
Abstract
Introduction
Breast hypertrophy is the excessive overgrowth of breast tissue with well-known physical and psychological consequences. Although conservative measures may be helpful for alleviating breast hypertrophy-related symptoms, reduction in mammoplasty remains the definitive treatment. Reduction mammoplasty is among the most performed plastic surgery procedures, but a relatively small percentage are performed on pediatric patients. 1 Adolescent breast hypertrophy is often idiopathic and is influenced by multiple factors, including hormonal imbalances and obesity. 2 Prior studies show that the majority of patients with breast hypertrophy fall within the overweight and obese body mass index (BMI) ranges,3–6 and as childhood obesity continues to rise, the rate of pediatric reduction mammaplasties may also follow that trend.
The risk factors associated with postoperative complications of reduction mammoplasty have been well studied for the adult population but little data exist for the pediatric population.7–9 Further, most of these studies focus on patient-reported outcomes3,9–13 and less on risk factors and objective postoperative complications.4,14–19 The purpose of this study is to identify trends in pediatric reduction mammoplasty and assess the relationship between preoperative patient characteristics to better understand the risk factors associated with the procedure in this age group.
Methods
Study Design and Sample
This is an epidemiological cross-sectional study of consecutive cases reported to the American College of Surgeons National Surgical Quality Improvement Program Pediatric database (NSQIP) between January 1, 2012, and December 31, 2019. Our institution did not require IRB approval for this de-identified, population-based, retrospective descriptive study. Our inclusion criteria for the study consisted of patients 18 years or younger and those who underwent a reduction mammoplasty during the study period. Reduction mammoplasty was identified with the Current Procedural Terminology (CPT) code: 19318. Patients were excluded as study subjects if they were older than 18 years or did not undergo a reduction mammoplasty during the study period. The NSQIP dataset is a risk-adjusted, nonadministrative, surgical outcomes database that collects 30-day postoperative patient outcomes data. 20
Variables
The study population included pediatric patients in the NSQIP pediatric database who underwent a reduction mammoplasty. The predictor variables were preoperative patient demographic data, including age, BMI, diabetes, chronic steroid use, time under anesthesia, and operative time. The primary outcome and response variable was the overall incidence of 30-day postoperative surgical site-related complication. These included superficial surgical site infection (SSI), deep incisional SSI, organ/space SSI, wound dehiscence, and pneumonia.
Data Collection
Certified surgical clinical reviewers (SCRs) collect data regarding more than 250 clinical variables, including preoperative risk factors, intraoperative variables, 30-day postoperative mortality, and 30-day postoperative morbidity from each participating site. 20 To maintain the quality of data abstraction, SCRs are mandated to complete various standardized online training modules, followed by a yearly certification exam that focuses on various aspects and processes of the program including instructions on coding and perioperative procedural definitions. They are also provided access to an online decision support system that shares specialized resources and enables individualized, case-based troubleshooting. 20 Each surgical procedure is assigned a primary postoperative diagnosis using International Classification of Diseases codes and a primary surgical procedure code using CPT codes. NSQIP utilizes a systematic, risk-weighted sampling strategy to minimize bias and ensure data quality. It routinely audits participating hospitals and SCR's to ensure interrater reliability which has demonstrated disagreement rates of less than 2.5% for all assessed program variables. 20
Data Analyses
Descriptive statistics were reported as a mean or median and standard deviation for continuous variables or frequency and percentage for categorical variables, respectively. Comparisons of proportions were performed with an “N-1” χ2 test. A logistic regression was constructed to identify associations between the predictor variable (age, BMI, diabetes, chronic steroid use, time under anesthesia, and operative time) with response variable (postoperative complication). To confirm this model, we calculated a lack of fit test and effect likelihood ratio test. In our regression model, we report odds ratios (ORs) for each effect. Before performing any tests, statistical significance was defined with a P-value <.05. All statistical analyses were performed using commercially available software (JMP 15, SAS, Inc.)
Results
A total of 1216 pediatric patients (ages 12-18) who underwent reduction mammoplasty between January 1, 2012, and December 31, 2019, were included in the study. At the time of surgery, the mean (standard deviation [±SD]) age was 16.6 years (±1.4), and the mean (±SD) BMI was 30.8 kg/m2 (±7.6). Six (6/1216; 0.5%) patients were classified as diabetic, and 2 (2/1216; 0.2%) patients reported chronic steroid use. The mean (±SD) time under anesthesia was 241.4 min (±79.7), and the mean (±SD) operative time was 182.9 min (±71.8). Full descriptive statistics of the patient population are provided in Table 1.
Patient Characteristics.
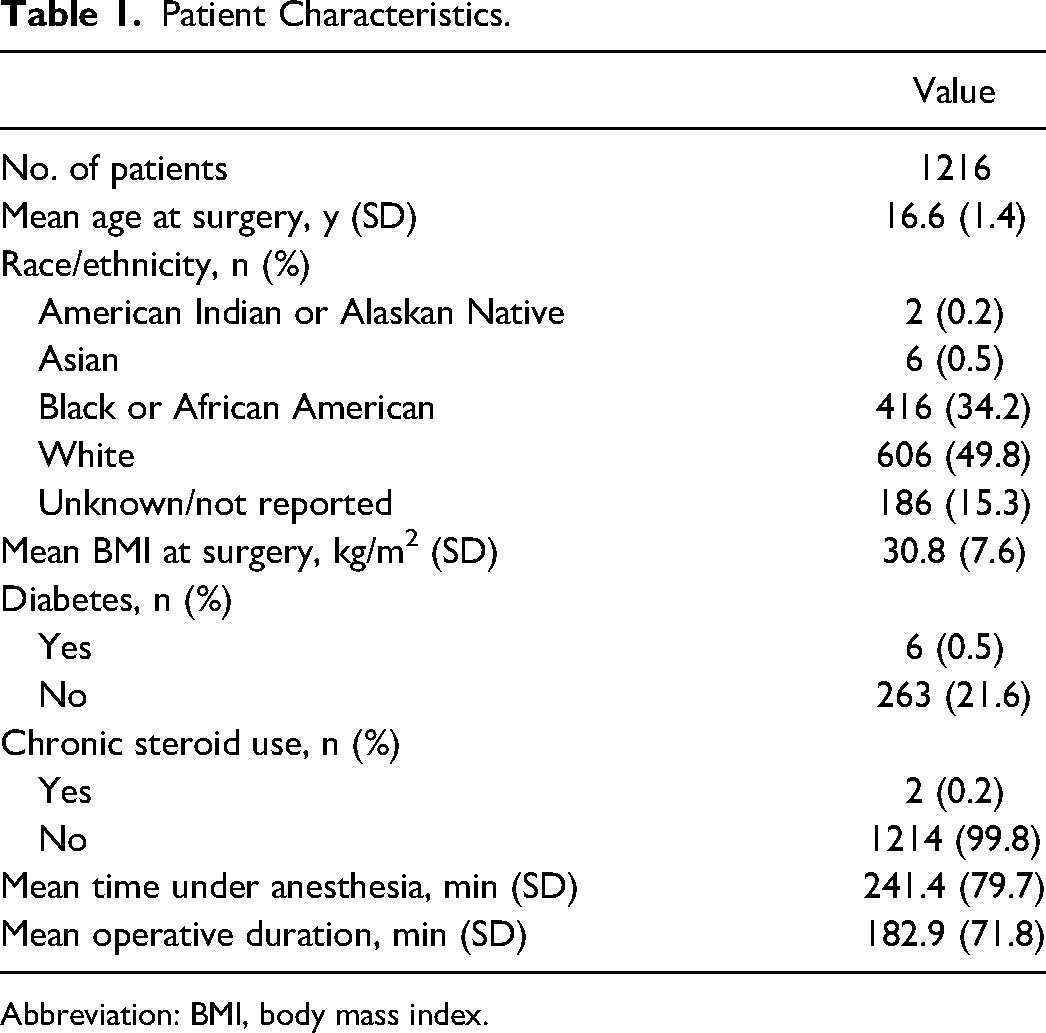
Abbreviation: BMI, body mass index.
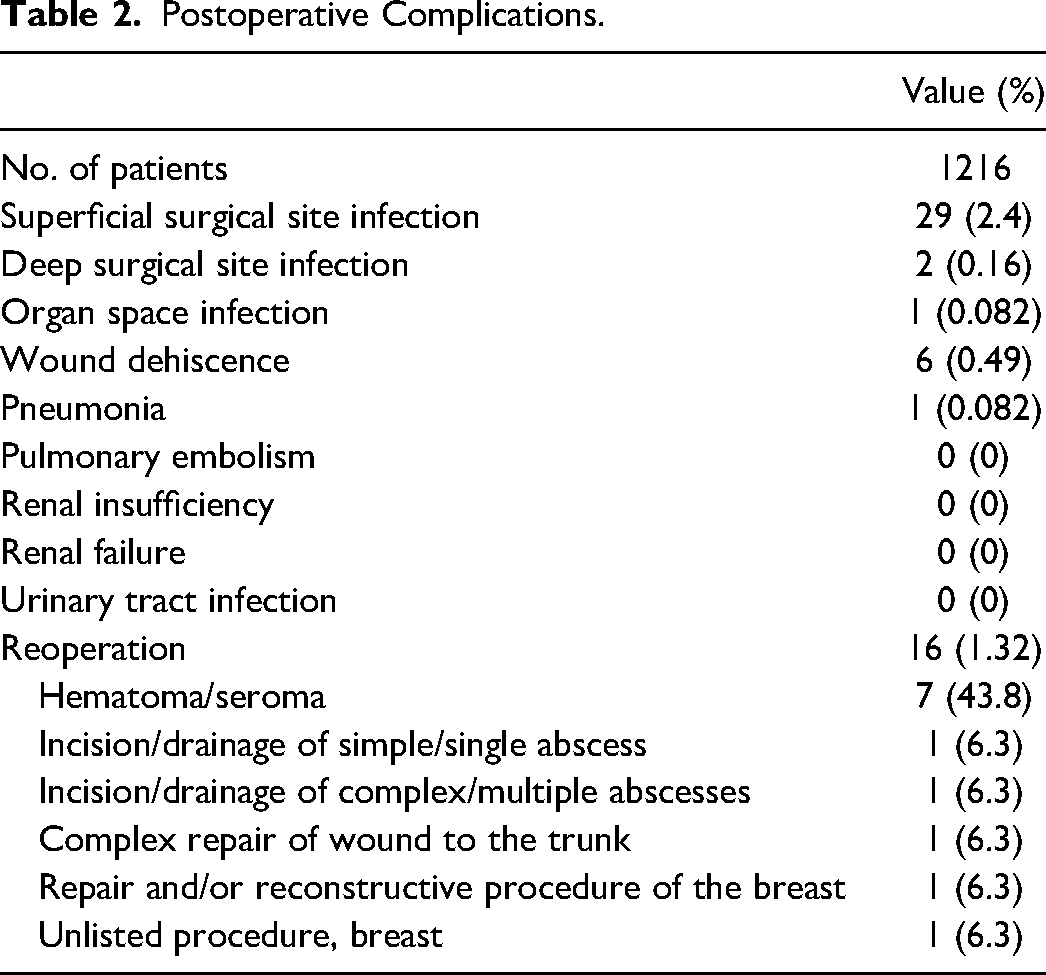
The overall incidence of postoperative complications was 4.6% (56/1216). The most common complication was superficial SSI (29/1216; 2.4%). Other less common complications included wound dehiscence (6/1216; 0.49%), deep SSI (2/1216; 0.16%), organ/space SSI (1/1216; 0.082%), and pneumonia (1/1216; 0.082%). Sixteen patients (1.32%) underwent a second operation, most commonly to address hematoma/seroma (7/16; 43.8%). Other less common reasons for reoperation included incision and drainage of simple/single abscess (1/16; 6.3%), incision and drainage of complicated/multiple abscess (1/16; 6.3%), complex repair of wound to the trunk (1/16; 6.3%), repair and/or reconstructive procedure of the breast (1/16; 6.3%), and unlisted procedure of the breast (1/16; 6.3%). No cases of pulmonary embolism, renal insufficiency, renal failure, or urinary tract infection were observed. A full summary of 30-day postoperative complications following reduction mammoplasty is provided in Table 2.
Postoperative Complications.
Logistic regression analysis revealed that BMI (OR: 1.03, 95% confidence interval [CI]: 1.00-1.05, P = .02) was significantly associated with superficial SSI. No significant association was observed between age, chronic steroid use, time under anesthesia, or operative time and the postoperative complications studied. Summary of logistic regression analysis for superficial SSI, deep SSI, and wound dehiscence is provided in Table 3.
Regression Analysis of Factors Associated With Postoperative Complications.
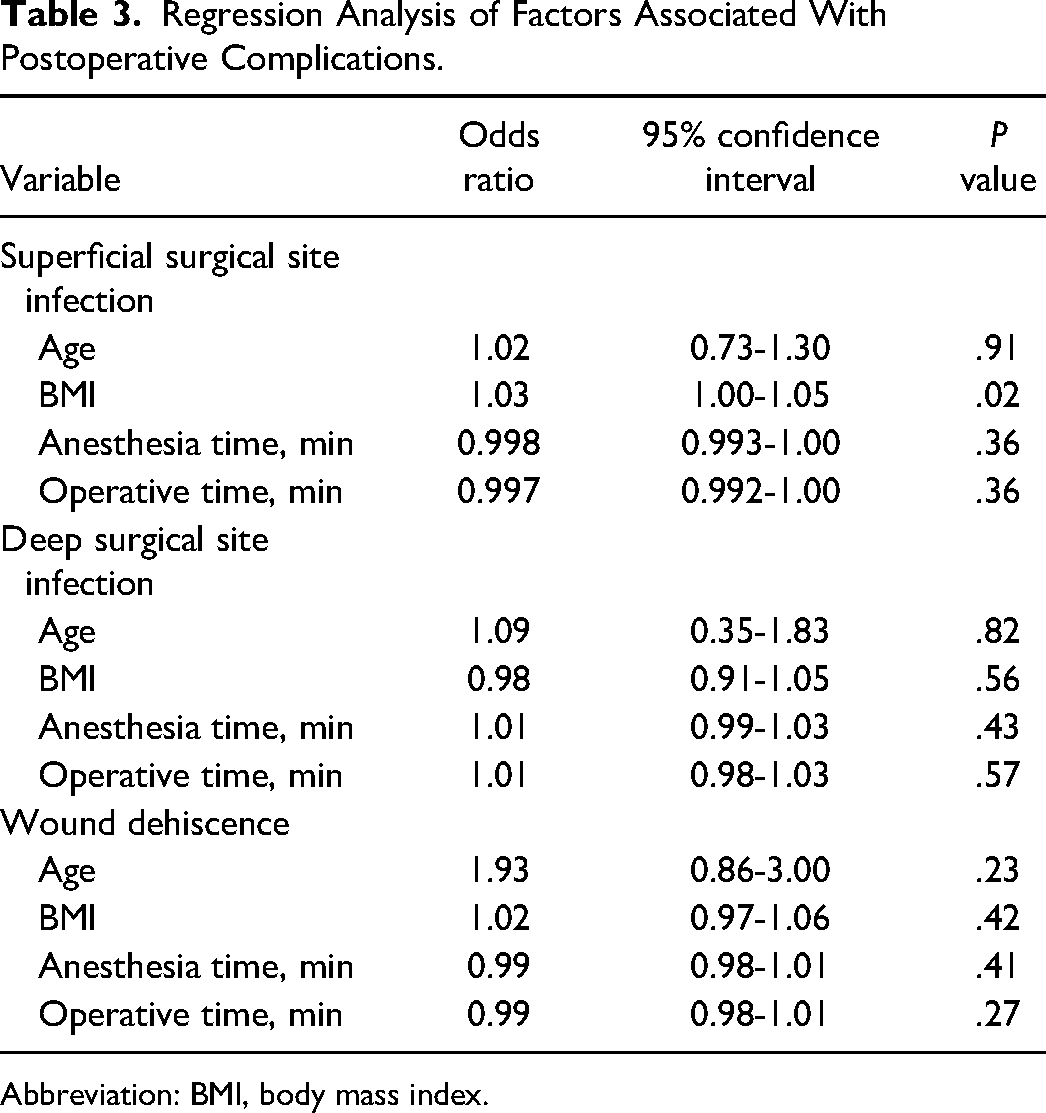
Abbreviation: BMI, body mass index.
Discussion
Reduction mammoplasty is an important therapeutic and aesthetic procedure to relieve the physical and psychosocial symptoms of breast hypertrophy and to improve patients’ quality of life. Although the proportion of reduction mammoplasties performed on pediatric patients is relatively small, the procedure is becoming more commonly done, 1 and it is important to understand the potential risk factors and postoperative complications. The data from the NSQIP dataset demonstrate that despite increases in total procedures recorded yearly in the dataset the proportion of pediatric breast reductions continues to rise (Table 4). This is consistent with data from the American Society of Aesthetic Plastic Surgery, which demonstrates that the reduction of mammoplasties performed on patients 18 years of age and younger increased from 1.9% to 2.3% from 2012 to 2019.1,21 Our study revealed a low overall postoperative complication rate of 4.6% which is like that of other pediatric studies, 22 which compares favorably to those published on postoperative outcomes following reduction mammoplasty in the adult population.7–9 SSI was the only complication with a rate greater than 1%, while all other complications were reported to be less than 0.5%. It is important to acknowledge that the statistical significance between BMI and SSI found in this study could be representative of the numbers reported in the NSQIP database during the study period rather than a true correlation.
Total Procedures and Reduction Mammoplasties Performed From 2012 to 2019 Based on Data From the NSQIP Database.
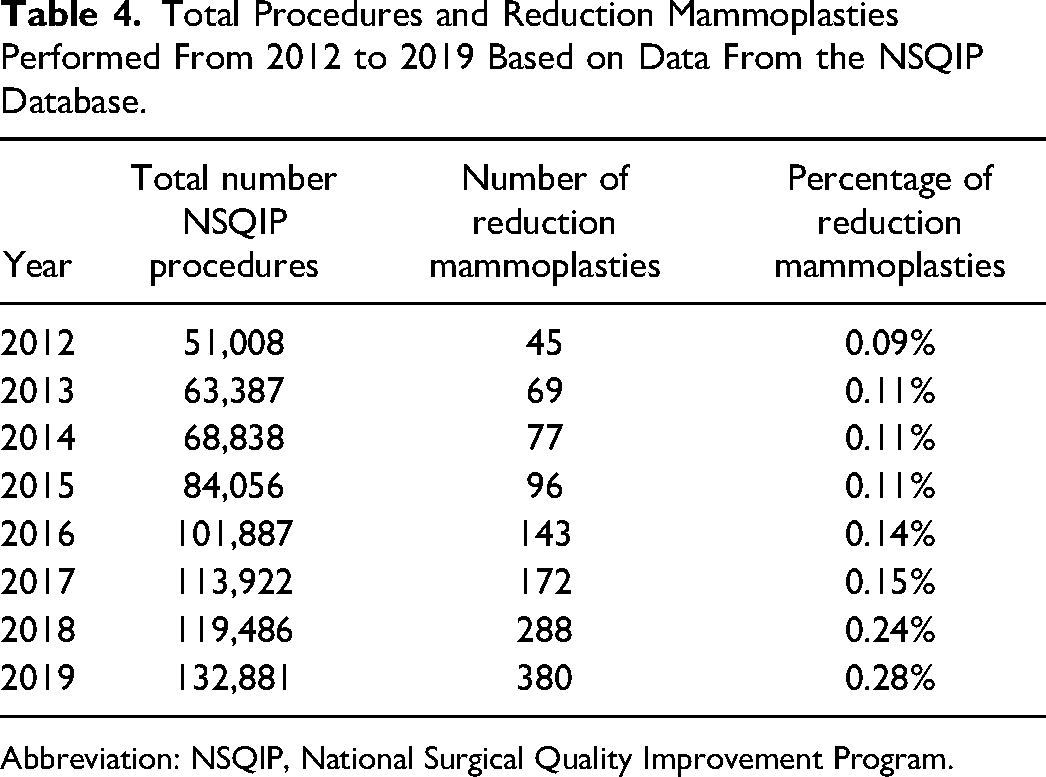
Abbreviation: NSQIP, National Surgical Quality Improvement Program.
The average BMI of the patient cohort in our study was 30.8 kg/m2. There are conflicting results regarding the relationship between BMI and postoperative complications following reduction mammoplasty. Although some have found no significant association between BMI and complication rates, 19 our results coincide with studies that show BMI is significantly associated with postoperative complications.16,23–25 Our investigation found superficial SSI and wound dehiscence to be the 2 most prevalent postoperative complications. Wound healing complications in obese patients, such as wound infection and dehiscence, have been well-documented. Chronic low-grade inflammation, poor oxygen tension, and decreased vascularity of adipose tissue are factors that may impair the healing cascade.26–28 In addition, high BMI is strongly correlated with diabetes, a well-known risk factor for postoperative complications. 24 Interestingly, our study did not identify diabetes as a risk factor. Perhaps the adverse metabolic effects of diabetes may not yet have a significant impact on this younger patient population. However, it is important to note that diabetic information was reported in only 269 of the 1216 participants. Due to the significant proportion of missing values from our study pool, it is difficult to conclude with certainty that diabetes is not significantly associated with postoperative complications.
Given the long anesthesia and operative time, a post hoc analysis was conducted to assess the relationship between BMI and operative and anesthesia time. P value was set to .05. A total of 593 patients had a BMI less than 30 kg/m2. The mean (standard deviation [ ± SD]) BMI, anesthesia time, and operative time were 25.7 (±2.7) kg/m2, 231.2 (±76.2) min, and 175.3 (± 67.8) min, respectively. Bivariate analysis showed no significant association between both anesthesia and operative time and decreasing BMI in patients with a BMI less than 30 kg/m2 (95% CI: −0.02 to 0.14, P = 0.12; 95% CI: −0.03 to 0.13, P = 0.20, respectively). A total of 622 patients had a BMI greater than 30 kg/m2. The mean BMI, anesthesia time, and operative time in this group were 35.4 (±4.5) kg/m2, 251.0 (±81.8) min, and 190.1 (±74.8) min, respectively. Bivariate analysis showed a significant association between both anesthesia and operative time and increasing BMI in patients with a BMI greater than 30 kg/m2 (95% CI: 0.03-0.19, P = .007; 95% CI: 0.002-0.16, P = .045). These results coincide with prior studies that have demonstrated that operative time increases with higher BMI.29–31
Although obesity and postoperative complications are linked, the benefit of weight loss prior to surgery is less well-defined. Insurance guidelines are discordant, with some insurers requiring the patient to reach a preferred BMI before considering surgery. Although these patients are typically advised to lose weight prior to surgery, few are successful. 32 Weight loss may be further impeded by chronic pain or discomfort with exercise, both of which are experienced by patients with breast hypertrophy. Despite evidence of obesity as a risk factor for postoperative complications, a recent study showed that reduction mammoplasty may facilitate subsequent weight loss in obese patients.33,34 A caveat of these studies that they were conducted with adult patients. Factors unique to adolescents that may affect surgical outcomes also need to be considered. These include normal weight fluctuations during adolescence, emotional and biological maturity of the patient, and the potential for breast regrowth after surgery.18,35 Many plastic surgeons hesitate to perform reduction mammoplasties on adolescents due to the potential for postoperative breast regrowth. For patients that experience at least some breast regrowth, the rate of revision reduction mammoplasty is much smaller.11,14,35,36 The biological time point at which breast size stabilizes can vary significantly. Special considerations may be required in obese patients. In a study of 481 pediatric patients, ages 12 to 21, who underwent reduction mammoplasty surgery between 2007 and 2019, researchers found that breast size may not stabilize until up to 9 years after menarche in obese patients, compared to 3 years after menarche in nonobese patients. 35 Although it may carry an increased risk for postoperative complications, obesity should not necessarily be considered as a contraindication for reduction mammoplasty in pediatric patients given the significant improvement in their quality of life. Discussing the optimal time of surgery is complex and should be approached in an individualized manner, taking into account the patient's biological and psychological maturity, physical symptoms, obesity status, and potential for postoperative benefits and complications.
A limitation of this study was that the NSQIP database is limited to 30-day outcomes, excluding data from long-term outcomes. Another limitation is that the analysis did not specify the complication rate within each BMI range. Moreover, the data analyzed in this study were limited to data captured in the NSQIP database, which excludes certain outcomes specific to reduction mammoplasty, such as the volume of tissue resected. Finally, our knowledge of the reasons for reoperation was limited to the CPT codes, if provided, in the NSQIP database. Further investigation would require a retrospective institutional study.
Conclusion
In a large series of patients, reduction mammoplasty was shown to be a safe and effective procedure to address breast hypertrophy in the pediatric population as most postoperative complications were minor. Higher BMI was significantly associated with the incidence of superficial SSIs after reduction mammoplasty, but no cases of postoperative pulmonary embolism, renal insufficiency, or renal failure were observed. Postoperative hematoma requiring reoperation was also rare. With our study, we substantiate the relatively safe risk profile associated with pediatric reduction mammoplasty and provide data to help inform physicians and patients about the potential risks associated with the procedure.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.