
Abstract
Introduction
The Dermabond (2-octyl cyanoacrylate) is a commonly used adhesive agent for wound closure. It has many advantages including the easy handling and good adherence to the skin surface. Stronger and faster skin closure is achieved as compared to the suturing alone. 1 It also acts as a barrier for bacterial entry into the incision line. 2 In addition, the Dermabond being waterproof allows patient to take shower early post-operatively. 2 -4 It also allows sutureless closure of small well approximated lacerations especially in the children. 5 -7
There are few reports in the literature regarding development of allergic contact dermatitis post application of Dermabond. 8 -14 However, there are very few studies regarding the incidence of contact dermatitis post application of Dermabond in surgical patients. In this retrospective study, we evaluated the incidence and characteristics of contact dermatitis post application of Dermabond (Trade name PRINEO manufactured by ETHICON) in patients who underwent plastic surgical breast procedures (Mastopexy and Reduction mammoplasty) in our hospital over the last 3 years.
Patients and Methods
We conducted a retrospective review of 60 patients who had application of Dermabond (PRINEO by ETHICON) over the suture line at King Abdullah bin Abdulaziz University Hospital (Princess Nourah Bint Abdulrahman University) between January 2017 and December 2019. The procedures performed on these patients included Mastopexy and Reduction mammoplasty (Table 1). All the 60 patients had underwent 2 layered closure of skin incisions using interrupted 4-0 polydioxanone (PDS) for dermal layer and continuous 4-0 Monocryl sutures for closure of subcuticular layer, this was followed by application of Dermabond (PRINEO) over the closed incision lines. Mepore dressing was used to cover the operated site, which was removed on the fifth post-operative day. Those patients with known positive allergic history to any medication or Dermabond were excluded from this study. The history of surgery, incidence of type IV hypersensitivity reaction, and characteristics of each patient were investigated from electronic patient record system and photographs.
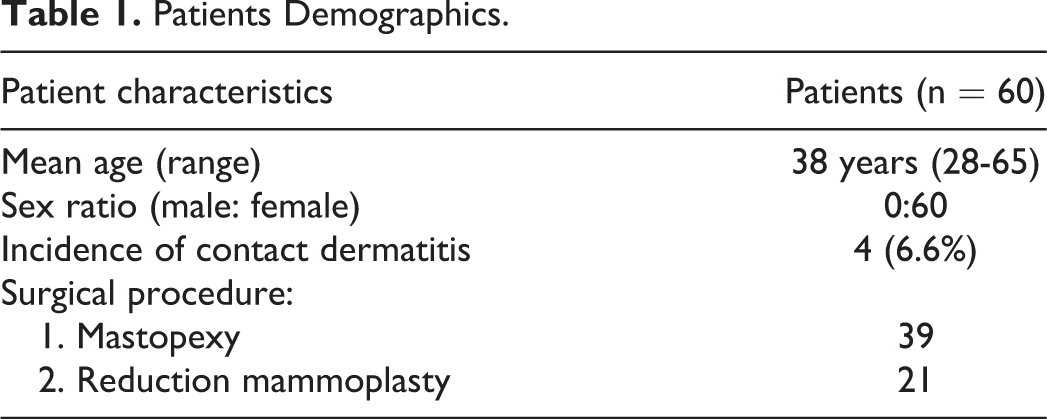
Patients Demographics.
Results
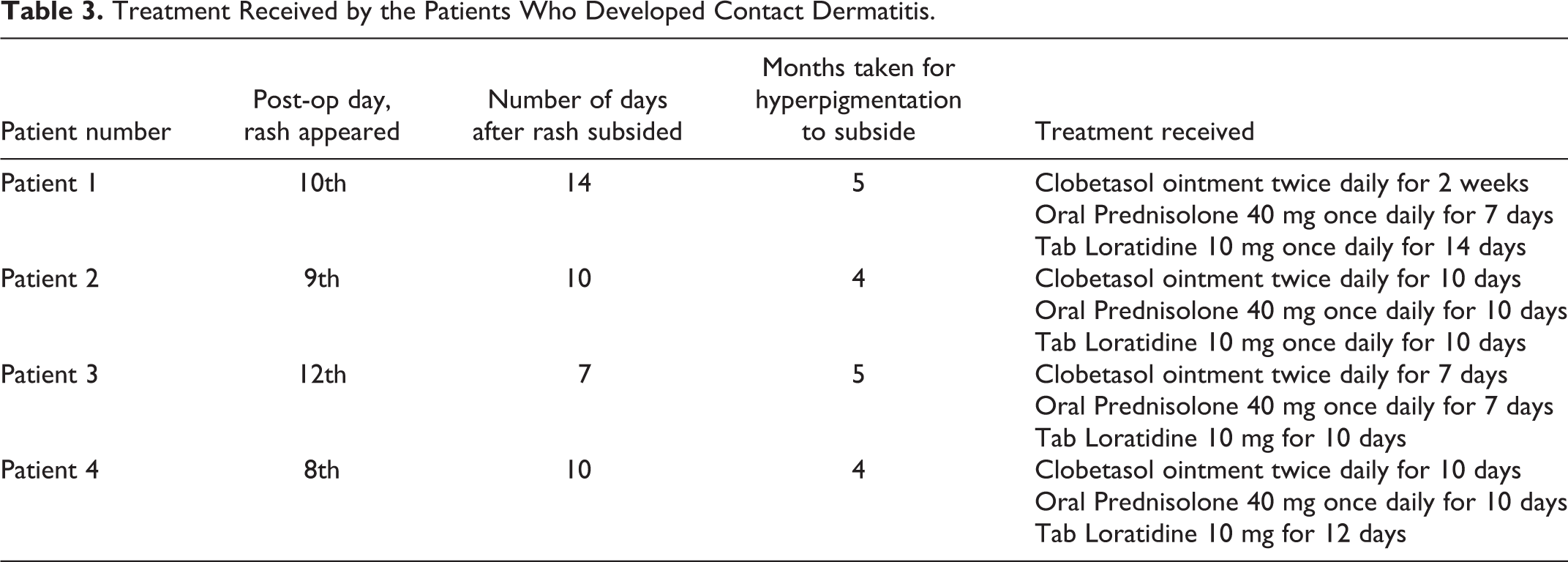
The mean age of the patients was 38 years (range 28-65 years; Table 1). Out of 60 operated patients, 4 (6.6%) had developed type IV hypersensitivity reaction and presented with typical contact dermatitis features including erythema, pruritic rash, and skin inflammation around the suture line. Their characteristics have been presented in Table 2. All of these 4 patients had developed signs and symptoms of allergic contact dermatitis in their second post-operative week. Out of these 4 patients, only 1 patient had history of exposure to Dermabond in the past. The contact dermatitis was treated by oral and local application of steroids and oral anti-histaminic medication. Acute symptoms like erythema and itching subsided on an average within 2 weeks of the treatment. However, post inflammatory hyperpigmentation took around 3 to 6 months to subside.
Characteristics of Patients Who Developed Contact Dermatitis.

Cases
Patient 1
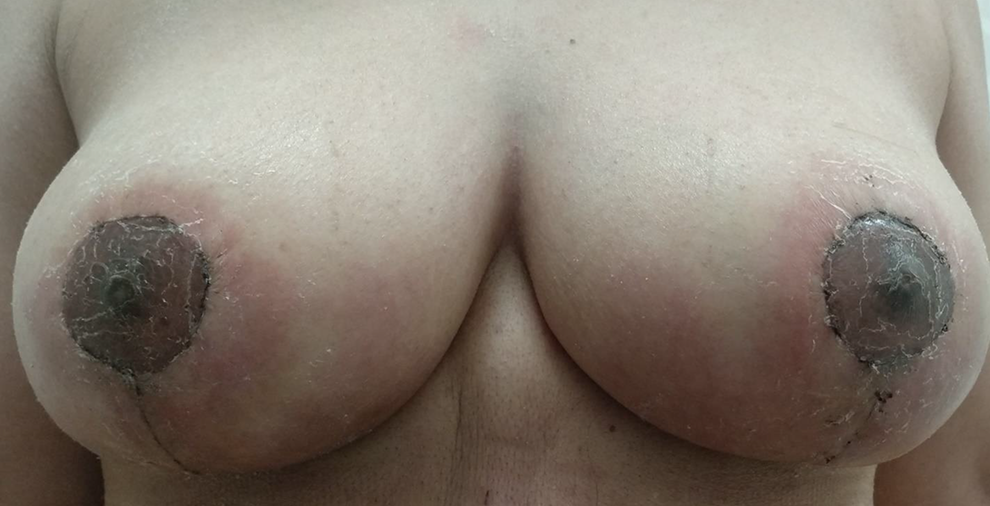
A 35-year-old female with no known history of any allergy underwent reduction mammoplasty. The patient reported to emergency department with complaint of erythema and itching over the suture line and adjacent skin (Figure 1; Table 3).

Allergic contact dermatitis to Dermabond with its demarcation in reduction mammoplasty patient.
Treatment Received by the Patients Who Developed Contact Dermatitis.
Patient 2
A 38-year-old woman with grade III breast ptosis underwent Mastopexy with Dermabond application on suture line at the end of surgery. The patient developed bilateral erythematous rash and itching around the suture line on ninth post-operative day (Figure 2; Table 3).
Erythematous rash around the suture line in patient of mastopexy.
Patient 3
A 40-year-old female with breast hypertrophy underwent reduction mammoplasty and had application of Dermabond over the suture line at the end of surgery. The patient developed bilateral rash and pruritus after 12th day of surgery around the suture line (Figure 3; Table 3).

Contact dermatitis post Dermabond application in reduction mammoplasty patient.
Patient 4
A 37–year-old female with no known positive allergic history in the past underwent Mastopexy for correction of breast ptosis, at the end of surgery Dermabond was applied over the suture line. The patient also had past history of Dermabond application over abdominoplasty suture line with no consequences. The patient presented on the 8th post-operative day with complaint of erythema and pruritus in both breasts around the suture line (Figure 4; Table 3).

Erythematous rash around suture line post application of Dermabond in mastopexy patient.
Discussion
Contact dermatitis is a type of eczema, which is triggered by the contact with a particular substance. There are mainly 2 types of contact Dermatitis: Irritant contact dermatitis and Allergic contact dermatitis. Irritant contact dermatitis is caused by a substance that directly damages the outer layer of skin, while as allergic contact dermatitis occurs when an allergen triggers cell mediated immune reaction to the skin and sometimes appears after the second and subsequent use of allergen. 15
In our this retrospective study, allergic contact dermatitis to the Dermabond (PRINEO by ETHICON) had developed in 4 out of the 60 patients who had Dermabond application over the suture line post breast surgical procedure. Therefore, total incidence of allergic contact dermatitis post application of the Dermabond was 6.6%. Due to this high incidence of allergic contact dermatitis, the Dermabond use was discontinued in our hospital and since then we had no new case of contact dermatitis.
Knackstedt et al in 2015 published a case series of 3 patients who had underwent reduction mammoplasty and developed contact dermatitis post application of Dermabond (PRINEO). 16 Chalmers et al in 2017 reported 0.5% incidence of contact dermatitis post application of Dermabond PRINEO in orthopaedic patients. 17 Michalowitz et al in 2020 compared Dermabond PRINEO with Exofin fusion and observed higher rates of Cellulitis in Dermabond cases. 18
We suppose that the body gets exposed to antigen (2-octyl cyanoacrylate) through small gaps in breast suture lines especially at the junctional points which are most liable sites for developing some wound gaps, 13 this in turn leads to sensitization of the body to Dermabond and subsequent development of type IV hypersensitivity reaction. In this study, we found out of the 4 cases who developed contact dermatitis, 3 developed it after their first contact with Dermabond, while as fourth case had past history of exposure to Dermabond in previous surgical procedure and in that patient we presume sensitization to Dermabond might had developed on its first application. In patients who developed contact dermatitis on first exposure to Dermabond, we presume the initial sensitization due to immunological cross-reaction that exists between 2-octyl cyanoacrylate and other acrylates, 12,19,20 found in many cosmetic products like acrylic nails, gel nails, and cosmetic glues used for eyelash extensions.
The time for development of pruritic skin rash varies from few hours to 3 weeks after contact with the allergen. 8,9,11,12 Therefore, a patient needs to be observed closely on post-operative follow-up for any signs and symptoms of allergic contact dermatitis. Dermabond is difficult to peel off once it dries up, which in turn leads to longer exposure of the wound to the antigen, therefore severe contact dermatitis is often seen in such cases that mostly needs treatment with systemic steroids. 12 Risk for development of contact dermatitis after application of Dermabond is significant and its possibility should be informed to the patient beforehand.
This study has limitations of being retrospective study and having no control group, hence further large sample study is recommended in the future.
Conclusions
There is a significant risk of developing type IV hypersensitivity reaction (allergic contact dermatitis) post application of Dermabond over the suture lines. Hence it is recommended that the patients should be well-informed and consented for possibility of such post-operative complication prior to any application of the Dermabond.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Deanship of Scientific Research (Princess Nourah Bint Abdulrahman University).