
Abstract
Introduction
The use of botulinum toxin has quickly become a preferred method for wrinkle control since its introduction in the cosmetic applications. 1 In fact, it is the most frequently performed cosmetic procedure in the United States. 1 In a study conducted in Saudi Arabia, the botulinum toxin injection was the second most widely undergone cosmetic procedure after laser hair removal. 2 The popularity of botulinum toxin injections can be explained by the fact that it is a minimally invasive procedure that provides noticeable results and positive patient satisfaction. 1 The botulinum toxin injection can be used to treat a variety of conditions. It is used to reduce the appearance of hyper-dynamic lines in specific areas, such as forehead, between the eyebrows, deep neck, and crow’s feet besides the eyes. 3 It can also be used for the treatment of hyperhidrosis, such as excessive sweating in the underarm, palms, or soles. 4
The botulinum toxin injection is considered as a relatively safe procedure with few side effects. Since botulinum toxin requires percutaneous injection to reach desired muscle sites, one of the main disadvantages of these injections is pain at the injection site. 5 Several techniques have been adopted to lessen the discomfort associated with these injections, including topical anesthetic creams and peripheral nerve blockage. 6,7 Reconstitution of botulinum toxin in different solutions can also help in reducing pain. 8 The current indication is that it should be reconstituted with normal saline (NS). 7 An alternative may also be reconstitution of botulinum toxin with alkalinizing agents such as sodium bicarbonate (SB) for isotonicity. 9,10 To the best of our knowledge, the effects of reconstitution of botulinum toxin A with SB on pain reduction and increase in its efficacy have not been studied yet. Therefore, in this study, the effects of reconstitution of botulinum toxin A injection with SB on pain perception, duration of action, and the onset of action in the aesthetic treatment of hyper-dynamic lines of forehead and glabellar region were investigated. Based on the results by Lowe et al, 10 as primary objective, the effects of botulinum toxin diluted with 0.1-mL SB and 2.4-mL NS were studied. Then, other concentrations of SB were also tested as secondary objectives to study the differences in pain scores between different concentrations.
Methodology
Study Design and Methods
The study followed a prospective, double-blinded interventional design. It was a split-face, parallel-group, randomized clinical trial where the unit of randomization was the individual unilateral forehead. The study was reviewed and approved by institutional review board at King Abdullah International Medical Research Center (KAIMRC; study number: RC19/371). Clinical trial number: NCT04579419.
Participants
Female patients of age >25 years, who presented to outpatient clinics and were scheduled to receive botulinum toxin injection, were invited to participate in the study. The participation in this study was voluntary. Exclusion criteria included the patients having neuromuscular diseases, any active infection in treatment area, receiving anticoagulants or diagnosed with bleeding disorders, or patients undergone prior facial cosmetic surgical procedures, such as eyebrow lift. The patients meeting the inclusion criteria were assessed prior to recruitment and provided with a full explanation of the study. The data were collected from February 23, 2020, through March 16, 2020. Follow-up was completed on June 16, 2020. Written informed consents were obtained from all the patients.
Sample Size
All the patients, who visited outpatient clinics for botulinum toxin injections from February 23, 2020, to March 16, 2020, and met the inclusion criteria, were enrolled in the study. A total of 30 patients agreed to participate in the study.
Blinding
Patients were randomly assigned to receive the botulinum toxin injections mixed with NS on one half of their face (left or right) and the solution containing the mixture of SB and NS on the contralateral side. Blinding was performed by assigning one investigator, who prepared the solutions and another investigator performed the botulinum toxin injections. Neither the investigator performing the injections nor the patients receiving them knew which solution was being injected. Both the solutions were drawn up with identical needles that contained no distinguishing marks. After the injections, another investigator took the pain Visual Analogue Scale (VAS) score from the patients.
Intervention
For the primary objective, the patients received either botulinum toxin reconstituted with NS only or botulinum toxin reconstituted with NS and 0.1 mL of SB. The solutions included: (1) Botulinum toxin reconstituted with NS; 100 MU Botox (onabotulinumtoxinA; Allergan) was reconstituted with 2.5 mL of NS; (2) botulinum toxin reconstituted with NS and SB; 100 MU Botox (onabotulinumtoxinA; Allergan) was reconstituted with 2.4-mL NS and 0.1-mL SB.
For the secondary objective, the botulinum toxin was diluted with 4 different concentrations, which included 2.45-mL NS with 0.05-mL SB; 2.25-mL NS with 0.25-mL SB; 2-mL NS with 0.5-mL SB; and 2.5-mL SB only.
The standard injection scheme was followed as per Food Drug Administration’s approved dosage. 11 For the glabellar lines, the injected dose was 0.1 mL (4 units) into each of the 5 sites, including 1 in the procerus muscle and 2 in each corrugator muscle, making a total dose of 20 units. Similarly, for the forehead lines, the total dose was 20 units, where 0.1 mL (4 units) was injected into the 5 forehead line sites. All the injections were performed identically on both sides of the face. The botulinum toxin solution was injected intramuscularly in a balanced flow of 3 to 4 seconds with a 30-gauge needle. The injection site was then pressed lightly in order to avoid botulinum toxin washout and bleeding. The patients were followed up for 10 minutes to make sure there were no complications.
Outcome Measures
Two modes of data collection were used. In order to assess pain severity, the patients were interviewed using a hard copy of VAS questionnaire survey. The VAS score ranged from 0 to 10, where 0 represented no pain and 10 represented the greatest imaginable pain. The onset and duration of action of botulinum toxin injections were assessed according to the patients’ subjective opinions. The patients were given a VAS scale questionnaire immediately after the botulinum toxin injections.
Statistical Methods
The data were entered and analyzed using Excel version 16 for Mac. The age was represented as mean and SD. For the VAS scores, the 2-tailed paired-sample t tests were completed, where sample sizes were permitted, with a significance threshold at P value of <.05. χ2 test was applied to investigate the significance of the onset and duration of action of the solutions.
Results
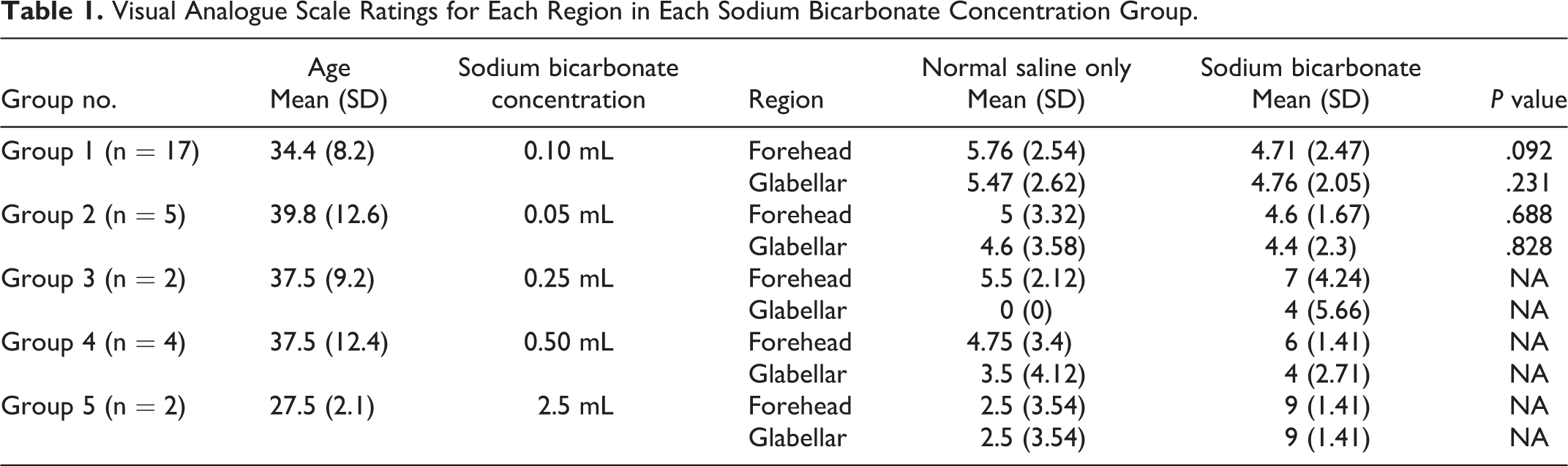
The characteristics of samples in each of the 5 dosage groups are listed in Table 1. The mean age of all the groups was similar, ranging from 27 to 39 years. For the VAS scores, group 1 reported a mean VAS score of 4.71 and 4.76 in the side containing SB and 5.76 and 5.47 in the side mixed with NS only of the forehead area and glabellar area, respectively. The VAS ratings at 0.01-mL SB are shown in Figure 1. The results of group 2 were as follows: For the forehead and glabellar region, mean VAS score was 4.60 and 4.40 in the SB containing side versus 5.00 and 4.60 in the side mixed with NS only. The mean and SD of VAS ratings of the other groups are listed in Table 1.
Visual Analogue Scale Ratings for Each Region in Each Sodium Bicarbonate Concentration Group.
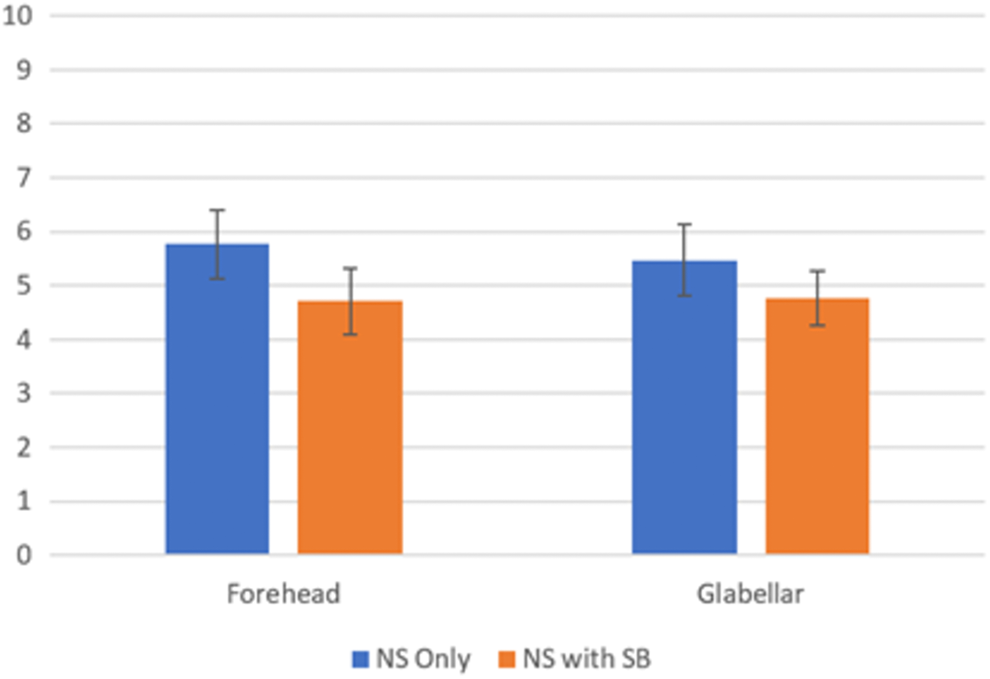
Pain intensity ratings for normal saline only and normal saline with 0.1-mL SB at each injection site.
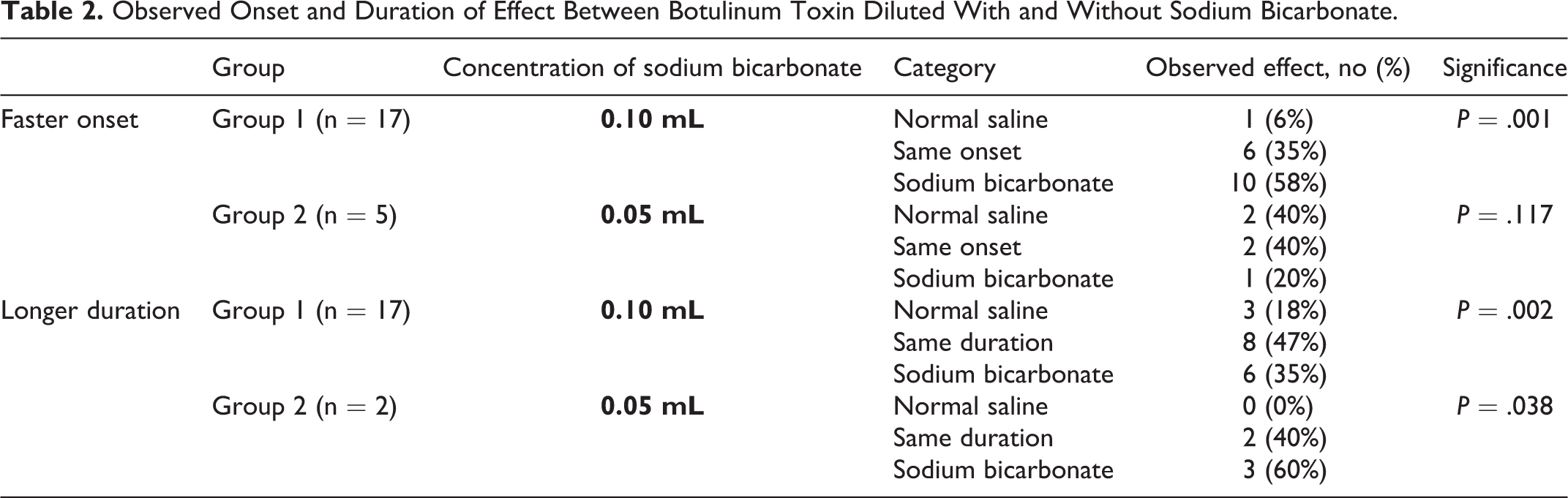
The comparison of the onset and duration of action between solutions mixed with and without SB in group 1 and group 2 is listed in Table 2. Regarding the onset of action, out of the 17 patients, who received a concentration of 0.1-mL SB, 10 (58%) patients had faster onset on the side containing SB (P < .001). In group 2, only 1 (20%) of the 5 patients showed a faster onset on the SB side of face. For the duration of action in group 1, 6 (35%) of the 17 patients had a longer duration of action on the side mixed with SB (P < .002), while 3 (60%) of 5 patients, who received an SB concentration of 0.05 mL, showed a longer effect in the SB containing side.
Observed Onset and Duration of Effect Between Botulinum Toxin Diluted With and Without Sodium Bicarbonate.
Physician evaluation 1 week after the injection showed a faster onset in the 0.1-mL SB containing side in one participant only. Physician did not notice a difference in onset or duration of action in any of the other participants.
Discussion
Pain Perception
Pain is the most common disadvantage of botulinum toxin injections.
12,13
This could be associated with its acidic nature, having pH of 5.6.
10,14
While the sample sizes were not enough for statistical testing in group 2, group 3, and group 5, trends were seen toward lower pain intensity ratings with the use of SB as compared to NS only in both the forehead and glabellar regions with 0.05 mL and 0.10 mL SB solutions. This trend approached significance in the forehead at 0.10 mL of SB (P = .092). Other studies have reported different types of solutions to reduce pain. One study compared the pain associated with lidocaine-reconstituted botulinum toxin with NS for the treatment of axillary hyperhidrosis using a 100-mm VAS scoring system. 4 Their study showed a significant reduction in pain with lidocaine-reconstituted solution with a P value of .0027. 4 Another study compared the use of preservative-containing bacteriostatic sodium chloride injection with preservative-free sodium chloride. 9 They reported that the average pain-level on the preservative-containing side was 54% less severe than that on the preservative-free side. 9 The degree of pain reduction was sufficient to be clinically significant for the vast majority of their patients with a P value of 0.0006. 9
In group 5, where botulinum toxin was reconstituted with 2.5 mL of SB, the patients experienced severe pain, erythema, and headache on the SB side that lasted up to 24 hours. This could explain that the higher pH levels are associated with more pain and complications. However, a large sample size is needed to confirm these results. Patients in group 1, group 2, group 3, and group 4 had minor complications, such as swelling and redness at the site of injection in both the solutions with no differences as to which solution had more side effects.
Onset of Action
The onset of action of botulinum toxin at each injection site was categorized into 3 groups: (1) faster onset of action on the botulinum toxin diluted with NS only side of face, (2) faster onset of action on the botulinum toxin diluted with the mixture of SB and NS side of face, and (3) equal onset of action in both sides. In the event that the effect of normal with SB is not distinct from the effect of NS only, all participants were expected to show equal onset times. The lack of this pattern could be explained as the inclusion of SB affected the onset of action. Therefore, the null effect, in which all the participants showed equal onset times, was compared with the observed effect using a χ2 test across the three possible outcomes.
Regarding the speed of onset of effects, a significant number of more participants than expected showed a faster onset of effect at the side containing 0.1-mL SB, as compared to the NS only side. At concentration of 0.05-mL SB, the observed pattern did not differ enough from the null effect to show significance, suggesting that this concentration may be too weak to impact the onset of effect or that a large sample size will be required to identify an effect.
Duration of Action
The duration of effect was also recorded using the same 3 categories; the effect was longest at the site mixed with NS only, the effect was longest at the mixture of NS and SB site, or the duration of effect was equivalent across both sites. The same χ2 testing procedure was applied to investigate the effect of adding SB on the duration of effect. In both the onset and duration of effect, the sample sizes allowed for testing with group 1 and group 2 only.
Similarly, a significant number of more participants than expected showed a longer effect duration in the site mixed with SB (both at 0.05 and 0.1 mL) as compared to the NS only site. This pattern suggested that the inclusion of SB may prolong duration of effect in some. At the concentration of 0.05 mL SB, 60% of the participants showed a longer duration of effect, while this proportion was only 35% in group 1, suggesting that the weaker concentrations may be most beneficial in prolonging the duration of effect.
In contrast to these findings, 1 individual showed a faster onset of effect and 3 showed a longer duration of effect at the NS only sites. This pattern might be attributed to random variability due to a relatively small sample size or might have been influenced by measures not controlled in this study, such as patients not paying enough attention to which side started effect first or which side showed a longer effect. It is also possible that the inclusion of SB was detrimental to affect the onset and duration of effects in these individuals. Additional testing may be required to delineate these findings.
Conclusions
The reconstitution of botulinum toxin with 0.1-mL and 0.05-mL SB reduces pain at the injection site, although not significantly. The onset of action of botulinum toxin mixed with 0.1-mL SB solution showed significantly faster effect than the NS alone. The addition of 0.05 mL and 0.1 mL of SB to the botulinum toxin proved longer duration of action. Further studies with large sample size are needed to determine whether the addition of SB can replace other methods of pain control.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.