
Abstract
Introduction
Primary breast augmentation is one of the most frequently performed aesthetic surgery operations worldwide. The overall rare complications can be divided into early and late complications with regard to their focus. Hematomas, seromas, and infections are early complications. In the further course, late seromas, double capsules, or capsule contracture can cause symptoms that require an operative revision.1–3 In case of capsular contracture, the indication for revision surgery is usually given from Baker stages III/IV, whereby the incidence for capsular fibrosis of this degree is stated between 3.6% and 10.8%4,5 after 10 years. The development of capsular contracture is subject to a multifactorial process that is influenced by numerous risk factors such as the implant, position, patient age,6–9 or peri- and postoperative complications (eg seroma, hematoma, infection).10,11 Overall, fibrosis, including capsular fibrosis, is characterized by a largely nonspecific tissue reaction in which activated fibroblasts increasingly produce interstitial connective tissue, which results in scarred changes that can lead to impairment or loss of organ function in the advanced stage.12,13 The pathogenesis of capsular fibrosis is similar to that of other fibroproliferative diseases (eg keloids, hypertrophic scars, systemic sclerosis, etc.).14,15 Fibrotic processes are controlled by secretory signaling proteins from the transforming growth factor beta (TGF-β_ superfamily and[ 16 ] the inhibin-activin-follistatin axis. 17 The dimeric protein Activin A and its inhibitor follistatin play a particularly important role. Activin A is a key regulator of multiple biological pathways.[ 18 ] It is formed in inflammatory macrophages and acts synergistically with TGF-β in differentiation of fibroblasts into myofibroblasts and the stimulation of collagen genes.19–21 If Activin A is produced as part of an inflammatory response, it has a profibrotic effect.18,22,23 The naturally produced glycoprotein follistatin binds to Activin A with high affinity, blocking activin receptor binding and neutralizing activin action.[ 18 ] A mismatch between Activin A and its inhibitor follistatin is associated with pathological fibrotic processes.[ 24 ] It can therefore be assumed that, in synergy with TGF-β, pathological collagen synthesis in the development of capsular fibrosis is also subject to an activin-induced pathway. This assumption is confirmed in the animal experiments with regard to capsular fibrosis as a pathological fibrotic process, where it could be demonstrated that the local application of follistatin in the implant pocket led to a significant reduction in pericapsular inflammation and fibrosis. 25 The aim of this study was to determine whether and how the serum concentrations of Activin A and follistatin changes after breast augmentation with silicone implants. This is intended to provide insights into the possible influence of the activin-follistatin axis in the development of the capsular contracture.
Materials and Methods
Patients and Groups
We state that all procedures conformed to the Declaration of Helsinki. This study was approved by the Ethics Committee of the appropriate authority (Landesärztekammer Nord-Württemberg, Germany) and informed written consent to publish personal and medical information was obtained from all patients.
From July 2015 to January 2019, all patients who agreed to participate in the study and came for control examination after primary breast augmentation or for revision operation because of capsular fibrosis were included. Blood samples were taken to determine the serum concentration levels of Activin A and follistatin and patients were separated in several groups.
The standard values for Activin A and follistatin were determined on the basis of blood samples from women before primary aesthetic breast enlargement occurred (control group).
During longitudinal observation, a small amount of these control group patients (n = 16) developed a capsular fibrosis within 2 years after primary breast augmentation, which is why these samples were examined in a separate group (short-term-positive group/STpos), retrospectively.
For capsular fibrosis-positive group (CFpos), blood samples were taken after diagnosis of Baker ° ≥III capsular fibrosis, which leads in an operation (capsulotomy or capsulectomy with implant change or removal).
The last group included all patients who had undergone primary breast augmentation and who showed an asymptomatic course with regard to the development of capsular fibrosis. From these patients all were isolated, in whom the primary breast enlargement was more than 10 years ago, (long-term-negative group/LTneg). Data were collected for patient age, implant type, position and size, and—if available—capsular fibrosis classified according to Baker.
Serum Cytokine Analysis and Immunoassays
Blood samples were collected from all patients. After clotting, the samples were centrifuged at 3200 rpm for 30 min, and the serum was isolated and stored at −80 °C for analysis. Activin A (RAB0324, Sigma-Aldrich, Taufkirchen, Germany) and follistatin (RAB0191, Sigma-Aldrich, Taufkirchen, Germany) were measured using a specific ELISA according to the manufacturer’s instructions.
Statistical Analysis
Results are expressed as mean ± SD. Data analysis was performed using a Mann–Whitney U test with significance assigned at p ≤ 0.05 (*).
Results
A total of 361 female patients (n = 361) were included in this study and blood samples were taken.
Of these, 167 had no implants at the time the first blood sample was taken. They were used to define the standard serum levels as control group (n = 167).
During longitudinal observation, 16 of these patients became positive for capsular fibrosis symptoms Baker ≥°III within 2 years after primary breast augmentation. They were considered separately in a short-term-Positive group/STpos (n = 16).
Eighty patients, who developed a capsular fibrosis Baker ≥°III and underwent revision surgery were collected in a capsular fibrosis-positive group/CFpos (n = 80).
One-hundred and fourteen patients asymptomatic for capsular fibrosis Baker ≥°III after primary breast augmentation were collected (n = 114). Thirty three of them were negative for capsular fibrosis symptoms even after more than 10 years. They were collected in a long-term-negative group/LTneg (n = 33).
Table 1 shows information about implants, surfaces, and implant pockets of each group.
Illustration of the different groups: Short-term-positive (STpos), capsular fibrosis-positive (CFpos), and long-term-negative (LTneg) concerning the used implants.
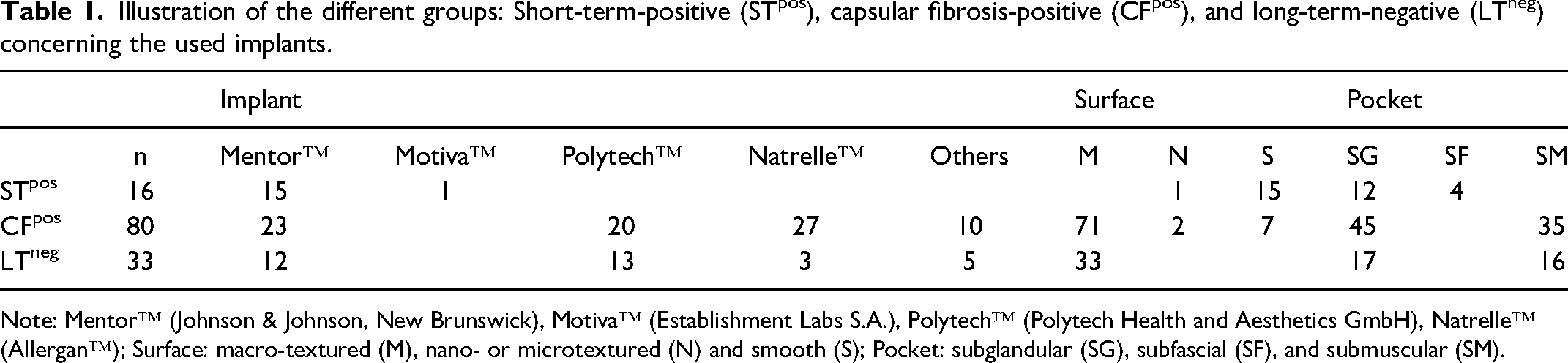
Note: Mentor™ (Johnson & Johnson, New Brunswick), Motiva™ (Establishment Labs S.A.), Polytech™ (Polytech Health and Aesthetics GmbH), Natrelle™ (Allergan™); Surface: macro-textured (M), nano- or microtextured (N) and smooth (S); Pocket: subglandular (SG), subfascial (SF), and submuscular (SM).
In STpos, most patients with smooth implants in a subglandular pocket developed capsular fibrosis.
Independent of the implant manufacturer in CFpos group, capsular fibrosis mostly occurred in patients with macrotextured implants in a subglandular pocket.
The patients in the LTneg group all had textured implants with an equal distribution on the subglandular and submuscular pocket.
The mean implant sizes were 345 mL (range: 275-450 mL) in STpos, 330 mL (range: 230-600 mL) in CFpos and 300 mL (range: 225-500 mL) in LTneg.
Mean age at surgery was 38 years (range: 18-60 years). Mean age of control group was 31 (range: 22-53 years), of capsular fibrosis group (CFpos) 31 (range: 22-53 years), and long-term group (LTneg) 44 (range: 28-62 years). There was no statistical difference among the groups (p > 0.05).
Serum Cytokines
From 167 patients, the blood samples were taken before their primary aesthetic breast augmentation. Their Activin A and follistatin values defined the standard serum levels of the control group (Activin A: 0.96 ± 0.15 ng/mL; follistatin: 8.42 ± 0.53 ng/mL).
Serum Activin A levels (Figure 1) of long-term group (1.55 ± 0.04 ng/mL) were significantly higher compared with those in the capsular fibrosis group (0.96 ± 0.05 ng/mL; p = 0.039) and to the control group (0.96 ± 0.15 ng/mL; p = 0.033).
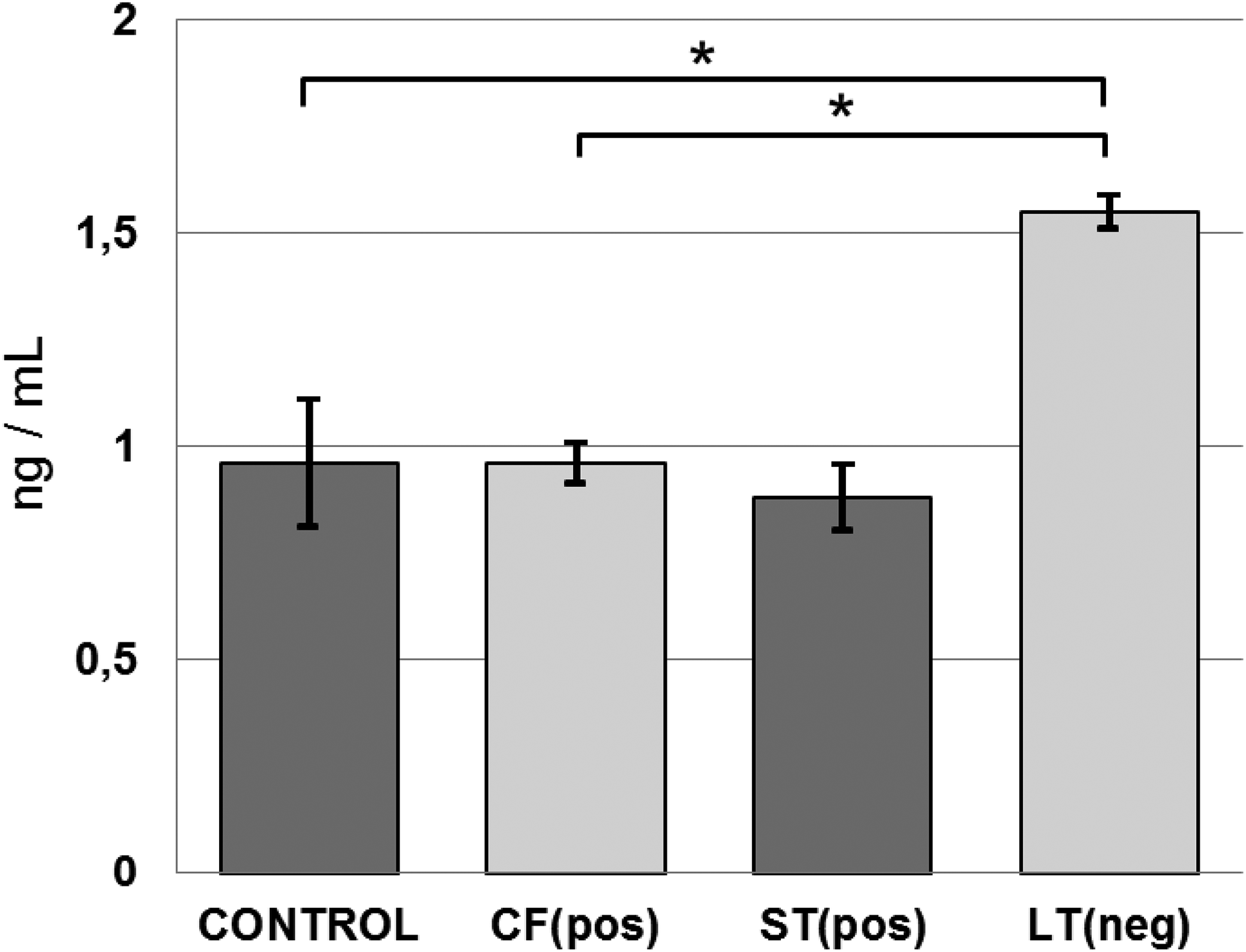
Activin A: Serum concentrations were significantly higher in the long-term group (LTneg) compared to the control group (control) and the capsular fibrosis group (CFpos). There were no statistical significant differences in serum concentrations between control, CFpos, and STpos.
Activin A levels of patients who developed capsular fibrosis during longitudinal observation within 2 years after primary breast augmentation showed no significant different Activin A levels before (0.81 ± 0.07 ng/mL) and after (0.88 ± 0.08 ng/mL) surgery compared to the standard serum level (0.96 ± 0.15 ng/mL).
In comparison, follistatin levels (Figure 2
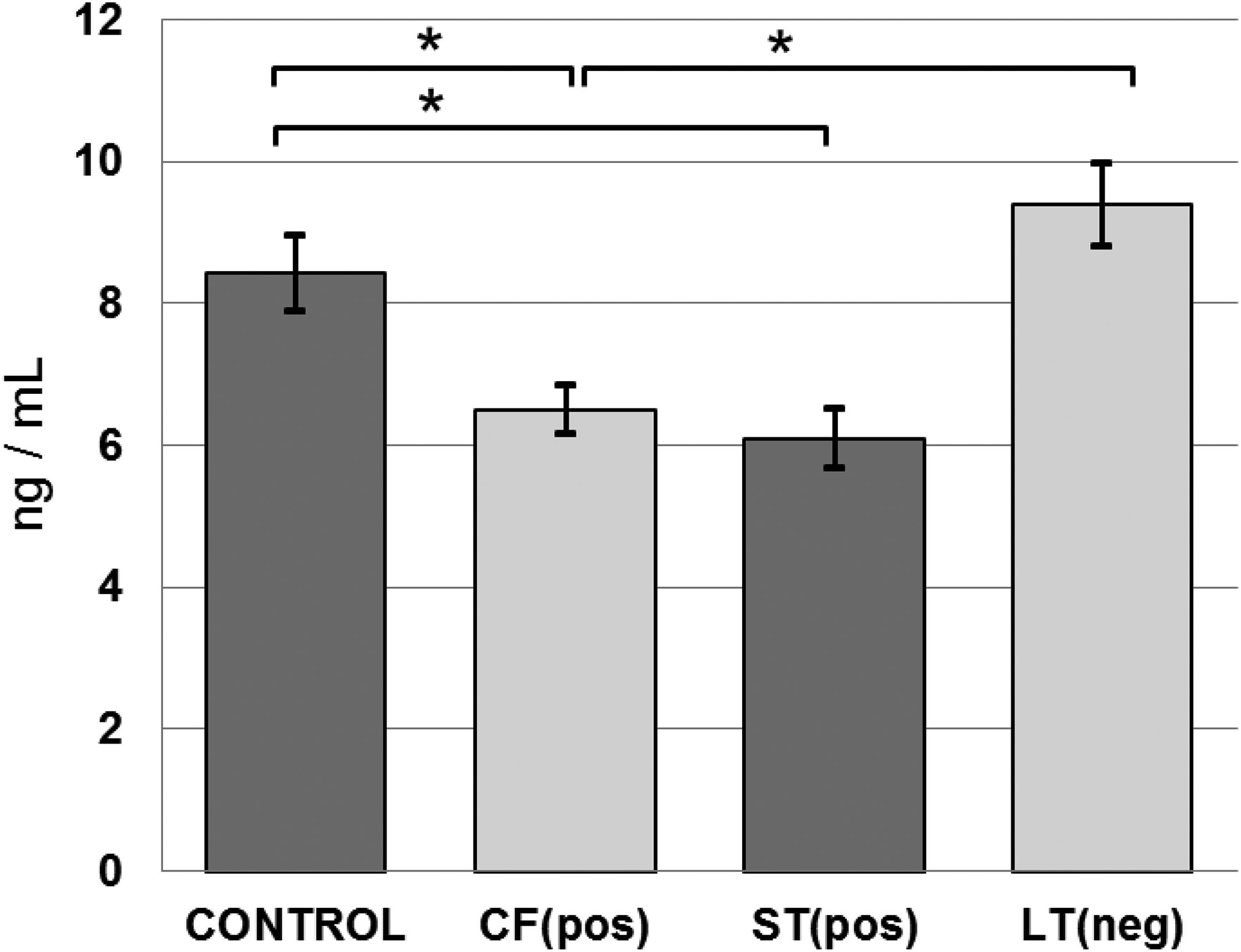
Follistatin: Serum concentrations of control group and long-term group were significantly higher than in the capsular fibrosis group. Serum concentration of patients who developed capsular fibrosis within 2 years after primary breast augmentation was significantly lower both before and after (STpos) surgery compared to the baseline data group.
Follistatin levels of long-term group (9.38 ± 0.59 ng/mL) showed no statistical relevant deviations (p > 0.05) compared to the control group (8.42 ± 0.53 ng/mL).
The follistatin levels of patients who developed capsular fibrosis during longitudinal observation within 2 years after primary breast augmentation were both before (5.57 ± 0.34 ng/mL) and after (STpos: 6.09 ± 0.41 ng/mL) the operation statistically relevant (p < 0.05) below the serum level (8.42 ± 0.53 ng/mL) of the control group.
Discussion
One of the most common reasons for revision surgery after breast augmentation is capsular contracture. In the development process of collagen formation and deposition, the cytokine TGF-β plays a decisive role. High levels of TGF-β occur in many fibrotic diseases.14,26–30 Activins belong to the TGF-β family of multifunctional cytokines. 31 TGF-β and Activin A have synergistic effects. 18 It is known that in keloid fibroblasts with an increased expression of the TGF-β receptors 32 and an increased TGF-β auto production, there is a massive increase in Activin A, but not its inhibitor follistatin. 33 In hypertrophic and burn scar-derived fibroblasts, an increased collagen synthesis induced by Activin A could also be demonstrated. However, simultaneous detection of changed serum Activin A/follistatin levels has not yet been demonstrated here. 24 Comparable results with regard to capsular fibrosis have so far not been obtained either by influencing components of the inhibin-activin-follistatin axis or by changes in the Activin A/follistatin serum levels in the run up to or when the disease occurred. Our data now show that serum concentration levels of Activin A and follistatin in patients with capsular contracture differ from the standard serum level determined by us and the values that occur in long-term patients asymptomatic with regard to capsular contracture.34,35
Contrary to Dohi et al. and Frenkiel et al.25,36, we could not observe that higher follistatin concentrations were also associated with higher Activin A concentrations. We observed normal Activin A serum levels and below standard follistatin levels in capsular fibrosis patients.
Excessive inflammation leading to excess collagen deposition is widely postulated as an important cause of capsular fibrosis. If inflammation can be controlled, capsular fibrosis rates can be reduced. Our research group modulated the effects of the inflammatory pathways to reduce fibrosis using Halofuginone, Phosphoyrylcholine, and Spider Silk. Although these studies were all animal studies, they prove the connection between inflammation and fibrosis and the ability to influence capsule formation by interfering with the signaling pathways and improving biocompatibility.37–41
Our study does not investigate and differentiate the possible causes of capsular fibrosis. Only the occurrence of such and the effects on the serum concentrations of Activin A and follistatin are assessed. This means that no conclusions can be drawn about the implant, its position, surface, or other influencing factors.
The comparison of our observations with other studies can only be made relatively with regard to the specific serum concentrations, since the variance of the serum concentrations given in the literature is not only stated very differently, but is also subject to different factors such as the menstrual cycle, pregnancy, or certain comorbidities.34,42–47
None of our patients were pregnant or had relevant concomitant diseases such as hyperthyroidism, liver cirrhosis, or chronic renal failure.
Changes during menstrual cycle are insignificant in relation to our observations, especially since they can only be observed with Activin A, but not with follistatin. 42
For Activin A and follistatin, it was observed that serum concentrations increase with age.43,45 The increase in mean serum concentrations observed by us in the long-term group without capsular fibrosis, which was on average about 10 years older than control group, could also be due to older age.
Since Activin A is also seen as a diagnostic marker of an acute inflammatory reaction (sepsis),23,48,49 a corresponding increase would not be expected in case of an existing capsular fibrosis. In the group of patients who developed capsular fibrosis within 2 years after the procedure, the concentration of Activin A did not differ from control group serum levels, but the follistatin serum concentration was significantly lower even before the procedure.
Conclusion
We found that Activin A serum levels in patients with and without capsular fibrosis are not subject to fluctuations. At most, they are subject to age-related changes.
In contrast, follistatin serum levels of patients with capsular fibrosis are below standard circulating levels. We also observed that in patients who developed capsular fibrosis within 2 years after breast enlargement, the follistatin serum levels were below standard serum level even before the procedure. These results show that besides many other factors, a dysregulation of the activin-follistatin axis may have importance on the pathogenesis of capsular contracture.
Footnotes
Acknowledgments
The author is grateful to Manuela Hofmann, Experimental Visceral Surgery; Department of General, Visceral, Transplantation, Vascular and Pediatric Surgery (Department of Surgery I); University Hospital Würzburg/Germany, for her skillful technical assistance with the ELISA experiments. Furthermore, the author thanks Prof. Dr. Christoph Otto (University Hospital Würzburg, Department of Surgery I) for providing a good environment and facilities to complete this project, helpful discussions, and for editing this publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.