
Abstract
Introduction
Nerve injuries are common after trauma and can be life altering for patients. 1 As the understanding of nerve pathophysiology has evolved over the years, so has the classification of nerve injuries. The earliest well known classification system comes from Seddon, an orthopedic surgeon in Oxford, who in 1942 proposed dividing nerve injuries into the three categories of neurapraxia, axonotmesis, and neurotmesis.2,3 While his original plan was to name the categories “transient block,” “lesion in continuity,” and “division of a nerve,” his professor of neurology colleague Cohen suggested the Greek terms for the classification system.4,5
Sunderland, a professor of anatomy in Melbourne, then expanded on this classification system by increasing it to five categories where axonotmesis and neurotmesis were each divided into two subcategories. 6 He predicted that modern physicians would not appreciate the use of Greek terms. As an anatomist, he focused on the nerve sheath layers to differentiate the injuries and recovery patterns. In chapter 9 of his textbook Nerve and Nerve Injuries, he described a numerical classification (I-V). 7 A I degree injury is a neurapraxia with preservation of the architecture of the nerve and complete recovery expected. He described a II degree injury as axonotmesis with an intact endoneurium and the potential for complete spontaneous recovery. A III degree injury involves scaring in the endoneurium and as a result of “cross-wiring”, does not achieve complete spontaneous recovery. Recovery after this injury would be variable depending on the severity of scarring and degree of axonal loss. Neurotmesis was divided into Sunderland IV degree (neuroma in continuity with complete scar block), and Sunderland V degree (complete transection). 7 After the observation that nerve injuries are complex and that injury patterns can vary across fascicles, Mackinnon added a VI degree (mixed injury) to describe this scenario. 8
In most modern nerve injury classification tables, Sunderland I degree nerve injuries are commonly known only as demyelinating lesions. However, in chapter 9 of his textbook, he refers to I degree injuries more generally as “conduction loss” which can be ischemic non-demyelinating but emphasizes the progression to a demyelinating lesion. However, chapter 6 of his textbook extensively reviews the concept of ischemic “conduction block” and differentiates between three “categories” which are transient ischemic block, acute block, and chronic block. More specifically, in category 3 chronic conduction block, the chronic ischemic block is described as a persistent stationary block that keeps the nerve in “suspended animation” until the cause is removed. 7 A classic example of dynamic ischemia would be a patient with carpal tunnel syndrome with nocturnal paresthesias that immediately reverse with shaking of the wrist or the use of night splints. However, as Sunderland described in his textbook, chronic ischemic block can also occur. 9 These patients present with normal electrodiagnostic (EDX) studies but complaining of pain and paresthesias that resolve almost immediately after decompression—too quickly to be considered remyelination.
This atypical presentation first came to our attention when observing that some patients with foot drop unexpectedly regained dorsiflexion in the recovery room after a common peroneal decompression (CPD). 9 Furthermore, these patients also had essentially normal preoperative EDX studies and were often turned away from other practitioners who were hesitant to operate on a patient without objective findings. Looking back to a previous retrospective review of 185 patients who underwent CPD from 2011 to 2017, we saw that out of the 99 patients with clinically overt footdrop, 10.1% had normal motor NCS and 12.1% had normal sensory NCS preop. 10 It became clear that this degree of nerve injury had been there all along and it simply needed to be recognized as a separate entity. We colloquially called it the “miracle” or “sleeping beauty” classification and observed this ischemic block in action by watching as epineurial microvessels reperfuse through the zone of injury before our eyes intraoperatively during a decompression. Thus, given the unique clinical presentation and recovery of patients with ischemic conduction block, we coin the term and refer to ischemic non-demyelinating injuries as Sunderland 0 “zero” degree injuries. 9
The recent emphasis on the importance of understanding the utility and the interpretation of electrodiagnostic studies with respect to traumatic nerve injuries has allowed expansion of the use of Sunderland's classification.11–14 Sunderland II degree injuries are defined by partial axonotmesis with a variable number of intact axons capable of collaterally sprouting into adjacent motor end plates. This is identified by early motor unit action potentials (MUAPs) on EDX by 3 months and predicts complete spontaneous recovery. Sunderland III degree injuries have more severe axonotmesis which leads to later presentation of MUAPs on EDX (>4 months) and limited final spontaneous recovery depending on the time, distance of injury, and subsequent changes in the neural pathway and end target receptors. 11 This paper revisits the classification of nerve injuries based on Sunderland's framework with the addition of Sunderland 0 and VI (Figures 1 and 2). Each grade of nerve injury is reviewed with a case example and accompanying electrodiagnostic findings. Finally, we present a simplified classification that is patient and physician oriented, reflecting prognosis, time to recovery, and degree of recovery (Table 1).
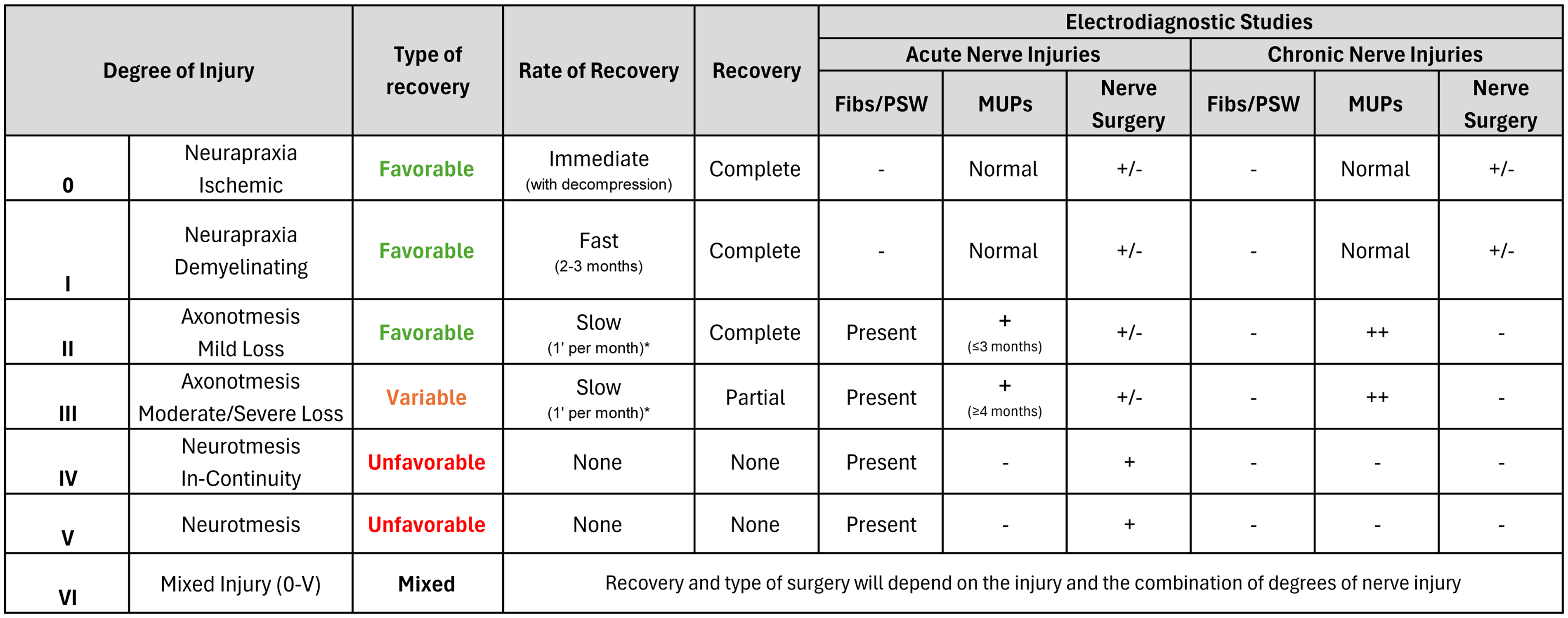
Classification of nerve injuries, electrodiagnostic findings, and expected recovery. We suggest that a simpler classification of nerve injury based on the rate and degree of recovery would be helpful for patients, trainees, and non-nerve surgeons. For example, favorable injuries have potential for complete recovery without surgical intervention or with decompression immediately (Sunderland 0), fast (2 months, Sunderland I), or slowly (an inch per month, Sunderland II). Axonotmetic injuries could also result in variable but not normal recovery slowly (Sunderland III) and are often treated with decompression and end-to-side nerve transfers to augment the final outcome. Neurotmetic injuries are unfavorable with no recovery anticipated (Sunderland IV, V) and require surgical intervention in the form of grafting and/or end-to-end nerve transfers. Lastly, all of the above can present simultaneously to varying degrees in mixed injuries (Sunderland VI).
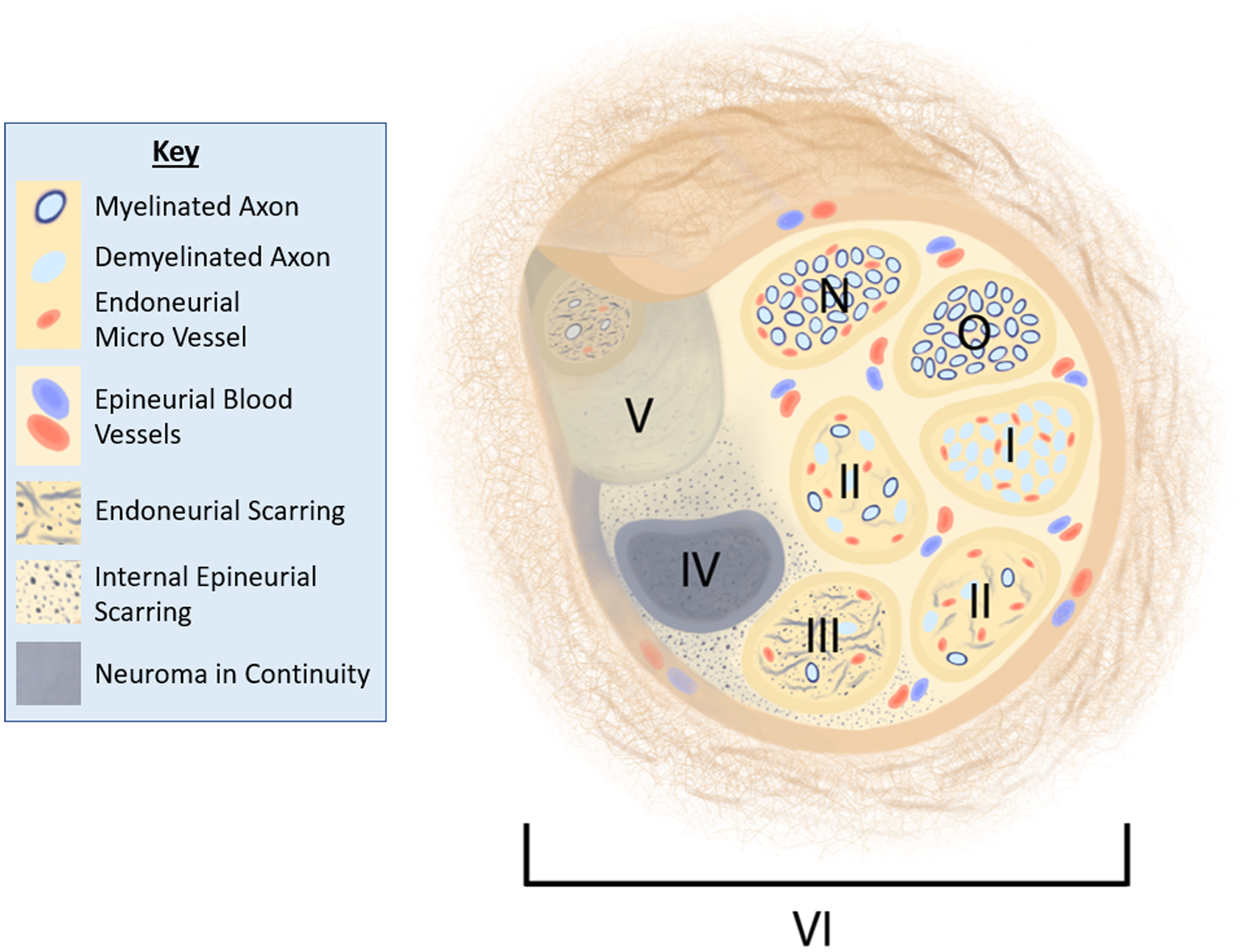
Cross-section of a peripheral nerve with each grade of nerve injury depicted in separate fascicles. Fascicle N at the top of the image represents a normal fascicle. Moving in a clockwise direction, fascicle 0 demonstrates a Sunderland 0 nerve injury with loss of endoneurial perfusion due to ischemic block. Fascicle I represents a Sunderland I degree demyelinating neurapraxia. Fascicles II represent a Sunderland II degree partial axonotmesis with varying degrees of axonal loss and endoneurial scarring. Fascicle III represents a Sunderland III degree severe axonotmesis with minimal to remaining intact axons, more profound endoneurial scarring, but intact perineurium. Fascicle IV represents and Sunderland IV degree neuroma in continuity with injured perineurium and complete scar block. Fascicle V represents a Sunderland V degree neurotmesis. The entire image represents the variable complexity of a mixed VI degree injury.
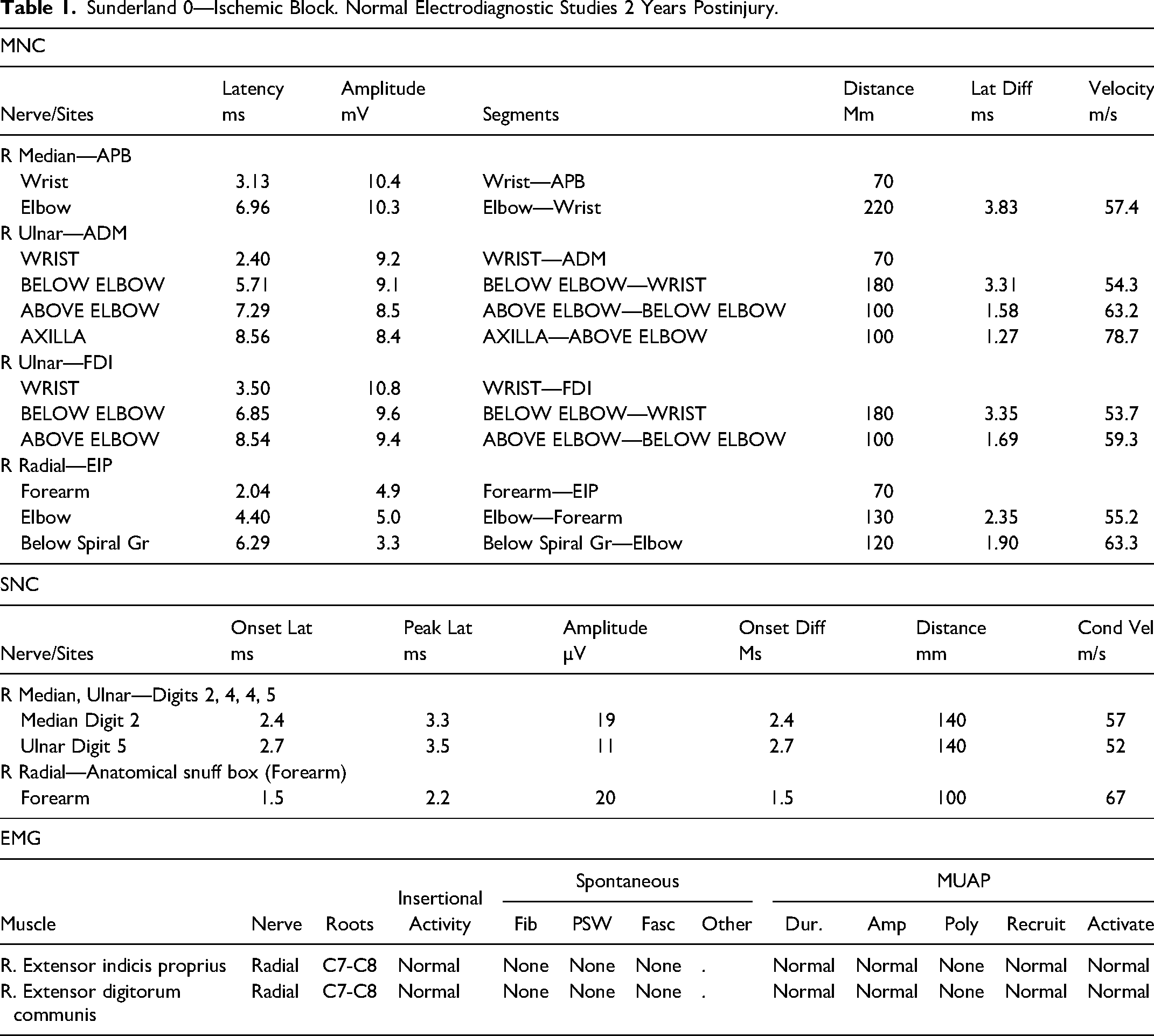
Sunderland 0—Ischemic Block. Normal Electrodiagnostic Studies 2 Years Postinjury.
Clinical Vignettes
Sunderland 0—Ischemic Block
A 55-year-old female presented with right dorsal forearm pain and weakness in her radial nerve. Two years prior, she had a motor vehicle accident that resulted in a crush injury to her right forearm. She did not sustain any fractures or undergo any surgical intervention. She did have significant bruising at that time, and her symptoms started immediately after her accident. On examination, she had preserved radial nerve sensation, Medical Research Council (MRC) grade 3/5 strength in her wrist and finger extensors, and pain with resisted wrist extension and resisted supination. She had tenderness, a positive Tinel sign, and a sensory collapse test15–18 which localized to the posterior interosseous nerve (PIN) entrapment point at the arcade of Frohse.
Her EDX was normal with preserved compound motor unit action potential (CMAP) and sensory nerve action potentials (SNAP) of her radial nerve and a normal electromyogram (EMG) (Table 1).
She underwent a right PIN decompression. By her next visit on the second postoperative day, she had recovered 4/5 radial nerve strength and she stated her pain had improved significantly. She went on to recover full 5/5 strength by her 6-week postoperative visit.
This is an example of a Sunderland 0 nerve injury which is defined by symptomatic dynamic or persistent ischemia with normal EDX studies. Reversing the ischemia by decompressing the PIN led to nearly immediate recovery of function and improvement in pain.
Sunderland I—Neurapraxia
A 50-year-old female presented with weakness, decreased sensation and pain in the left ulnar nerve distribution after a fall from standing height 4 months prior where she sustained a left radial head fracture requiring an open reduction and internal fixation via a lateral approach. Postoperatively, she developed pain and paresthesias in the ulnar nerve distribution along with ulnar weakness in the left hand. On examination, she had 3/5 strength in flexor carpi ulnaris (FCU), flexor digitorum profundus to the small finger (FDP-SF), and the ulnar intrinsic muscles. Her Semmes–Weinstein monofilament testing revealed a sensation threshold of 4.31 in her ulnar nerve distribution, consistent with diminished protective sensation. She had a positive Tinel sign and sensory collapse test at her left cubital tunnel with negative provocative testing at Guyon's canal.
The EDX demonstrated a decreased conduction velocity above and across her elbow along with a conduction block. This was evidenced by a reduced CMAP by more than 50% of the abductor digit mini (ADM) and first dorsal interosseous (FDI) muscles above and across the elbow on the motor nerve conduction studies with normal CMAPs at the wrist and forearm. Her ulnar SNAP was mildly reduced, and her EMG was normal (Table 2).
Sunderland I—Neurapraxia. Demyelinating Conduction Block 4 Months Postinjury.
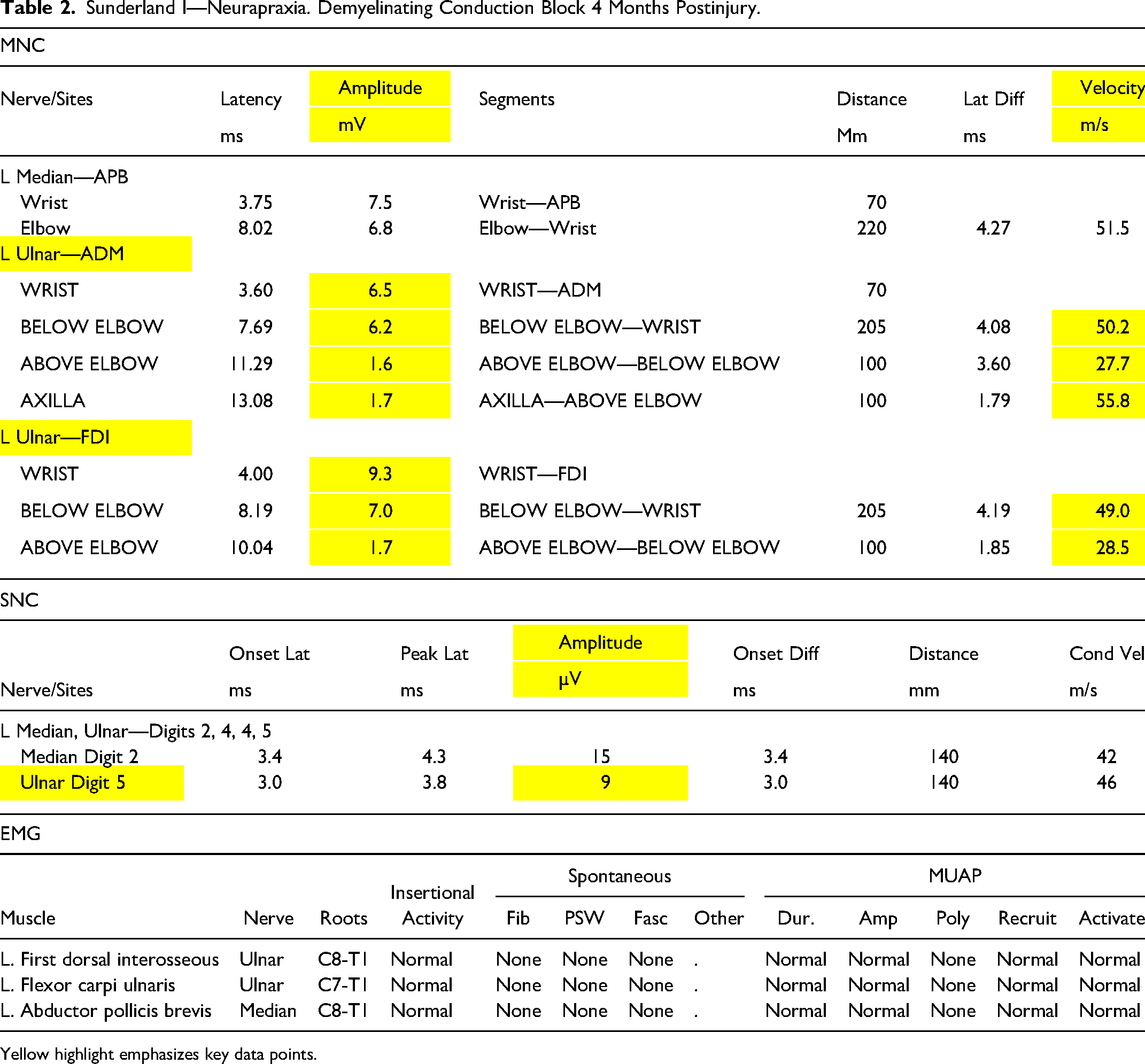
Yellow highlight emphasizes key data points.
She underwent a left ulnar nerve release and submuscular transposition of the ulnar nerve. Her pain and paresthesias improved within 2 days postoperatively. Her ulnar extrinsic and intrinsic weakness and sensory deficit improved 2 months following surgery.
This is an example of a Sunderland I degree injury which is defined by a demyelinating neurapraxia. The preoperative EDX demonstrated a conduction block with reduction of the FDI and ADM CMAP values when measured across the elbow. Decompression allows for remyelination and complete recovery in a 2- to 3-month time frame. The immediate improvement in pain and parasthesias implies a component of a Sunderland 0 injury.
Sunderland II—Axonotmetic Injury
A 14-year-old male presented with a 3-month history of left upper extremity ulnar weakness and decreased ulnar sensation after sustaining distal radial and ulnar shaft fractures from a fall. He underwent open reduction and internal fixation of both fractures. Postoperatively, he developed diminished left ulnar sensation and loss of intrinsic muscle function with an ulnar claw hand. On examination, he had clawing with intrinsic atrophy, and normal FCU and flexor digitorum profundus to the small finger (FDP-SF) strength. He was unable to cross his fingers and he had 1/5 intrinsic muscle strength. He reported 4/10 sensation in his left ulnar nerve distribution as compared to his right. He had a positive Tinel's sign and sensory collapse test at his left Guyon's canal.
His EDX obtained at 3 months postinjury demonstrated no response in motor nerve conduction of his ulnar nerve and a decreased sensory conduction velocity in his ulnar nerve. On EMG, he had fibrillations and positive sharp waves of his left ADM and FDI along with a single MUAP in his FDI and mildly reduced recruitment and nascent MUAPs present in his ADM (Table 3).
Sunderland II—Axonotmetic Injury. Single Motor Unit Action Potential 3 Months Postinjury.
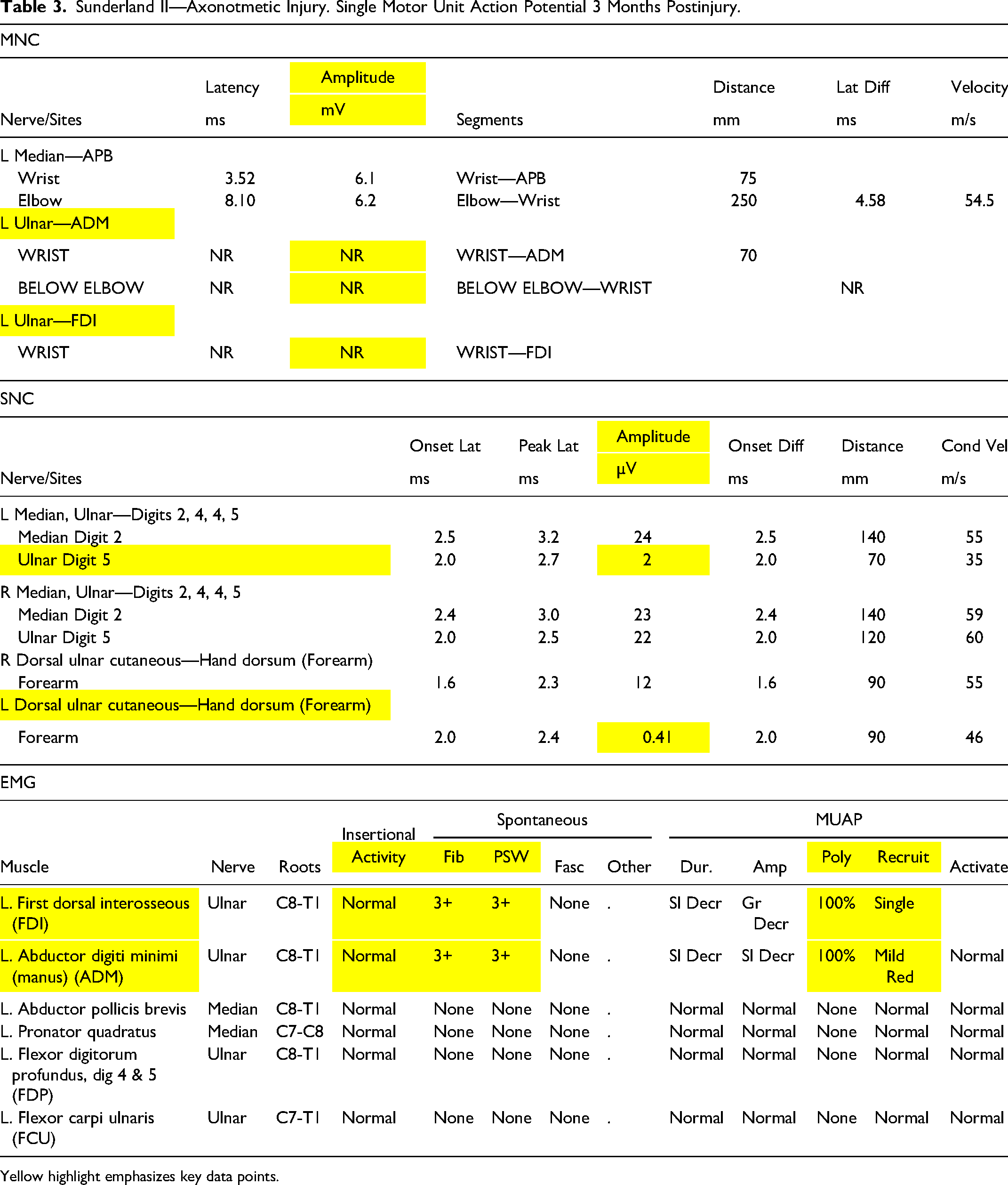
Yellow highlight emphasizes key data points.
He underwent a left Guyon's canal release and his sensation and intrinsic function fully recovered within 9 months.
This is an example of a Sunderland II degree injury which is defined by severe but partial axonal loss. The presence of even a single MUAP at 3 months suggests that enough normal axons remain intact to collaterally sprout to reinnervate adjacent denervated motor end plates and increase force 5×.19,20 We call this the critical plateau for functional recovery (CPR) (Fig. 3). This collateral sprouting and subsequent regeneration of injured axons (nascent axons) combine to provide enough innervated muscle for normal or near normal function at recovery. Given that this injury localized clinically to Guyon's canal, a known area of nerve entrapment, a decompression was performed to maximize the recovery of any associated Sunderland 0 or I degree superimposed compression.
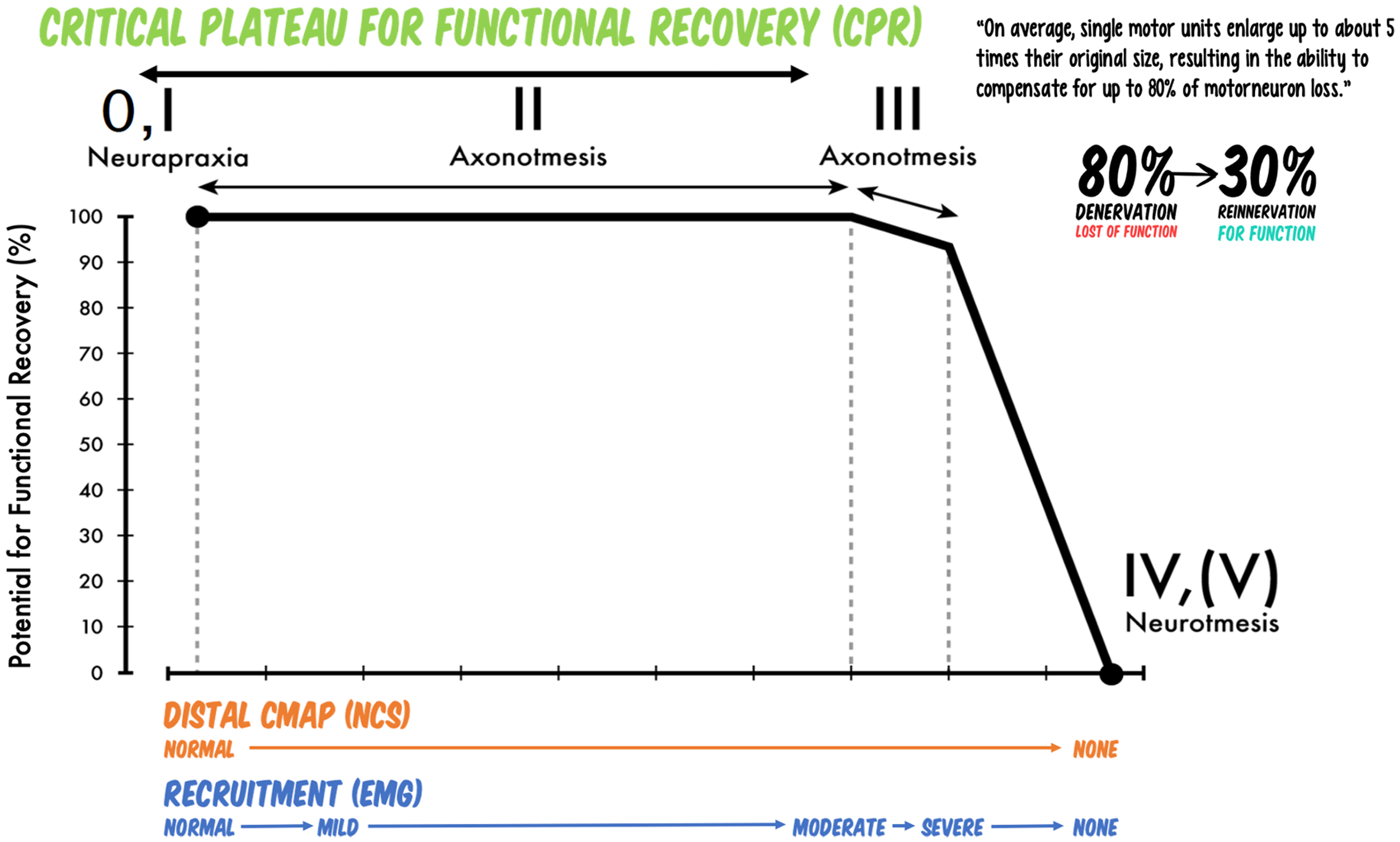
A representation of the critical plateau for functional recovery (CPR). Muscles will maintain normal functional contraction strength with up to 80% denervation as the remaining MEPs are recruited more rapidly to generate up to 5× as much force. When over 80% of the axons are lost, there is a rapid drop in functional strength as the muscle essentially “falls off the cliff.” This can be correlated to Sunderland grades of nerve injury with Sunderland III degree axonotmetic injuries representing the edge of the cliff before collateral sprouting alone will not restore normal function. Supercharge end-to-side nerve transfers are utilized in this situation to supplement enough additional axons to bring the muscle “up the cliff and on to the functional plateau.”
Sunderland III—Severe Axonotmetic Injury
A 21-year-old male presented with right shoulder pain, weakness, and numbness after an injury 8 months prior when a forklift fell onto his right shoulder. He did not sustain any fractures or dislocations. On examination, he had right deltoid atrophy with decreased 3/5 shoulder abduction strength. He had no numbness in the lateral upper arm. He had tenderness over his quadrangular space and pain with the positional provocative test (starting with the shoulder flexed at 90° and the elbow fully extended, the elbow is flexed to 90° first, and then the humerus is internally rotated to provoke tightness of the long head of the triceps and teres minor, respectively, at the quadrilateral space).
Review of his first EDX obtained at 3 months showed no MUAPs in the deltoid and teres minor. His current EDX when he presented at 8 months demonstrated fibrillations and positive sharp waves along with nascent MUAPs in all three portions of the deltoid and the teres minor (Table 4).
Sunderland III—Severe Axonotmetic Injury. Nascent Regeneration 8 Months Postinjury.
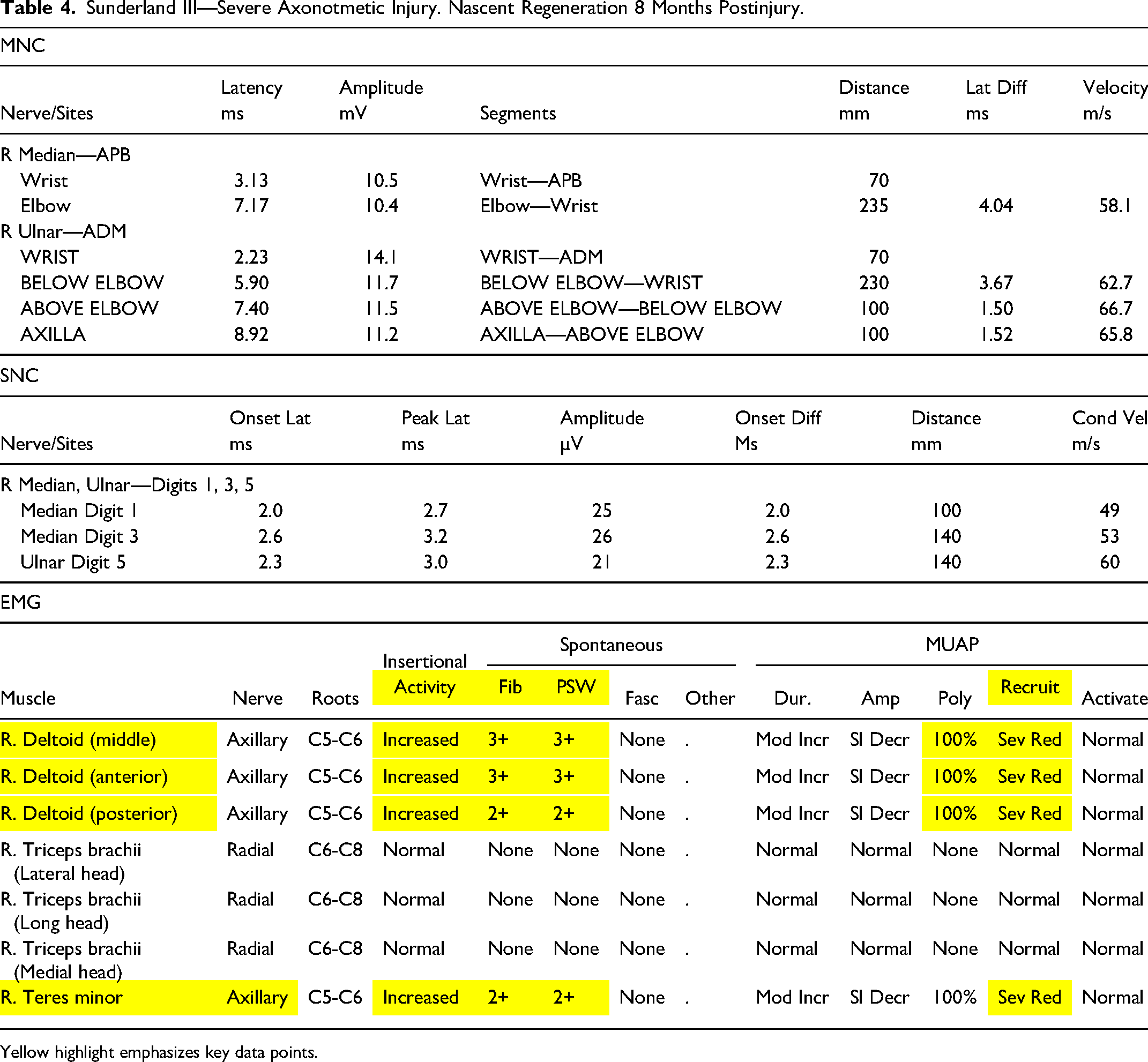
Yellow highlight emphasizes key data points.
The patient underwent an axillary nerve decompression and supercharge end-to-side nerve transfer of the medial triceps nerve to the axillary nerve with step lengthening of the long head of the triceps tendon. 21 He achieved 5/5 deltoid strength 1 year postoperatively.
This is an example of a Sunderland III degree injury which is defined by a severe axonotmetic injury. Very few axons remain in continuity for collateral sprouting and as a result, EDX at 3 months shows no MUAPs. Later EDX identifies nascent regenerating native injured axons (ie original injured axons regenerating, not collateral sprouting), but these are not sufficient for full clinical recovery due to the fall off the critical plateau (Figure 3). In order to optimize and maximize the recovery, the axillary nerve was decompressed and supercharged with an end-to-side nerve transfer.
Sunderland IV—Neuroma-in-Continuity
A 75-year-old, morbidly obese female presented 9 months after a fall from a 4-ft height resulting in a closed right lateral malleolus fracture which was treated nonoperatively in a cast. She was noted to have a right foot drop along with numbness in her superficial peroneal nerve (SPN) distribution after cast removal. On examination, she had 0/5 ankle eversion and dorsiflexion. She had a positive Tinel's sign and sensory collapse test of her right common peroneal nerve (CPN) at the fibular head.
Her EDX at the time of presentation demonstrated no response of her right extensor digitorum brevis and tibialis anterior muscles CMAPs (note: peroneal SNAPs of NR can be unreliable given temperature and the smaller amplitude of SNAPs vs CMAPs). On EMG, both the tibialis anterior muscle and peroneus longus muscles had fibrillations and positive sharp waves but no MUAPs. Tibial innervated muscles were normal (Table 5). Although no previous EDX was available to compare, the severity of the findings on the 9-month EDX are sufficient to prognosticate this patient to a Sunderland IV classification where no spontaneous recovery is expected.
Sunderland IV—Neuroma-in-Continuity Neurotmetic Injury. No Motor Unit Action Potentials 9 Months Postinjury.
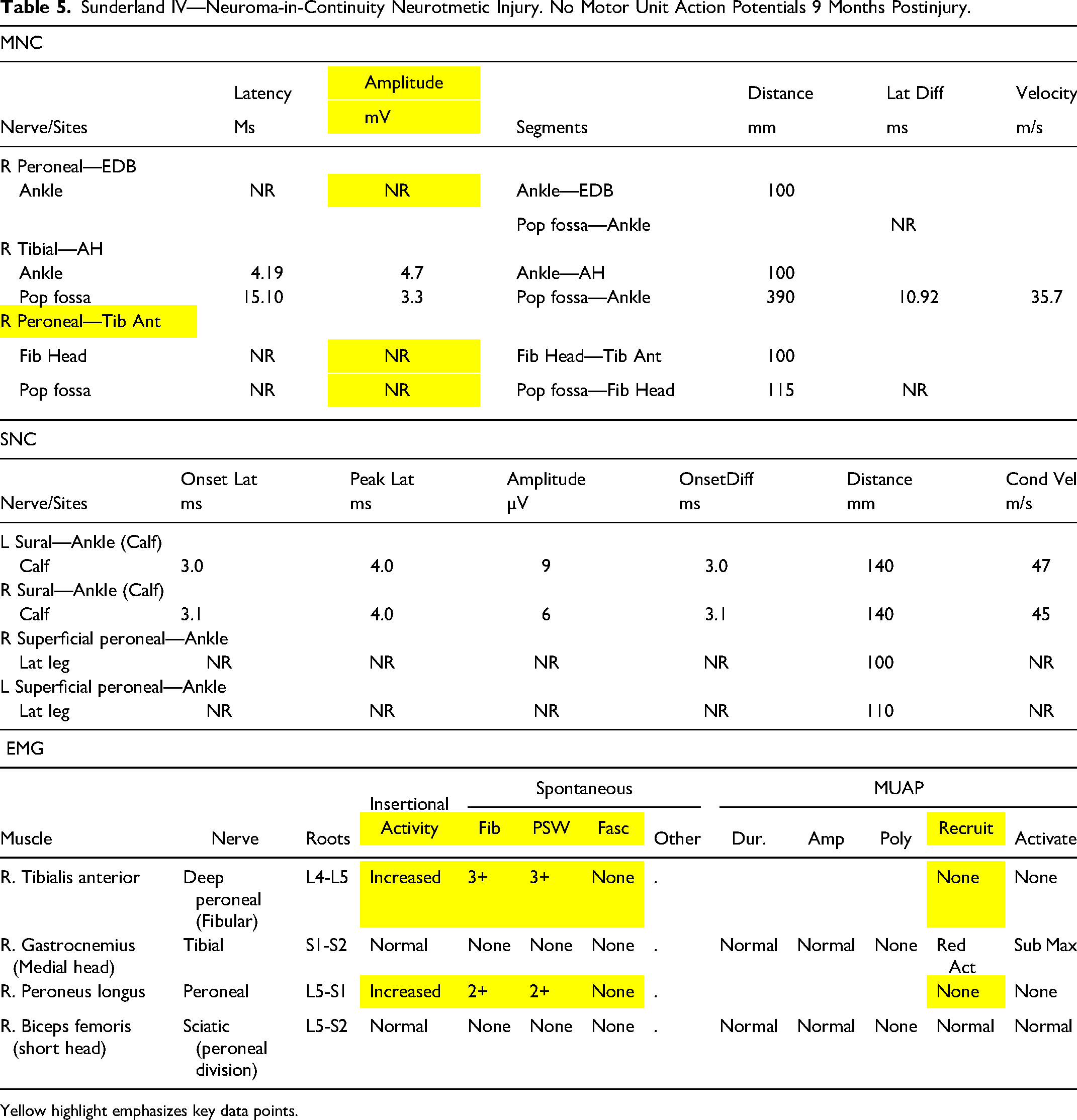
Yellow highlight emphasizes key data points.
She underwent a right CPN release and the nerve was noted to be firm and scarred for a distance of 9 cm. Postoperatively, her pain improved significantly, but her foot drop persisted. She remained compliant with her ankle foot orthosis and elected for a posterior tibial to anterior tibial tendon transfer 1 year later.
This is an example of a Sunderland IV degree nerve injury which is defined by a complete neurotmetic injury with the nerve in continuity. This is supported on the EDX by a lack of SNAPs or CMAPs, and presence of fibrillations and positive sharp waves without any MUAPs at 9 months. The patient was not a candidate for nerve grafts and thus only a decompression was performed given the extensive length of the injury and time since injury. Due to the degree of the nerve injury, no recovery was achieved, and a tendon transfer was done secondarily to restore dorsiflexion. Had she presented sooner, a 3- to 4-month EDX would likely have warned of the injury severity. She would have been counselled on the likely need for surgical intervention and then followed with another EDX at 5 to 6 months. At this point it would have been evident that no spontaneous recovery is expected, and she could have been offered nerve grafting and/or a nerve transfer to reconstruct her common peroneal deficits. 11
Sunderland V—Neurotmetic Injury
A 65-year-old female presented 6 weeks after sustaining a stab wound to the right medial elbow with complete loss of ulnar nerve function. On examination, she had atrophy of the ulnar intrinsic muscles. She had 0/5 FCU, FDP-SF, FDI and ADM strength. She had a positive Froment's sign and a strong Tinel's sign was present posterior to the medial epicondyle over her laceration. Her Semmes–Weinstein monofilament testing was unresponsive to a filament diameter of 6.65 in the right ulnar nerve distribution.
Her EDX obtained 6 weeks postinjury demonstrated no response on motor or sensory nerve conduction study of the ulnar nerve. On EMG, her FCU, FDI, and ADM had fibrillations and positive sharp waves without any MUAPs (Table 6).
Sunderland V—Neurotmetic Injury. Complete Loss of all Ulnar Function 6 Weeks Postinjury.
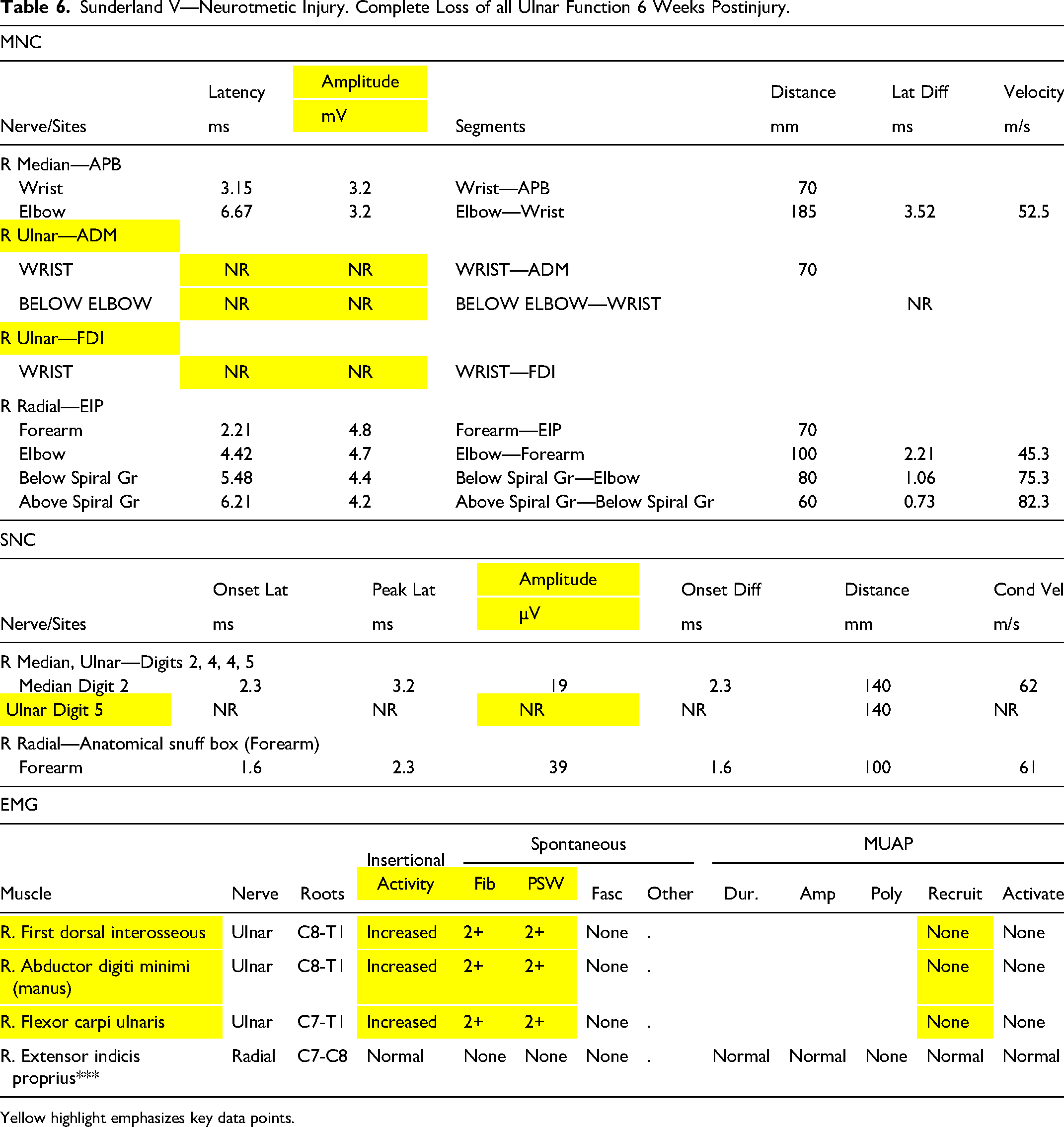
Yellow highlight emphasizes key data points.
During surgery, she was found to have a completely transected ulnar nerve at her elbow. She underwent an ulnar nerve repair with medial antebrachial cutaneous nerve grafts, submuscular transposition, FDP tenodesis, Guyon's canal release, anterior interosseous nerve supercharge (AIN) and ADM turbocharge end-to-side nerve transfers, along with median to ulnar cross-palmar sensory nerve transfers with nerve allograft.22,23 She recovered 4/5 FDI strength by 1.5 years postoperatively along with protective sensation.
This is an example of a Sunderland V degree nerve injury which is defined by complete nerve transection. The sharp mechanism and high suspicion for nerve laceration prompted immediate exploration at the time of referral. Due to the distance required for nerve regeneration from the site of the injury, the nerve repair was supplemented with supercharge/turbocharge end-to-side nerve transfers (SETS) distally.
Sunderland VI—Mixed Injury
A 40-year-old female presented 5 months after a horse stepped on and fractured her right humerus. She had an immediate loss of radial nerve function. At surgery for open reduction and internal fixation of the humerus, her radial nerve was noted to be intact. On examination, she had 5/5 triceps and brachioradialis function, but no distal radial nerve function. A positive Tinel's sign was present at the radial tunnel.
Her EDX showed no sensory or motor NCS response of her radial nerve. On EMG, her triceps and brachioradialis were normal. Finger and wrist extensors had fibrillations and positive sharp waves with regenerative MUAPs (Table 7).
Sunderland VI—Mixed Injury. Variable Findings 5 Months Postinjury.
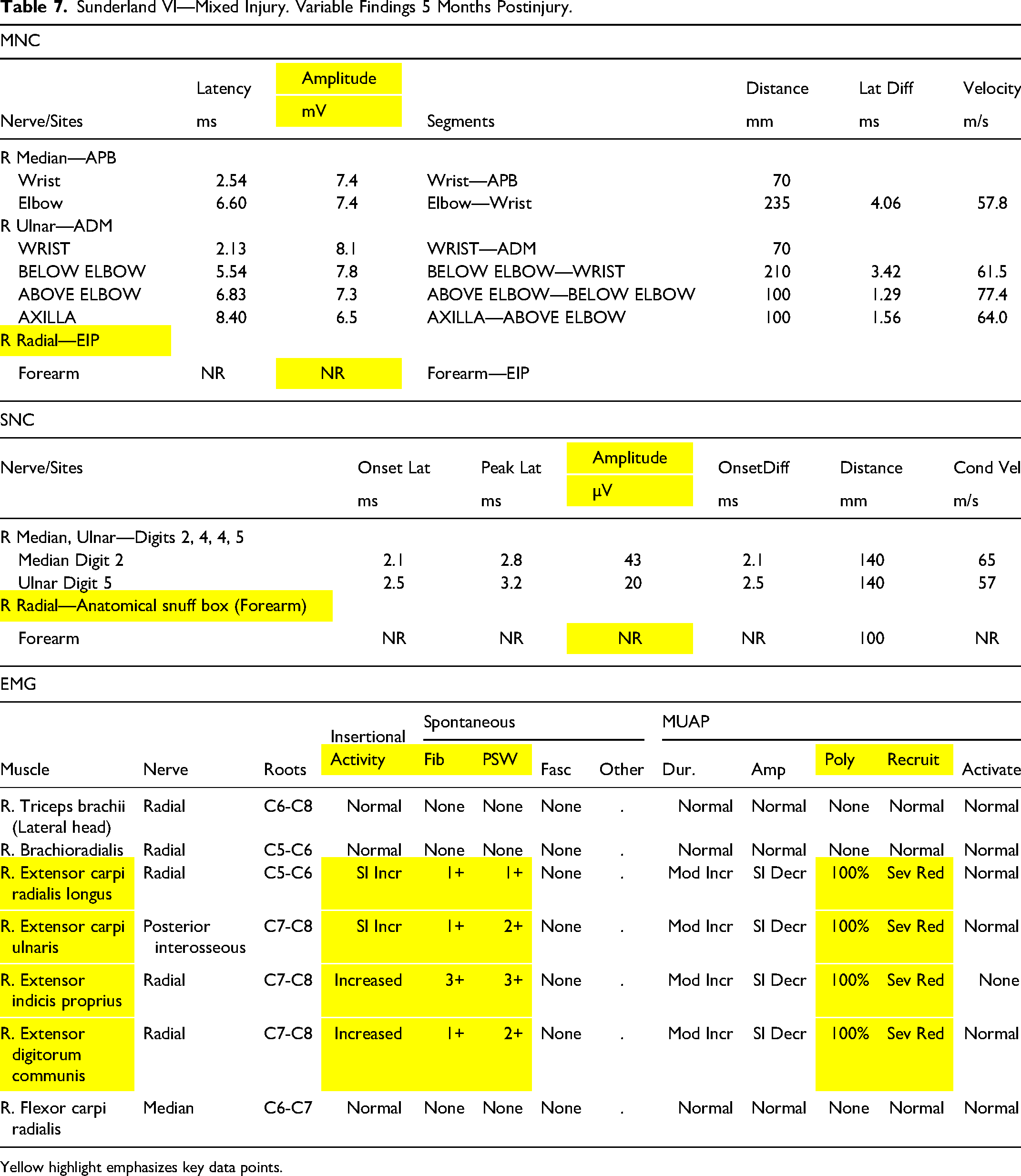
Yellow highlight emphasizes key data points.
The patient underwent a right PIN release and end-to-side supinator to PIN transfer. At her 2-week postoperative appointment, her pain had improved, and she had 1/5 wrist extension, 2/5 extensor pollicis longus (EPL) and extensor digitorum communis (EDC) muscle strength. At 2 months postoperatively, her motor strength improved to 3+/5 in wrist, finger and thumb extension. She eventually recovered full radial nerve motor function and normal radial nerve sensation 1.5 years after surgery.
This is an example of a Sunderland VI degree injury which is defined by a mixed injury and therefore variable timing of recovery. In this case, pain and PIN motor function improved by the first postoperative visit which corresponds to the Sunderland 0 component of the mixed injury evidenced by near immediate partial recovery after decompression and reversal of the ischemia. Further continued improvement and recovery at 2 months postoperatively is indicative of a component of Sunderland I degree demyelination neurapraxia. It is too early at this stage to attribute the recovery to the supinator nerve transfer. Lastly, there was also a significant element of Sunderland III degree injury based on the active denervation and minimal MUAPs at 5 months. This continued to recover through both nascent axonal regeneration and via the supercharge end-to-side nerve transfer over a year.
Conclusion
Seddon and Sunderland's original nerve injury classification systems have stood the test of time over the last 70 years and continue to be widely used today. However, since those original descriptions, knowledge of nerve pathophysiology and healing has advanced, electrodiagnostic results have become more refined, and surgical options have increased to include nerve grafting, use of allografts, nerve transfers (both end-to-end and end-to-side), among many other novel techniques.8,11,24–28 As a result, some of the limitations of the original classification system are coming to light. These limitations include the lack of a category for predemyelination ischemia, as well as the previously recognized lack of a category for mixed injuries where individual fascicles have variable injury severity (Sunderland VI).8,9
Importantly, we emphasize that blood flow and ischemic block are not identified by EDX but can impede recovery at known areas of nerve entrapment. It is well established that the pathophysiology of nerve compression starts with ischemia, progresses to edema and breakdown of the blood nerve barrier, advances to demyelination, and lastly results in axonal loss. 29 The current widely used Sunderland classification system skips the initial ischemic stage and begins at demyelination (despite the fact that Sunderland thoroughly discussed these concepts in his textbook). By recognizing a patient population that does not fit into Sunderland I-V, we propose a predemyelination category. Given that these patients will by definition have normal EDX findings, we accentuate the power of clinical examinations, using pressure, positional and other provocative tests (Tinel and Sensory Collapse Test). 15 We coin this Sunderland 0 injury.
We also highlight the variability of axonotmetic Sunderland II degree injury as relating to the number of uninjured axons available for collateral sprouting to reinnervate denervated neuromuscular junctions in a timely fashion, to either facilitate recovery on their own with very mild II injuries (physiological nerve transfer) or with the eventual assistance of additional proximal native injured axons regenerating over time to provide in sum the critical number of axons (>30%) to reach the threshold for normal function (II) or partial function (III).11,19
We offer a revisited review of the nerve injury classification to incorporate this new knowledge for the modern era of nerve surgery. By following this nerve injury framework, and our previously published algorithm for managing nerve injuries using EDX, 11 clinicians can better assess, prognosticate, and manage patients. 11
Supplemental Material
Footnotes
Author Contributions
![]() ; made a significant contribution to the concept, design, acquisition, analysis, and interpretation of data; drafted the article or revised it critically for important intellectual content; approved the final version for publication; and agreed to be accountable for all aspects of the work and to resolve any issues related to its accuracy or integrity.
; made a significant contribution to the concept, design, acquisition, analysis, and interpretation of data; drafted the article or revised it critically for important intellectual content; approved the final version for publication; and agreed to be accountable for all aspects of the work and to resolve any issues related to its accuracy or integrity.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was not required.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Barnes-Jewish Hospital Foundation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.