
Abstract
Objective:
Perforator flaps are one possible surgical treatment for burn scar contractures; however, a review of evidence on this topic is lacking.
Methods:
MEDLINE was searched for articles related to perforator flaps for burn contractures. Following title and abstract screen, full texts were searched to identify articles describing perforator flaps for burn scar joint contractures. Data were extracted and summarized descriptively. Only articles that contained ≥10 patients with burn scar contracture were considered.
Results:
Two hundred forty-eight articles were identified, of which 17 met criteria for review. Of these, 16 were low-quality case series, while 1 was an open randomized controlled trial. In total, perforator flaps were performed on 339 patients (age range: 3-75 years), with the most common contracture locations being cervical (n = 218) and knee (n = 41). Nine of the 17 articles described a rehabilitation strategy. In general, functional outcomes were excellent, with the majority of patients experiencing return of normal joint range of motion and no recontracture. Compared to full-thickness skin grafts, perforator flaps showed greater improvements in joint range of motion. Cosmetically, perforator flaps were shown to have good color match with surrounding tissue, good contour around anatomical landmarks, and improved overall patient appearance. The most common complications were marginal flap necrosis (n = 26 patients) and venous congestion (n = 17 patients).
Conclusions:
Preliminary evidence from low-quality case series and 1 high-quality trial suggests perforator flaps may be successful for resurfacing released burn scar contractures; however, there is a need for additional trials comparing perforator flaps to other approaches.
Introduction
Burns represent a major cause of morbidity worldwide. 1 While resuscitation and management of burns has greatly improved over the past many years, many patients still experience ongoing functional and cosmetic disability from burn scar contracture. Burn scar contractures of the skin are more likely to occur following deep partial thickness or full-thickness burns that do not receive primary excision and skin grafting but may also occur after excision and skin grafting. The shortened and abnormally tight scar tissue may be a consequence of abnormal scar remodeling, inappropriate initial management, or lack of physical rehabilitation following burn injury. Recent studies have suggested that 23% to 54% of individuals admitted to burn units and requiring autograft eventually develop a burn scar contracture associated with some disability. 2 –5
Burn scar contractures can cause abnormal or limited motion. 6 Epidemiologically, the most common joint to experience contracture is the shoulder; however, any joint or tissue surface that experiences a major burn is susceptible. 3,4 The incidence of burn scar contractures may be reduced by implementing early physical rehabilitation intervention following burn injury. 7,8 On the other hand, it has been shown that while helpful, early joint stretching does not completely eliminate the occurrence of burn scar contractures. 9,10 Recent mathematical models of wound healing have suggested that a threshold exists, beyond which even early and aggressive physical rehabilitation may not influence burn scar contracture formation. 11 Once burn scar contractures have become established, surgical intervention is often necessary to release the contracture, followed by physical rehabilitation to maintain the increased range of motion and function of the affected joint.
When managing burn scar contracture, there is surprisingly little scientific evidence to support one surgical approach over another. 12 Our experience suggests the most common approach involves contracture release, followed by resurfacing of the resulting defect with a skin graft—a procedure first introduced over 100 years ago. 13 Flaps are used when the resulting defect has exposed bone, tendon, joint capsule, or any other non-graftable surface. It may be that even in cases where the wound base is graftable, the thicker, more pliable coverage afforded by a flap is desirable; a perforator flap represents 1 flap option. Perforator flaps, designed to contain a source vessel, theoretically import skin and soft tissue with robust perfusion and greater pliability than a skin graft. However, evidence on the clinical outcomes of perforator flaps for burn scar contracture reconstruction is limited. This is a problem for the practicing plastic surgeon, as there is currently no summary of the best available evidence for reference when managing a patient who may benefit from such a procedure.
Given the scarce evidence on the topic of perforator flaps for burn scar joint contractures, we sought to conduct a literature review on the topic and summarize the best available evidence. The purpose of this article is to review reported cases where perforator flaps were used for reconstruction following release of cutaneous burn scar joint contractures and to summarize the rehabilitation, functional, cosmetic, and safety outcomes of this procedure. It is hoped that this review may serve as a resource for surgeons considering reconstruction of burn scar contractures with perforator flaps and highlight potential benefits and concerns for those involved in the management of patients with burn scar contracture.
Methods
The full study selection process is shown in Figure 1. MEDLINE was searched using the following strategy: [(perforat*.mp AND flap*.mp) OR Perforator Flap (MeSH)] AND [burn*.mp OR Burns (MeSH)]. The search was performed without any restrictions to date or language and revealed 248 articles.
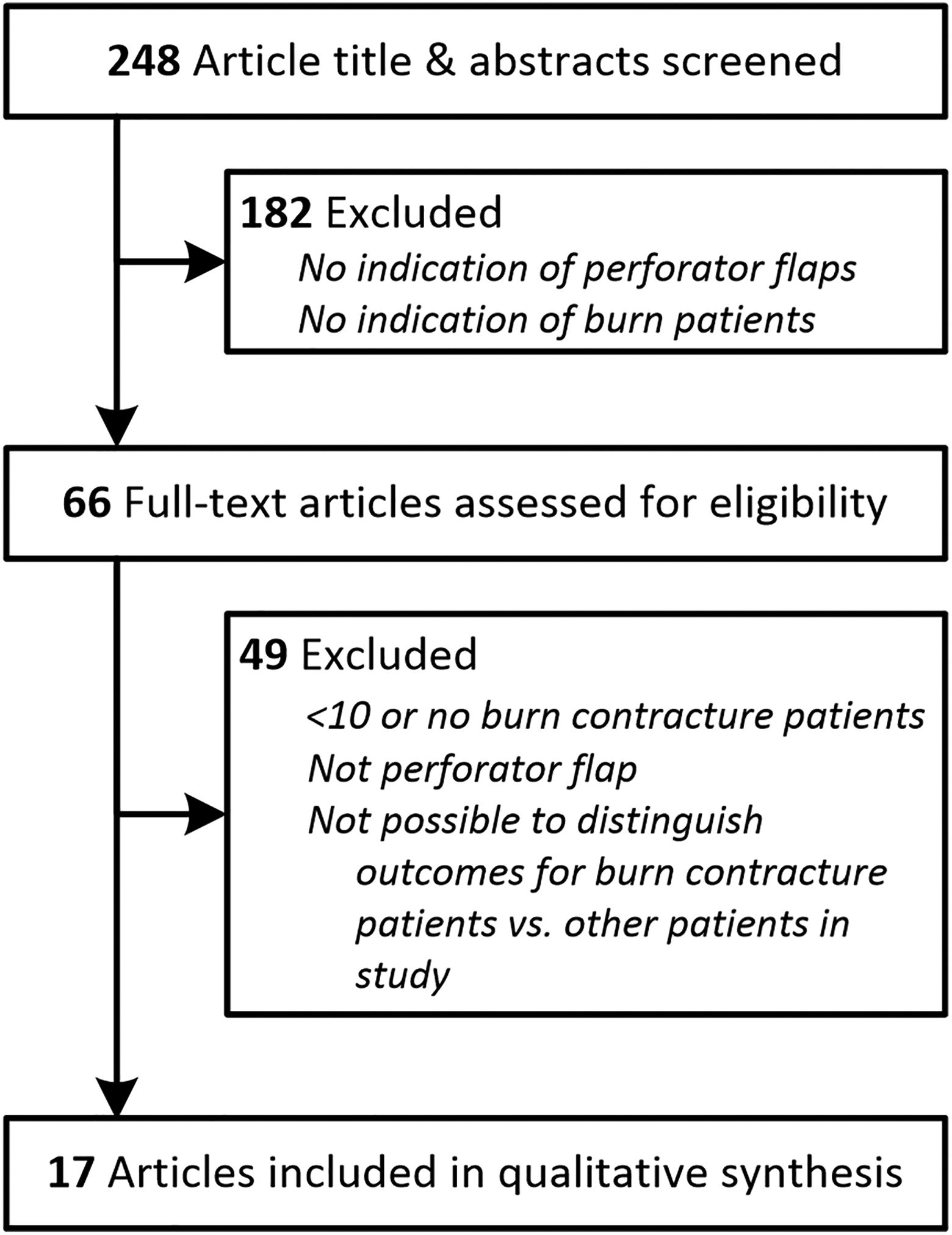
Process flowchart for selecting articles for review. Some articles contained patients with burn contracture and other surgical indications. In these cases, the article was only retained for review if outcomes specific to the burn contracture patients were reported.
Articles identified by the initial search were then reviewed individually by title and abstract to select articles of potential relevance to our review, based on whether the article might address burn scar contracture or perforator flaps. In total, 66 articles were identified by title and abstract screen that were of potential relevance for our review.
Finally, each of the 66 articles were reviewed in full text to select the articles that would be included in the review. Primary inclusion criteria were (1) surgical management of burn scar contracture and (2) use of perforator flaps. As the vast majority of the identified articles were isolated case studies, secondary inclusion criteria were applied to enhance the overall quality of evidence provided for this review: (1) articles must report on at least 10 cases of burn scar contracture and (2) articles must provide data specific to burn scar contracture patients. Using these criteria, articles containing reports of patients with burn scar contracture as well as other surgical indications were only considered if there were at least 10 burn scar contracture patients and with data specific to burn scar contracture patient outcomes distinguished from other patient outcomes. Together, these criteria help to ensure a minimum amount of person-time follow-up in each study and allow for greater statistical power from each study, together serving to reduce bias. This resulted in 17 articles that were eligible for inclusion in the review.
In this review, we considered a broad definition for perforator flaps to be any of the following (Figure 2): (1) a pedicled flap in which the flap site was planned to prevent transection of a known cutaneous perforator supplying the flap, (2) an island flap with a retained intact vascular perforator, or (3) a free flap with a transected vascular perforator that would be anastomosed at the defect site. Importantly, it must be acknowledged that pedicled flaps are not typically considered true perforator flaps. They were considered in this review only on the basis of an important distinction between pedicled perforator flaps and standard pedicled flaps: that the authors intentionally identified a known cutaneous perforator, usually by Doppler, and actively planned surgery around preservation of this vascular supply. This is similar to an island flap, but without full tissue dissection and elevation. This is in contrast to standard pedicled flaps where the collateral blood supply to the flap is not necessarily planned in advance, and instead assumed. While this broad definition of perforator flaps is atypical, it was considered here for completeness in summarizing all studies that used any attempt to preserve a known perforating vessel in flap design, given the paucity of summary data on this topic. Since our initial search strategy was broad and utilized standard terminology of true perforator flaps, inclusion of pedicled perforator flaps would not affect identification of true perforator flaps (ie, island and free flaps) and instead only served to broaden our review.
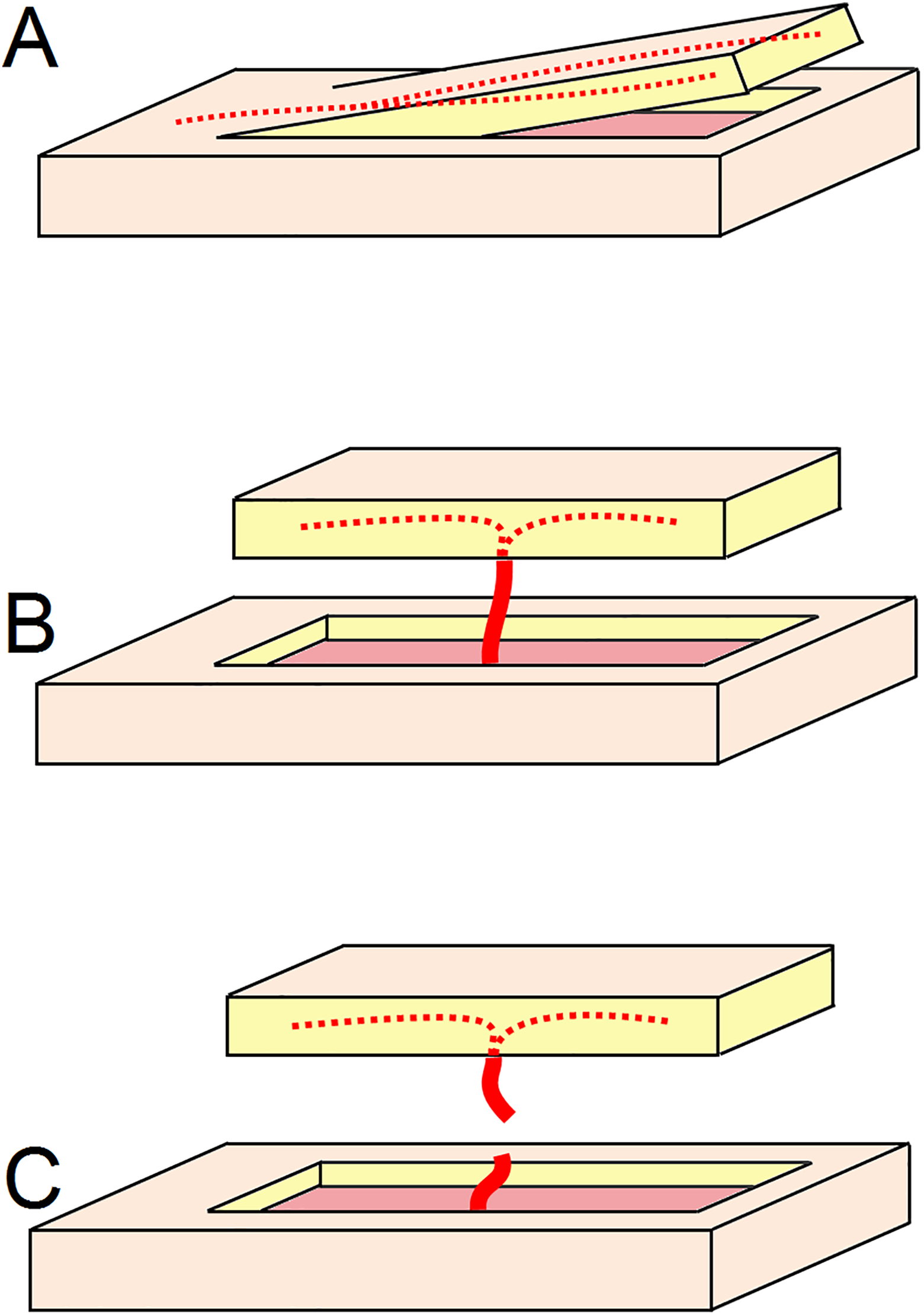
Definitions for method of flap elevation used in this review. A, Pedicled flap, where a bridge of healthy tissue remains intact with a known cutaneous perforator supplying the elevated flap. B, Island flap, where a perforator is dissected but left intact. C, Free flap, where the perforator is dissected and then transected with the intent of anastomosing the vessel at a distant site. In each, the red lines represent the perforator source to the flap. (A) and (B) may be referred to as local flaps, as their use is restricted by the length and/or maneuverability of the tissue or vascular pedicle.
The identified articles were typically case series with heterogeneous patients, surgical methods, and outcomes descriptions. Consequently, meta-analyses of data were determined to be inappropriate. Therefore, we extracted all relevant information from each article and summarized data across articles descriptively. Data extraction was performed and confirmed by 2 researchers (R.T.L. and L.C.C.). To provide indication of study quality, we utilized the Oxford Centre for Evidence Based Medicine (OCEBM) Levels of Evidence framework for treatment studies, which provides both a level of evidence for each individual study and an overall grade of recommendation for the data supplied in this review. 14 Study quality was assessed and confirmed by 2 researchers (R.T.L. and L.C.C.).
Results
A total of 248 articles were identified, of which 17 met criteria for review (Figure 1). Table 1 shows a summary of study levels of evidence, while Tables 2 and 3 show characteristics of all articles, flaps, and outcomes, grouped by contracture location. The majority of articles originated from outside of North America and all but 1 were case series (level of evidence 4) of perforator flap surgery. As such, overall study quality in this review was low, with an overall evidence grade of recommendation of C for perforator flaps for burn scar contracture. However, 1 article was a high-quality open randomized controlled trial (level of evidence 2) comparing perforator flaps (usually pedicle flaps) to full-thickness skin grafts (FTSG). 30 This trial found that perforator flaps resulted in greater improvements in range of motion and surface expansion compared to FTSGs without compromising skin elasticity. Furthermore, this study found that observers rated the appearance of flaps as better than FTSGs, while patients found no difference between the two. Those with perforator flaps had less color mismatch compared to those with FTSGs. Perforator flaps also had a lower rate of necrosis compared to FTSGs.
Study Quality and Overall Quality of Evidence.a
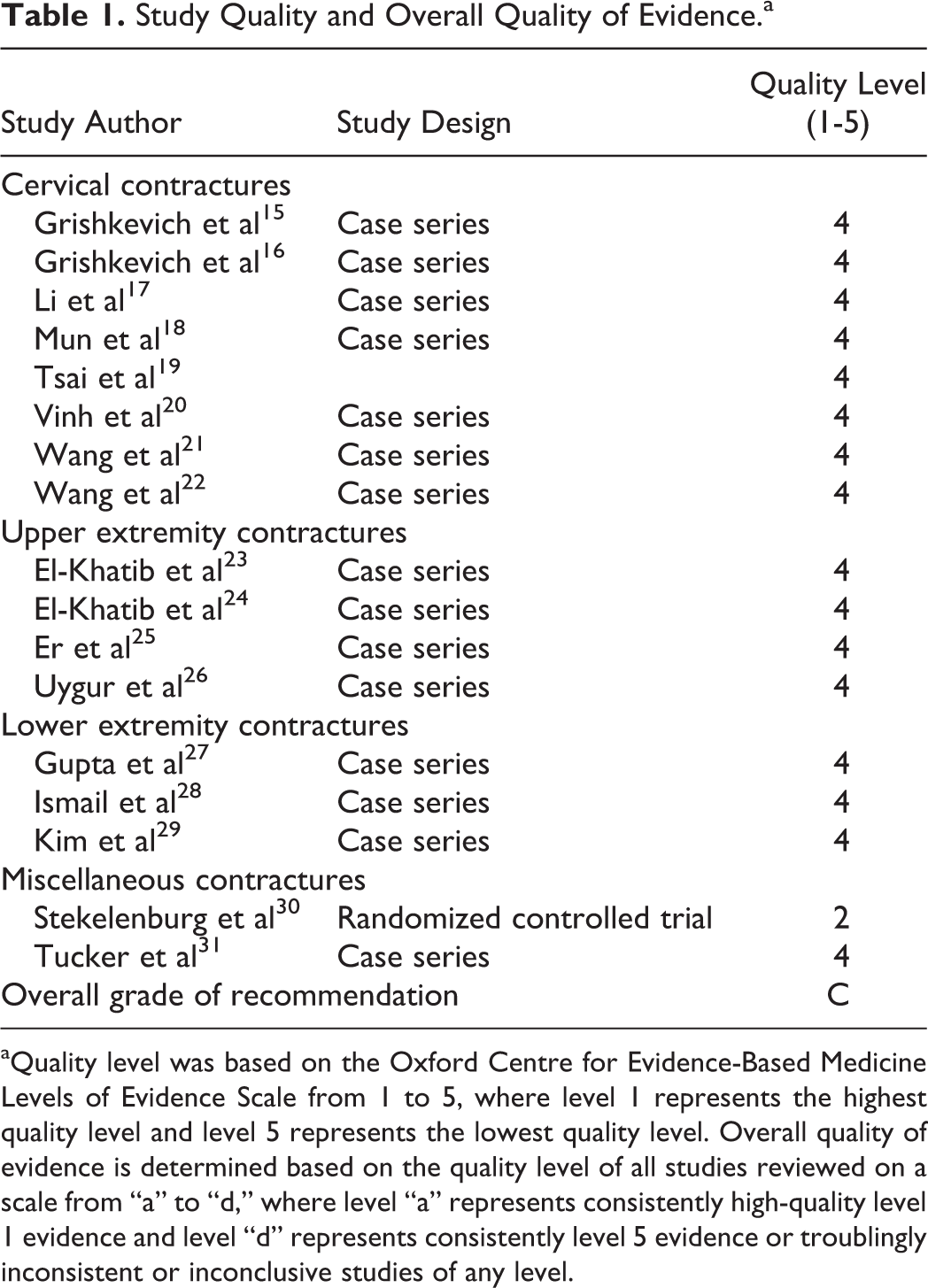
aQuality level was based on the Oxford Centre for Evidence-Based Medicine Levels of Evidence Scale from 1 to 5, where level 1 represents the highest quality level and level 5 represents the lowest quality level. Overall quality of evidence is determined based on the quality level of all studies reviewed on a scale from “a” to “d,” where level “a” represents consistently high-quality level 1 evidence and level “d” represents consistently level 5 evidence or troublingly inconsistent or inconclusive studies of any level.
Study, Patient, and Flap Characteristics.
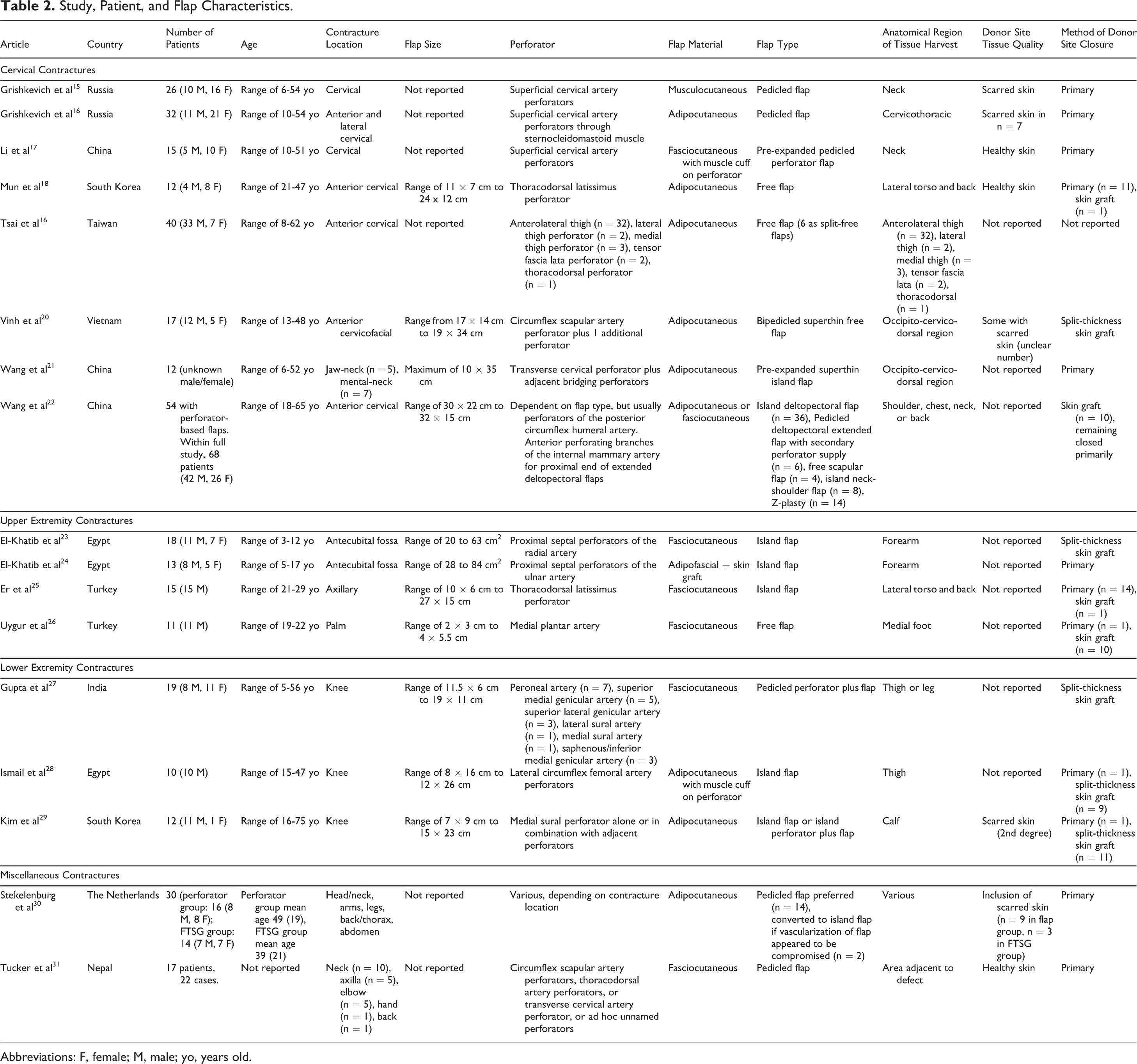
Abbreviations: F, female; M, male; yo, years old.
Study Outcomes.
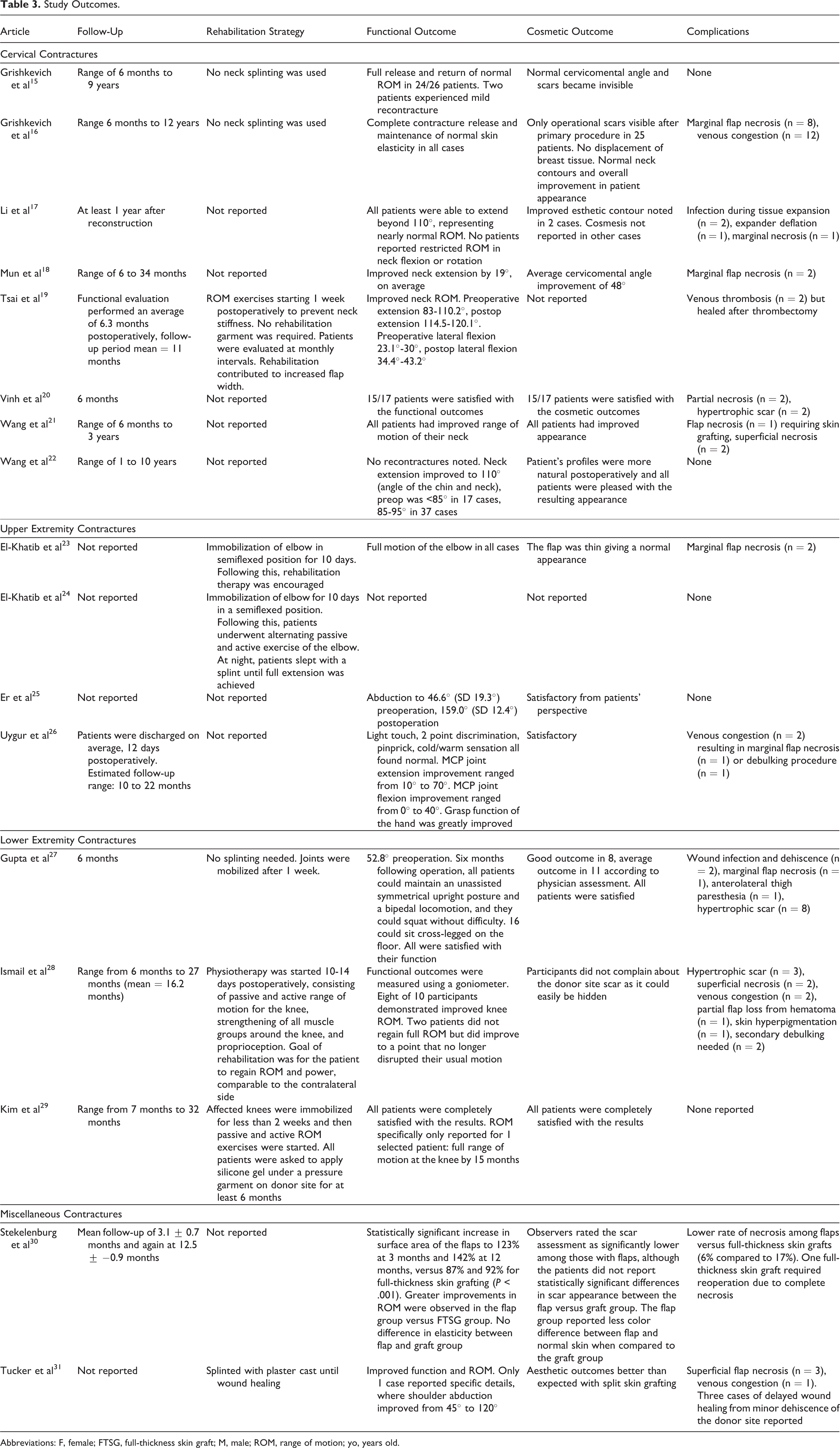
Abbreviations: F, female; FTSG, full-thickness skin graft; M, male; ROM, range of motion; yo, years old.
In total, this review summarizes the results of perforator flaps in 339 patients (age range: 3-75 years) with burn scar contractures across varying joints. There were 157 males, 99 females, and 83 in which sex was not reported or sex distribution could not be determined. The most common locations for contracture were cervical (n = 218), knee (n = 41), antecubital fossa (n = 36), axilla (n = 20), hand (n = 12), back (n = 1), and a mixture of head/neck, arm, leg, back/torso, abdomen (n = 16). Flap size ranged from 2 × 3 cm (6 cm2 area) up to 19 × 34 cm (646 cm2 area). Flap type was described primarily based on the vascular perforator and secondarily by the method of elevation (Figure 2). Among these flaps, 84 were performed as free flaps (most commonly for cervical contractures), 126 as island flaps, and 129 as pedicled flaps. The most common free flap used was the anterolateral thigh free flap. Flap composition was most commonly adipocutaneous, followed by fasciocutaneous and rarely musculocutaneous or adipofascial. Follow-up time ranged from 3 months to 12 years, although follow-up time was not reported in 4 studies. In the case of pedicled perforator flaps, donor sites were most often closed primarily. For island and free flaps, donor sites were generally closed primarily when the donor site was on the torso or back and generally closed with a skin graft when the donor site was on the extremities. At least 54 patients received a flap that contained scarred skin, usually as pedicled flaps. For repair of cervical contractures, superficial cervical artery pedicled flaps were most common (n = 73), as musculocutaneous, adipocutaneous, or fasciocutaneous. For knee contractures, the medial sural perforator adipocutaneous island flap was most common (n = 12). For antecubital fossa contractures, fasciocutaneous island flaps with proximal septal perforators of the radial artery were most common (n = 18). For axilla contractures, thoracodorsal latissimus perforator fasciocutaneous island flaps were the most common (n = 15). For hand contractures, medial plantar artery fasciocutaneous free flaps were most common (n = 11).
Nine of the 17 articles described a postoperative rehabilitation strategy. This generally involved some form of immobilization for 7 to 10 days after which mobilization (with or without formal physiotherapy) was encouraged. It is unclear how long physical rehabilitation was continued.
In general, functional outcomes were excellent, with most patients experiencing return of normal joint range of motion. Among the 17 articles, 8 gave objective data regarding range of motion of the contracted joint following surgery. The remaining articles simply reported functional outcomes in subjective terminology such as “excellent,” “all patients were satisfied,” or “improved range of motion.” Two articles provided information concerning performance of tasks in a functional capacity such as walking or sitting. Function was usually surgeon defined and not based on patient perception. Two articles commented on the neurologic or mechanical features of the flap such as sensation and elasticity.
Cosmetically, perforator flaps were believed by the authors to have good color match with surrounding tissue, good contour around anatomical landmarks, and improved overall appearance of the patient. There was no standardized approach for assessing cosmetic outcomes across studies, and most simply reported that patients were satisfied.
The most serious complication was flap necrosis (1 flap; pre-expanded transverse cervical perforator island flap) and partial flap loss (1 flap), but these were rare outcomes. The most common complications were venous congestion (17 flaps) and marginal/superficial flap necrosis (26 flaps). In total, 73 complications occurred at the recipient site, representing an overall complication rate of approximately 20%. Interestingly, 45 of 73 complications occurred with pedicled flaps, representing a complication rate of 35% with these flaps. Among island/free flaps, the complication rate was 13%.
Discussion
This review summarizes evidence on the use of perforator flaps for management of burn scar joint contracture. By providing levels of evidence for each study, it is hoped that the practicing physician may be able to utilize this review as a resource when considering applying a flap to their own patients with burn scar joint contractures. While overall quality of evidence identified in this review was low, with an overall OCEBM grade of recommendation of “C” based on most studies being case series in design, there was consensus in the findings across articles that perforator flaps led to favourable outcomes in terms of function, cosmesis, and low rates of severe adverse events. The evidence from these case series was further supported by a high-quality randomized controlled trial, where it was found that perforator flaps were superior to FTSG in terms of function, with fewer side effects, and perhaps superior in terms of cosmesis as well. Consequently, there is preliminary evidence from several case series and 1 high-quality randomized controlled trial to suggest that perforator flaps may be an effective option for management of burn scar contractures overlying joints. Importantly, this trial predominantly used pedicled perforator flaps, and no trial was identified assessing predominantly island or free flaps. A variety of different perforator flaps were successfully used across studies, suggesting that the specific flap used may depend on specific patient factors and surgeon preference, but it seems critical that further higher quality studies be undertaken to convincingly document the benefit of these procedures.
An important observation across studies was the significant degree of heterogeneity in outcomes reported. More objective reporting of outcomes is necessary to compare this surgical strategy to others. Specifically, many studies did not describe a rehabilitation plan or used vague terminology to describe functional and cosmetic results. Rehabilitation strategies may be important in ensuring optimal outcomes, and thus, future studies on this topic should provide detailed rehabilitation plans. For functional outcomes, we recommend detailed joint range of motion recording with a goniometer in the preoperative and postoperative state to quantify the benefit achieved from surgery. For cosmetic outcomes, we propose that a standardized scale be utilized that captures information such as normal contour/bulk, normal color, scarring, and patient satisfaction. Together, a more detailed approach to documenting rehabilitation, functional, and cosmetic outcomes will allow for improved knowledge translation regarding the benefits, risks, and indications for perforator flap surgery in patients with burn scar contractures.
Perforator flaps have been performed using a variety of modes of elevation, each with general success. However, complication rates appeared to be somewhat higher for pedicled flaps despite a seemingly more simple procedure. Since pedicled flaps were more likely to contain scarred tissue in flaps in this review, it is possible this damaged tissue may affect flap success. Nonetheless, it must be emphasized that these additional complications were generally minor, such as tip necrosis or transient venous congestion. Additionally, since the flaps contained scarred skin, it is possible these patients were more challenging cases, and thus, it remains unknown whether perhaps there would have been more severe complications for these patients if an island or free flap were to have been used.
This review is limited by substantial heterogeneity across studies, making any form of meta-analysis unfeasible. We attempted to reduce bias that could be introduced from low person-years follow-up (and therefore less time exposed to show benefits and adverse events) by selecting reports with a minimum sample size of 10 patients. However, in so doing, bias could also be introduced by failure to capture all existing data on the topic, and so other potential benefits and risks of perforator flap surgery for burn scar contracture may not be documented in this review. Importantly, we considered a broad definition for perforator flaps in this review, which included pedicled flaps with active attempt to preserve a known perforator. This broad definition did not likely affect our ability to identify true perforator flaps (ie, island and free flaps) in this review due to the use of recognized and broad terminology for perforator flaps in the original search strategy. However, it is possible we may have missed some studies that used pedicled flaps that did not use the terminology of “perforator” in their article since it is atypical to define these flaps as such. Thus, this review should be considered as a comprehensive review of the best quality evidence for island and free perforator flaps for burn scar contractures, with supplemental data from identified studies using pedicled flaps with a known perforator. Based on the overall low quality of evidence, as assessed by the OCEBM framework, and identification of just one high-quality trial, it is recommended that randomized controlled trials be undertaken to better establish the benefits of perforator flap surgery for burn scar contracture compared to other treatment modalities, especially since the only trial we identified predominantly considered pedicled flaps. Additionally, more detailed surgical procedure reporting would allow for improved clinical translation. Future investigations should explore the preferred type of perforator flap given the contracture location, whether it is preferable to use local tissue or a free flap, whether it is necessary to use skin grafting to close the donor site, what factors predict improved success with a perforator flap versus FTSG, and the recontracture rate between the 2 procedures.
In conclusion, this review has provided a summary of evidence available on the topic of perforator flap surgery for management of burn scar contractures overlying joints. Studies generally suggested favourable functional and cosmetic outcomes of perforator flaps with low complication rates; however, since overall study quality was low, with just one high-quality trial, more research is required to substantiate these findings and identify which patients and clinical situations are most likely to benefit from this surgical approach compared to more conventional approaches such as FTSG.
Footnotes
Level of Evidence
Level 3, Therapeutic
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Ryan T. Lewinson and Lauren C. Capozzi are funded by Alberta Innovates MD/PhD Studentships.