
Abstract
Introduction
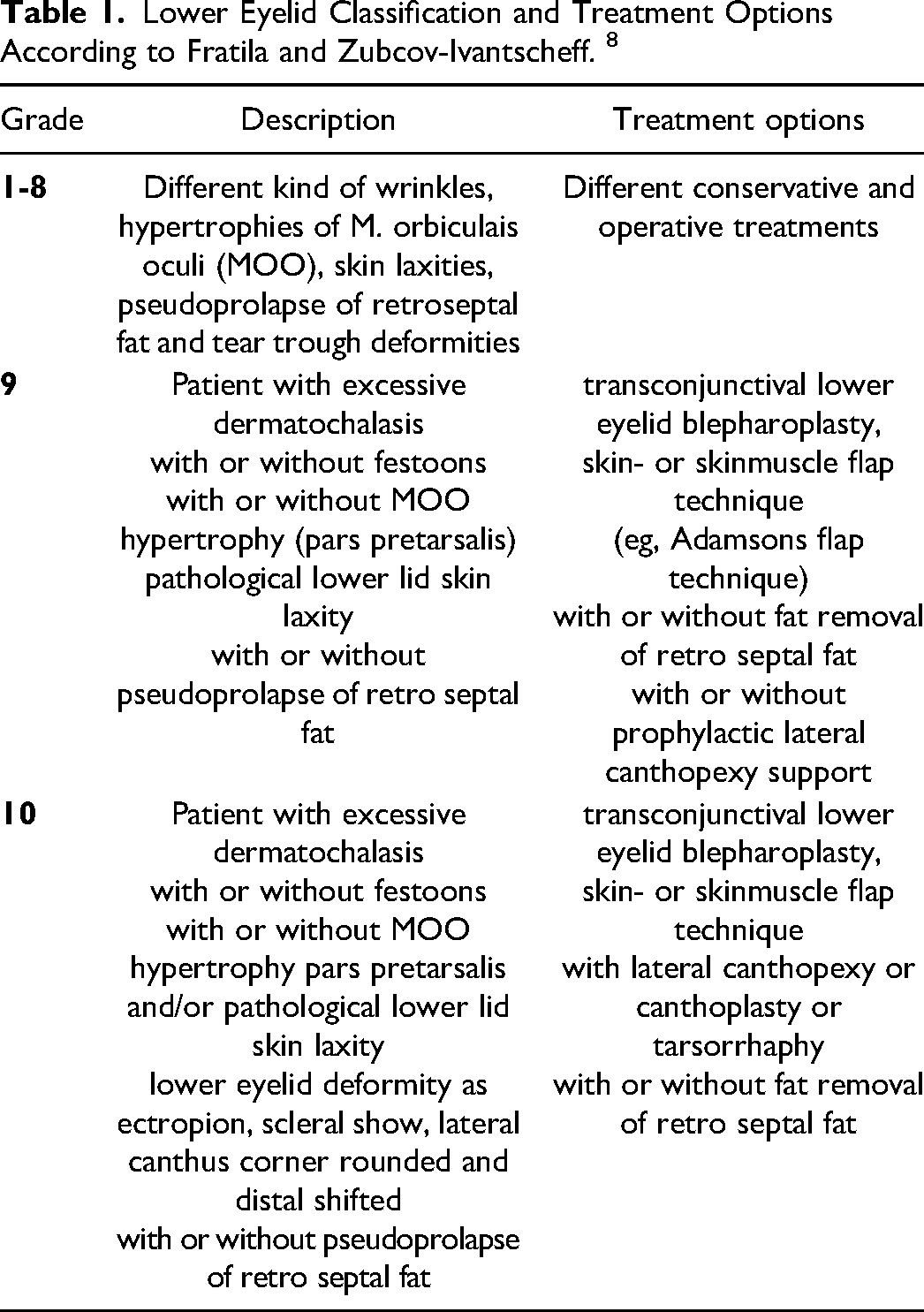
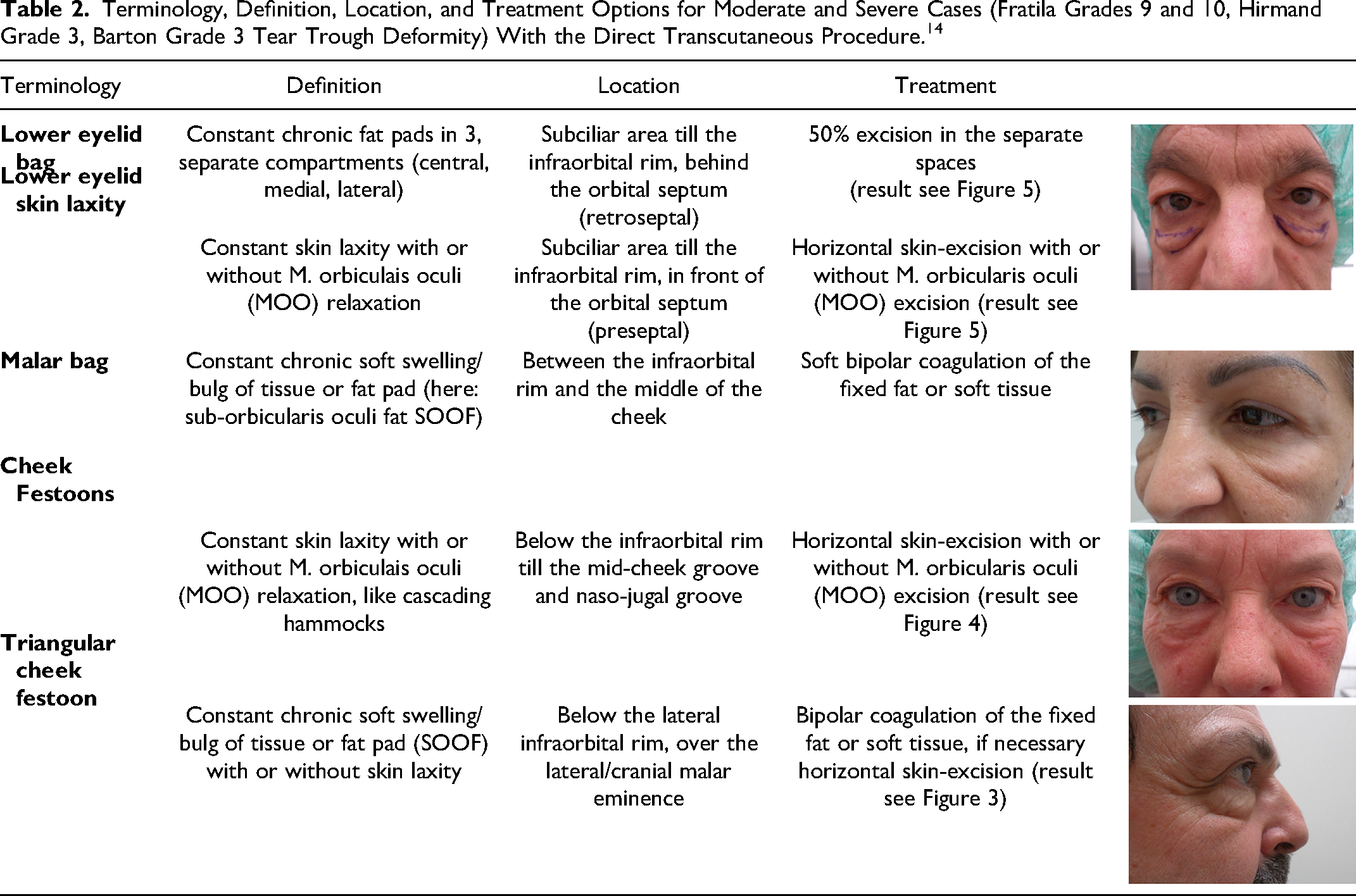
Operative treatments for distinct lower eyelid skin laxity accompanied by prolapsed orbital fat with hollowing of the tear trough, suborbicularis oculi fat (SOOF), and triangular cheek festoons (often found on sun-damaged skin) are complex.1–7 For lower eyelid deformities with Fratila grades 9 and 10 8 (Table 1) or Hirmand grade 3,9,10 transconjunctival fat removal or repositioning and subciliary skin resection in combination with lateral canthopexy support are the established procedures.6,11–13 Furthermore, an additional laser resurfacing technique allows patients to achieve the specific goal of better skin quality. 3 These procedures usually require local anesthesia in combination with intravenous sedation or general anesthesia. The advantages of these techniques are nearly invisible scars, an intact infraorbital septum, and preservation of the orbicularis oculi muscle (MOO). The disadvantages are possible complications such as ectropion, asymmetry, and undesired changes in the eyelid shape or poor cosmetic results; however, these are mainly dependent on preoperative clinical examination results and the experience of the surgeon. 13 Accessing and correcting pronounced tear trough deformities, SOOF laxity, and festoons can be difficult with the established techniques, however (Table 2).
Lower Eyelid Classification and Treatment Options According to Fratila and Zubcov-Ivantscheff. 8
Terminology, Definition, Location, and Treatment Options for Moderate and Severe Cases (Fratila Grades 9 and 10, Hirmand Grade 3, Barton Grade 3 Tear Trough Deformity) With the Direct Transcutaneous Procedure. 14
Other possible operative techniques include pinch blepharoplasty (subciliary) of the lower eyelid 15 or direct excision of the lower eyelid at the infraorbital rim to remove skin laxity and pigmentation.16–18 Direct excision of the infraorbital rim is advantageous because it is an easy, safe, and controllable procedure with low complication rates. However, its disadvantages include a potentially visible scar, muscle/nerve injury of the MOO, and infraorbital septum trauma.
Some patients, such as those with a history of smoking, high-grade deformities, and revision blepharoplasty, often decline complex procedures because of the fear of complications. Therefore, we used direct transcutaneous blepharoplasty via the orbital rim of the lower eyelid under local anesthesia to correct tear trough deformities, fat prolapse of the SOOF, and festoons.
Materials and Methods
All procedures performed during this study conformed to the Declaration of Helsinki. This study was approved by the Ethics Committee of the appropriate authority. Additional informed consent was obtained from all participants for whom identifying information is included in this article.
Patient Selection
Before planning the surgical procedure, a precise patient evaluation was performed. The physical examination focused on the quality and amount of periocular skin, orbital fat prolapse, the presence of a tear trough deformity, inferior scleral show, horizontal lid laxity, canthal tendon laxity, cheek projection, and festoons. 19
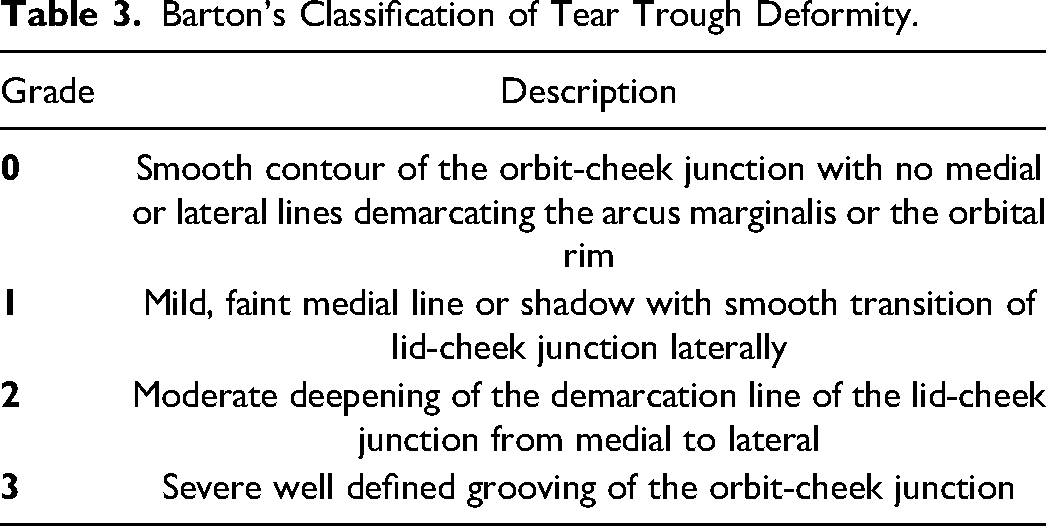
Patients with Fratila grades 9 and 10, Hirmand grade 3, and Barton grade 3 tear trough deformity (Table 3) were included and underwent lower eyelid blepharoplasty. From January 2010 to December 2018, a total of 21 patients underwent direct transcutaneous lower eyelid blepharoplasty via an infraorbital incision under local anesthesia. Patients whose primary concern was massive skin laxity, fat depot prolapse of the lower eyelid fad pads, SOOF, hypertrophy of the MOO, festoons, and hyperpigmented periorbital skin were included.
Barton's Classification of Tear Trough Deformity.
Informed consent was provided to ensure that each patient understood the exact procedure and the resulting scars at the infraorbital region after direct infraorbital lower blepharoplasty.
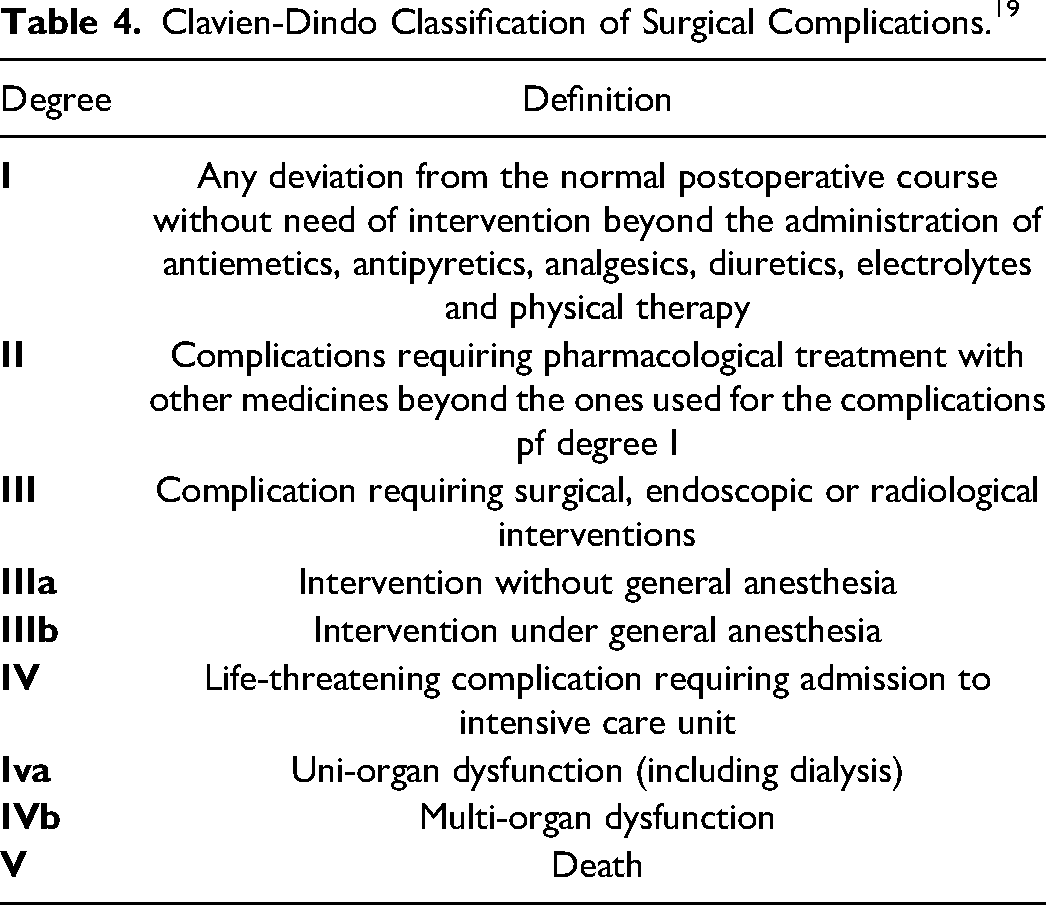
A retrospective chart review was performed to obtain data regarding patient age, comorbidities, smoking history, and lower eyelid surgery history. Complications were documented and graded using the Clavien-Dindo classification for surgical complications 20 (Table 4). The cohort included 13 women and 8 men. All surgeries were performed by the same surgeon (U.E.Z.).
Clavien-Dindo Classification of Surgical Complications. 19
Surgical Technique
Preoperative skin markings were created with the patient in the sitting posture before local anesthetic solution injection. The expected scar (of the skin tension lines) was designed as a horizontal/elliptical formation between the sulcus palpebralis inferior and sulcus palpebromalaris. Maximum mouth-opening and upward gazing were necessary to limit the maximum skin resection by pinching with anatomic forceps. The fat compartments (lateral, medial, central) and triangular cheek festoons were marked (if present) (Figure 1). Surgery was performed with the patient in an elevated (30°) lying position. All patients were administered a transcutaneous local anesthesia injection (total on both sides: 20 mL mepivacaine 1% with additional epinephrine 1:1 000 000). For 8 patients, additional intravenous sedation with midazolam (5-7 mg) was applied. All 3 retroseptal fat bags were injected separately (∼1-2 mL in each pocket). Surgeries were performed in an outpatient setting.
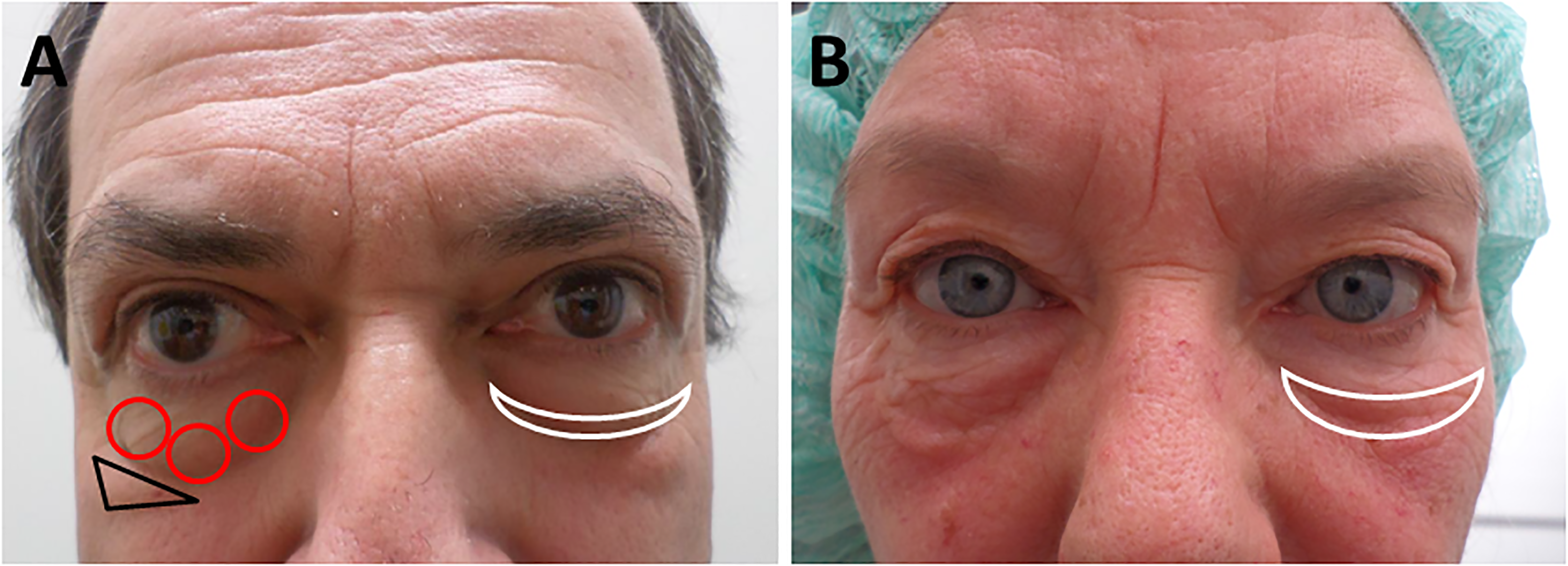
(A) Preoperative markings showing the lateral, medial, and central suborbicularis oculi fat (SOOF), retroseptal fat pad (red), triangular cheek festoon (black), and crescent-shape or elliptical markings for skin excision above the infraorbital rim to address lower eyelid skin laxity (white). (B) The skin area was marked to address skin excision above and below the infraorbital rim in the case of skin relaxation in this area.
There are 2 different ways of creating the surgical design around the infraorbital rim. These are dependent on the position of the relaxed skin. Patients with skin relaxation above the infraorbital rim only require a crescent-shape or elliptical skin excision in this area (Figure 1A). However, patients with skin relaxation above and below the infraorbital rim also require skin excision above and below the infraorbital rim to obtain correct and esthetic results (Figure 1B).
After complete excision of the skin, the underlying MOO fraction was excised if indicated. Then, the orbital septum was addressed and horizontally incised and the protruding fat pads were removed or repositioned (Figure 2A and D). It is recommended that all 3 (lateral, medial, and central) fat spaces should be opened separately and the fat pads should be allowed to prolapse. Then, only half of the prolapsed fat has to be excised (if indicated) under coagulation to avoid a hollow appearance. To treat the triangular cheek festoons, we performed soft bipolar coagulation of the fixed fat under and above the MOO with or without resection of the skin. Sutures of the orbital septum were consciously refrained. Running sutures (nonabsorbable suture material, 5-0) were applied to only the skin. Strips were applied over the sutures and proximal maxilla area. Cooling pads were applied over moist gauze. Patients were monitored for at least 30 min postoperatively to exclude bleeding and other complications. The suture material was removed after 8 days. Further postoperative examinations were performed 14 days, 3 months, and 6 months postoperatively.
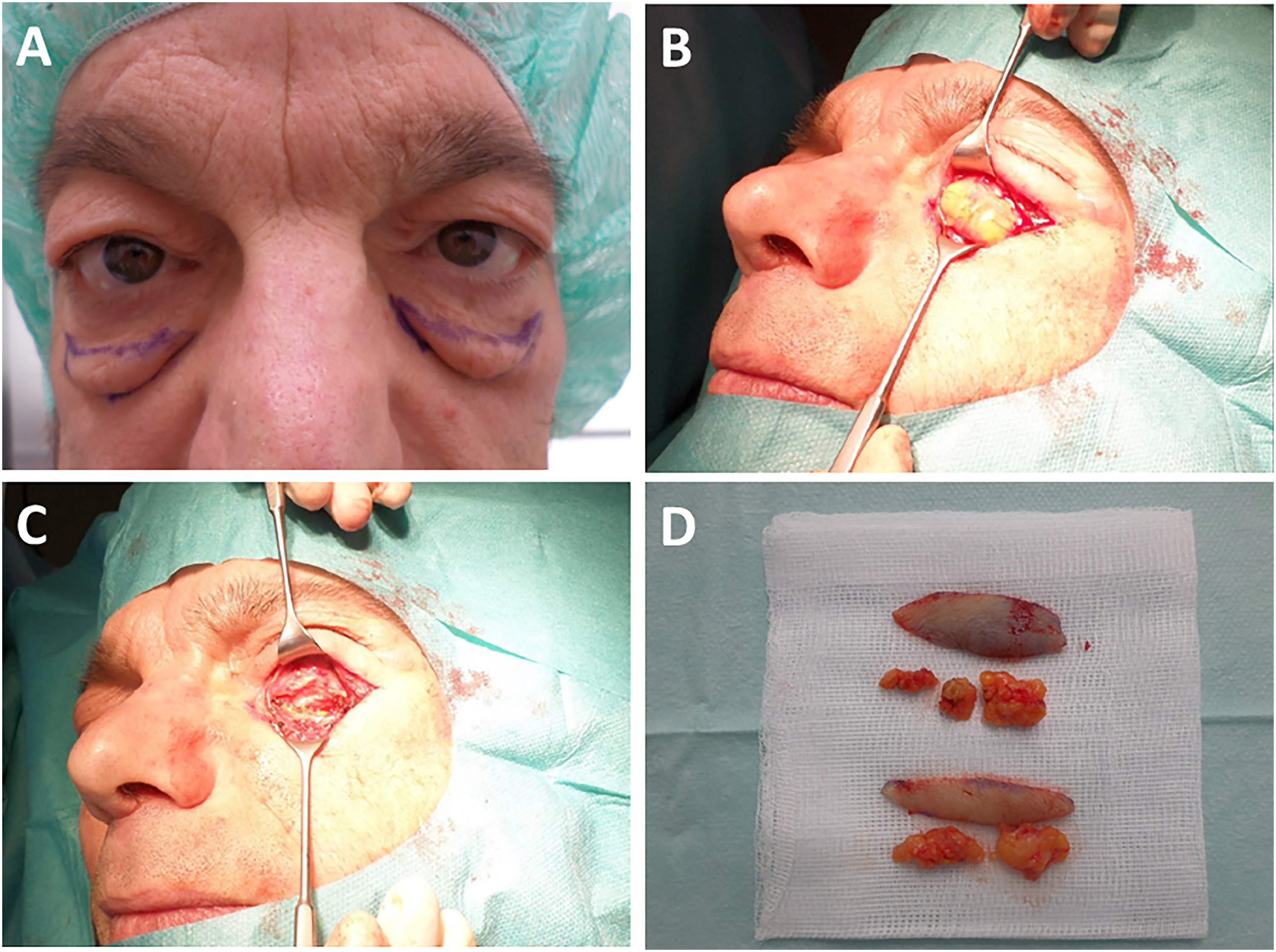
Preoperative markings (A) and intraoperative findings after the orbital septum was addressed and horizontally incised. The fat pad is shown before (B) and after (C, D) excision.
Results
A total of 21 patients were included in this study. The mean age of the patients was 53.5 years (range: 42-79 years). Nine (43%) patients underwent lower blepharoplasty alone. The majority (n = 12; 57%) underwent additional upper eyelid blepharoplasty during the same procedure (Table 3). No patients required canthopexy. Two patients had undergone previous lower eyelid blepharoplasty. The average operative time for lower blepharoplasty was 27 min; however, the average operative time for the combination with upper blepharoplasty was 48 min.
For 18 patients (86%), prolapsed orbital fat and tear trough deformities were treated with retroseptal fat resection. Only one of those patients had hypertrophy of the central fat compartment, 6 had hypertrophy of the central and medial fat compartments, and 11 had hypertrophy of the lateral, central, and medial fat compartments. Five patients presented with a triangular cheek festoon. The postoperative Barton classifications were grade 0 for 20 (95.2%) patients and grade 1 for 1 (4.8%) patient. There was no significant difference between the male and female patients (Figures 3 to 5).
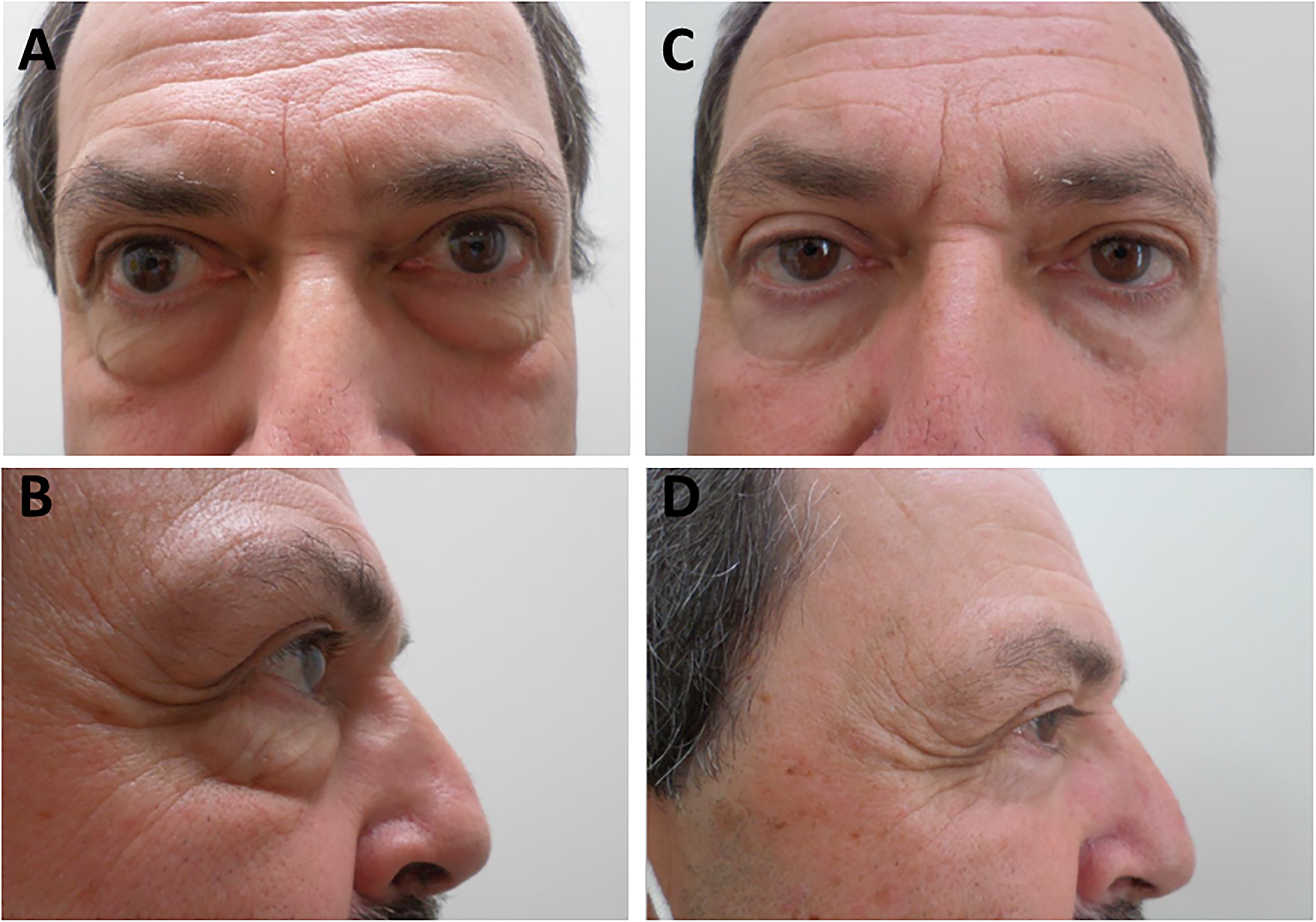
Frontal and side views of the patient from Figure 1A before (A, B) and after (C, D) direct transcutaneous lower blepharoplasty.

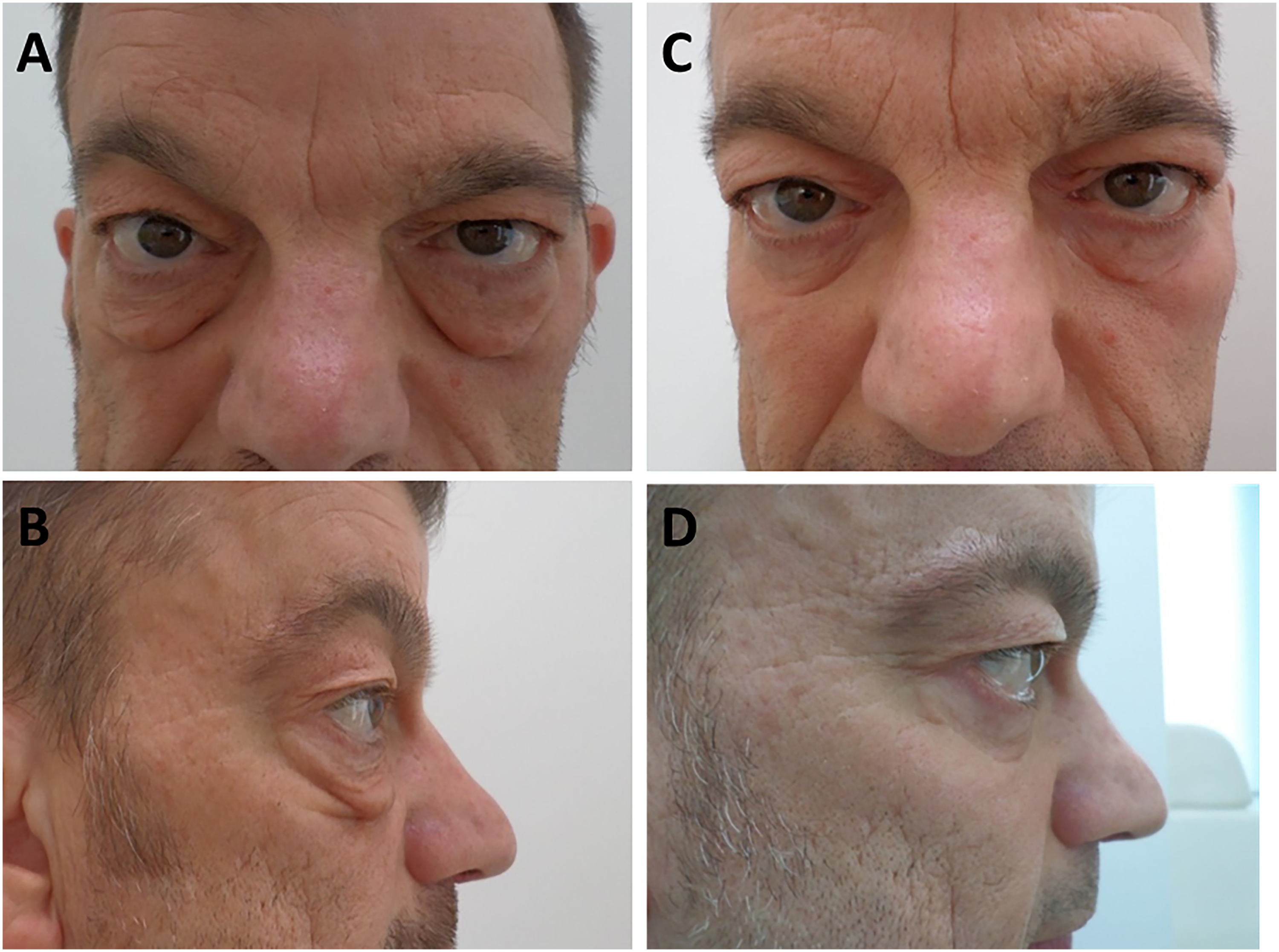
Frontal and side views of the patient from Figure 1B before (A, B) and after (C, D) direct transcutaneous lower blepharoplasty.
Frontal and side views of the patient from Figure 2 before (A, B) and after (C, D) direct transcutaneous lower blepharoplasty.
The pinch test (forward distraction test) times were 1.0 s for 12 patients and 1.5 s for 9 patients. The lid snap-back test times were 3.0 s for 19 patients and 4.0 s for 2 patients.
Regarding smoking, 11 (52.4%) patients were current smokers, 6 (28.6%) patients were nonsmokers, and 4 (19.0%) patients were previous smokers. The mean nicotine use of the current smoker group was 14.2 cigarettes per day for more than 30 years. The previous smoking group had smoked cigarettes for 8 to 25 years (mean: 21.50 years) and quit smoking 7 to 20 years previously. One male patient presented with wound dehiscence after direct eye trauma 10 days postoperatively that required surgical revision and scar correction 5 months postoperatively. Another male patient required surgical refinement of the left lateral lower eyelid because of persistent skin laxity and redundancy. Both patients had Clavien-Dindo type IIIa complications. No postoperative ectropion was observed 1 year after surgery.
Discussion
Operative treatments performed for lower eyelid deformities are challenging and require the surgeon to have vast expertise. This is because of the complex anatomy and different changes that occur during aging of the periorbital region and midface.1,2,4–7,21 Genetic dispositions, facial expressions, and damaging toxins (eg, sun exposure and long-term history of smoking) lead to different imperfections of the lower eyelid of patients older than 50 years. 12 The correction of tired, damaged, and aged appearances is desired by patients. Naik et al 22 described deformities as “hills and valleys.” Hills are formed by the orbicularis roll, the prolapse or pseudoprolapse of orbital fat (fat bags), and triangular malar mounds. Valleys are forged in the cheek descent by hollow tear trough depression at the orbital rim, eyelid creases, and the zygomatic hollow. Additionally, we noticed different skin transparencies, loss of skin elasticity, and hyperpigmentation mainly with sun-damaged skin. An accurate preoperative examination and description of the deformities are necessary to ensure that therapy is tailored to each individual patient.
The preoperative classifications of lower eyelid deformities have been described by Hirmand et al 9 and Fratila et al. 8 Furthermore, postoperative changes have been rated by Barton et al. 23 With lower-grade eyelid deformities, botulinum toxin-A treatments with or without additional ablative laser skin resurfacing and fillers, such as hyaluronic acid, are used. Higher-grade deformities can be treated with lipofilling or hyaluronic acid and transconjunctival operative procedures, including the removal or repositioning of fat pads. Subciliar lower eyelid blepharoplasty that removes excessive skin and releases the orbitomalar ligament can be necessary to correct the tear trough deformity.
In addition to the lifting and removing techniques for high-grade (Fratila grades 9 and 10, Hirmand grade 3) deformities, a skin or skin-muscle flap technique (Adamson's flap) with or without prophylactic lateral canthopexy support can be performed. Sometimes tarsorrhaphy is indicated. 23 As mentioned, the operative procedures for high-grade (Fratila grades 9 and 10 and Hirmand grade 3) deformities require the surgeon to have broad surgical expertise to avoid complications. These types of procedures are performed under sedation. The proper techniques ensure barely visible scars with the subciliary approach, avoid translamellar scarring, and allow for the preservation of innervation of the MOO as well as the orbital septum. 24 The disadvantages are high tension on the subciliary scar, which can lead to complications such as ectropion and rheumy eye. The corresponding elliptical resection of the skin is difficult to judge and can end in asymmetric results, especially if the MOO is injured during dissection. Furthermore, it could cause a change in the eyelid shape. Therefore, patients sometimes avoid high-risk surgery and request an easy and safe procedure under local anesthesia with acceptable end results to correct their problems.
Simple pinch blepharoplasty of the lower eyelid with a subciliary incision has been described for high-grade deformities.8,15–18 This type of procedure can be performed under local anesthesia; however, it is associated with high complication rates and is limited to small amounts of skin excision. Because it has absolutely no effect on orbicularis rolls in the lower part of the eyelid, the triangular malar mound of the infraorbital rim (tear trough), and festoons, its indications are limited.
For certain clinical and patient-specific problems, Bellinvia et al 17 and Glasgold et al 16 recommended direct transcutaneous lower eyelid blepharoplasty through an infraorbital incision. This technique leads to cosmetically and functionally superior results compared to those of traditional methods; however, they are controversial. Both authors described the procedure as advantageous for skin removal in cases of pigmented, poorly textured, and overlying skin because of its safety. Postoperative swelling and incisional erythema occur temporarily. The excellent outcomes of direct excision lower eyelid blepharoplasty described by Glasgold et al 16 (n = 22) and Bellinvia et al 17 (n = 55) were confirmed by our study. This procedure has been indicated for severely excessive skin and pigmentation. We found the technique to be useful for the treatment of tear trough deformities, SOOF laxity, and festoons. Our results show that direct excision is a safe, effective, and controllable method for these cases. We strictly avoided tension on the lower eye lid and canthus to minimize the risk of ectropion. Our results also showed that innervation or orbicularis muscle injuries in the infraorbital region did not influence the esthetic outcome. In the literature, higher rates of changes, deformities, and muscle denervation have been described after the performance of deep caudal incisions of the infraorbital rim.6,24 When the correct incision line is chosen and restricted resection is performed, scars are barely visible at the infraorbital rim. Patients are willing to accept the resulting scars because they are similar to fine wrinkles. With this technique, we can intraoperatively decide whether fad pads should be removed or repositioned.2,4,5,11,21,25 If festoons existed, then they were treated with bipolar coagulation underneath the orbicularis oculi because surgical removal of the fat pad leads to unpredictable inner scarring and unaesthetic outcomes. We believe that the indication is dependent on the fixed fat pad. Release of the orbitomalar ligaments was performed for our patients if necessary.
Skin closure, when performed without tension and avoiding scleral show, ensures the avoidance of ectropion during scarring. We do not combine the procedure with ablative laser therapy at our clinic because of the prolonged recovery time. Instead, we recommend ablative laser or chemical peeling treatments as a preparation before surgery.
The procedure was also indicated for lower eyelid blepharoplasty revision. During our retrospective study, 2 patients presented with a history of high-grade deformities and previous lower eyelid blepharoplasty (subciliary cut). They were treated successfully, safely, and satisfactorily with the direct incision infraorbital technique. Surgical refinement is easily possible under local anesthesia. During our study, one (7.8%) patient (out of 21 patients) who underwent surgical correction 5 month after the primary treatment experienced scarring problems. Postoperative bruising and erythema in the scar area are common caused by MOO resection and the opening of the orbital septum; however, they could be well-treated conservatively. To avoid extensive swelling, we taped the infraorbital and upper maxilla areas for 2 to 4 days. Both upper and infraorbital lower eyelid blepharoplasty were performed during the same procedure for 12 (57.1%) patients. No ectropion occurred and complete closure of the eyelids was possible for all patients. One of these patients requested surgical refinement of the lower and lateral left eyelids. Eleven (52.4%) of 21 patients were current smokers and 4 (19.0%) had a history of smoking; both groups had corresponding deformities and poor skin quality. No patients experienced any problems with wound healing, scarring problems, or ectropion; acceptable cosmetic results were achieved. None of the patients reported any postoperative problems. The scars were barely visible and all patients were satisfied with the final results. Therefore, infraorbital transcutaneous lower eyelid blepharoplasty could be performed for selected cases.
Conclusion
This study was performed in an outpatient setting to analyze the versatility of an orbital rim incision as a safe treatment approach to lower lid deformities. We found that orbital rim incision blepharoplasty can be performed under local anesthesia and is technically simple. Additionally, it allows for the adequate treatment of several lower lid deformities during one procedure. Furthermore, the technique is an excellent alternative to the established methods, especially for lower lid blepharoplasty revision and patients with a history of smoking. The orbital rim incision minimizes the risk of postoperative ectropium. Postoperative scars were inconspicuous and the patients were satisfied with the esthetic outcomes when properly prepared during the informed consent process. This method is safe for treating lower lid skin laxity, lower lid eyebags, festoons, and malar mounds through a single incision, results in good esthetic and functional outcomes, and is associated with low complication rates.
Footnotes
Acknowledgements
The authors would like to thank Julia Obermeyer MD DDS for her support.
Declaration of Conflicting Interests
The authors disclose any commercial associations or financial interests.
The authors declare no conflict of interest.
Helsinki Statement
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Informed Consent Statement
Informed consent was obtained from all individual participants included in the study. Additional informed consent was obtained from all individual participants for whom identifying information is included in this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.