance (din) to the corner of the oral commissure, the angle (θ, δ) and length (x, y) of which are determined, can be used to determine both the vertical and lateral position of the oral commissure by using trigonometric functions.
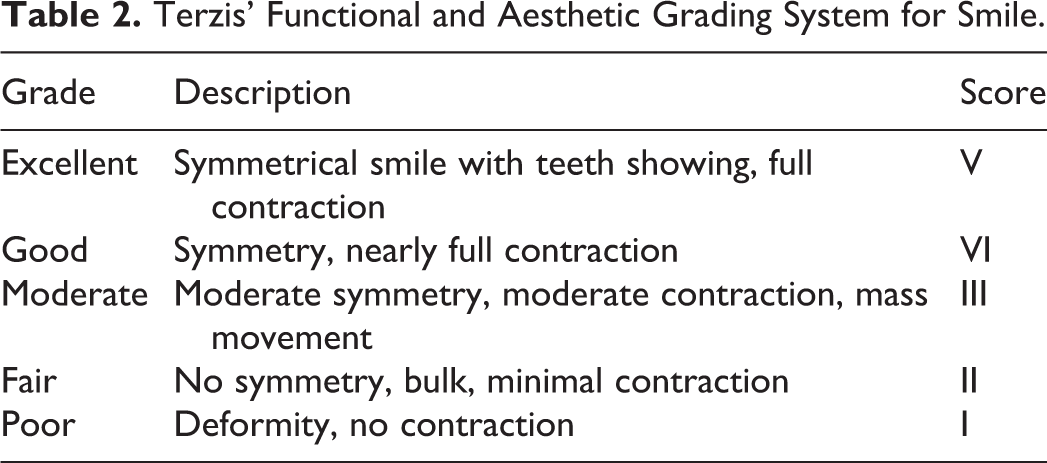
Five surgeons from outside our division experienced in the treatment of facial paralysis evaluated preoperative and post-operative photographs. Surgeons were blinded to all information apart from the paralyzed side and photograph follow-up time after surgery. Photographs were graded using the Terzis’ Facial Grading System 17 (Table 2) and by a perceived improvement score post-operatively compared to preoperatively from 1 to 10 (where 10 is excellent or dramatically better, 7 is good or moderately better, 5 is neutral or no change, 3 is bad or moderately worsened, and 0 is very bad or dramatically worsened). The panel likewise graded the scar at the melolabial fold using the Manchester Scar Scale 18 (Figure 7).
Terzis’ Functional and Aesthetic Grading System for Smile.
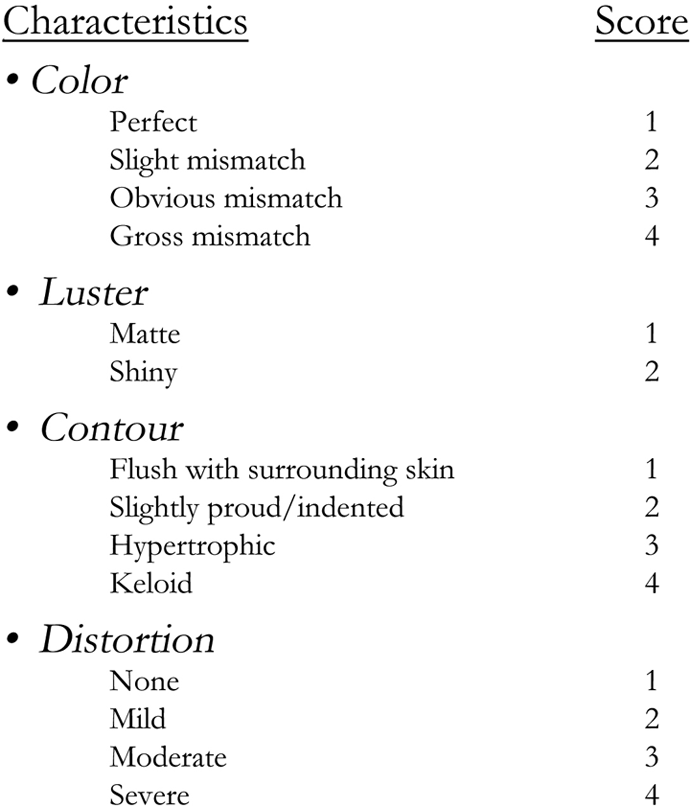
The Image Assessment Panel for scar assessment developed by Beausang et al was used in order to grade the resulting scar at the melolabial fold.
The Delphi method, defined as “a multiple iteration technique usually meant to be anonymous with the purpose of refining the expert opinion and ultimately arrive at a combined or consensual position,” 19 was utilized to reach expert consensus for preoperative and post-operative grading as well as scar grading. The panel was surveyed using paper surveys and responses were kept anonymous. In the initial survey, the grading process was explained. Following the first round of grading, results were deidentified to reduce interobserver discrepancy, compiled, summarized, and distributed among the group for review and discussion. The panel was then again surveyed using the same method, and results were compiled and analyzed.
Statistical Analysis
Standard error of the mean was computed for symmetry between the 2 sides. A 2-tailed unpaired t test was done to determine if a difference in outcomes existed between the previously invasive approach and the new minimally invasive approach, with a P value <.05 being consider statistically significant.
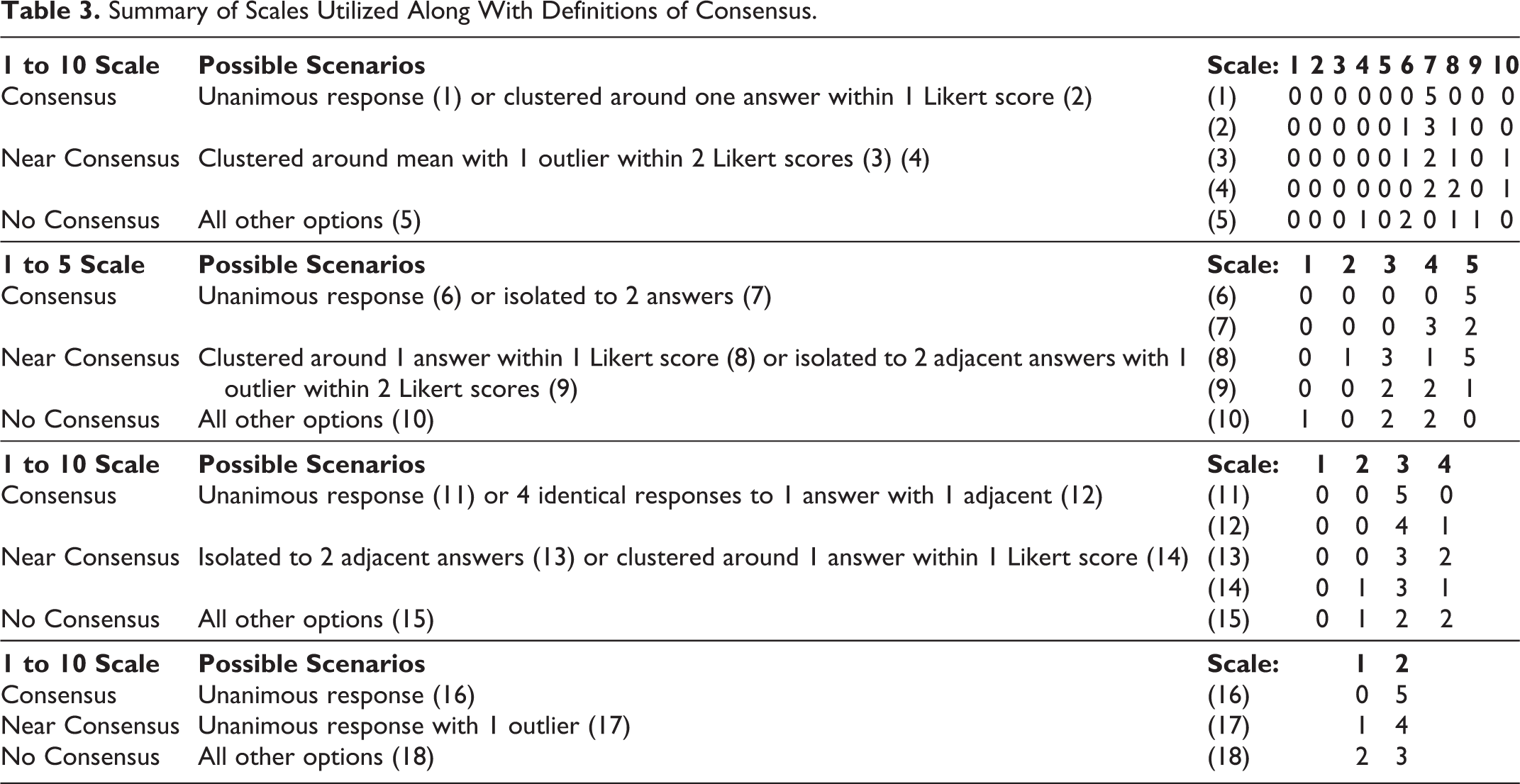
The Delphi method was employed to determine which items reached consensus, near consensus, and no consensus by the panels of experts. Due to the use of 3 distinct grading scales with 4 numbered scales, the definition of what constituted consensus, near consensus, and no consensus had to be defined separately in each case, although an attempt was made to maintain uniformity (Table 3). Median and mean values are reported for the responses of each survey question.
Summary of Scales Utilized Along With Definitions of Consensus.
Results
Follow-up time from surgery ranged from 0.7 to 14.4 months with a mean of 3.4 ± 0.9 months (mean ± standard error of the mean [SEM]). Photographic analysis using imaging software (Mirror) was conducted to measure commissure position, allowing determination of symmetry with smiling by computing the percentage of difference between the vertical positions of the oral commissure on the paralyzed side compared to the unaffected side (Table 4). Four patients were excluded from our symmetry analysis due to not having a preoperative smile photo.
Comparison of Pre-Operative and Post-Operative Smile Symmetry Based on Vertical Position.
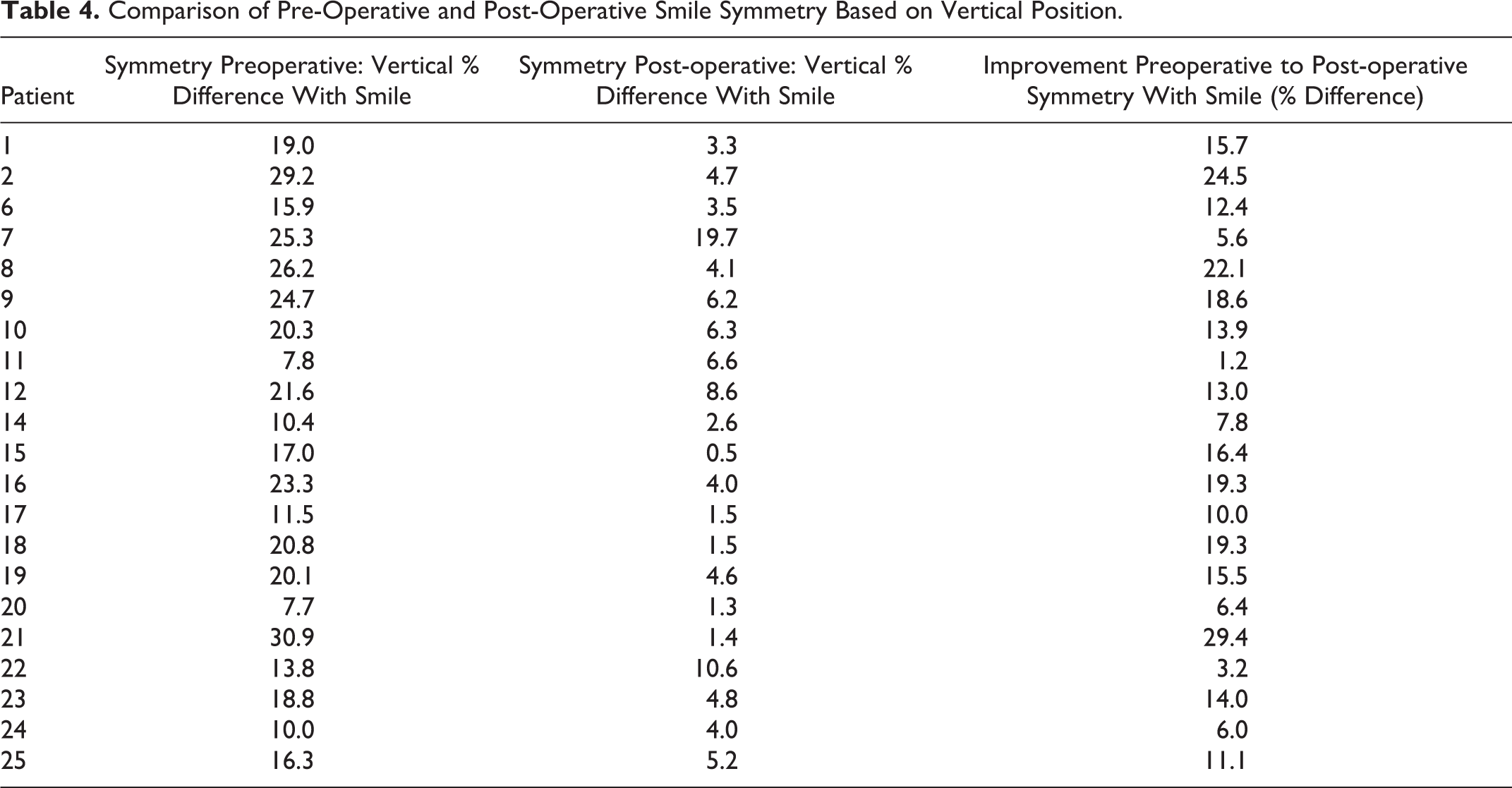
The percentage of difference in vertical elevation with smiling preoperatively was 18.6% ± 1.5% (mean ± SEM) and post-operatively was 5.0% ± 0.9% (mean ± SEM), an improvement in the percentage of difference of 13.6% ± 1.6% (mean ± SEM). Statistical analysis between our previously used invasive preauricular/melolabial approach, and our novel MIT3 procedure by either the transoral or melolabial approach, shows no significant difference in symmetry with smiling (P = .39). Figures 8 and 9 demonstrate achieved surgical outcomes together with objective measurements.

Patient #3 is a 42-year-old woman who presented to our center with a greater than 5-year history of House-Brackmann grade V facial paralysis. She is shown preoperatively at rest (A), preoperatively with smiling (B), post-operatively at rest (C), and post-operatively with smiling (D). Vertical change at rest post-operatively (C) improved by 1.64 cm and vertical change with smiling (D) improved post-operatively by 1.92 cm. Smile symmetry improved from 18.3% preoperatively (C) to 9.7% post-operatively (D).
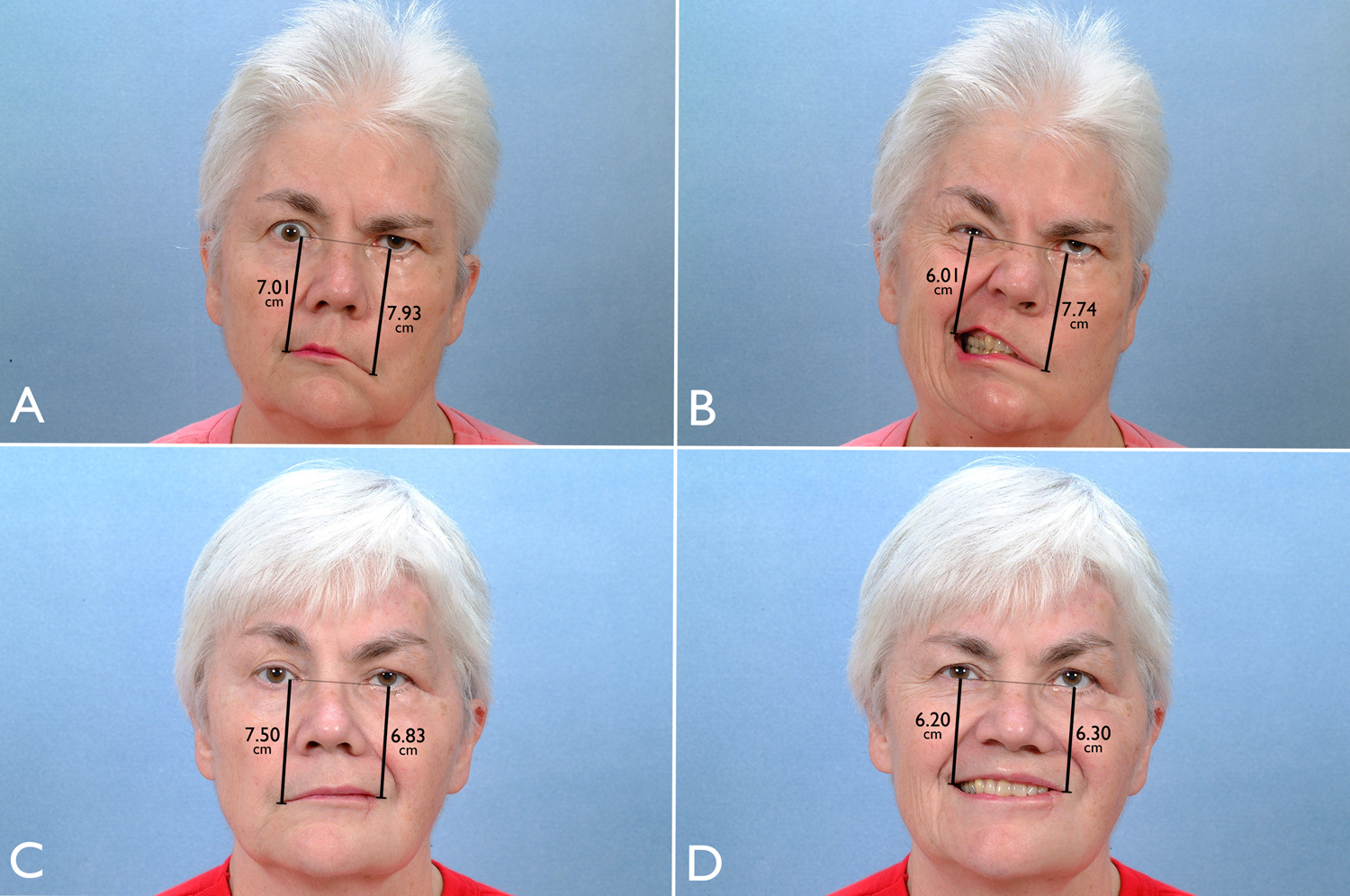
Patient #5 is a 62-year-old woman who presented to our center with a nearly 2-year history of complete facial paralysis. She is shown preoperatively at rest (A), preoperatively with smiling (B), post-operatively at rest (C), and post-operatively with smiling (D). Vertical change at rest post-operatively (C) improved by 1.10 cm and vertical change with smiling (D) improved post-operatively by 1.62 cm. Smile symmetry improved from 22.3% preoperatively (C) to 1.7% post-operatively (D).
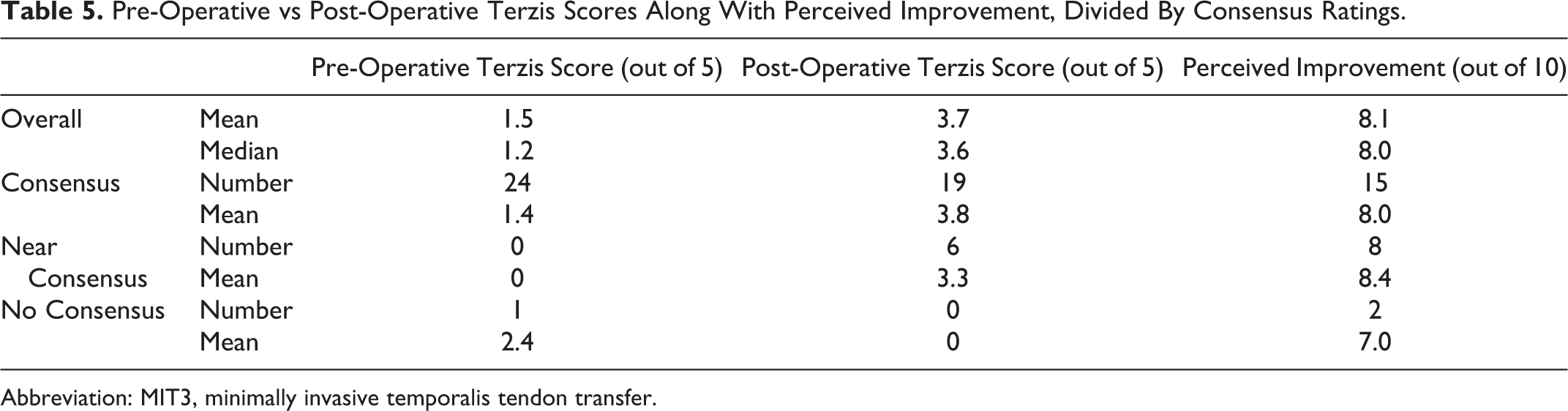
Using the Terzis scoring system, surgeons overall found there to be improvement post-operatively (mean 3.7; median 3.6) compared to preoperatively (mean 1.5; median 1.2) with the MIT3 procedure (Table 5). Perceived improvement as judged by surgeons was also largely favourable (mean 8.1; median 8.0). For preoperative Terzis scores, 24 items reached consensus, 0 near consensus, and 1 no consensus. For post-operative Terzis scores, 19 items reached consensus, 6 near consensus, and 0 no consensus. For perceived improvement, 15 items reached consensus, 8 near consensus, and 2 no consensus. Despite some items not achieving complete or near consensus, examination of individual questions shows that surgeons felt each patient achieved some degree of improvement, with no patients achieving a worsened outcome.
Pre-Operative vs Post-Operative Terzis Scores Along With Perceived Improvement, Divided By Consensus Ratings.
Abbreviation: MIT3, minimally invasive temporalis tendon transfer.
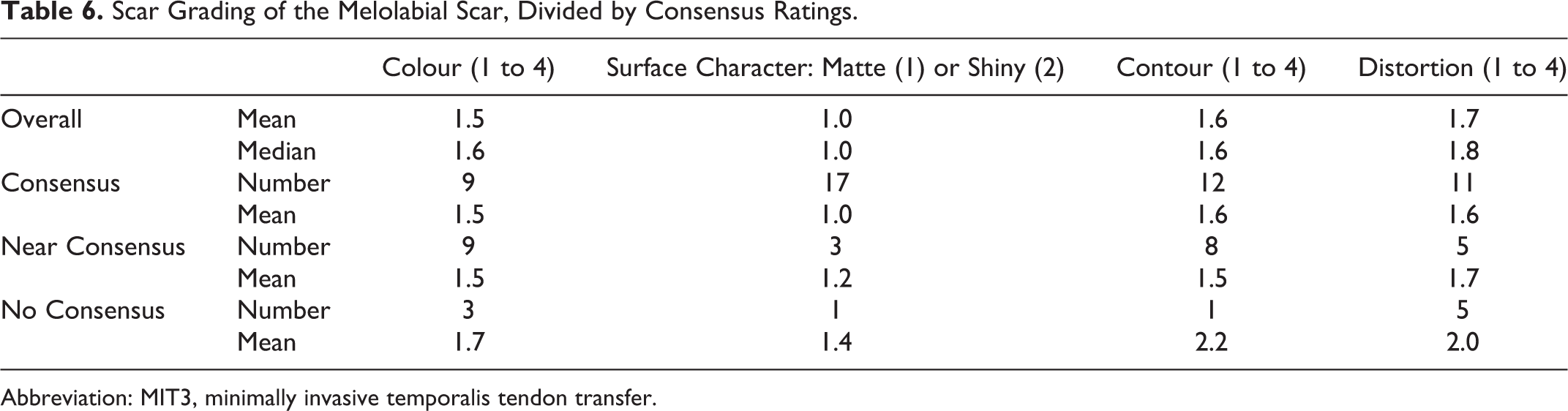
Grading of the scar at the melolabial fold following the MIT3 procedure was performed. For colour, 9 items reached consensus, 9 near consensus, and 3 no consensus. For surface character, 17 items reached consensus, 3 near consensus, and 1 no consensus. For contour, 12 items reached consensus, 8 near consensus, and 1 no consensus. For distortion, 11 items reached consensus, 5 near consensus, and 5 no consensus. Surgeons were generally in consensus, or near consensus, in all 4 grading categories (Table 6). Surgeons rated the scars favourably in terms of colour (mean 1.53—perfect to slight mismatch), surface character (mean 1.05—matte), contour (mean 1.60—flush to slightly proud), and distortion (mean 1.74—none to mild).
Scar Grading of the Melolabial Scar, Divided by Consensus Ratings.
Abbreviation: MIT3, minimally invasive temporalis tendon transfer.
Discussion
In cases of long-standing complete paralysis where reinnervation techniques are not possible, the options for facial reanimation include free tissue transfers and adjacent muscle transfers. The gold standard for a spontaneous and symmetric smile is a gracilis free flap powered by a cross-facial nerve graft. However, this strategy has some potential drawbacks. Free tissue transfer requires a period of reinnervation lasting many months, 12 requires multiple stages, has the possibility of reinnervation failing, may cause asymmetry due to the added bulk of transferred tissue, and will often require future revisions. 1,5,20 The gracilis muscle may add noticeable facial bulk and contribute to asymmetry. Chuang found that only 50% of patients achieved satisfactory results, and many required revision procedures such as debulking, contracture release, upper and lower lip revisions, blepharoplasty, brow lift, facelift, or fat injection. 5 Similarly, Terzis found that 72% of patients requiring a third stage of revisions. 21 These limitations mean that the use of regional muscle transfers remains a popular choice in some patients. The temporalis muscle provides a near ideal vector of pull, resulting in a contractile force perpendicular to the melolabial fold and producing a symmetrical smile. 17
Our group finds the MIT3 procedure to be effective in cases of long-standing complete facial paralysis, in patients who are either not good candidates for free tissue transfer, or those desiring a single-stage procedure with rapid recovery. Candidates for the procedure must have a functioning temporalis muscle. The MIT3 procedure can be performed concurrently with nerve grafting. This is particularly helpful in oncologic cases, such as radical parotidectomies, in which the tendon transfer is performed concurrently. Cable nerve grafting can be performed prior to or following temporalis tendon transfer. In such cases, we find the oral commissure elevation to be more durable and predictable than that achieved with static slings.
A key advantage of the MIT3 procedure over the classic temporalis sling (and in some respects, free tissue transfer) is the elimination of any newly created change in facial symmetry. The effective treatment of facial paralysis requires a systematic and meticulous effort to improve facial symmetry. Many procedures that restore dynamic function can unfortunately add volume to the midface and even cause temporal depression. The temporal depression of the classic temporalis sling can be limited by the use of temporal implants or by approximation of the temporal fascia. Although the muscle over the arch may atrophy, the MIT3 procedure avoids these issues entirely.
We find the MIT3 procedure to be an effective, predictable, and easy-to-perform dynamic facial reanimation procedure. The transfacial approach may result in severing the zygomaticus major, zygomaticus minor, and levator labii superioris, all of which are reapproximated at the time of closure. However, since this procedure is performed only in patients with complete, long-standing paralysis, these factors are minimal concern. We find the facial scar of the melolabial approach to have minimal impact, as it heals well and is hidden in the melolabial fold (Figure 10). The melolabial approach to the coronoid provides direct access to the temporalis tendon without the need for extensive dissection and osteotomies as in the preauricular/melolabial approach. The transoral approach does not create a scar in the melolabial fold and is preferred in most patients, as long as the contralateral crease is minimal or absent. If a crease is present on the contralateral side, a melolabial incision may be chosen for access to the coronoid. Statistical analysis shows no significant difference in outcome between the invasive approach we utilized previously and our minimally invasive approaches, and surgeon’s overwhelmingly graded the scar favourably.

Patient #16 is a 64-year-old woman who received the minimally invasive temporalis tendon transfer (MIT3) procedure via the melolabial approach. The resulting scar is hidden in the melolabial fold on the right side and is shown at 16 weeks post-operatively.
Inadequate temporalis tendon length has been cited as a limitation of this procedure. Fascia lata extensions and releasing incisions at the posterior third of the temporalis muscle origin have been used as solutions. 9,22 In the MIT3 technique, elevating the temporalis tendon off the medial surface of the mandibular ramus down to the buccinator line, and transecting the coronoid in an oblique fashion to ensure maximum tendon attachment avoid these problems. In most of the cases of this series, released temporalis tendon length was sufficient to reach the oral commissure without need for fascia lata extensions. However, we did elect to use fascia lata extensions in 6 cases and acellular dermis in 7 other cases. This was performed when the philtrum was markedly deviated to the contralateral side. Fascia lata or acellular dermis was tunneled into the lips to pull the philtrum toward the midline. 23
Objective symmetry results show a distinct improvement with smiling in all patients. Objective grading of the preoperative and post-operative photos by surgeons confirms this as surgeons felt that all patients benefited from the procedure in some way, with no patients achieving a worsened outcome. Consensus or near consensus was achieved in the majority of cases, and only these values were used in analysis. Using the Terzis scale, surgeon’s rated 96% of preoperative images as being poor to less than moderate (average 1.5/5), compared with only 17% of post-operative images rated poor to less than moderate and 83% being considered above moderate to excellent (average 3.7/5). Similarly, by the perceived improvement scale 83% of patients achieved a good to excellent result, and 15% a neutral to good result (average 8.1/10). These results indicate that generally surgeon’s felt the procedure yielded very favourable results.
Short follow-up time may be seen as a limitation of this study. However, this was chosen to minimize confounding factors. Although many of our patients had later follow-up photos available, these were often taken after additional surgical procedures. We chose instead to use photos that were taken without any additional procedures having been performed apart from those concurrently.
Conclusion
The MIT3 technique offers immediate, predictable, and symmetrical return of smile function that has several distinct advantages over procedures such as the classical temporalis muscle transfer, free tissue transfers, or other reinnervation techniques. Our group’s experience, combined with our objective symmetry analysis and the results of expert grading, lead us to conclude that this procedure is an effective approach to facial reanimation in certain patients when other procedures have failed or when a direct return to function is desired. Expert consensus has established that the procedure largely provides positive results, and has likewise found that the scar created at the melolabial fold is not significant and is an acceptable concession for improved function. As such, there is no statistically significant difference between the melolabial and transoral approach, and both are applicable depending on unique patient factors.
Footnotes
Authors’ Note
Each of the authors has contributed to, read and approved this manuscript. This manuscript has not been previously published, nor is it under consideration elsewhere.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.