
Abstract
Background:
Little is known with regard to patient-reported outcomes (PROs) in the setting of implant-based reconstruction (IBR) with post-mastectomy radiation therapy (PMRT).
Methods:
We identified patients who underwent immediate IBR from a prospectively compiled database. The Breast Reconstruction Satisfaction Questionnaire (BRECON-31) was scored and compared between patients with and without PMRT.
Results:
Sixty-four women met the study criteria. Forty-eight did not receive PMRT and 16 did. Nine women had an unanticipated indication for PMRT. The PMRT group was similar to the control group with regard to baseline characteristics (ie, age, marital status, body mass index, tobacco use, and comorbidities). However, treatment and oncologic characteristics (eg, diagnosis, tumour characteristics, systemic therapy use) differed. Of all complications, only capsular contracture rates differed (1.2% vs 13%; P = .01). Of the 9 subscales, 7 showed no difference in satisfaction between the groups. Radiated women scored lower in the arm concerns and breast appearance subscales. Scores were similar whether the indication for PMRT had been anticipated or not.
Discussion:
Women with immediate IBR scored similarly to their nonradiated counterparts across 7 of 9 domains of satisfaction. Arm concerns and breast appearance scores are lower with PMRT, likely secondarily to more extensive nodal procedures in higher stage patients and to the side effect profile of radiotherapy. Our findings are in line with the few available studies using other PRO tools to evaluate the impact of PMRT on patient satisfaction and studies objectively measuring the effect of PMRT on arm morbidity and cosmetic outcomes.
Introduction
Immediate breast reconstruction after mastectomy for cancer is on the rise. 1 –3 Among available options, implant-based techniques remain widely used in the immediate reconstructive setting. 4 –6 Post-mastectomy radiation therapy (PMRT) is also on the rise leading to a reduced risk of loco-regional recurrence and reduction in breast cancer mortality in some patient subsets. 7,8
The side effect and complication profile of PMRT after implant-based reconstructive surgery has been explored in nonrandomized studies, with evidence pointing toward increased complications, 9,10 including an increased rate of capsular contracture 11 and corrective surgery. 12,13 Furthermore, radiation planning concerns include challenges in achieving a uniform dose with expanders in place, avoiding the contralateral breast, and minimizing lung dose, while achieving appropriate coverage of internal mammary nodes. 14 Unfortunately, many of the indications for adjuvant radiation therapy use in early breast cancer are based on definitive histologic tumour characteristics that are often not identifiable preoperatively, such as final tumour size and lymph node positivity. Thus, clinicians and patients may be faced with an unexpected recommendation for PMRT after immediate breast reconstruction. Alternatively, a patient may voice strong preference for an implant-based reconstruction (IBR), even though they know of a possible indication for PMRT.
One strategy to avoid capsular contracture and radiation planning challenges is the avoidance of immediate reconstruction altogether, if histologic characteristics in the final mastectomy might warrant radiotherapy and delaying tissue-based reconstruction. Unfortunately, in the Canadian system, wait times for delayed breast reconstruction are prohibitive. 15 After post-mastectomy radiotherapy, women generally need a flap reconstruction such as a deep inferior epigastric perforator flap (DIEP) for which not all women are candidates. Furthermore, delaying reconstruction is known to depress BREAST-Q scores 16 and that radiated women later having delayed DIEP flap breast reconstruction report lower satisfaction than those with immediate reconstruction. 17 It is therefore important to know whether women who have radiotherapy after immediate implant reconstruction regret their decision.
A study to evaluate patient satisfaction after reconstructive surgery and PMRT would help surgeons and oncologists in counselling future women facing a similar decision tree. In this study, we sought to compare the patient-reported outcomes (PROs) of women who received PMRT after implant reconstruction with women who had reconstructive surgery without radiotherapy.
Methods
Ethics approval was gained through the University of Calgary Research Ethics Board (REB15-2275). Consecutive patients who underwent immediate, implant-based reconstructive surgery by a single plastic surgeon at the Foothills Medical Centre from February 2012 to June 2015 were identified using a prospectively compiled database. Patients who had had radiation therapy to the chest pre-reconstructive surgery were excluded.
As standard of care, patients complete the Breast Reconstruction Satisfaction Questionnaire (BRECON-31) questionnaire once reconstruction is complete at their final follow-up appointment. The BRECON-31 is a validated self-administered questionnaire on patient satisfaction after breast reconstructive surgery. This questionnaire includes 31 questions appropriate for all women having reconstruction and is scaled on a 4-point Likert format. Eight subscales are related to the patient experience of breast reconstruction surgery, including self-image, arm concerns, intimacy, satisfaction, recovery, self-consciousness, expectations, and breast appearance. An additional 4 questions examine nipple concerns for women having nipple-sparing mastectomies or nipple reconstruction, and another 10 items inquire the after-effects of the abdominal donor site for women having DIEP flap reconstruction. 18 –20 We extracted from the database all patients who had completed reconstruction and a BRECON-31 questionnaire and divided them into 2 groups: patients who received PMRT (PMRT group) and patients did not require radiotherapy (control group). These patients constitute the study population. A subgroup analysis was also conducted comparing the scores of irradiated women splitting them into 2 groups based on whether radiation had been expected or not.
It was hypothesized that there would be a difference in expectations and satisfaction between these patients, because those with known indications for radiotherapy would have been counselled thoroughly on expectations of the surgery plus radiation. This would have included discussion about a reduced aesthetic outcome, capsular contracture, symmetry issues, and the higher likelihood of revision surgery. It is conceivable that women not expecting radiotherapy may not have had their expectations calibrated to the same degree, resulting in satisfaction surveys showing inferior results.
Retrospective chart review allowed determination of individual patient characteristics; date and type of surgery; indication for mastectomy (prophylactic, ductal carcinoma in situ, or invasive breast cancer); adjuvant treatment modalities, if applicable; post treatment complications, divided into minor complications (managed expectantly or with a procedure requiring local anesthetic) or major complications (such as capsular contracture managed by procedures requiring general anesthetic); and need for corrective surgery.
Patient characteristics at baseline as well as treatment factors were compared using χ2 and 2-tailed Student t test, using a threshold for significant difference of P < .05. The BRECON-31 total and subscales results between the 2 groups were compared using Student t test.
Results
Demographics
Review of the database identified 64 women who had undergone implant-based, immediate breast reconstruction and had completed the BRECON-31, with 48 women in the control group and 16 in the PMRT group. Table 1 illustrates the patient characteristics at baseline. The control group was similar to the PMRT group with regard to age (48 vs 43 years old; P = .07), marital status (52% vs 94% married; P = .13), body mass index (26 vs 28; P = .13), tobacco use (8% vs 0% smokers; P = .18), and Charlson comorbidity index (69% vs 88% score 0; P = .64).
Patient Characteristics.
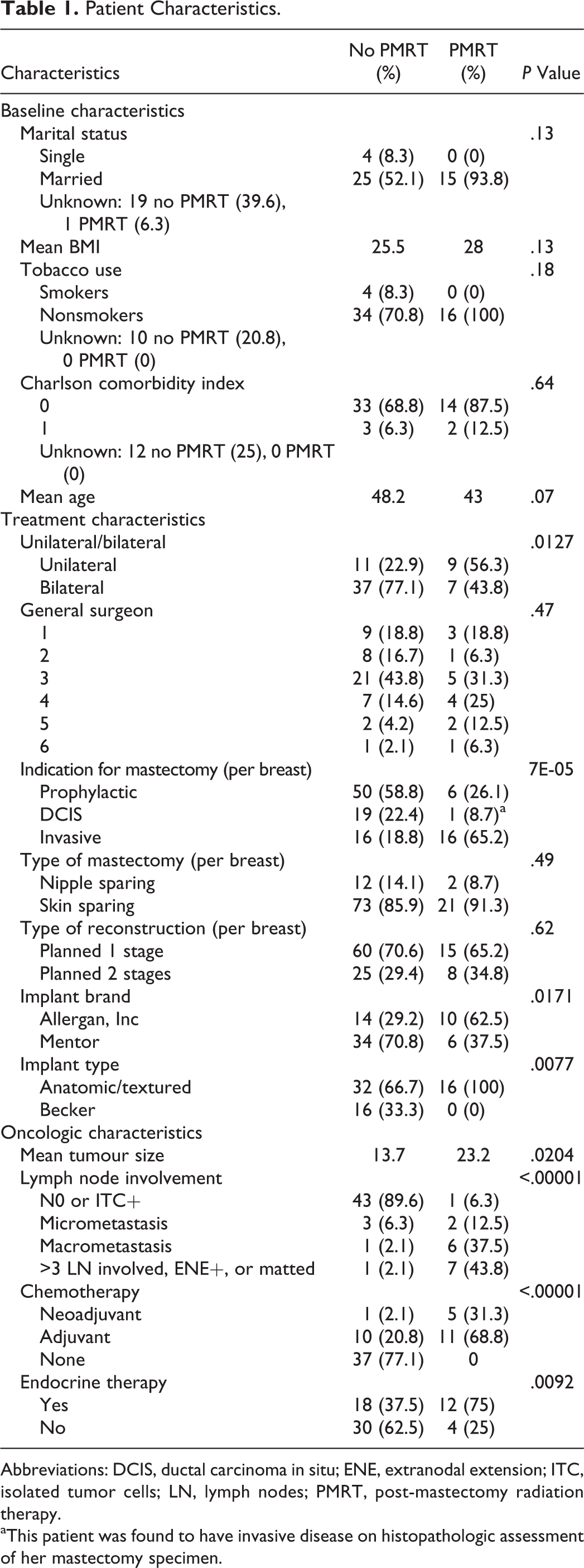
Abbreviations: DCIS, ductal carcinoma in situ; ENE, extranodal extension; ITC, isolated tumor cells; LN, lymph nodes; PMRT, post-mastectomy radiation therapy.
aThis patient was found to have invasive disease on histopathologic assessment of her mastectomy specimen.
Treatment Characteristics
More patients in the control group had bilateral mastectomies (77% vs 44%; P = .01), and the indications for surgery were less likely to be invasive disease in that group (19% vs 65%; P < .01). They were also more likely to have had a Mentor (70.8% vs 37.5%; P = .02) and Becker (33% vs 0%; P = .008) type of implant. The type of mastectomy (skin sparing vs nipple sparing), general surgeon proceeding with the mastectomy, and the type of planned reconstruction (planned 1 stage vs 2 stages) did not differ significantly between the 2 groups.
Oncologic Characteristics
The groups differed in tumour characteristics. The control patients had smaller tumours (14 vs 23 mm; P = .02), lower nodal burden (10% vs 94% N+; P < .001), and were less likely to have received chemotherapy (23% vs 100%; P < .001) and endocrine therapy (38% vs 75%; P = .009). Of note, all patients in the PMRT group received chemotherapy, whether it was in a neoadjuvant (5 patients, 31%) or adjuvant (11 patients, 69%) fashion.
Among the women who received adjuvant radiation therapy, 7 (44%) had a known indication for PMRT prior to breast reconstruction because of known lymph node involvement or tumour size greater than 5 cm, while 9 (56%) had an unexpected recommendation for PMRT, their indication having been determined by final histopathologic characteristics.
Complications
Post-treatment complications are detailed in Table 2. Of note, some patients experienced more than one complication, as enumerated in Table 2. Occurrences of minor complications, that is, those treated with expectant management, oral antibiotic treatment, or minor office procedure, did not differ significantly between the 2 treatment groups. Among major complications, capsular contracture rates were higher in women receiving PMRT (13.0% vs 1.2%; P = .008). There were 2 reconstruction losses in each treatment group (8.7% vs 2.4%; P = .15).
Complications by Treatment Group.
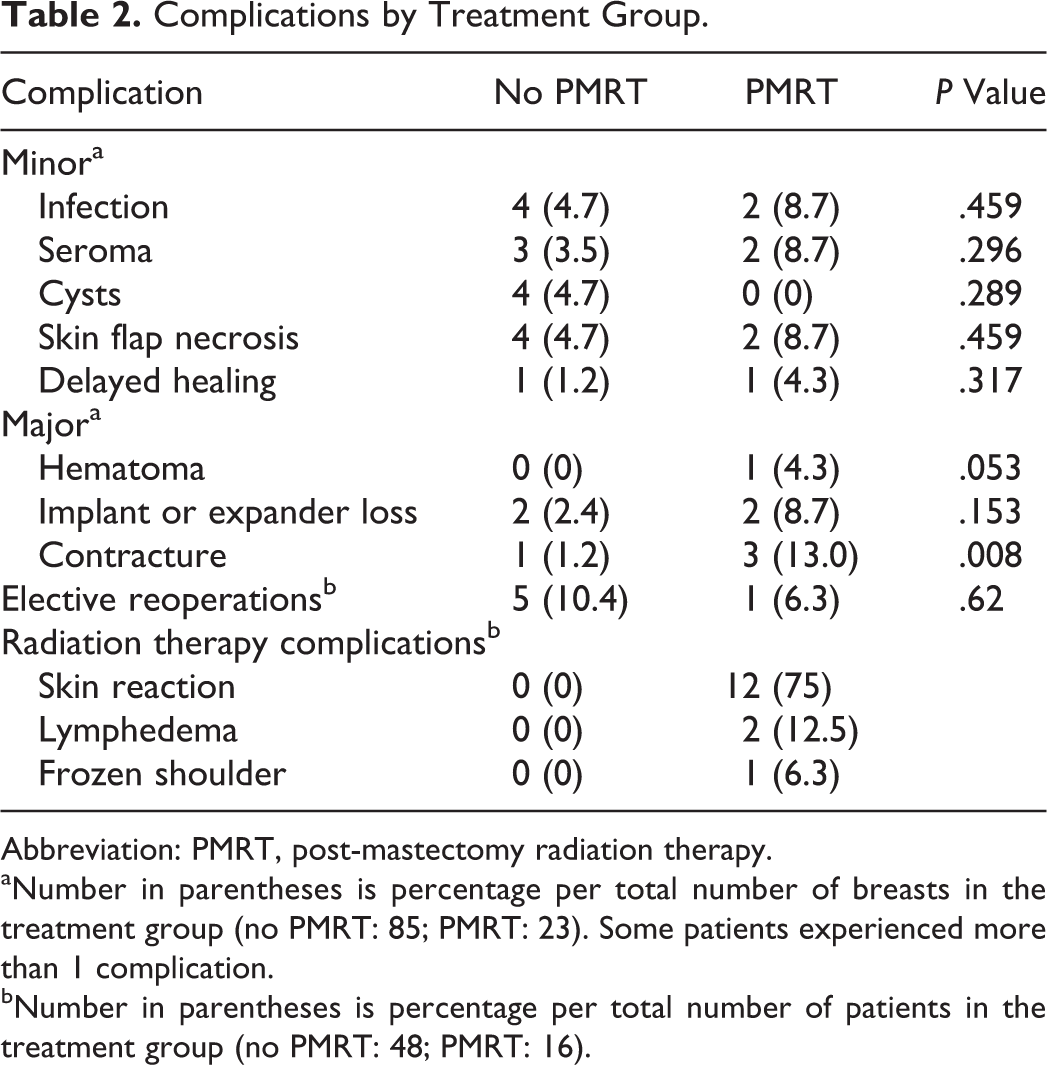
Abbreviation: PMRT, post-mastectomy radiation therapy.
aNumber in parentheses is percentage per total number of breasts in the treatment group (no PMRT: 85; PMRT: 23). Some patients experienced more than 1 complication.
bNumber in parentheses is percentage per total number of patients in the treatment group (no PMRT: 48; PMRT: 16).
Fewer elective corrective procedures were performed in the PMRT group (6.3% vs 10.4%; P = .62). This may reflect reluctance to reintervene on radiated tissues. Post-PMRT complications are also noted in Table 2. Of note, 2 patients developed lymphedema after PMRT: one had had a sentinel lymph node biopsy at the time of the index procedure and the second patient an axillary lymph node dissection.
Patient-Reported Outcomes Data
The BRECON-31 questionnaire was completed at a mean of 506 days (range: 56-1284 days) following initial surgery by the control group and 499 days (range: 230-993 days) following surgery and 315 days (76-881 days) following last radiation therapy session for the PMRT group. Overall, a third of the patients of the control group completed the BRECON-31 within a year of initial surgery, and more than half had done so within 2 years. These figures were lower for the PMRT group (12.5% at 1 year and 37.5% at 2 years), reflecting the lengthier interval between initial surgery and last clinic follow-up induced by the PMRT treatment itself.
Table 3 shows the comparison in BRECON-31 total and subscale scores between the control and PMRT groups. Of note, 1 patient in the control group lost her implant after having completed the BRECON-31 questionnaire, and 1 patient in the same group lost her tissue expander (due to a mycobacterial infection) but went on to complete her reconstructive process and the BRECON-31 questionnaire; their answers were included in the analysis. Two patients in the radiated group lost their reconstructions (due to infections and subsequent exposure in one and exposure in another) and, at the time of BRECON-31 completion and analysis of this study, had not yet finished their reconstructive process; their questionnaire responses were thus not available to include in the analysis.
BRECON-31 Scores Analysis by Treatment Group.a
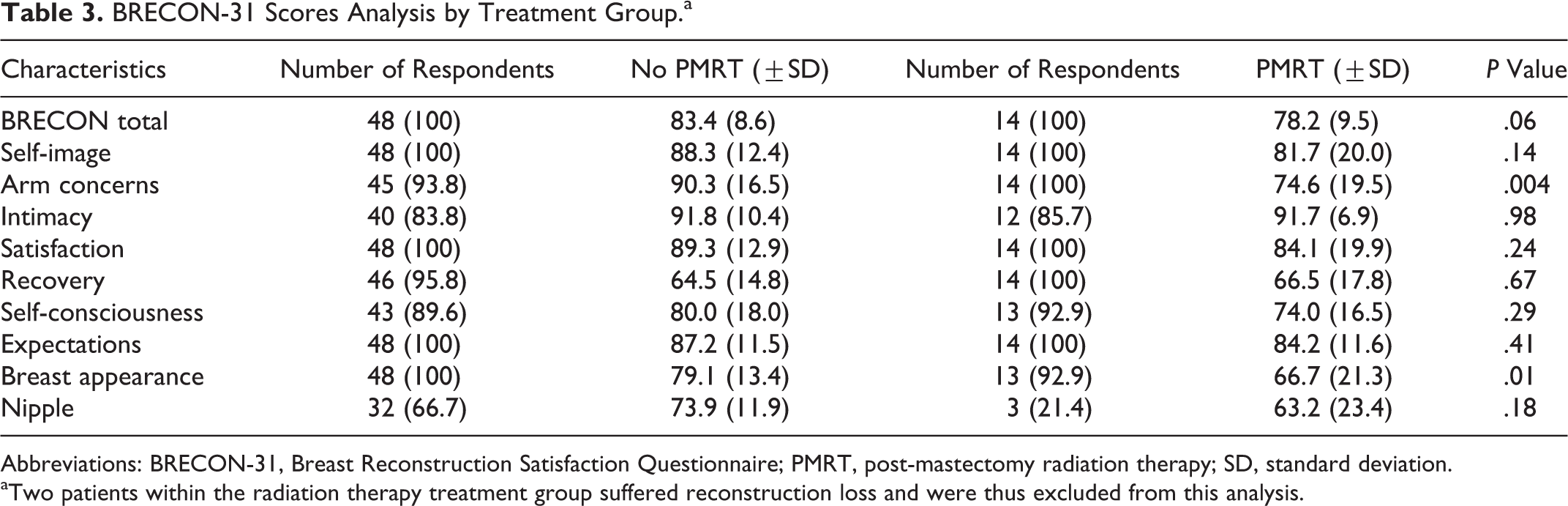
Abbreviations: BRECON-31, Breast Reconstruction Satisfaction Questionnaire; PMRT, post-mastectomy radiation therapy; SD, standard deviation.
aTwo patients within the radiation therapy treatment group suffered reconstruction loss and were thus excluded from this analysis.
The total BRECON-31 score was 5 points higher out of a total of 100 in the control group, although not significantly different (78.2 vs 83.4; P = .06). Using the “half standard deviation” 21 approach to determining a clinical significance, the difference was not clinically important.
Seven of 9 subscales within the BRECON-31, including self-image, intimacy, satisfaction, recovery, self-consciousness, expectations, and nipple concerns subscales, showed no statistical or clinically important differences in scores for control and PMRT patients. Most notably was the similarity within the satisfaction subscale, which poses the statements “I am satisfied with my breast reconstruction,” “If I had to do it all over again, I would choose this type of reconstruction,” “I would recommend my type of breast reconstruction to a friend,” and “the breast reconstruction turned out the way I thought it would.” These items drill down on satisfaction with the reconstruction and the experience and reflect decision regret. Both the control and PMRT groups scored high (89.3 and 84.1; P = .24).
Figure 1 graphs the scores across the different domains of satisfaction. Statistically and clinically poorer scores were seen in radiated women in the “arm concerns” subscale (74.6 vs 90.3; P < .01), which explores lymphedema, shoulder and arm pain, and range of motion.
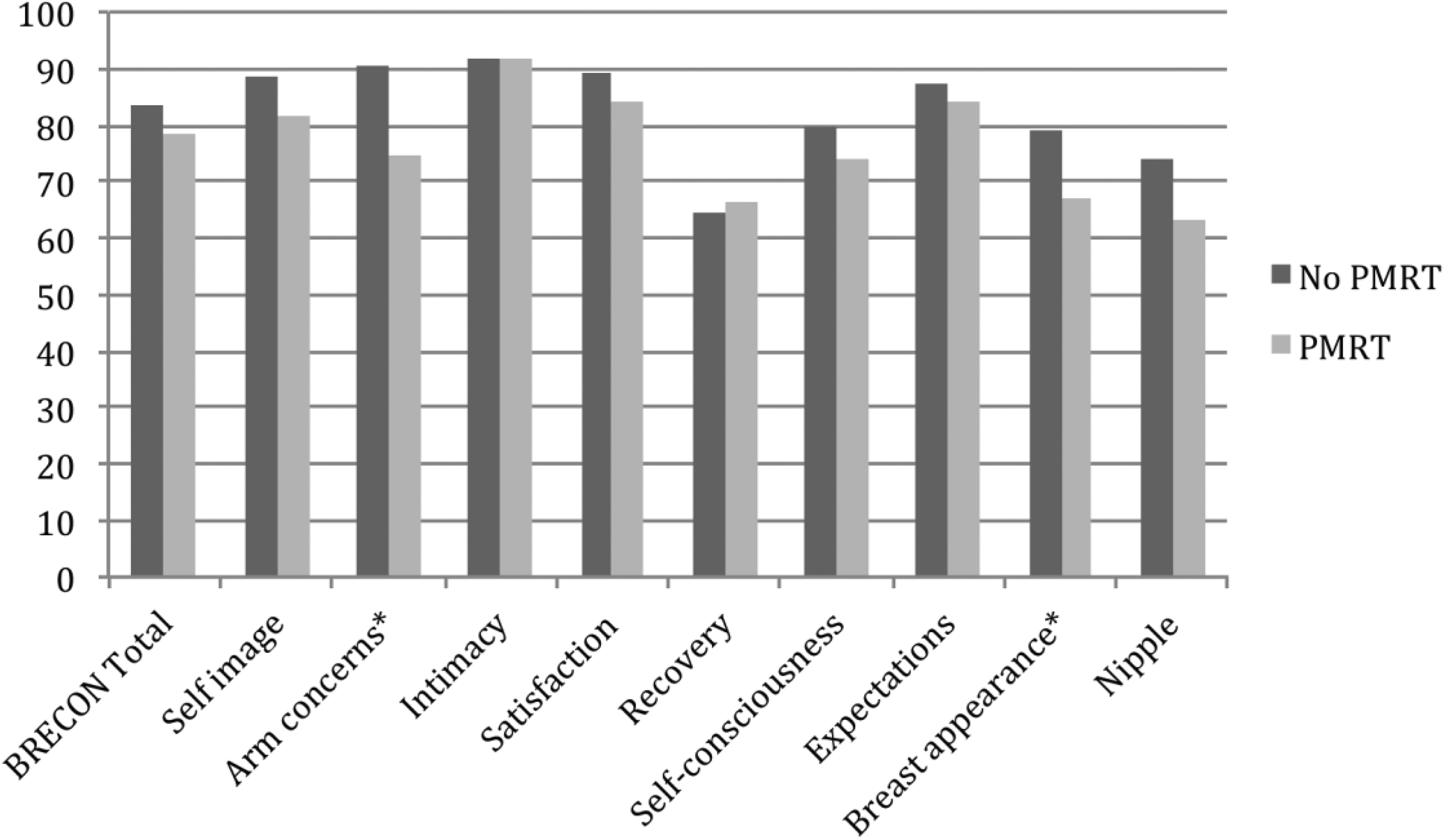
Breast Reconstruction Satisfaction Questionnaire (BRECON-31) score analysis by treatment group. *Statistically significant difference.
The PMRT group also scored lower in the “breast appearance” subscale (66.7 vs 79.1; P = .01, respectively). Breast appearance items include difficulty fitting a bra, feeling that the reconstruction is the right size, and the appearance in comparison to original breast.
To better explore the impact of pre-surgical discussions of expectations following radiotherapy on overall satisfaction, we performed a sub-analysis of the BRECON-31 total and subcategory scores, separating the patients who had a definite expectation of PMRT prior to their surgery and those who did not. We excluded from this analysis the 2 patients who experienced implant loss and who both had their indication for PMRT determined by final staging after mastectomy. The BRECON-31 total and subscores were similar between the 2 groups, as shown in Table 4 (mean total score 77 for known indication vs 79 for unanticipated indication; P = .66).
BRECON-31 Score Analysis by Expectation of PMRT.
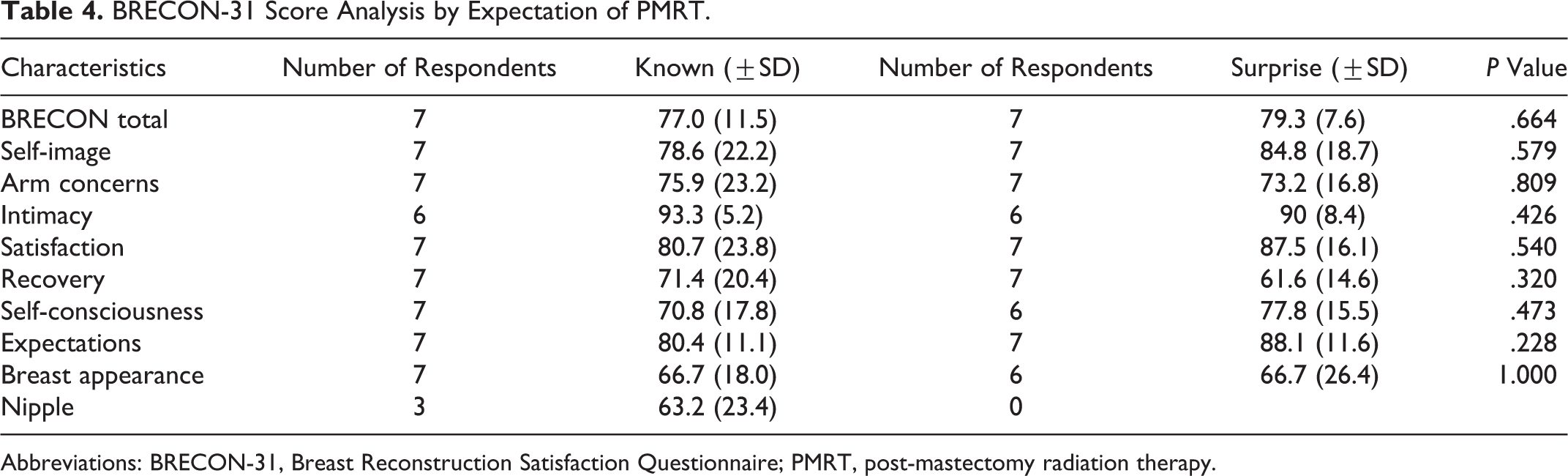
Abbreviations: BRECON-31, Breast Reconstruction Satisfaction Questionnaire; PMRT, post-mastectomy radiation therapy.
Discussion
This is the first study using the BRECON-31, a validated tool for evaluation of PRO measure in breast reconstructive surgery, to look at satisfaction related to receipt of PMRT after immediate, implant-based breast reconstruction. Women with immediate IBR and PMRT scored similarly to their nonradiated counterparts across 7 of 9 domains of satisfaction and quality of life. Furthermore, these scores were quite high, ranging from the mid 70s to the low 90s, with the exception of the “recovery” subscale which scored in the 60s for both radiated and not radiated women. Poor recovery scores is a consistent, concerning finding across flap and implant patients, radiated or not. 22 It indicates the need to apply enhanced recovery after surgery principles to breast reconstruction patients to ameliorate this (Figure 2). 23 –25

Patient cosmetic results after implant-based reconstruction (IBR) and post-mastectomy radiation therapy (PMRT) with Breast Reconstruction Satisfaction Questionnaire (BRECON-31) total scores.
The PMRT group struggled in the “arm concerns” domain. The use of adjuvant radiation therapy is known to lead to local morbidity, namely acute radiation dermatitis, higher rates of lymphedema, and shoulder mobility restrictions. 26,27 Furthermore, more women in the PMRT group had complete axillary node dissections (50% vs 8.3%), which is also associated with increased lymphedema rates and sensory deficits. 28 The higher rate of arm concerns in the PMRT group could be interpreted as the consequence of having higher stage disease requiring more axillary therapy, rather than a consequence of a radiated breast reconstruction.
The PMRT group also scored lower on the “breast appearance” subscale. This correlates with literature presenting expert opinion on the aesthetic results of IBR in the setting of adjuvant radiation therapy. 29 Our findings are consistent with that of 100 women who received PMRT in the setting of an implant reconstruction and scored lower on “satisfaction with breasts” on the BREAST-Q lower than nonradiated peers. 30 Our PMRT cohort also had more unilateral reconstructions (44% vs 77%) than the control group making symmetry and bra fitting challenging irrespective of receipt of PMRT, which could bias the results in favour of better breast appearance scores in the control group.
Patient perception of outcomes is linked to reasonable expectation setting. 31 Managing expectations with regard to outcomes is an important component of the preoperative consultation. In women with a known plan for PMRT, extensive discussion about increased complications, capsular contracture, and other adverse outcomes is important to increase satisfaction with reconstruction. However, we did not find differences among subscale scores in women who required unanticipated radiotherapy who might not have been educated preoperatively about the potential for a poor outcome, although the sample size of the subgroup analysis is small.
Delayed, autologous tissue breast reconstruction is currently recommended in the setting of possible or definite indication for PMRT. 32,33 However, immediate implant reconstructive options remain popular among patients and physicians for multiple reasons including improved appearance due to the ability to preserve the skin in skin- and nipple-sparing mastectomies. In addition, avoidance of a large, visible lighter colored abdominal skin paddle, 34 reduced adverse impact of mastectomy in psychosocial well-being, waiting for delayed reconstruction, and potential reduction in the total number of necessary surgeries are motivating factors. 35
Our results contrast with a large, multicenter study comparing PMRT and nonradiated implant patients, where the PMRT group scored statistically lower in 5 reported subscales (satisfaction with breasts, satisfaction with outcome, psychosocial well-being, sexual well-being, and physical well-being: chest and upper body). 6 The survey did not report on other components of the BREAST-Q, such as expectations and satisfaction with care, questioning whether those subscales did not differ or possibly those scales were not tested. The difference scores were small however, and although statistical significance was reached, the minimal clinically important difference (MCID) was below half of a standard deviation, questioning whether these scores reflect a clinically relevant lower score to support abandoning IBR in this subset.
Consistent with our findings are results from a 10-year review of 313 patients having reconstruction with LD flaps and expanders. 36 Higher complications and unplanned interventions were seen in radiated patients, but no worsening of long-term satisfaction. Our single-surgeon approach could be a factor in driving higher scores in the radiated patients based on intensive patient education and expectations management, and a shared decision-making approach, 22 which may not be generalizable.
Thus, our study supports the body of literature that while immediate implant breast reconstruction in the setting of PMRT is associated with less optimal patient-rated appearance, a claim with which few clinicians would argue, the majority of subscales of satisfaction that are of importance to patients such as self-image, self-consciousness, intimacy, and expectations are similar in radiated and nonradiated women. As such it seems that a blanket approach of imposing a delayed autologous reconstruction on women expecting PMRT, which can take over 2 years in the Canadian context, 15 may not be the ideal approach for maximizing a woman’s health-related quality of life. In addition, some women aren’t autologous candidates such as those with multiple abdominal scars, thin body habitus, coagulopathy, or multiple comorbidities; thus, immediate implant reconstruction may present their only opportunity shy of accepting a radiated mastectomy chest wall deformity.
A hybrid approach used by Hirsch et al 37 may be something to consider. He inserts a tissue expander at the time of mastectomy to preserve the skin-spared skin, proceeds with tissue expansion and PMRT, and delays the choice of permanent method of reconstruction (implant or autologous) until several months after completion of radiation therapy. Even this conservative approach must respect radiation planning concerns vis-à-vis challenges in applying a uniform dose and adequately covering internal mammary nodes, making multidisciplinary consultation and excellent communication a must in the management of this subset of patients.
Our study is limited by its nonrandomized convenience sample, retrospective design, and a small number of radiated patients. However, examining the impact of PMRT on breast reconstructive surgery via a randomized model may be unachievable. The external validity of our results is limited by the sample groups all having had their reconstruction by a single plastic surgeon, introducing an element of homogeneity that may not be representative of the diverse specialists involved in the care of patients with breast cancer. Finally, although the mean time to completion of the BRECON-31 questionnaire exceeded 1 year, this may not adequately reflect the long-term consequences of PMRT.
Footnotes
Level of Evidence
Level 3, Therapeutic
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Claire Temple-Oberle has unrestricted education grants from Acelity, Allergen, Mentor, Merck. The funding disclosed is not related to the research, authorship and/or publication of this specific article.