
Abstract

To the Editor,
Mattress sutures remain a core component of surgical skills teaching for medical students and residents. Vertical and horizontal mattress techniques are commonly taught as distinct options, each emphasizing different priorities in wound closure. In routine practice, however, both patterns have recognized limitations, including difficulty achieving consistent dermal apposition without epidermal compression, the risk of track marks, and potential compromise of wound edge perfusion when tension is poorly distributed.1,2
Experimental and clinical studies consistently demonstrate that suture geometry and bite placement influence tissue perfusion, eversion, and wound edge behaviour.1–3 Modifications such as the Allgower Donati stitch have shown improved incisional perfusion compared with vertical mattress closure, 2 and several authors have described hybrid or modified mattress patterns that deliberately combine elements of established techniques to improve eversion, handling, or cosmetic outcome.3–7 Collectively, this literature supports the principle that effective skin closure depends on mattress geometry rather than strict adherence to traditional vertical or horizontal patterns.
In this context, I wish to describe a simple and reproducible technique that I have used for many years and routinely teach to trainees, yet rarely see taught formally. The technique is a 4-bite mattress configuration with deliberately noncollinear puncture points and a longitudinal offset. I refer to it as the Tension distributing, Appositional, Bilayer, Longitudinally offset, Eversion optimizing (TABLE) suture.
The defining feature of the TABLE suture is the deliberate longitudinal offset between the superficial and deeper bites. Two bites are placed further from the wound edge to capture robust dermis and distribute tension. Two additional bites are placed closer to the wound edge but offset along the long axis of the incision to refine epidermal alignment. This geometry differentiates the stitch from a classic vertical mattress, in which paired bites lie on a single perpendicular axis, and from a classic horizontal mattress, in which bites are aligned parallel to the wound. The clinical aim is to achieve reliable dermal contact and controlled eversion while minimizing epidermal compression and preserving edge perfusion (Figures 1 and 2). This approach is consistent with evidence demonstrating that both bite depth and distance from the wound margin influence margin adaptation and tissue behavior.8,9
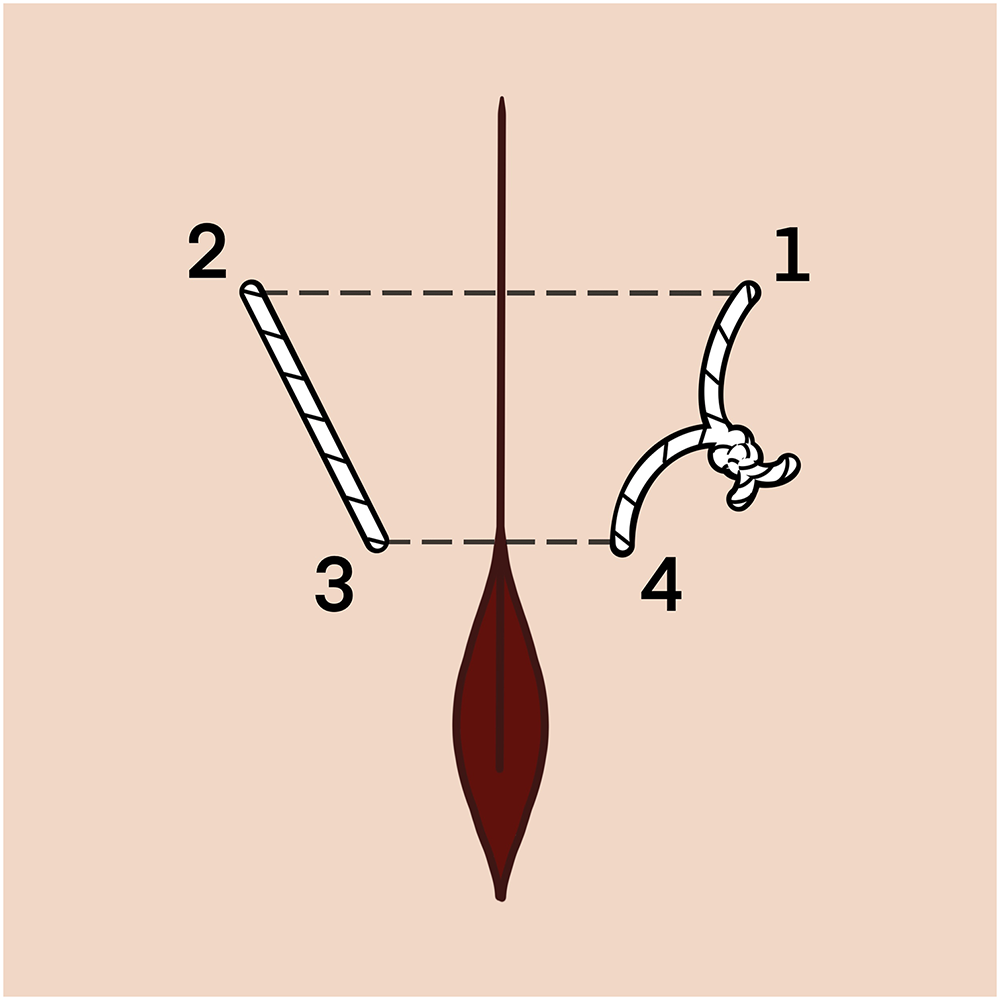
Overhead view of the tension distributing, appositional, bilayer, longitudinally offset, eversion optimizing (TABLE) suture demonstrating 4 puncture points arranged in a noncollinear and longitudinally offset configuration. Two bites are placed further from the wound edges (1 and 2) to provide dermal support and tension distribution. Two bites are placed closer to the wound edges (3 and 4), but offset along the long axis of the incision to refine epidermal alignment. This geometry differentiates the TABLE suture from classic vertical and horizontal mattress techniques.
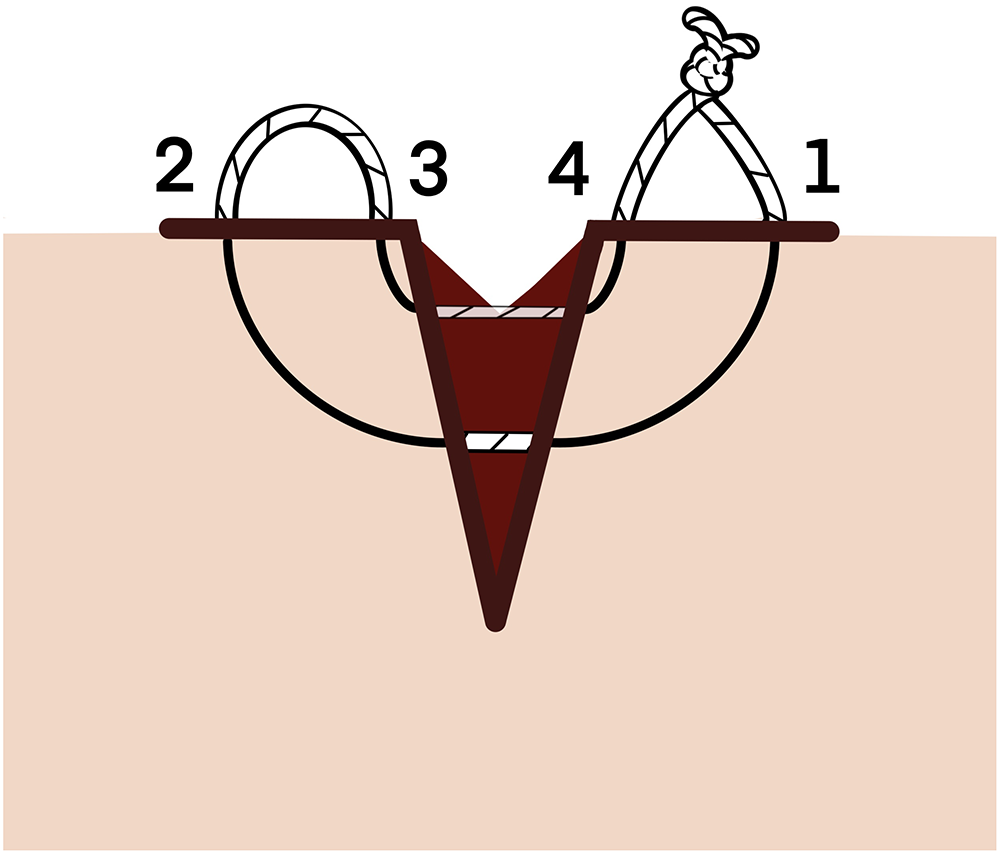
Lateral cross-sectional view of the tension distributing, appositional, bilayer, longitudinally offset, eversion optimizing (TABLE) suture illustrating bilayer capture. Deeper bites (1 and 2) placed further from the wound edge are paired with more superficial bites (3 and 4) placed closer to the edge. The convergent suture path produces controlled eversion and dermal apposition while minimizing epidermal compression and preserving edge perfusion.
Two technical aspects of execution merit emphasis. First, as with well-performed simple interrupted sutures, needle entry should be perpendicular to the skin surface rather than tangential. Vertical entry facilitates predictable dermal purchase, reduces epidermal shearing, and promotes controlled eversion. Tangential insertion, particularly when combined with mattress techniques, risks shallow dermal capture and imprecise epidermal alignment. Second, the needle should be held approximately five-eighths along its length from the tip, rather than close to the swage or end. This grip allows accurate control of curvature, consistent depth of bite, and smooth passage through the dermis. Together, these principles reinforce the TABLE suture as a technique grounded in fundamental closure mechanics rather than compensatory stitch geometry.
From a teaching perspective, the TABLE suture consolidates several core principles of skin closure into a single, intuitive pattern. Trainees are not required to choose between vertical and horizontal mattress sutures, yet retain the advantages that originally justified each. In my experience, the geometry is readily understood when demonstrated visually and produces consistent aesthetic results across a range of wound types.
Two schematic line drawings are provided to illustrate the technique (Figures 1 and 2). An overhead view demonstrates the longitudinally offset, noncollinear puncture geometry, and a lateral cross-sectional view illustrates bilayer capture and controlled eversion. I propose that this technique is well-suited for inclusion in undergraduate and postgraduate skills curricula and merits wider dissemination as a practical alternative to traditional mattress sutures.
Footnotes
Acknowledgments
The author would like to thank Kira Samardziski for the artwork.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.