
Abstract
The hypercoagulable state of COVID-19 infection presents a challenge to microsurgeons. While the American Society of Anesthesiologists recommends deferring surgery for 4–10 weeks for COVID-19-infected patients, little else is known regarding how to mitigate thrombotic complications for patients undergoing free tissue transfer. Here, we present a presumed COVID-19-induced hypercoagulable state in a patient undergoing abdominally based free tissue transfer for breast reconstruction as a brief review of the literature to guide clinical decision making.
Introduction
The American Society of Anesthesiologists (ASA) recommends deferring surgery for 4–10 weeks in COVID-19 positive patients. 1 As a result, there is a scarcity of knowledge and thus treatment recommendations to mitigate the presumed heightened risk for perioperative thrombotic complications, particularly for patients undergoing free tissue transfer. Very few case reports describe free flap surgery during the peri-COVID-19 infection window.2-5
Here, we present a presumed COVID-19-induced hypercoagulable state in a patient undergoing abdominally based free tissue transfer for breast reconstruction as a brief review of the literature to guide clinical decision making.
Case Report
The patient is a 47-year-old fully vaccinated female presenting with right invasive ductal carcinoma and a high-risk genetic mutation (pathogenic ATM gene mutation). She elected to undergo bilateral mastectomies with immediate autologous breast reconstruction. She had no risk factors for venous thromboembolism (VTE). Per hospital preoperative protocol, she underwent a polymerase chain reaction (PCR) COVID-19 test within 48 h of surgery which resulted negative.
Bilateral nipple-sparing mastectomies were performed with right sentinel lymph node biopsy. Concurrently, a 3-perforator deep inferior epigastric artery perforator (DIEP) flap was harvested from the right hemiabdomen to reconstruct the left breast whereas a muscle-sparing transverse rectus abdominis muscle (TRAM) flap was harvested from the left hemiabdomen to reconstruct the right breast. No complications were noted with flap harvest, recipient exposure, or during microanastamosing to the anterograde internal mammary (IMA/IMV) system. However, during the flap inset on the left, the arterial signal was lost. Upon inspection of the arterial anastomosis, no flow was noted, and the anastomosis was excised. While the anastomosis appeared pristine, white thrombus was identified. A heparin infusion was started at 500 u/h after a 2000 unit intravenous (IV) bolus was given. The arterial anastomosis was repeated, but again developed a white thrombus approximately 10 min later. The anastomosis was again inspected extensively and found to be in pristine condition without evidence of mechanical obstruction. After flushing the pedicle with heparinized saline, another 2000 IV unit bolus of heparin was administered and the heparin drip was increased to a full anticoagulation protocol of 12 u/kg/h. The anastomosis was again repeated using the retrograde IMA due to decreased length on the anterograde IMA from multiple excised anastomoses. The contralateral flap anastomosis was then performed without complication. The patient was transferred to the ICU where full anticoagulation heparin infusion was continued.
On postoperative day (POD) 2, she was mildly hypotensive, with frankly sanguineous drain output and her hematocrit had decreased from 28 to 21 the day prior, requiring a unit of packed red blood cells. Physical exam findings were consistent with a left breast hematoma. The Heparin infusion was stopped, and the patient was emergently taken back to the operating room (OR).
Hemostasis was achieved without any microsurgical intervention and continuous arterial doppler signals were robustly present throughout. Just prior to extubation and circa 90 min after the heparin infusion had been discontinued (corresponding to the half-life of heparin), the arterial doppler signal was again lost.
The anastomosis was obstructed again, excised, and inspected. No technical issue was identified but an obstructing thrombus was again encountered. A mechanical embolectomy was performed followed by intra-flap administration of tissue plasminogen activator (TPA). A 2000 unit IV bolus of heparin was administered followed by a continuous heparin infusion at 500 u/h. Unfortunately, after 20 min, the recurrent arterial thrombus had formed. The anastomosis was again noted to be technically pristine with obstructing thrombus present.
Full anticoagulation protocol heparin infusion at 14 u/kg/h was restarted and an end-to-side anastomosis was performed given the size mismatch between the now shortened pedicle and recipient IMA. Flow was re-established and remained intact via continuous signals. Unfortunately, approximately 1 h later (day 3 of hospitalization), she was noted to have a massive hematoma on the contralateral right side. Heparin infusion was discontinued, a circumferential compressive dressing was placed, and she was emergently returned to the OR. After hemostasis was obtained on the right side, the left flap was inspected and found to be non-viable-likely secondary to overwhelming intra-flap thrombus and was thus debrided. Enoxaparin 40 mg daily was started the following day.
Per hospital protocol, repeat COVID-19 testing was performed prior to return to the OR and was found to be positive. On POD3, she developed pharyngitis, cough, and shortness of breath with increased oxygen requirements and was started on remdesivir. Chest radiograph revealed new bilateral pleural effusions (Figures 1 and 2) consistent with COVID-19 radiographic findings. 6 Oxygen requirements were weaned over the next 3 days. Hematology was consulted and a full hypercoagulable workup was initiated. She was discharged home with enoxaparin 40 mg daily for 30 days. Hypercoagulable workup was completed once anticoagulation was completed and did not demonstrate any known mutations. No additional complications were noted on post-admission follow-up.

Preoperative chest radiograph 5 days prior to surgery.

Chest radiograph taken 5 days after initial surgery in the setting of acute COVID-19 infection.
Discussion
As we enter the third year of the COVID-19 pandemic, the scientific understanding of the virus pathophysiology, specifically as it pertains to general hypercoagulability has become quite robust. Therapeutic anticoagulation with low molecular weight heparin and unfractionated heparin has been extensively shown to reduce mortality in critically ill patients as well as optimize organ support in noncritically ill.7-12 In addition to its anticoagulation effects, heparin inhibits proteolytic activity of SARS-CoV-2, competes with cell binding sites, and modulates inflammatory mediators.7,8,13
A recent randomized control trial found that therapeutic-dose anticoagulation with heparin increased probability of survival to hospital discharge in noncritically ill patients infected with COVID-19. 10 Similarly, a 2022 metanalysis showed a significant reduction in major thrombotic events in the full anticoagulation cohort without significant difference in bleeding events. 11
The role of therapeutic dose heparin in microsurgery, however, must be balanced with bleeding risks. We present a patient who likely was inoculated right after her PCR test 40 h preoperatively. She demonstrated significant micro-vascular thrombotic proclivity responsive only to therapeutic heparin therapy and became recurrently pro-thrombotic with cessation thereof. In fact, the traditional 500 u/h infusion described for other hypercoagulable conditions 14 was insufficient. Unfortunately, her propensity for life-threatening hemorrhage ultimately precluded its use and led to eventual flap loss. Given an otherwise unremarkable history and hypercoagulable workup, as well as lack of technical error in any of the microsurgical anastomoses, her active COVID-19 infection was the diagnosis of exclusion for her hypercoagulable state. Similarly, the seesaw oscillation between prothrombotic versus bleeding state seen in this patient is typical of COVID-19. 15
To mitigate bleeding complications of anticoagulation, alternative heparin titration algorithms have been proposed using thromboelastography (TEG) and conventional coagulation tests (CCT). While this approach is relatively new, TEG/coagulation marker-guided heparin dosing algorithms may be considered in the management of COVID-19 positive patients undergoing microsurgical reconstruction to reduce hematoma risk.
Strong evidence suggests the heightened risk of perioperative VTE and PE in COVID-19 positive patients, especially in the acute illness phase.9,16-18 The COVIDSurge Collaborative study found that symptomatic convalescent patients 7 weeks from infection had higher mortality compared to asymptomatic patients. 19 Other studies showed hypercoagulable states can persist for up to one-year post-infection. 20 Whether this translates to the microanastamosis in the same manner remains unclear, however given COVID-19's pro-inflammatory effect on the cardiac and renal microcirculation, similar consequences are possible.
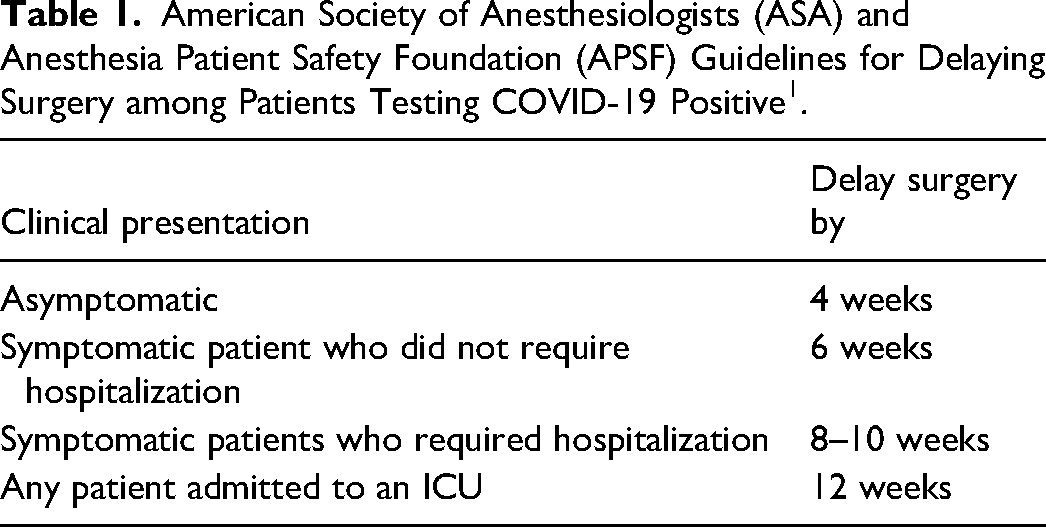
Evidence-based guidelines for how long to delay free tissue transfer post-infection also remain nebulous. The American Society of Anesthesiologists (ASA) and Anesthesia Patient Safety Foundation (APSF) have published general guidelines 1 (Table 1), however, none exist for the microsurgical patient specifically.
American Society of Anesthesiologists (ASA) and Anesthesia Patient Safety Foundation (APSF) Guidelines for Delaying Surgery among Patients Testing COVID-19 Positive 1 .
Some suggest guiding surgical timing based on laboratory values and imaging studies, however, conclusive evidence remains sparse. 12 D-dimer, ferritin, fibrinogen, partial thromboplastin time (PTT), vonWillibrand factor, interleukin-6 (IL-6), and c-reactive protein (CRP) have all been demonstrated to persist following COVID-19 infection with potential thrombogenic implications.21-23 Unfortunately, many of these markers are non-specific and in isolation are difficult to interpret.
Conclusion
Extrapolating from the literature, for any non-emergent cases, delaying microsurgical reconstruction for 6–12 weeks appears prudent. Routine preoperative COVID-19 testing and delaying in the event of a positive test should be strongly considered. When delaying free tissue transfer is not feasible or COVID-19 positivity is diagnosed post-operatively, obtaining CCTs and TEG to gauge possible hypercoagulability and using TEG/CCTs guided heparin dosing algorithm should be also considered to avoid excessive bleeding risks of standard therapeutic heparin protocols.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.