
Abstract
Purpose:
In syndromic craniosynostosis, the Le Fort III osteotomy is used to correct dental/skeletal imbalance, improve exorbitism, and increase the airway. The purpose of this study is to perform a cost comparison between the standard technique of single-stage rigid internal fixation and distraction osteogenesis (DO) in the Le Fort III osteotomy in this patient population.
Method:
Hospital cost accounting databases were queried for patients undergoing single-stage advancement (SS) or DO from 2007 to 2016. Nominal cost data were adjusted using the Bank of Canada Consumer Price Index. Reported costs represented the full length of stay for all utilization per patient. Demographic information and cost data for single-stage osteotomy and DO were compared.
Results:
Total costs for single-stage (n = 8) were higher than distraction (n = 6; mean $CAD57 825 vs $38 268, P < .05). Intensive care unit (ICU) costs for single-stage were significantly higher than distraction (mean, $17 746 vs $5585, P < .005). Distraction cases had higher operating room (OR) costs than single stage, but the difference was not significant (mean, $12 540 vs $9696). Length of stay was significantly longer for SS patients (mean, 11 days vs 7 days, P < .05).
Conclusions:
This single-institution retrospective cost analysis indicates standard SS rigid internal fixation Le Fort III is more costly than DO. Despite higher OR costs, prolonged ICU and hospital stay was the primary reason behind this difference. This information may be of benefit when advocating for new technology perceived as high cost.
Introduction
The Le Fort III osteotomy is an integral component of the reconstructive approach for patients with syndromic craniosynostosis and is designed to address dental/skeletal imbalance, improve exorbitism, and correct airway obstruction. 1 –3 Two general algorithms for performing the Le Fort III advancement include immediate advancement in a single-stage procedure using rigid internal fixation with intermaxillary fixation (IMF) or gradual movement of the midface using distraction osteogenesis (DO). Both techniques are safe and presently used with good outcomes. 4,5 It has not been established if one technique is superior to the other and this topic continues to be debated.
Specific advantages reported for DO include greater achievable advancement distance, better bone formation, and decreased relapse rates. 4 –6 Disadvantages include prolonged treatment times, need for additional procedure, and equipment cost. 7,8 Proponents of a single-stage Le Fort III advancement cite the challenges wearing an external head frame with attendant risks and morbidity. Choice of technique often relates to surgeon preference. At the Hospital for Sick Children, Toronto, there is a unique opportunity where the 2 senior authors differ in philosophy in how best to perform the Le Fort III osteotomy for patients with syndromic craniosynostosis, with one routinely using internal rigid fixation and IMF (J.H.P.) and the other being an advocate for DO using the external head frame (C.R.F.).
The aim of this retrospective analysis was to compare the relative incurred costs when performing single-stage advancement versus DO for Le Fort III osteotomies in syndromic craniosynostosis patients at the Hospital for Sick Children, Toronto. Identifying cost differences and the driving factors responsible for disparities may ultimately promote cost-efficient delivery of services in pediatric craniofacial surgery.
Methods
Patient Selection
Following study approval from the Research Ethics Board at The Hospital for Sick Children (#1000043524), the patient database for the Centre for Craniofacial Care and Research was retrospectively searched for patients who underwent Le Fort III between April 1, 2007, and March 31, 2016. This time period coincided with the initiation of cost data collection by the Decision Support unit in fiscal year 2007. Data sources included the Discharge Abstract Database and National Ambulatory Care Reporting System.
Recorded data were sorted as either demographic or cost associated. The former included diagnosis, date of birth, age at surgery, gender, date of Le Fort III operation, surgical history prior to Le Fort III operation, and indications for surgery. Queried cost data included length of surgery, intensive care unit (ICU) and non-ICU costs, operating room (OR) costs, and hardware used. Cost data could be further stratified as direct and indirect costs as recommended by the Panel on Cost-Effectiveness in Health and Medicine.16 Direct costs associated with a patient’s care included nursing, allied health, imaging, laboratory, therapeutic, food services, pharmacy, ambulatory care, and medical/surgical supplies. Indirect “overhead” costs related to administrative and support services performed on behalf of all patients (ie, information systems and housekeeping).
Associated physician costs were compared using the Ontario Ministry of Health and Long-Term Care Physician Fee Schedule. Due to the lack of separate fee codes for the single-stage and distraction procedures, we did not conduct further analysis of physician payment because there were no differences in fee disbursement between the 2 groups.
The retrieved cost data were initially provided with a uniform 3% annual inflation rate applied to adjust to the latest 2015/2016 fiscal year. However, after reviewing the Bank of Canada Consumer Price Index, it was clear that average inflation ranged between 1.16% and 1.59% during the study period. In other words, the 3% uniform adjustment was overcompensating actual inflation rates. Results are reported in Canadian dollars (CAD). We adjusted nominal cost data (CAD) to 2016 dollars using respective annual inflation rates for each given fiscal year according to the Bank of Canada Inflation Calculator.
Data Analysis
All data were analyzed using descriptive statistics. Student t test was used for the majority of analyses and Wilcoxon rank tests were used for data that were not normally distributed. The 6 hypotheses tested were differences in total, direct, indirect, ICU, non-ICU, and OR costs. Therefore, Bonferroni correction was applied to the threshold for statistical significance of α = .05. Analyses were performed using SPSS, version 24 (SPSS, Chicago, Illinois).
Results
Of the records reviewed, 14 patients (4 years to 13 years old) with syndromic craniosynostosis met the criteria for inclusion in this study, 7 underwent DO and 7 had single-stage advancement with rigid internal fixation and IMF (SS). Sex distribution, diagnosis, and ages were similar between the 2 groups (Table 1). Indications for surgery included airway compromise (8 patients), skeletal/dental imbalance (14 patients), and exorbitism (14 patients).
Patient Demographics.
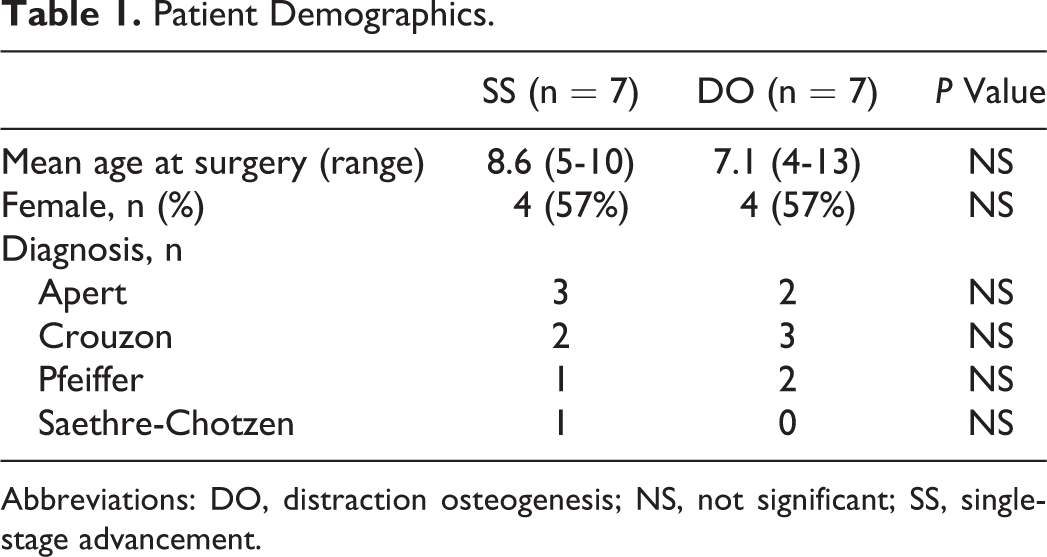
Abbreviations: DO, distraction osteogenesis; NS, not significant; SS, single-stage advancement.
Total treatment costs for performing a Le Fort III osteotomy were significantly greater in the SS group ($57 825 CAD; range: $36 900-$82 695) compared with the DO group ($38 268 CAD; range: $20 736-$64 033; Table 2).
Average Treatment Costs (CAD $) and Length of Stay.
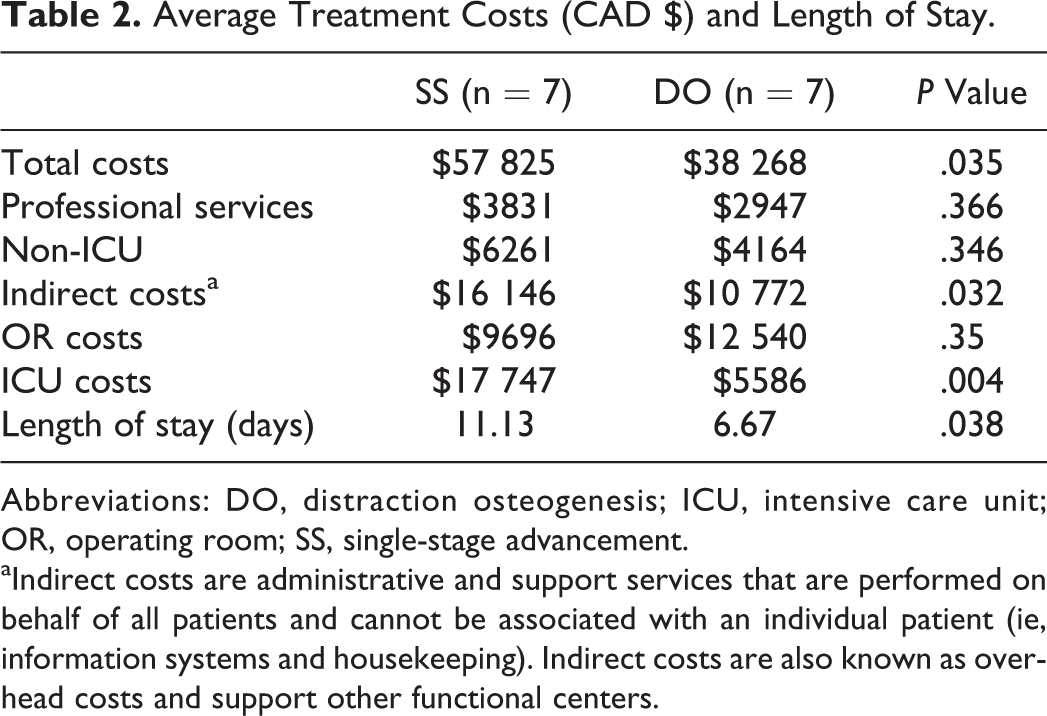
Abbreviations: DO, distraction osteogenesis; ICU, intensive care unit; OR, operating room; SS, single-stage advancement.
aIndirect costs are administrative and support services that are performed on behalf of all patients and cannot be associated with an individual patient (ie, information systems and housekeeping). Indirect costs are also known as overhead costs and support other functional centers.
While the actual duration of treatment for patients undergoing DO (time from surgery to removal of the head frame or arch bars) was longer compared to the SS group (87 days; range: 56 to 106 vs 35.5 days; range: 25-44, P < .05), time in the length of hospitalization were all significantly shorter in the DO group (Table 2)
Total treatment costs were not significantly different between differing diagnoses (Figure 1). Cost categories of professional services, non-ICU, and indirect costs did not differ between the SS and DO groups of patients (Table 2).
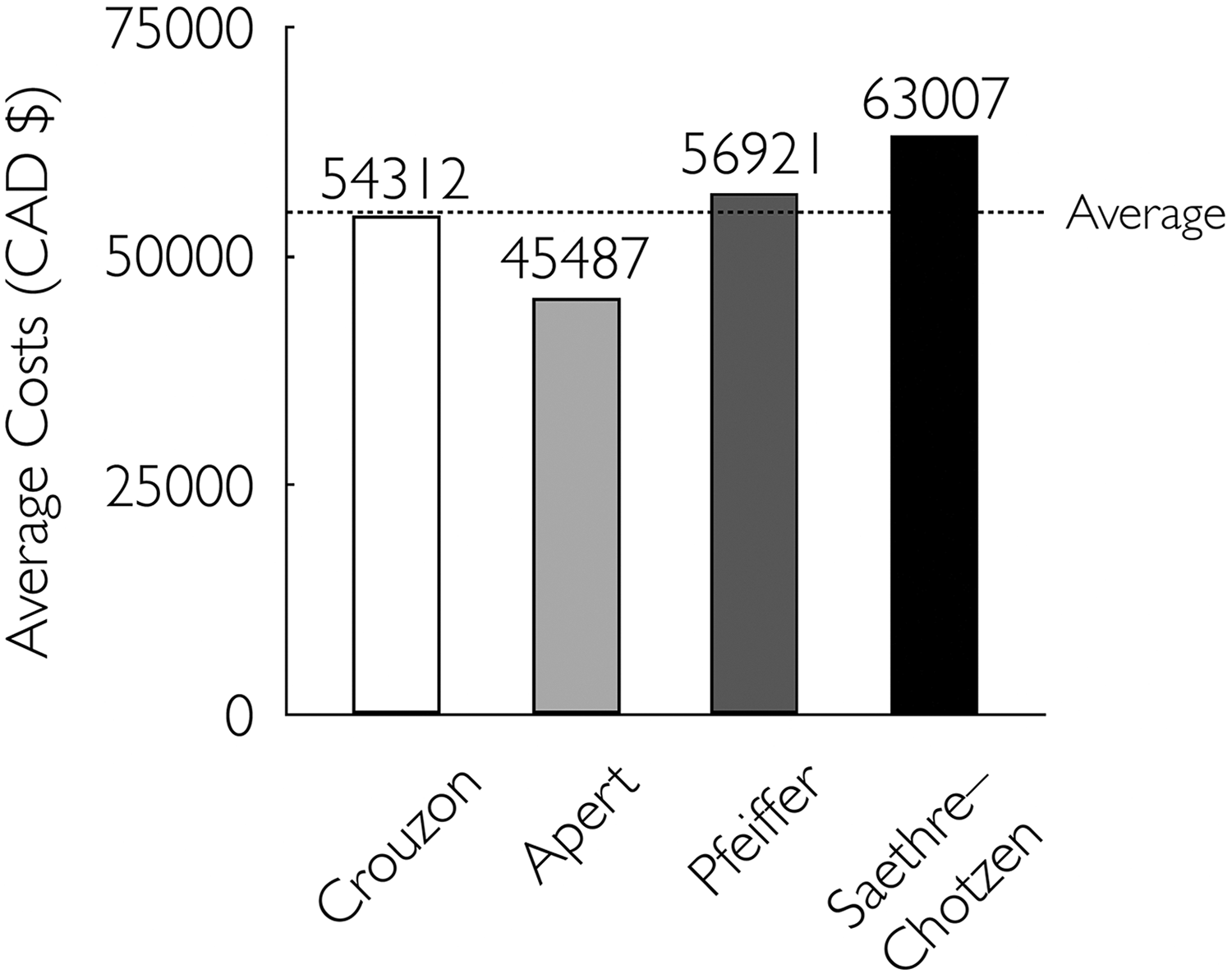
Average cost comparison by craniofacial syndrome.
Differences in costs between the 2 groups were seen in the breakdown of mean ICU expenses (DO $5585 ± $1594 compared to SS $17 747 ± $8451; P = .004) and total OR costs (DO $12 540 ± $6215 compared to SS $9696 ± $3.714 NS; P = .35; Figure 2).
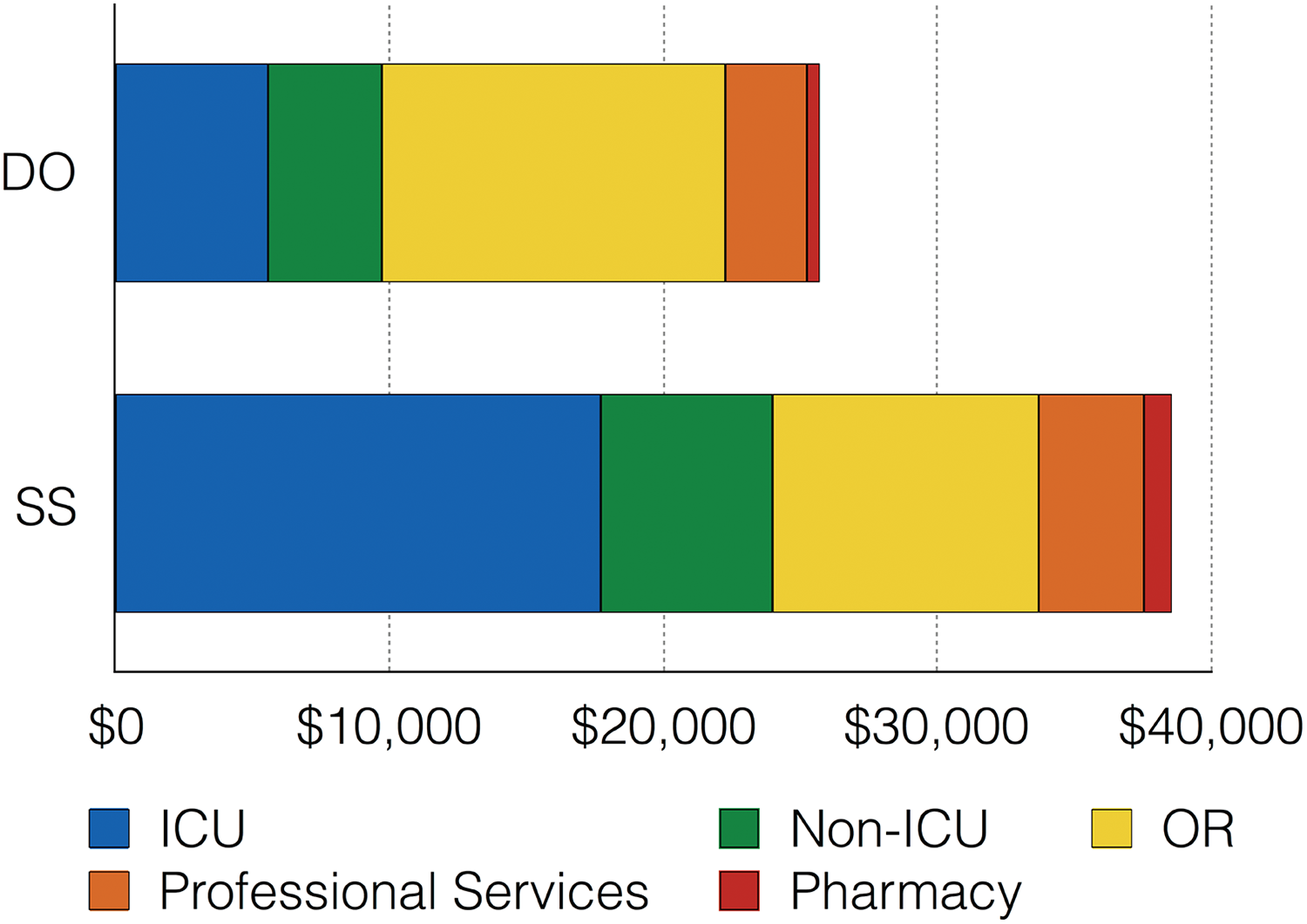
Average cost breakdown by category of expenditure.
Discussion
In this study, comparing costs of the Le Fort III osteotomy in patients with syndromic craniosynostosis at the Hospital for Sick Children, Toronto, demonstrates average total treatment costs are significantly lower when DO techniques are employed compared with the costs of single-stage rigid internal fixation and IMF. Furthermore, time in the OR, length of stay in the ICU, and hospital length of stay are also significantly shorter in the DO group.
In a recent retrospective analysis of outcomes and costs following primary cranial vault remodeling for isolated sagittal craniosynostosis, Wolfswinkel et al found that daily average costs for a general ward bed and ICU bed were US$5700 and US$11 220, respectively. 9 Furthermore, for the group of 98 patients, the authors calculated that reducing postoperative ICU length of stay by 1 day would result in $540 960 in savings over 7 years. These values also align with previously reported financial savings by Seruya et al in a cohort of pediatric patients with craniosynostosis who underwent fronto-orbital advancement. 10 In that study, mean daily charges in ICU were $7652 compared to $2470 for care on a medical–surgical ward.
Equipment costs have often been cited as a reason not to employ DO techniques as they may range from US$3100 to US$5950. 7 However, it would appear that while equipment expenses, as reflected in the OR costs in patients with DO, are slightly greater, they are overshadowed by the financial burden brought about due to longer length of stay in the ICU and prolonged hospitalization in patients undergoing SS Le Fort III osteotomies with rigid internal fixation and IMF.
Treatment using DO techniques involves a 2-stage approach with a brief return to the OR to remove the external head frame under anaesthesia, and this technique prolongs the total length of treatment. In our institution, a second return for arch bar removal was also performed in the OR under anaesthesia, but the length of total treatment time was shorter with the SS technique.
What hasn’t been measured as a part of this study is the considerable burden of care placed on the patients and parents with these techniques. Distraction osteogenesis requires parents to turn the device twice daily for 2 to 3 weeks and this may generate transient but real discomfort to the patient. Furthermore, daily pin site care and pin tightening is required. Continual observation and activity restriction is a concern in young children with external head frames. Furthermore, despite no obvious contraindications, most patients undergoing DO tend not to attend school while wearing the head frame. On the contrary, prolonged ICU stay (range 4-11 days) and length of hospitalization (range 7-14 days) in addition to the burden of being maintained in IMF and the concomitant nutritional, oral hygiene, and communication issues must be weighed against the advantages of a shorter length of treatment.
Ultimately, it would be of benefit to assess outcomes of these 2 different treatment paradigms to determine whether economic advantage is associated with improved clinical results. Patient satisfaction, relapse, need for additional surgery, airway, and morphometric assessment of the craniofacial skeleton are desired parameters to measure but out of the scope of this study. Additionally, a comprehensive cost analysis incorporating these factors along with long-term data on complications, reoperation rates, and aesthetic outcomes would be a major contribution to the literature but are beyond the scope of this study.
This study is limited by a small sample size of relatively heterogeneous patients and the potential problem of siloed institutional financial practices. Specifically, cost savings in one area may not have relevance in another, although the budget-driven system of the Canadian health-care system will demonstrate an impact on the bottom line. Nevertheless, coordinated efforts to collect cost data between multiple Canadian pediatric craniofacial centers would yield valuable information to inform future practice.
Future studies could factor in the impact of multiple clinic visits to global cost differences, especially those incurred directly by families that were not captured by our cost accounting department. Parental lost wage as a result of time-off work is another cost that was not factored into our analysis. 11 Integrating patient-reported outcomes on their satisfaction with the entire course of treatment would augment our understanding of what factors are important to emphasize to patients when presenting surgical options. Studies presenting cost of interventions will have greater impact on policy and medical decision-making if methods compare cost and outcome measures in terms that incorporate patient preference and morbidity. 12
Conclusion
This single-institution retrospective economic analysis indicates Le Fort III osteotomy in syndromic craniosynostosis with single-stage advancement has higher overall costs than DO. Despite higher OR costs, recovery time and costs incurred during ICU admission led to this cost discrepancy. Future cost-effectiveness studies of these 2 techniques should incorporate patient-reported outcomes and metrics of quality of life.
Footnotes
Level of Evidence
Level 3, Therapeutic
Author’s Note
A.M., E.H., C.R.F., M.F., L.Z., and J.P. contributed to the background literature review, data analysis, and the manuscript writing and revision.
Declaration of Conflicting Interests
The author(s) have no existing conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.