
Abstract
Introduction
Following mastectomy, surgical management of breast cancer patients commonly involves autologous free tissue transfer. Among the current techniques, the deep inferior epigastric perforator (DIEP) flap remains one of the most frequently performed flap procedures. 1 While using the DIEP flap may reduce donor site morbidity compared to other abdominal free flaps,2,3 the operation is not without complications. Potential postoperative complications include flap loss, skin necrosis, delayed wound healing, and dehiscence at the donor site. 2 Several patient risk factors have been previously implicated in developing these postoperative complications.3–5
Researchers have examined the relationship between morphology-based parameters and postoperative complications following breast reconstruction. These morphometric measurements include adipose tissue and muscle composition, perforator mapping, and bone density measured using computed tomography angiography (CTA). Muscle atrophy and increased subcutaneous adipose tissue have been associated with poor surgical outcomes and an increased risk for non-breast-related postoperative complications.6,7 However, recent literature regarding the relationship between CTA findings and complications following breast reconstruction has been conflicting. For example, while Boehm et al demonstrated delayed wound healing in patients with thicker abdominal wall measurements, Modarressi et al conversely found no significant relationship between abdominal wall thickness and complication rates.8,9 The effect of sarcopenia on postoperative complications following abdominally based breast reconstruction has also demonstrated inconsistent findings.10–12 Therefore, research examining the interplay between CTA characteristics and patient risk factors in complications following DIEP breast reconstruction requires continued investigation.
Assessment of morphometric measurements through preoperative CTA imaging may be advantageous for risk stratification of patients undergoing abdominally based breast reconstruction. This study examines the effect of CTA morphometric findings and other patient risk factors on postoperative abdominal wound healing and infectious complications following abdominally based autologous breast reconstruction.
Methods
Patient Data Collection
The authors conducted a retrospective cohort study of consecutive patients who underwent abdominally based breast reconstruction by five surgeons at a single institution between the years 2013 and 2018. Patients met inclusion criteria if they had undergone DIEP or muscle-sparing transverse rectus abdominis (TRAM) flap for breast reconstruction. Patients were excluded if they did not have preoperative CTA images for review.
After receiving Institutional Review Board approval, the electronic medical record was reviewed, and data were collected on patient demographics at the time of operation. Population characteristics included BMI, smoking history (including smoking within a year of surgery), diabetes, hypertension, and history of previous abdominal surgeries. The operative details were also recorded, including operative time, mastectomy weight, number of perforators included in the flap, and amount of rectus muscle (cm2) included in the flap.
Each patient's postoperative course was reviewed for abdominal donor site complications. The primary outcome was the total incidence of abdominal donor site delayed healing. Subsequently, this was subdivided into mild, moderate, and severe delayed healing. Secondary outcomes included abdominal infections (total incidence and incidence of mild, moderate, and severe infection), skin necrosis, epidermolysis, hematoma, seroma, postoperative hernia, and laxity/bulge complaints (Table 1).
Abdominal Donor Site Complication Definitions.
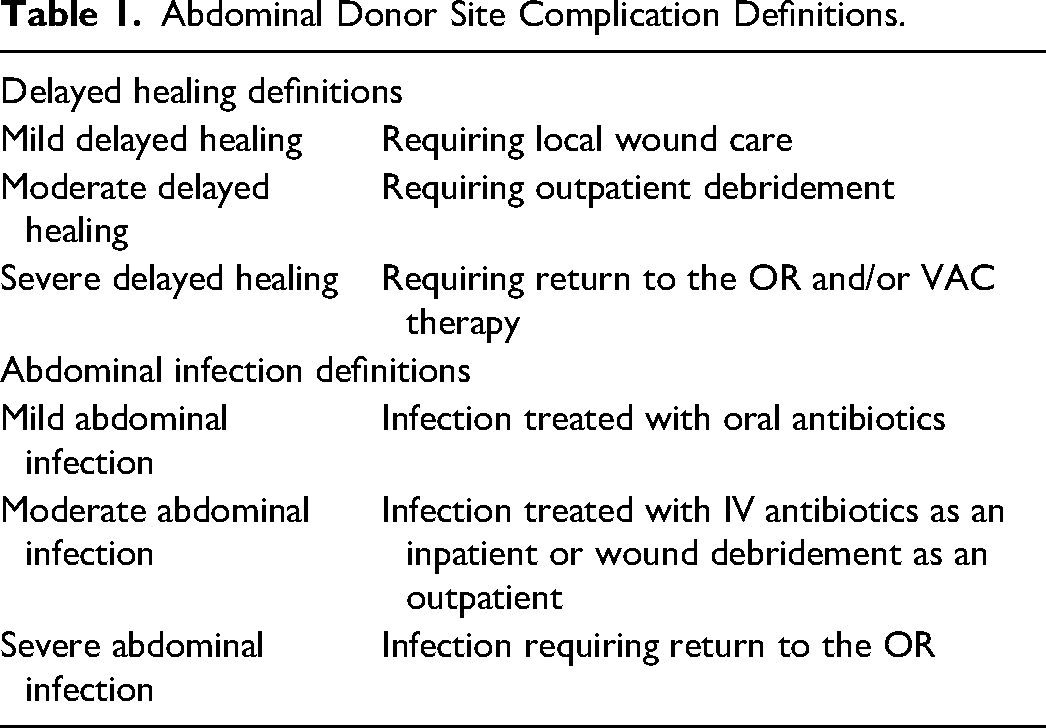
Image Processing
Preoperative CTA scans were reviewed on GE Advantage Workstation, software ADW server Volumeshare 5. The abdominal adipose tissue, skeletal muscle variables, and bone density were measured on a single cross-sectional CTA image at the most inferior level of the third lumbar vertebra (L3). This level was selected as previous literature has demonstrated that cross-sectional CTA images at this level provide the most precise estimates of body composition compared to other vertebral bodies. 13
One fourth-year medical student (who received formal training and had measurements verified by a radiologist with 11 years of experience) independently analyzed adipose tissue, skeletal muscle variables, and bone density and was blinded to the patient's medical record. Measurements were isolated based on variations in radiographic density and defined as the following (Figure 1):
Subcutaneous adipose tissue (SAT; mm2):
Total area adipose tissue between skin envelope and muscular fascia within tissue threshold of −190 HU to −30 HU. Visceral adipose tissue (VAT; mm2):
Total area adipose tissue within abdominal fascial envelope within tissue threshold of −150 HU to −50 HU, therefore removing the peritoneal and retroperitoneal organs from inclusion. Skeletal muscle area (SMA; mm2):
Total area muscle tissue (including bilateral rectus abdominis, oblique complexes, psoas, and paraspinous muscles) within tissue threshold −29 HU to 150 HU. Rectus muscle cross section (mm2):
The cross-sectional area of rectus muscle at the inferior-most level of L3 vertebrae. Psoas muscle cross-section (mm2):
The cross-sectional area of psoas muscle at the inferior-most level of L3 vertebrae. Bone density (HU):
Measured at the inferior-most portion of L3 vertebrae.
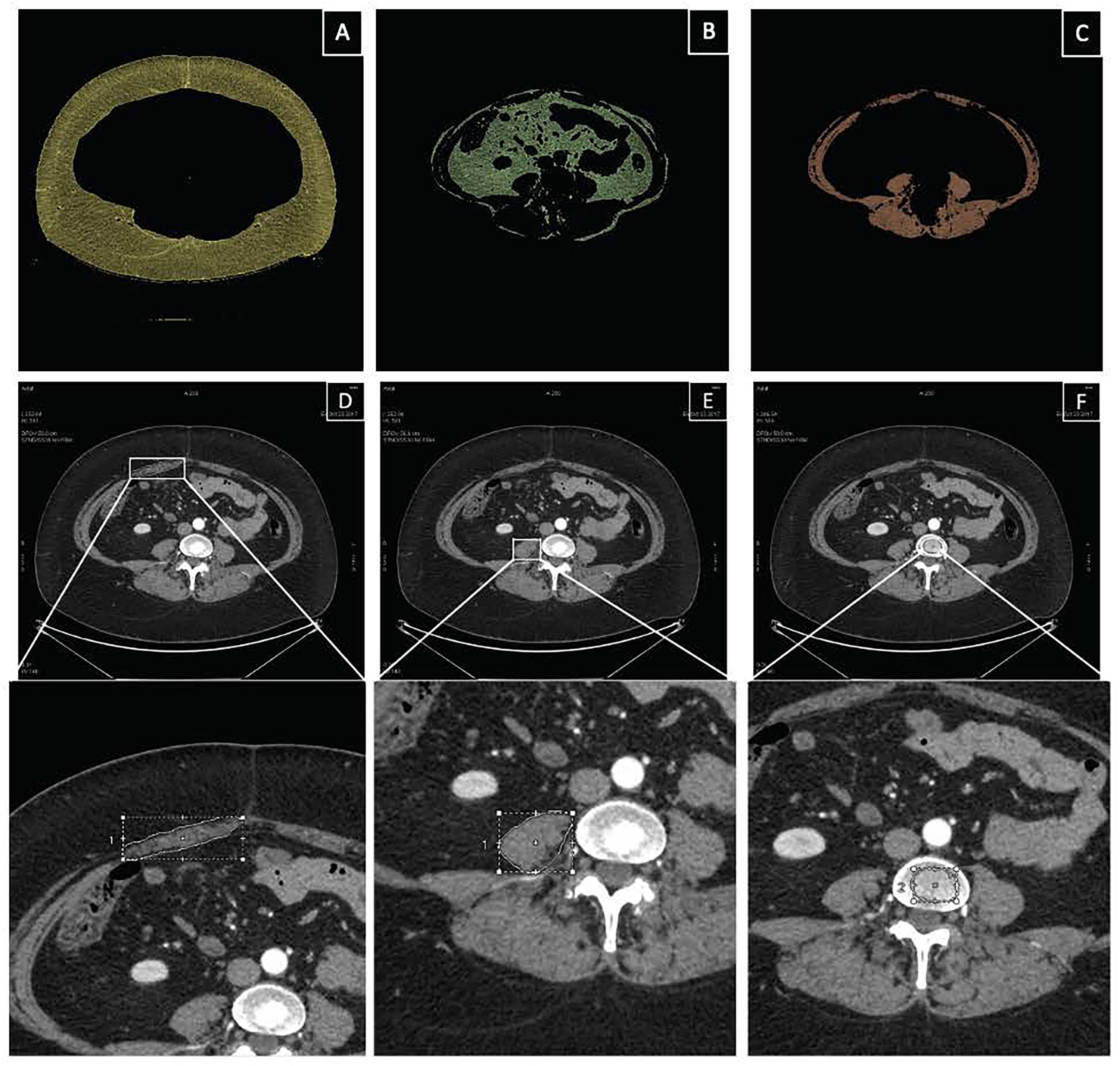
Depiction of CTA morphometric measures. (A) Subcutaneous adipose tissue (SAT; mm2), (B) Visceral adipose tissue (VAT; mm2), (C) Skeletal muscle area (SMA; mm2), (D) Rectus muscle cross section (mm2), (E) Psoas muscle cross section (mm2), (F) Bone density (HU).
Measurement data were further analyzed to obtain the subcutaneous to adipose tissue ratio and skeletal muscle index (SMI; cm2/m2). Skeletal muscle index was defined as skeletal muscle area (cm2) divided by patient height (m2). Sarcopenia was defined as an SMI of less than or equal to 41 cm2/m2.
Statistical Analyses
Descriptive sample statistics were calculated for demographic information, CTA measurements, and postoperative complications. Simple logistic regression models were used to examine the association of patient and surgical characteristics with each postoperative complication. The effects of every 100-unit change in SAT, VAT, skeletal muscle tissue, rectus cross-section, and psoas cross-section were examined for regression analyses. A 100-unit change was implemented instead of a one-unit change to provide more informative results while still examining the measures on a continuous scale. Patient BMI was examined as both a continuous and a dichotomous variable, with a cut point of BMI > 30 indicating obesity. All other independent variables were kept on their original scales. Postoperative complications were described as abdominal infection (mild, moderate, or severe), delayed abdominal healing (mild, moderate, or severe), epidermolysis, hematoma, skin necrosis, seroma, hernia, and patient-reported laxity/bulge complaints. All statistical analyses were conducted in SAS software (Version 9.4, SAS Institute Inc., Cary, NC) and assessed at the α = 0.05 level. No statistical corrections for multiple comparisons were used.
Results
Population Characteristics
A total of 174 patients who underwent abdominally based flap breast reconstruction met inclusion criteria with a mean age of 49.3 ± 9.0 years. A total of 88 patients (50.6%) were classified as obese (BMI>30.0 kg/m2) with a mean BMI of 30.4 ± 4.5 kg/m2. About 63.8% of patients underwent bilateral reconstruction with DIEP/TRAM flaps. The average follow-up time was 882.1 ± 643.3 days. Population characteristics are demonstrated in Table 2. Four patients were excluded from the study.
Population Characteristics.
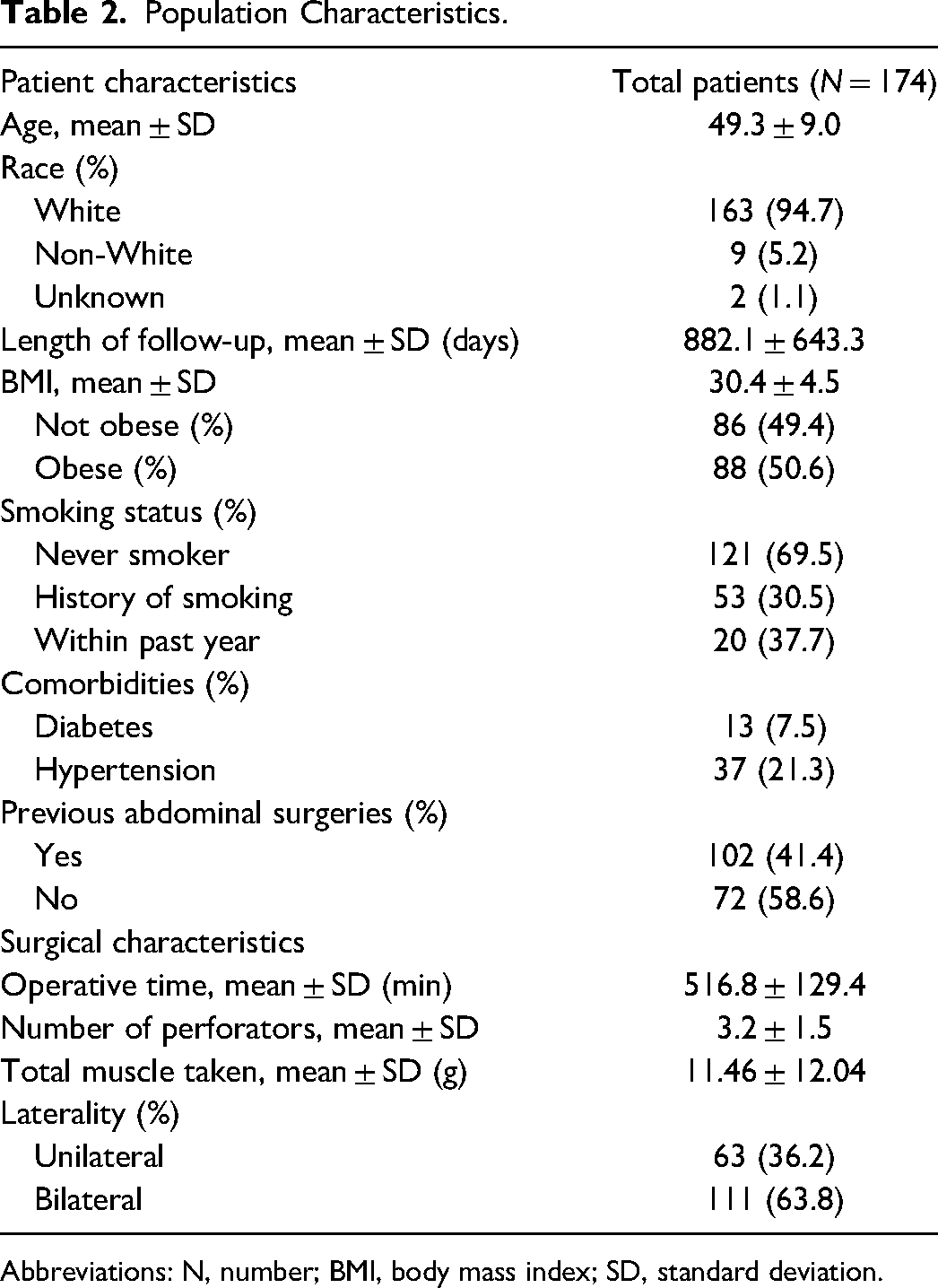
Abbreviations: N, number; BMI, body mass index; SD, standard deviation.
Abdominal Complications
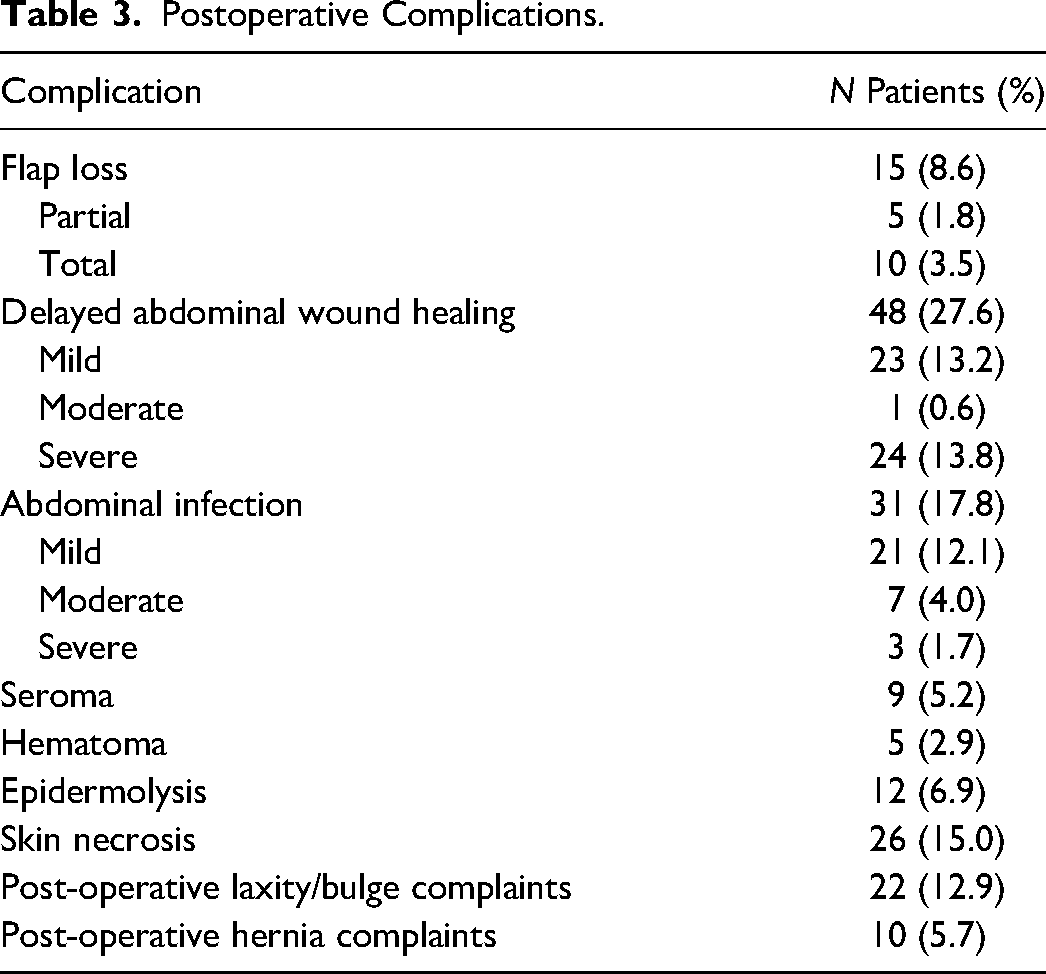
Overall, 48 patients (27.6%) developed delayed abdominal wound healing. Of these patients, 23 patients (13.2%) had mild delayed healing, 1 patient (0.6%) had moderate delayed healing, and 24 patients had severe delayed healing (13.8%). Postoperative complications are depicted in Table 3. Several patient characteristics were associated with a significantly increased likelihood of developing delayed abdominal wound healing, including obesity (OR 2.21; 95% CI 1.11-4.39; P = .024), a history of smoking (OR 2.01; 95% CI 1.00-4.05; P = .049), and smoking within the past year (OR 3.05; 95% CI 1.18-7.89; P = 0.021). Regarding surgical characteristics, the number of perforators in the harvested DIEP flap significantly increased the likelihood of delayed abdominal wound healing (OR 1.29; 95% CI 1.02-1.64; P = .035). Increasing visceral adipose tissue, subcutaneous adipose tissue, and skeletal muscle index were not significantly associated with delayed abdominal wound healing (P = .20, P = .39, and P = .43, respectively). No other CTA variables (Table 4) or other population characteristics influenced the risk of developing delayed abdominal wound healing (Table 5). There was no difference in abdominal complication rates when comparing patients who underwent DIEP versus TRAM flaps for breast reconstruction.
Postoperative Complications.
CT Variables.
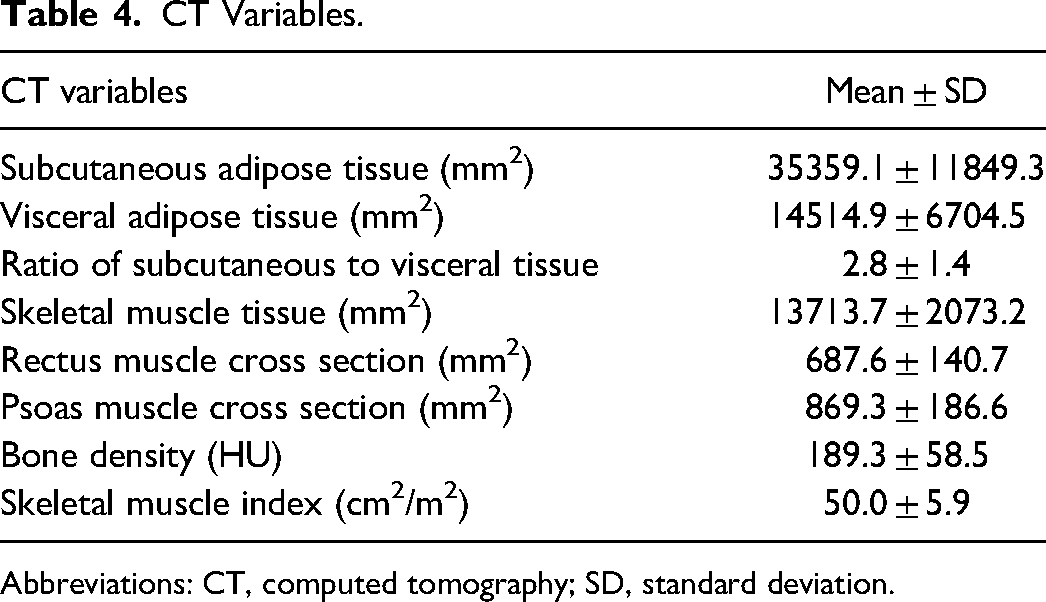
Abbreviations: CT, computed tomography; SD, standard deviation.
Logistic Regression for Total Delayed Abdominal Healing and Total Abdominal Infection.
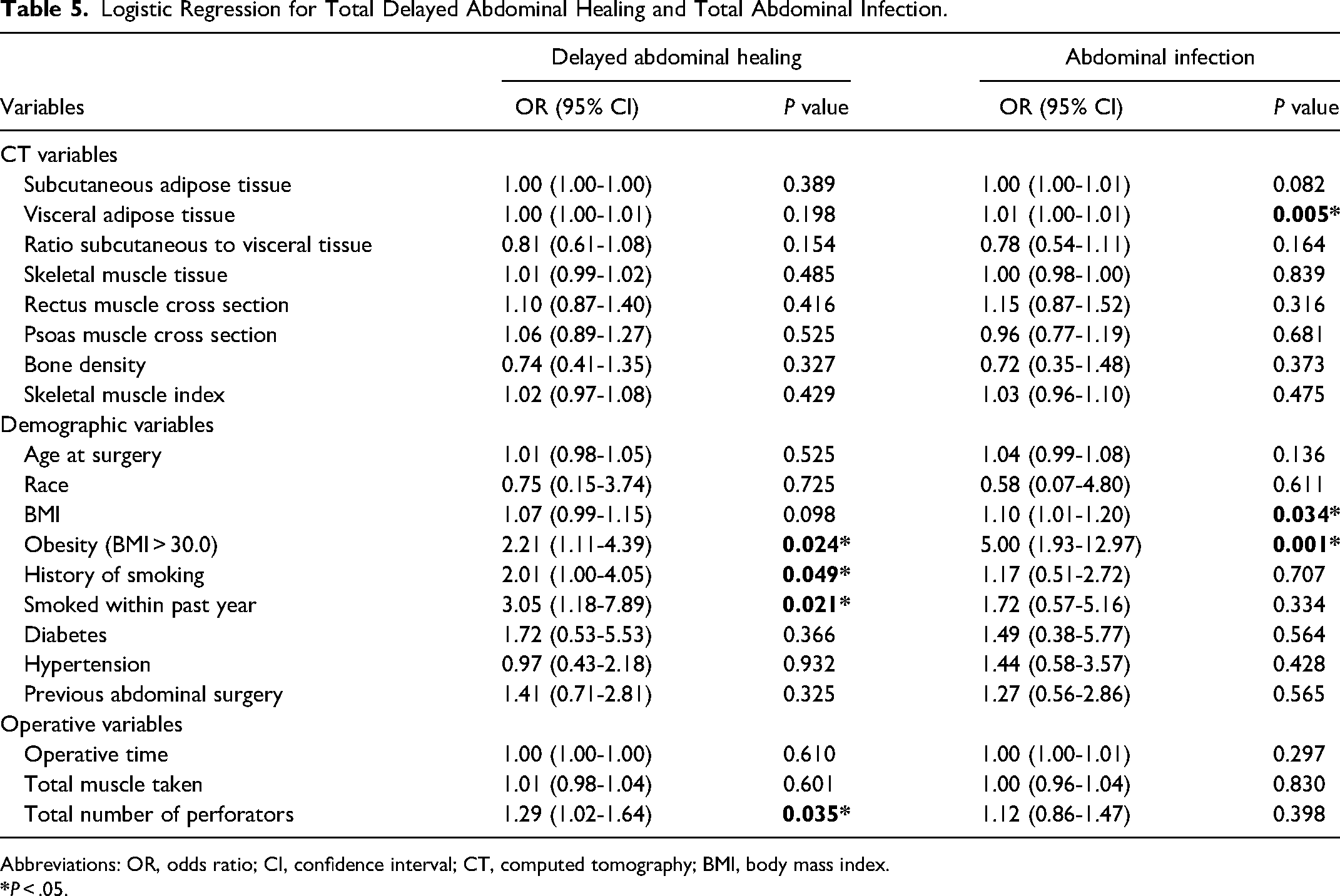
Abbreviations: OR, odds ratio; CI, confidence interval; CT, computed tomography; BMI, body mass index.
A total of 31 patients (17.8%) developed postoperative abdominal infections. A total of 21 patients (12.1%) had mild infections, 7 patients (4.0%) had moderate infections, and 3 patients (1.7%) had severe infections (Table 3). Increasing visceral adipose tissue on CTA imaging was significantly associated with an increased likelihood of developing an abdominal infection (OR 1.01; 95% CI 1.00-1.01; P = .005). The subcutaneous to visceral adipose tissue ratio was not associated with an increased likelihood of abdominal infection (P = .16), nor was the skeletal muscle index (P = .48). No other CTA findings significantly contributed to the risk of developing an abdominal infection (Table 5). Obesity and increasing BMI significantly increased the odds of an abdominal infection (OR 5.00; 95% CI 1.93-12.97; 0.001; OR 1.10; 95% CI 1.01-1.20; P = .034, respectively). Smoking history (P = .71) and other demographic factors were not associated with postoperative abdominal infections.
Other Postoperative Complications
A total of 12 patients (6.9%) developed epidermolysis, 5 patients (2.9%) developed hematomas, 9 patients (5.2%) developed seromas, 10 (5.7%) developed hernia, and 22 (12.9%) patients reported postoperative laxity/bulge complaints (Table 3). Increasing visceral adipose tissue on CTA imaging significantly increased the likelihood of developing both epidermolysis (OR 1.01; 95% CI 1.00-1.02; P = .031) and seroma (OR 1.01; 95% CI 1.00-1.02; P = .040), while increasing bone density was associated with a decreased likelihood of seroma formation (OR 0.21; 95% CI 0.05-0.89; P = .034). Increased age at breast reconstruction was associated with a significantly increased likelihood of developing a seroma (OR 1.10; 95% CI 1.01-1.20; P = .028). No other CTA variables or population characteristics influenced the odds of developing other postoperative abdominal complications. There was no significant association between the morphometric data, or the number of perforators harvested and postoperative patient-reported laxity/bulge complaints (Table 6).
Logistic Regression for Total Epidermolysis, Hematoma, Skin Necrosis, Seroma, Postoperative Laxity/Bulge, and Postoperative Hernia Complaints.
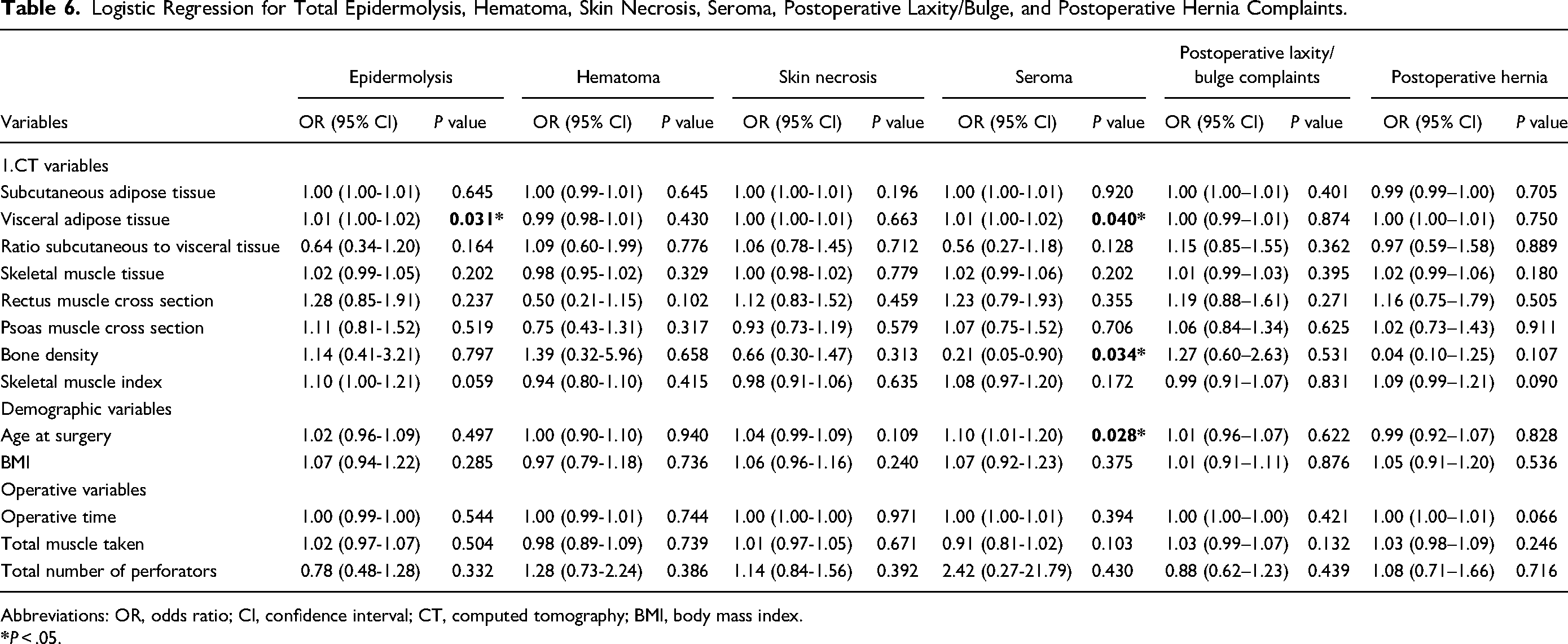
Abbreviations: OR, odds ratio; CI, confidence interval; CT, computed tomography; BMI, body mass index.
Discussion
In this study, we perform an extensive retrospective review to evaluate if preoperative CTA findings and patient characteristics can be used to determine the risk of abdominal donor site complications. Additionally, our study is the first to include adipose morphometric data, muscle distribution, and bone density in patients undergoing autologous breast reconstruction with DIEP or TRAM flaps. We demonstrated that, while no specific CTA variable was associated with delayed abdominal wound healing, increased visceral fat is significantly associated with the likelihood of developing seroma (OR = 1.01, P = .04), epidermolysis (OR = 1.01, P = .031), and infection (OR = 1.01, P = .005) at the abdominal donor site and increased bone density was significantly associated with a decreased likelihood of developing seroma (OR = 0.21, P = .034).
Abdominal visceral adipose tissue has been described as an accurate indicator of patient baseline health than BMI. Its presence, in excess, has been linked to multiple pathologic conditions, including metabolic syndrome, ischemic heart disease, and arterial hypertension.14–16 Regarding direct surgical factors, previous literature has demonstrated increased visceral fat volume associated with predisposition to multiple cancers, prolonged hospital stay, and increased risk of hospital mortality.17–19 The mechanism by which increasing visceral fat results in an increased risk for infection, seroma, and epidermolysis is unclear but may be secondary to compromised vascular endothelial function and angiogenesis. 20
Prior studies evaluating the impact of preoperative CTA abdominal visceral adipose distribution on donor site complications in patients undergoing abdominally based autologous reconstruction have demonstrated inconsistent findings. A small proof of concept study published by Levi et al found a significant correlation between visceral fat area (VFA) with abdominal wound dehiscence (OR = 1.24, P = .002). 21 Conversely, a more extensive retrospective review of 97 patients by Timmermans et al concluded that visceral fat was not a significant predictor of abdominal wound dehiscence. 22
Incorporating the variable of visceral fat area into practice can be achieved through discussion with your institutional radiologist. Measurements of visceral fat area can be performed preoperatively and included in the final image interpretation. While a specific cutoff value for visceral fat area predicting abdominal donor site complications was not obtained in this study due to a limited patient population, previous studies have cited a cutoff value of 1030 mm2 being predictive of obesity-related health risks. 23 Further study is needed to confirm that this value is also predictive of operative complications.
Studies evaluating subcutaneous adipose fat, measured as abdominal wall thickness, have also produced conflicting wound healing and infection findings.7,8 We found no significant correlation between subcutaneous adipose tissue with donor site complications. One explanation for our results may be our total subcutaneous adipose tissue measurement compared to subcutaneous fat thickness. A high correlation between a single abdominal area in cross-section and the total volume of adipose tissue has been shown in the literature. 24 Measurement of abdominal wall thickness at a single location may not adequately represent total subcutaneous adipose tissue and may have impacted our statistical analysis.
We found no significant correlation between skeletal muscle cross-section or skeletal muscle index and donor site complications. Studies from other surgical subspecialties have demonstrated a significant correlation between morbidity and mortality with decreasing muscle area.6,25–27 However, breast reconstruction is performed on an elective basis and allows time for preoperative preparation. Broyles et al found no association between sarcopenia in patients undergoing abdominally based breast reconstruction and surgical complications within the surgical oncology literature. 10 Of our 174 patients, only 10 (5.7%) met the criteria for sarcopenia. Our average skeletal muscle index was 50 (± 5.9) cm2/m2 despite 43% of patients receiving preoperative chemotherapy. This may indicate an inherent selection bias where reconstruction was delayed until patients had adequately recovered from chemo or radiation therapy, given that sarcopenia is a reversible etiology, as demonstrated in the SMART trial. 28 Furthermore, while rectus cross-sectional area has been identified as a risk factor for abdominal bulge/hernia formation, we found no association between muscle (rectus and psoas) cross-sectional area and patient-reported postoperative laxity/bulge complaints.29,30
Our study was the first to assess bone density in patients undergoing autologous breast reconstruction. We demonstrated that an increased bone density was significantly associated with a decreased likelihood of seroma formation postoperatively (OR = 0.21, P = .034). The pathophysiology of this finding is unclear as the current literature focuses on the impact of bone density on fracture healing, and no studies have focused on the association between bone density and seroma formation. One possible explanation could be that higher bone mineral density is associated with decreased frailty, indicating better overall health status. Previous literature evaluating risk factors for seroma development identified moderate-strength evidence that patients with higher BMI, more complex mastectomy procedures, and high initial drain output are associated with a higher likelihood of seroma formation. 31 Existing evidence is inconclusive for age as a risk factor for seroma formation. 32
Multiple patient characteristics were associated with abdominal morbidity, including a significant association between obesity (BMI > 30.0 kg/m2) with delayed abdominal healing and abdominal infection and smoking (including smoking within the last year) and delayed abdominal healing. These findings are consistent with what has been presented previously in the literature. High BMI, specifically a BMI > 30 kg/m2 has consistently been a significant risk factor for complications after autologous breast reconstruction and emphasized by a meta-analysis performed by Lee and Mun.3,5,33–37 This must be weighed against the fact that there is greater patient satisfaction with autologous reconstruction in the obese patient population. 38 Furthermore, as previously discussed, BMI may fail to accurately reflect the distribution of abdominal adipose tissue or other underlying medical conditions, given that it is a measure of body size based on height and weight. A study by Camhi et al demonstrated an inconsistent relationship between BMI and visceral fat area, which may allude to why BMI was associated with delayed wound healing while visceral fat area does not. 39
Due to its vasoconstrictive effects, active or previous smoking has also been emphasized in the literature as a significant risk factor for abdominal complications in patients undergoing autologous reconstruction.40–42 Goltsman et al looked at the effect of smoking on wound complications in over 40,000 patients and found that overall, smokers are at a 1.5 increased risk of wound complications compared to nonsmokers. 43 Our study identifies that any history of smoking and smoking within a year of surgery has detrimental effects on abdominal healing with a two-fold increased risk of developing delayed abdominal healing. At our institution, we now employ screening using urine cotinine and, in a delayed setting, will wait until a patient is known to have quit before proceeding with reconstruction. Nevertheless, extensive education is provided regarding the increased risk of complications if the patient has any prior smoking history.
Regarding operative variables, we demonstrated a significant association between increased number of perforators taken with the flap and the risk of abdominal delayed wound healing with a nearly 30% increased odds (OR = 1.29, P = .035) of delayed healing. This may be secondary to reduced skin perfusion postoperatively, given greater anatomic disruption from dissection. Furthermore, no significant association was demonstrated between the number of perforators harvested and postoperative laxity/bulge complaints. While no prior literature has specifically looked at the impact of the number of perforators harvested and abdominal donor site complications, an article by Hembd et al described the harvest of lateral, medial, and lateral row perforators increases the risk of abdominal bulge. 44 Conversely, including multiple perforators within the TRAM or DIEP flap, is associated with a decreased risk of flap fat necrosis. Baumann et al demonstrated a nearly eight times risk (P = .007) of flap fat necrosis when comparing 1–2 versus 3–5 included perforators. 45 Potential need to harvest multiple perforators may be discussed both pre-and postoperatively with the patient to appropriately discuss the risks of abdominal morbidity versus the benefits of flap perfusion.
Our study demonstrates that assessing the total volume of visceral adipose tissue from preoperative CTAs is beneficial to help determine individuals who may be at greater risk of postoperative abdominal morbidity. Preoperative identification of high-risk patients could benefit from a discussion about changes in lifestyle habits and weight loss with an additional delay of reconstruction to mitigate risk. Additionally, individuals with more perforators harvested during reconstruction should be counseled regarding the risk of delayed abdominal healing. Regarding our current protocols, patients at our institution undergo standard use of preoperative prophylactic antibiotics and intraoperative drain placement to mitigate infection and seroma formation. Drains are maintained until their output is less than 30 cc for 48 h.
The strengths of our study are that this is a large retrospective study where we examined the use of preoperative CTA morphometric variables in patients undergoing autologous breast reconstruction. We plan to continue the evaluation of patient morphometric data prospectively to develop a risk assessment tool and identify a threshold value for visceral fat volume, which could preclude a patient from being an optimal candidate for autologous-based surgery.
We acknowledge there are limitations to our study. First, this is a retrospective, single-institution study that could limit the application of data. Second, given the low frequency of specific outcomes (e.g., hematoma and seroma), the generalizability of results may be biased. However, our incidence of these complications is consistent with previously reported values. 46 Furthermore, while we assessed the incidence of laxity/bulge complaints, we did not specifically analyze the odds of revision surgery for hernia development. Third, despite subcategorizing the incidence of delayed abdominal healing and infection into mild, moderate, and severe, our results were only significant when accounting for total events. Fourth, despite exceeding prior power calculations to demonstrate the effectiveness of morphometric variables, our patient population was insufficient to create a risk assessment tool for clinical application—a goal of the study a priori.
Conclusions
This study demonstrates that increased visceral adipose tissue is significantly associated with an increased risk of abdominal donor site complications. CTA morphometric data combined with identifying high-risk patient variables can help guide preoperative counseling and better quantify surgical risk.
Footnotes
Author Contributions
ECS lead contributor to project development, data acquisition, data analysis; lead contributor to manuscript writing/editing. NL assisted in project development, data acquisition, data analysis; assisted in manuscript writing. AJS assisted in project development, data acquisition, data analysis; assisted in manuscript writing and editing. TJZ lead in imaging acquisition and analysis; assisted in manuscript editing. SOP major contributor in manuscript writing and editing. BFM major contributor in project development/methodology; major contributor to manuscript writing and editing.
Statement of Presentations
Accepted for Presentation at PSTM 2022, Boston, MA.
Ethical Approval
University of Wisconsin IRB Approval Code: 2019-0775.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.