
Abstract
Background:
In facial reanimation via microneurovascular muscle transfer, dual-nerve reinnervation of the muscle capitalizes on the synergistic effects of spontaneous motion from cross facial nerve grafting (CFNG) and increased excursion from masseteric nerve transfer. Two-stage approaches that delay masseteric nerve transfer until the time of the muscle flap increase spontaneity by maximizing muscle reinnervation from the CFNG. While this 2-stage, dual-nerve approach has been described in adults, we present a series of pediatric patients who underwent this reconstructive technique.
Methods:
We retrospectively reviewed all pediatric patients who underwent 2-stage, dual-nerve reconstruction with CFNG and ipsilateral masseteric nerve transfers. Procedures were performed between 2004 and 2016 by 2 surgeons at a single centre. Degree of facial paralysis before and after surgical intervention was measured using House-Brackmann scores.
Results:
Nine patients with a mean age of 8.6 (range: 5-15 years) years at time of surgery underwent 2-stage, dual-nerve reconstruction. Average time between CFNG and transfer of the free gracilis with masseteric nerve transfer was 13.3 (SD 2.4) months. Mean follow-up was 27.3 months (SD 25.7). Patients demonstrated initiation of voluntary movement on paralyzed side by 3.6 months (SD 0.6) on average, with 3 patients demonstrating spontaneous movement at 3 months.
Conclusion:
The 2-stage, dual innervation technique using CFNG and delayed ipsilateral masseteric nerve transfer with a free gracilis is a promising reconstructive option to maximize spontaneous expression in pediatric patients. Validated, objective scoring systems for excursion are needed before meaningful comparisons can be made to other reconstructive strategies.
Introduction
Congenital facial paralysis affects approximately 21 per 100 000 children and is a debilitating condition that significantly impairs non-verbal communication. 1,2 It also results in functional deficits including nasal obstruction, oral incompetence, dysgeusia, dental decay, and corneal exposure with possible loss of vision. 3,4 As such, facial paralysis patients have a variety of negative psychological and physical sequelae that lead to diminished quality of life. 3,5
For patients undergoing microneurovascular muscle transfer for smile reconstruction, coaptation of the muscle’s motor nerve to a cross facial nerve graft (CFNG) allows for spontaneity of movement but is frequently limited by weak excursion. 6,7 One-stage procedures that isolate a branch of the masseteric nerve for neurotization of the muscle transfer results in greater excursion but fail to provide spontaneous expression. 6 To overcome these limitations and to allow both spontaneous motion and improved neural drive for the transferred muscle, dual innervation of the muscle transfer via both a CFNG and an ipsilateral masseteric nerve transfer performed in a single stage has reported improved outcomes in the adult population. 8,9 A 2-stage, dual innervation technique has also been described in the adult population, with cross-facial nerve grafting done as the first stage. After a suitable time for regeneration of contralateral facial nerve axons to the end of the CFNG, a microneurovascular transfer with its motor nerve coapted to both the CFNG and an ipsilateral masseter motor nerve. 9 The goal of this approach to enhance spontaneous expression by allowing axons from the CFNG to reach the muscle transfer at the same time as the masseteric axons. Because of their increased capacity for neuronal plasticity, children often adapt more readily to reconstructive efforts than adults making a dual-nerve strategy promising for this patient population. 10 We report a series of pediatric patients who underwent facial reanimation via gracilis microneurovascular transfers using a 2-stage, dual-nerve approach. We hypothesized that after a 2-stage, dual innervation technique in pediatric patients, we would observe both spontaneous motion and excellent excursion of the transferred muscle.
Methods
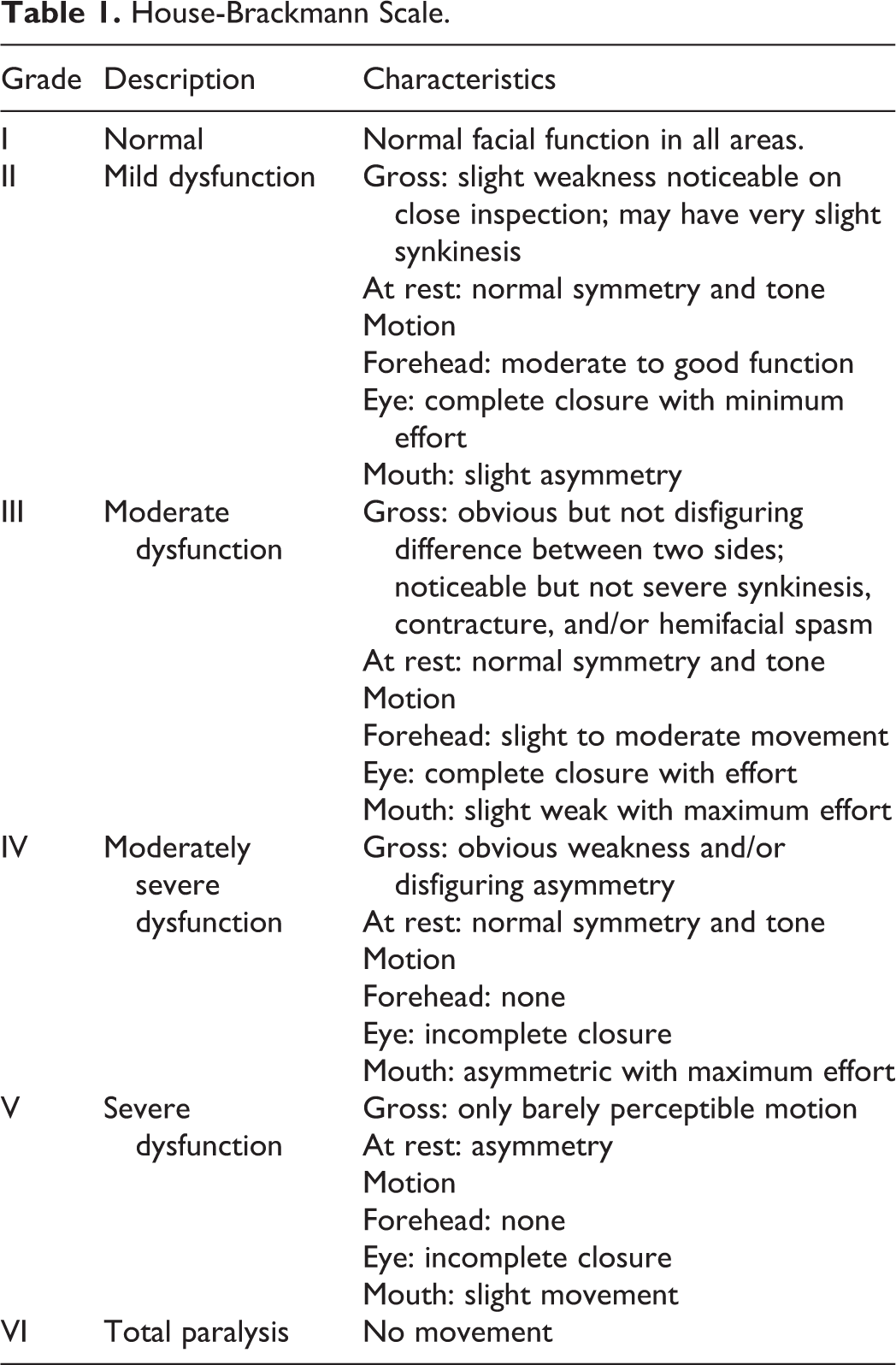
After obtaining approval from the institutional review board at the University of Michigan (IRB approval HUM00130877), we reviewed all pediatric patients manifesting unilateral facial paralysis who underwent 2-stage, dual-innervation of a gracilis microneurovascular muscle transfer for facial reanimation. All procedures were between March 2004 and August 2016. All patients underwent CFNG during the first procedure. After enough time for regeneration of facial nerve axons to the terminus of the CFNG, a microneurovascular segmental gracilis muscle transfer was performed for smile reconstruction. Innervation of the muscle was via a coaptation of the distal ends of both the CFNG and an ipsilateral masseteric nerve to the proximal end of the muscle motor nerve (Figure 1). Demographic information including age, sex, and etiology of paralysis were recorded. In addition, hospital data including length of stay, length of surgery, and interval between surgeries were recorded. Finally, clinical outcomes including time to voluntary and spontaneous expression, post-operative complications, and pre- and post-operative House-Brackmann (HB) scores were recorded. House-Brackmann scores were recorded at 6 months and 12 months. House-Brackmann ratings are given on a scale of I (normal) to VI (total paralysis) shown in Table 1. 11 This system includes secondary defects, differentiates between moderate degrees of dysfunction, and facilitates interpretation and communication of facial nerve reanimation results. 11 As HB ratings below IV require forehead movement, patients with involvement of the temporal and zygomatic branches were incapable of attaining scores better than IV. 11
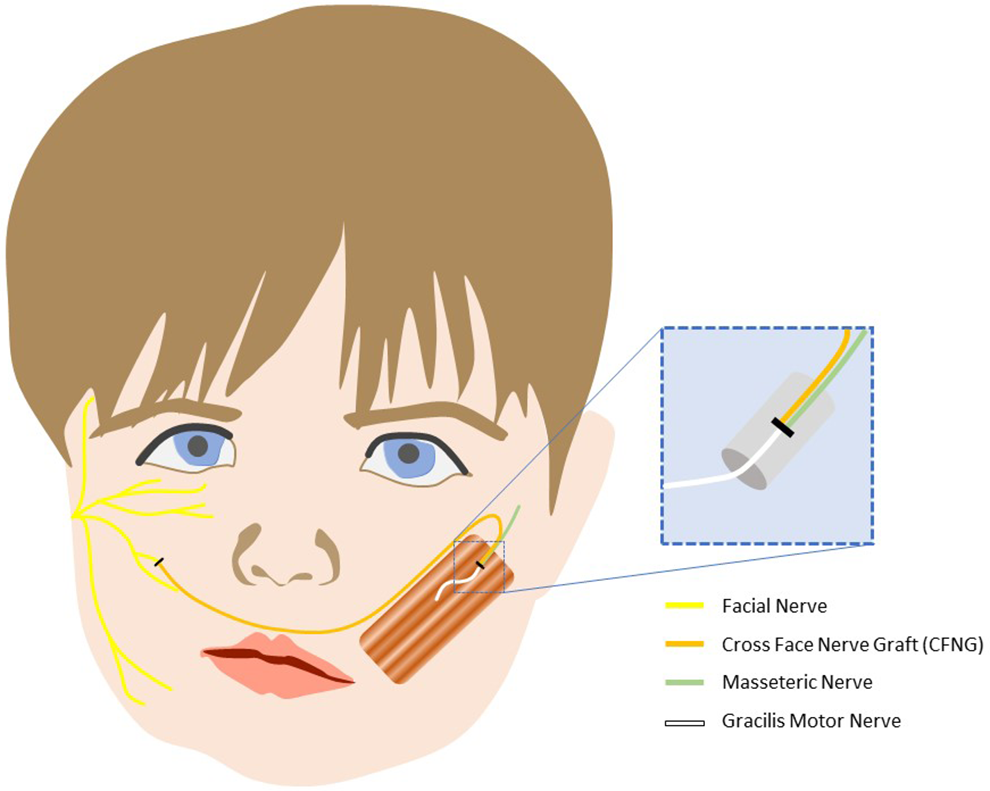
Coaptation of the distal ends of the CFNG and the ipsilateral masseteric nerve to the proximal end of the muscle motor nerve.
House-Brackmann Scale.
Surgical Technique
For the first stage, we harvested a sural nerve graft for cross facial innervation. A pre-tragal incision was used to identify branches of the facial nerve distal to the parotid gland on the non-paralyzed side of the face. A buccal branch controlling primarily smile (upper lip elevation and lateral commissure motion) was identified and selected for division and coaptation to the reversed sural nerve graft. Care was taken not to select any branches innervating the orbicularis oculi. After coaptation to the buccal branch, the CFNG was then passed to the paralyzed side through a tunnel inferior to the nasal vestibule. The distal end of the graft was positioned anterior to the tragus, clipped, and marked with a prolene suture for easy identification in the second stage.
During the second procedure, all patients underwent ipsilateral free gracilis muscle transfer. After examining the vector of smile on the normal side of the face and marking the nasolabial fold on both sides, pre-tragal incision was made on the paralyzed side, and a standard sub-superficial musculoaponeurotic system (SMAS) dissection was performed. First, recipient vessels were isolated and identified, typically the facial artery and vein. The masseter motor nerve and the previously placed CFNG were identified and isolated. A series of 2-0 Vicryl stitches were placed into the oral commissure, the upper lip, and the lower lip to anchor the insertion of the muscle transfer and so that traction on the sutures resulted in a natural nasolabial crease and smile. Next, an ipsilateral segmental gracilis muscle flap of the appropriate dimensions was harvested with its neurovascular bundle. Prior to transferring the muscle, Vicryl stitches were used to mark out 1-cm intervals along the muscle to demarcate the degree of stretch in its resting state. The muscle was then harvested and brought to the face. The origin of the muscle was anchored to the fascia overlying the zygomatic arch, and the insertion to the commissure, upper, and lower lips using the previously placed stitches. The smile was slightly over corrected, and all efforts were made to maintain the resting tension of the gracilis muscle following inset. The muscle was re-vascularized via anastomosis of the flap vessels to the facial artery and vein. The gracilis transfer was reinnervated using a microporous collagen nerve tube (Neuragen bovine graft, Integra Lifesciences) with the CFNG and the masseter motor nerve in the proximal end and the gracilis motor nerve in the distal end. The nerves were anchored within the tube using 8-0 nylon epineural stitches; a 1 to 2 mm gap was left between nerve ends within the tube. A drain was left on the affected side.
Follow-up visits with patients occurred at 2 weeks, 6 weeks, 3 months, and then every 2 to 3 months for a year (or until evidence of movement was noted). Patients were then seen every 6 to 12 months based on progress. Follow-up visits consist of a facial nerve exam, static and dynamic photos, as well as video.
Results
Nine patients fulfilled inclusion criteria in our study (Table 2). Four were males, and 5 were female, with an average age of 8.6 years at the time of free functional muscle transfer. Four children had congenital facial paralysis, 2 children developed paralysis iatrogenically following surgical excision of congenital tumours, and 3 children acquired paralysis following trauma. On average, 12 (SD 2.1) months elapsed between CFNG and functional gracilis free transfer. The second surgery lasted on average 7.6 (SD 1.75) hours, and patients had an average post-operative hospitalization period of 3.8 (SD 0.93) days. The average follow-up period was 2.3 (SD 2.2) years.
Patient Demographics and Results.
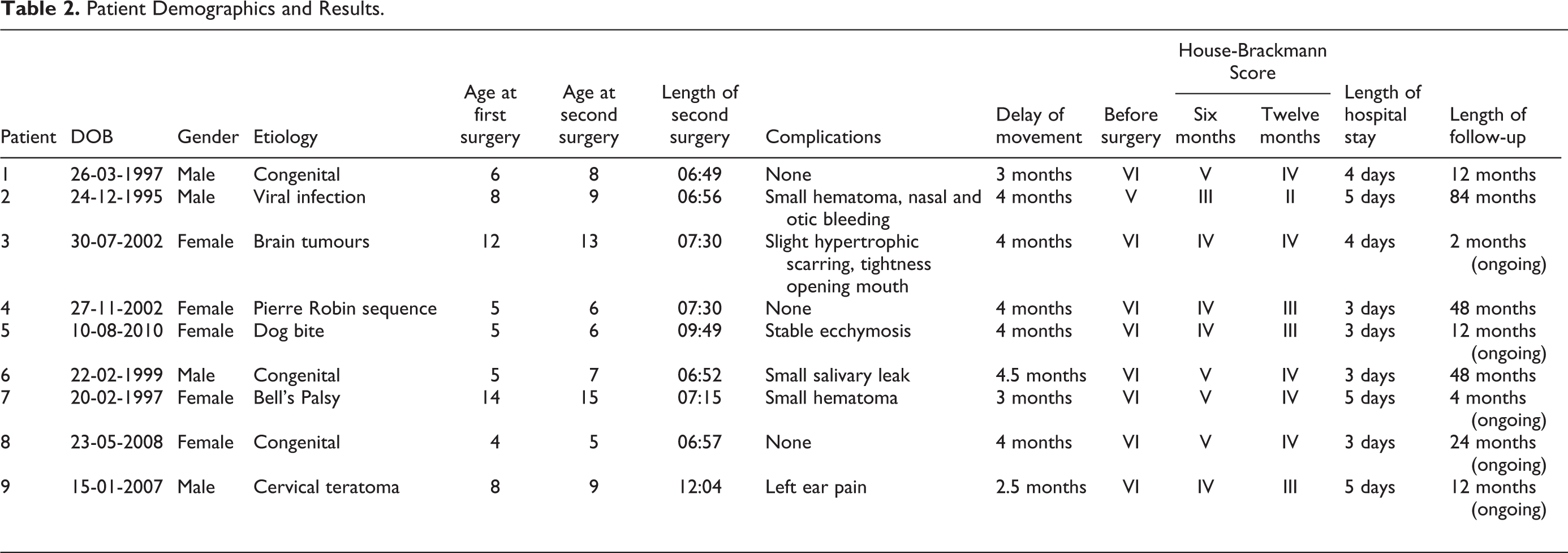
The first observed instances of muscle firing were recorded between 2.5 and 4 months for all patients, with a mean time to firing being 3.6 (SD 0.6) months. Once firing was observed on exam, patients were instructed on “mirror exercises” to improve spontaneity of their smile. Spontaneous movement was noted between 3 and 7 months, with a mean time to spontaneity of 4.8 (SD 1.4) months. We noted interval gains in muscle excursion that stabilized around 12 months for all patients (Figures 2 –4). Eight of the 9 patients had initial HB scores of VI (total paralysis) and 1 patient had an initial HB score of V (severe). At 6 months, all patients demonstrated improvements in HB ratings by at least 1 level of severity. House-Brackmann ratings continued to improve such that the final HB scores included 5 patients with a score of IV, 3 patients with a score of III, and 3 patient with a score of II.
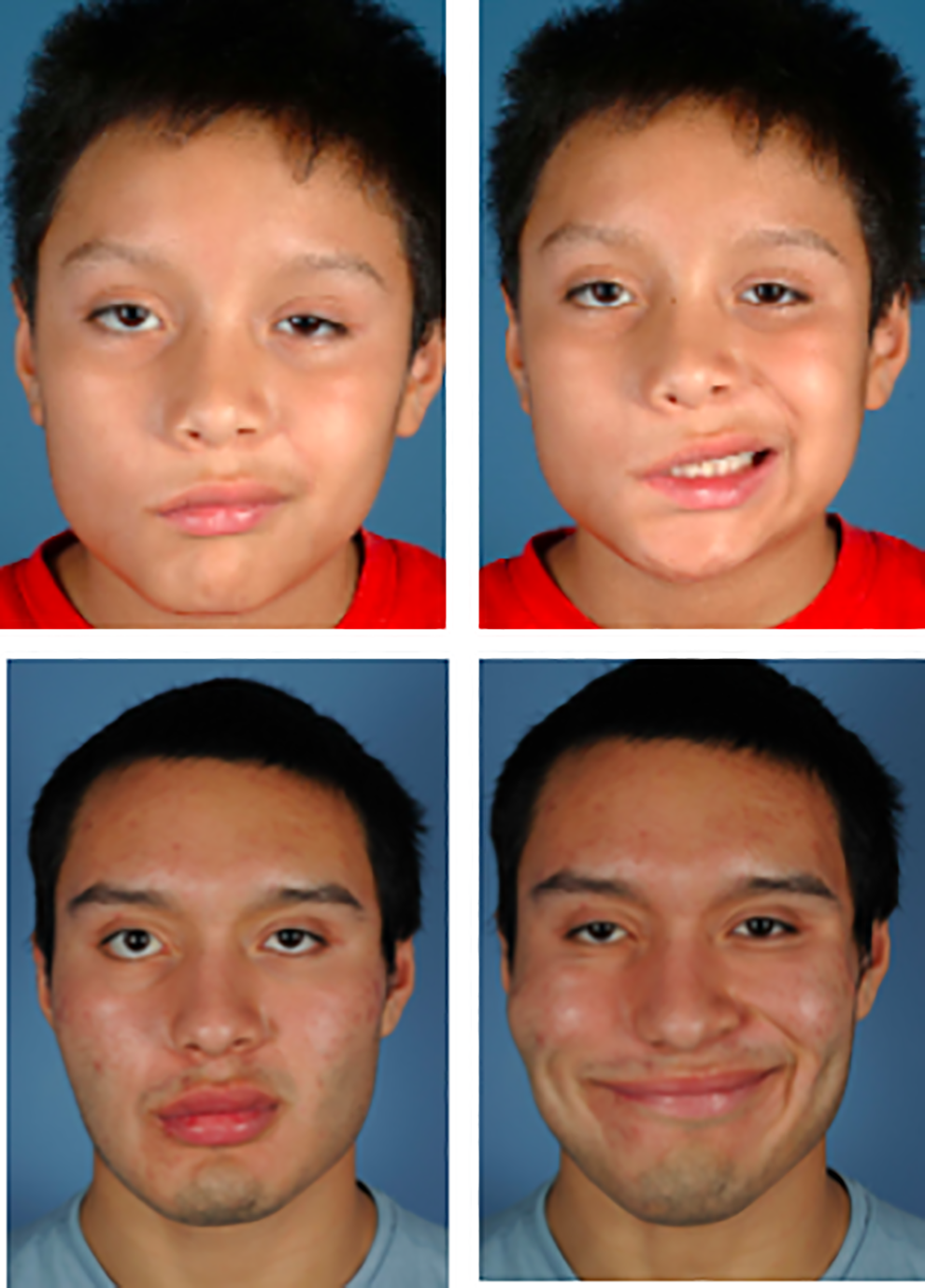
Patient 2 before surgery (top) and 39 months after dual facial innervation of the gracilis free flap (bottom). While smiling, patient was instructed to clench teeth.

Patient 5 before surgery (top) and 5 months after dual innervation with gracilis free flap (bottom). While smiling, patient was instructed to clench teeth.

Patient 9 before surgery (top) and 6 months after dual innervation with gracilis free flap (bottom). While smiling, patient was instructed to clench teeth %.
Regarding complications, 1 patient developed a salivary leak, and another patient complained of hypertrophic scarring along the pre-tragal incision and tightness with mouth opening. The salivary leak and scarring resolved with conservative care without necessitating surgical intervention.
Discussion
In this case series, 9 pediatric patients successfully underwent 2-stage, dual-nerve innervation for the treatment of facial paralysis. Patients gained excursion by 3.6 months on average, with continued improvement until 12 months. Three patients demonstrated spontaneity in excursion as early as 3 months, and all 9 patients demonstrated spontaneity by 7 months. All patients demonstrated improved HB scores. Of note, some patients could not achieve a score above IV, as scores of I-III indicate either normal or mild forehead dysfunction. 11 Therefore, since the 2-stage, dual-nerve innervation treatment does not provide motion to the forehead, only patients with normal or mild forehead dysfunction could score below IV. Moreover, very few complications occurred.
Pediatric reconstruction for prolonged facial paralysis was performed in 2 stages: CFNG followed by a second-stage free muscle transfer 12 to 18 months later. 3 The gracilis is favoured over other options because of its expendability, consistent anatomy, parallel-fiber architecture, and comparative ease of harvest. 12 Free gracilis muscle transfers have frequently been used for facial reanimation patients with long-term facial paralysis, as facial mimetic muscles atrophy after approximately 1 year of denervation. 3,12,13 Additionally, sensory donor nerves (eg, the sural, medial antebrachial cutaneous, or great auricular) are preferred for CFNG due to their low morbidity. 14,15
Critical factors in this procedure include the selection of the appropriate motor nerve to innervate the muscle flap. 14,16,17 The contralateral facial nerve remains superior in terms of coordinated movements of the reanimated face since it provides a similar motor source of innervation. 7 Although free functional muscle transfer with coaptation to a CFNG allows for spontaneity of movement, weak excursion in some patients has been consistently reported. 6,7 Reddy and Redett describe their optimal approach to facial reanimation in the pediatric patient as consisting of 3 stages: (1) cross-facial nerve graft, (2) free tissue transfer, (3) cosmetic balancing procedures. However, only utilizing the cross-facial nerve graft allows weakness in excursion secondary to both the distance the axons must travel and fewer axonal inputs compared with other viable nerve options. 7 The buccal branches of the facial nerve typically chosen for CFNG have only 100 to 200 axons, of which only 10% to 50% reach the distal end of the CFNG. 18 In contrast, neurotization of the gracilis by the masseteric nerve provides up to 1500 motor axons and generally allows for a more “powerful” smile. 7,15,19 The drawback in utilizing the masseteric nerve alone is the need for long-term biofeedback training due to the necessity of activating the masseter muscle in order to produce a strong smile. 15,19 Although this is effective in some patients, many patients, especially adolescents, with masseter-motor nerve innervated fail to incorporate their muscle transfers into effective facial animation. So, single-nerve procedures that isolate a branch of the masseteric nerve for neurotization of the muscle provide greater excursion at the expense of spontaneity and those that rely on CFNG allow spontaneity at the expense of excursion/power. 6
Previously described dual reinnervation techniques in the adult population take advantage of the benefits of both nerve options while simultaneously mitigating their respective disadvantages. 20,21 In addition to using the contralateral facial nerve, the masseteric nerve is also coapted to the obturator nerve at the time of free gracilis transfer. This provides better results by maximizing excursion via the masseteric nerve and spontaneity via the CFNG.
Dual innervation can be done in 1-stage, as described in the adult population, which aims to minimize surgical procedures for the patients and improve recovery time. 8,22,23 However, performing the reconstruction in 2 stages allows increased innervation from the CFNG by delaying the masseteric nerve transfer, possibly leading to improved spontaneity. 9 In more recent years, this approach has been described in the adult population by Cardenas-Mejia et al using the masseteric nerve and CFNG. 9 They propose that while coaptation of the masseter nerve and the CFNG in a single stage can achieve more rapid reinnervation and stronger muscle contraction, spontaneity will be lessened. 9 This result arises from the interference of the axons from masseter nerve with the recruitment of motor units to the CFNG axons. 9
We similarly advocate for a 2-stage, dual innervation technique in the pediatric population because concern remains that masseteric nerve axons may overpower the cross facial nerve axons in a single-stage procedure. 9 If the masseteric axons are allowed to innervate the gracilis while cross facial nerve axons travel across the face over several months, the CFNG axons will encounter only stable, reinnervated motor units and will be unable to form synaptic connections with the target muscle. 9 Therefore, the benefits of added control and spontaneity with a CFNG in addition to the powerful excursion provided by the masseteric nerve may never be realized in a one stage procedure. 9 In the literature, 1-stage facial reanimation studies have reported mildly increased delays of spontaneity. 8,22,23 Bianchi et al performed 1-stage CFNG and masseteric nerve cooptation on 8 patients and observed spontaneity in excursion 7 to 13 months post-operatively. 8 In comparison, our 2-stage, dual innervation technique demonstrated spontaneity in excursion 3 to 7 months post-operatively. While this comparison does not speak to degree excursion, quicker improvement in spontaneity encourages patients to further pursue mirror exercises that improve reanimation outcomes and overall quality of life.
This study it is not without limitations. First, we were limited by low power and a single-centre design, thus limiting the generalizability of our results. Additionally, we were unable to compare this technique to a single-stage technique
Conclusion
Using a 2-stage dual innervation technique for long-standing facial paralysis maximizes the potential for spontaneous expression by allowing the CFNG axons to reach the recipient nerve prior to masseteric nerve coaptation and free muscle transfer. This approach should be considered when considering facial nerve reanimation in the pediatric population. A more expansive study, incorporating comparisons of various techniques, would further delineate the best reconstructive option for facial reanimation in children. Additionally, the development of patient-reported outcome measures specific to this patient population is critical for determining the impact of these operations from the patient perspective.
Footnotes
Authors’ Note
This paper has been presented at the Plastic Surgery Research Council 2019.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Katelyn G. Makar is currently supported by the National Institute of Dental and Craniofacial Research (1F32DE027604-01).