
Abstract
Introduction
Surgical training, historically characterized by long hours, hierarchical culture, and critical feedback, has been associated with burnout and mental health challenges. Reforms, including duty-hour limits, competency-based education, and initiatives promoting wellness, equity, and psychological safety, have begun reshaping training in Canada. This review provides a national overview of these cultural shifts, mapping recommendations for best practices and research.
Design
A systematic review identified studies on Canadian surgical residency culture. Two reviewers independently screened and extracted data, with risk of bias (ROB) assessed.
Results
Twenty-one studies were included. Key themes were wellness and mental health (19 studies), feedback and learning environments (20), evolving surgical culture (17), equity, diversity, and inclusion (12), duty-hour reforms (14), and international transferability (8). ROB was low in 44.00%, medium in 36.00%, and high in 20.00% of studies.
Discussion
This review of 25 studies highlights evolving themes in Canadian surgical training culture. Traditional endurance-based models are shifting toward inclusivity, wellness, and equity, with increasing attention to mental health, mentorship, and structured feedback. Duty-hour reforms, parental leave policies, and competency-based initiatives indicate generational and structural changes, though implementation varies across programs. Studies emphasize culturally responsive mentorship, psychological safety, and systemic supports to improve learning environments. While Canadian experiences provide valuable insights, differences in legal, institutional, and cultural contexts limit direct transferability internationally. Recommendations include implementing fatigue management plans, mentorship, simulation-based learning, and national coordination to foster a sustainable, learner-centered surgical culture.
Conclusion
Canadian surgical training is evolving through duty-hour reforms, wellness initiatives, and equity-focused policies. While progress has been made, challenges remain in mentorship and cross-provincial consistency.
Introduction
Surgical training has traditionally involved long hours, steep hierarchies, and feedback too often rooted in criticism and shaming.1,2 Once seen as essential for resilience and technical skill, these practices are now linked to burnout, mental health challenges, attrition, and patient safety concerns.3,4
Over the past two decades, structural and cultural changes, including duty-hour limits, competency-based medical education, and initiatives addressing mistreatment and psychological safety, have begun reshaping residency training, although adoption varies by province and program. 2 Among retired American College of Surgeons members, over half (52.4%) wished they had done parts of their career differently, most wanting more family time and prioritizing well-being (23.9%). 5 While studies have examined duty hours and wellness, no synthesis maps broader cultural shifts nationally. The historically paternalistic culture appears to be shifting with increasing focus on diversity, equity, inclusion, and wellness. 4
A systematic review is therefore timely, providing an overview of Canadian surgical training trends from traditional endurance-based models to frameworks emphasizing wellness, equity, and professionalism, mapping recommendations for best practices and future research.
Methods
This review followed the PRISMA guidelines for systematic reviews (Supplementary Figure 1). 6 A search of PubMed, Ovid MEDLINE, and CINAHL was done, from database inception to September 15, 2025, using keywords related to surgical training, residency, wellness, duty hours, equity, and professional culture. Full search strategies are in Supplementary Figure 2. Eligible studies included original research and commentaries on cultural, structural, or policy aspects of surgical residency, including wellness, equity, or learning initiatives. Studies not focused on surgical residency, or the Canadian context, were excluded.
Title and abstract screening, and full-text review, were conducted independently by two reviewers (S.B.AM and R.E.), with disagreements resolved by discussion. Bibliographies were also screened.
Data were extracted using a standardized spreadsheet. One reviewer (S.B.AM
Risk of Bias Assessment
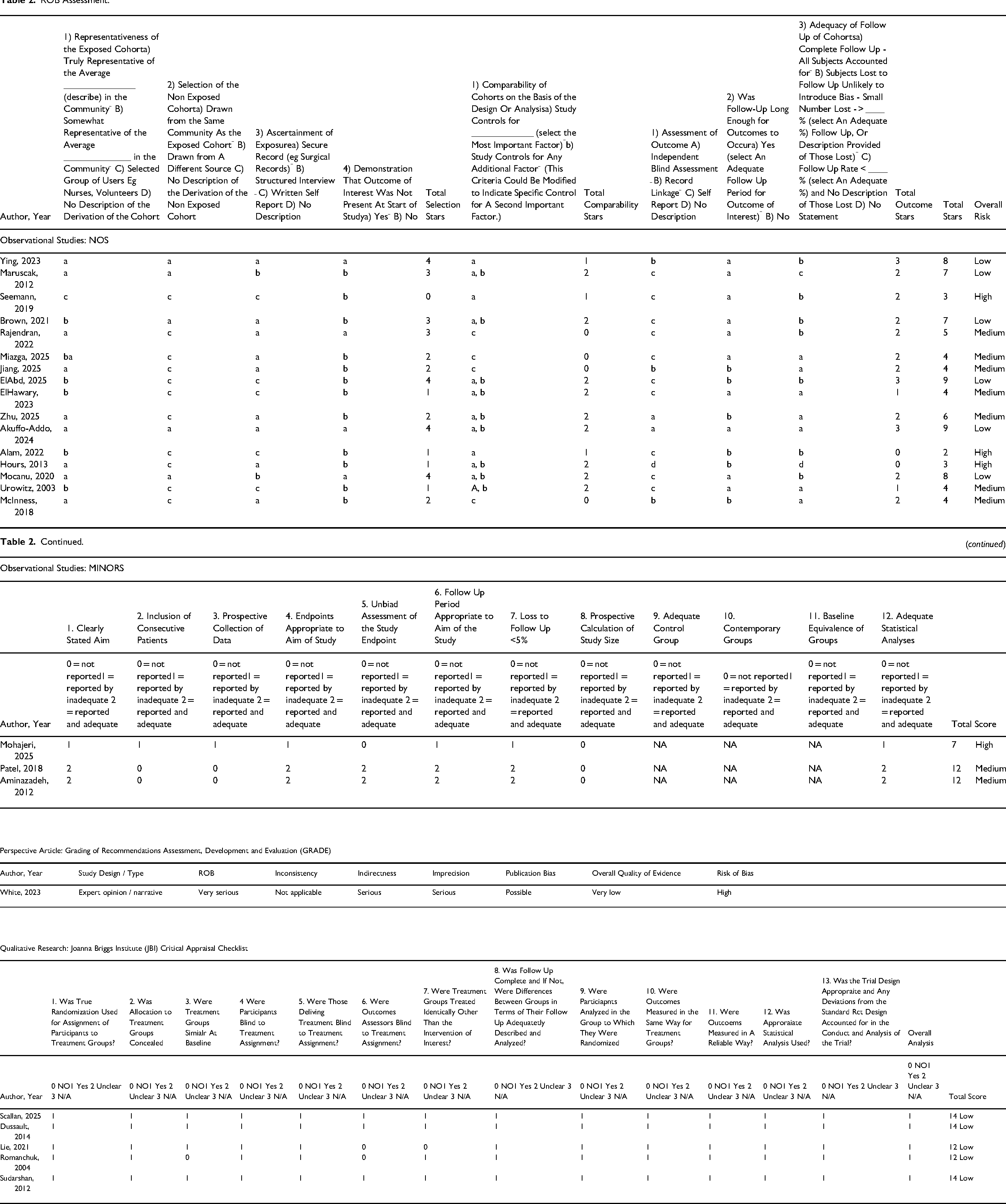
Risk of bias (ROB) was assessed. Observational cohort studies were evaluated using the Newcastle-Ottawa Scale (NOS). 7 Non-randomized observational studies were assessed with the Methodological Index for Non-Randomized Studies (MINORS) tool. 8 Perspective articles were appraised using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. 9 Qualitative studies were evaluated with the Joanna Briggs Institute Critical Appraisal Checklist for Qualitative Research. 10
Results
The search yielded 25 articles (Table 1). A total of 17 articles1,3,4,11-24 examined the evolving definitions of surgical culture from traditional hierarchies towards wellness, inclusion, and mentorship. Eighteen1-4,11,14,16,20-30 focused on duty-hour reforms, including parental leave (n = 7)4,11,14,16,21,24,27 and reduced call hours (n = 9).1,2,4,11,20,21,25,26,28 Wellness and mental health initiatives emerged as a theme in 21 articles1-4,11-22,24-28 with the mention of structured initiatives that address burnout (n = 7)1,2,4,11,19,21,27 and discrimination (n = 5)11,13,16,24,27 through mentorship and mindfulness programs (n = 2).1,19 Thirteen addressed equity, diversity, and inclusion1,2,4,11,13,14,16,19,21,24,25,27,31 mainly by advising the creation of structured mentorship groups (n = 3)11,16,19 and inclusive training (n = 10).1,4,11,13,16,21,24,25,27,31 Feedback and the learning environment were discussed in 24 articles1-4,11-16,18-31 through the discussion of competency-based training (n = 2),23,25 mindfulness (n = 1) 15 and the use of digital learning (n = 2).3,12 Finally, 11 explored global variation and transferability.2,4,14,20,21,24,25,27-29,31 Notably, only one article provided specific recommendations for Canada. 2
Overview of 25 Studies Included in Review.

There has been an increasing trend in the number of published manuscripts over time, with regular yearly publications since implementation of the Royal College Competency by Design: 2003 (n = 1), 30 2012 (n = 3),4,25,29 2013 (n = 1), 2 2014 (n = 1), 26 2018 (n = 2),18,28 2019 (n = 1), 22 2020 (n = 1), 16 2021 (n = 2),3,13 2022 (n = 2),12,19 2023 (n = 3),23,24,27 2024 (n = 1), 11 and 2025 (n = 6).1,14,15,17,21,31 (Figures 1 and 2) A timeline of key moments26,32-35 in the reform of surgical training in Canada is represented in Figure 3.
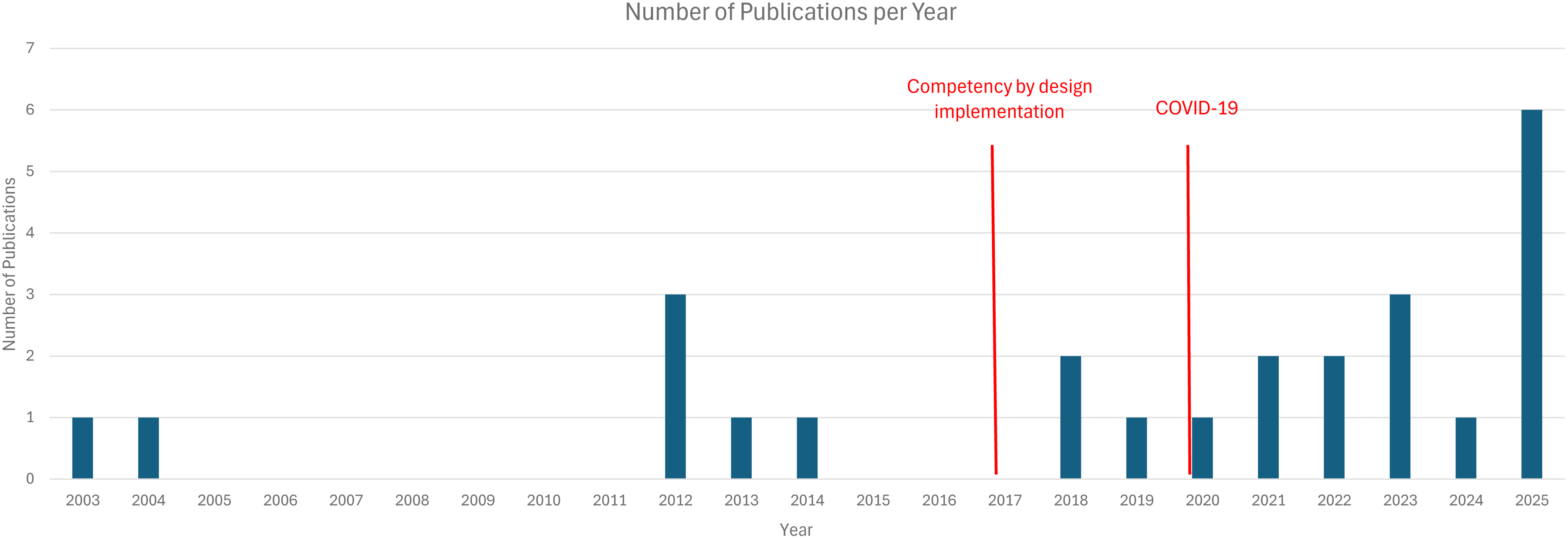
Number of Publications per Year.
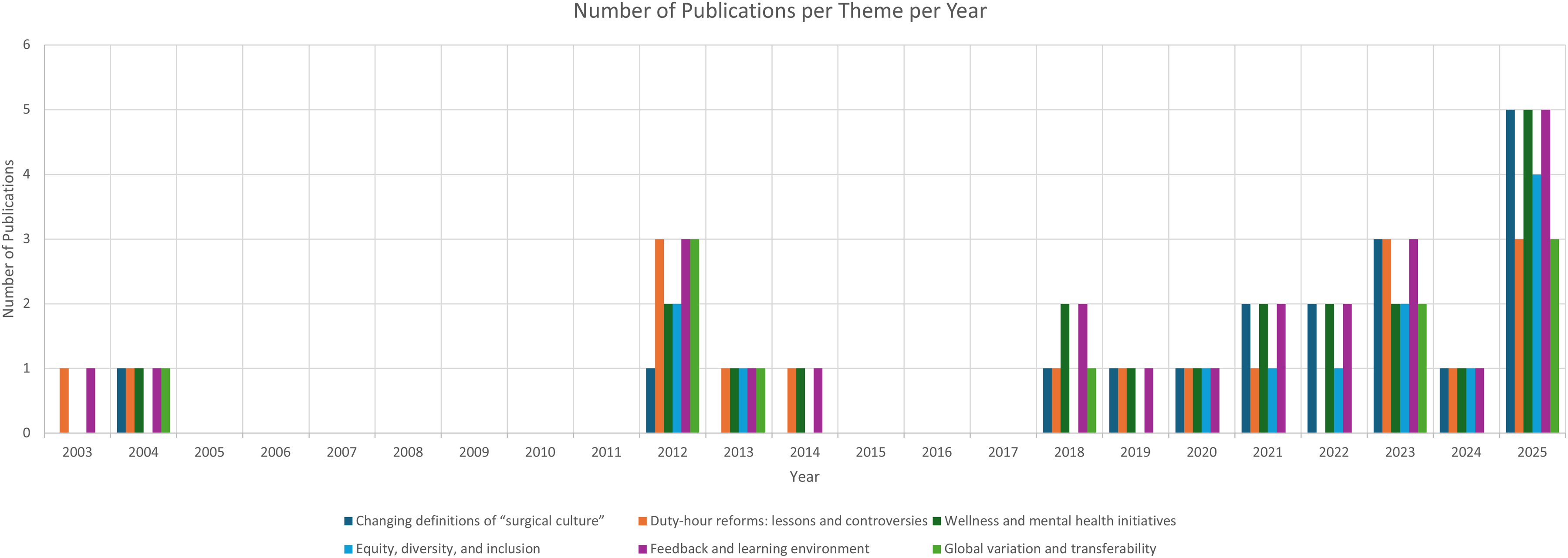
Number of Publications per Theme Per Year.
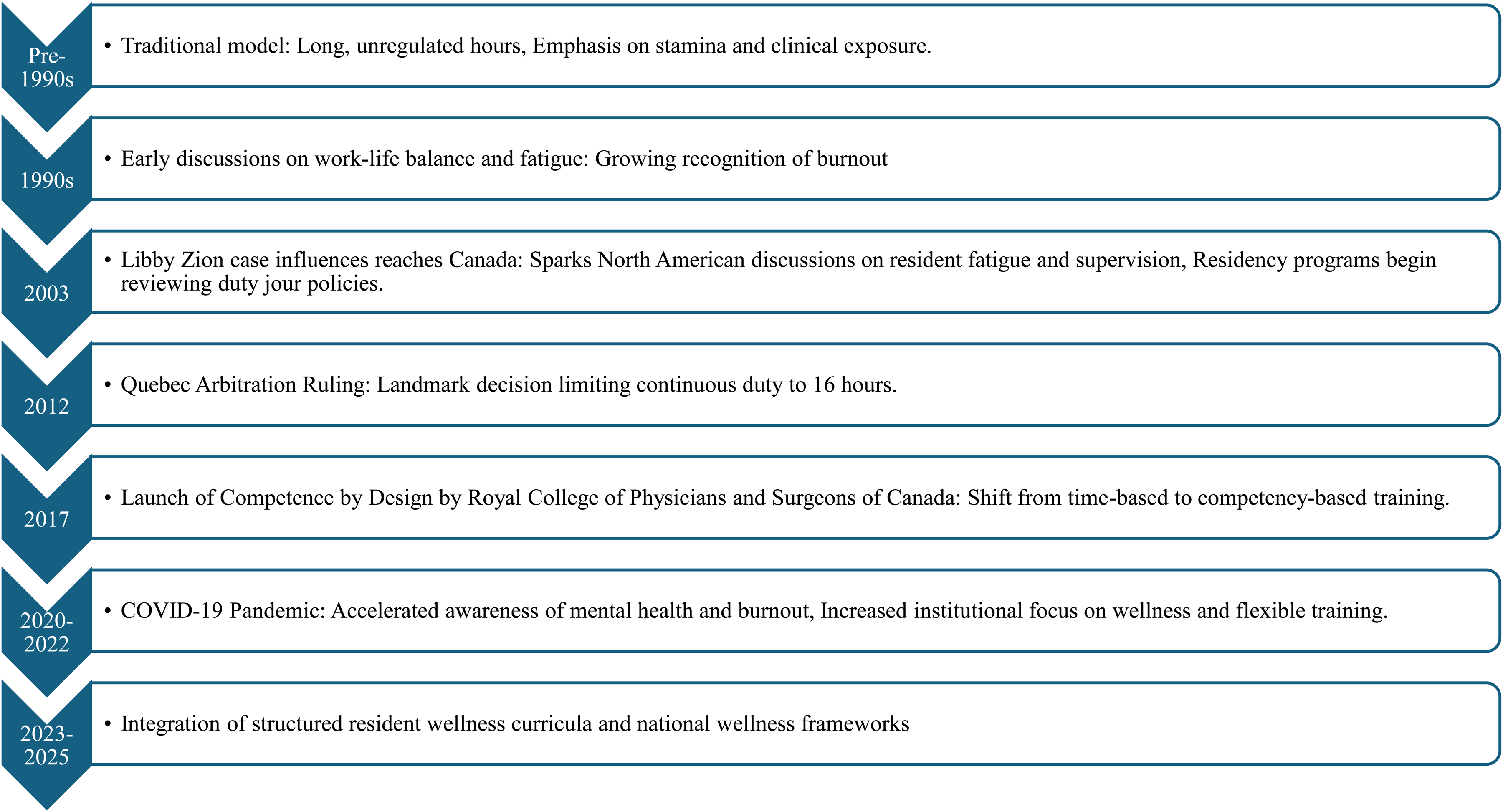
Timeline of Key Events in the Reform of Surgical Training in Canada.
ROB Assessment
For the 16 observational studies evaluated with the NOS, 6 scored as low ROB.14-16,19 However, 5 of these showed medium risk,14,15,19,27,28,30,31 and 3 were flagged for high risk.2,12,22 Three additional observational studies were assessed using the MINORS tool, with 1 17 rated high risk and 218,25 medium risk. One perspective article 23 was evaluated using GRADE and had high ROB. Five qualitative studies assessed with the Joanna Briggs Critical Appraisal tool all scored low risk.3,20,21,26,29 In total, 44.00% (n = 11) studies were low ROB, 36.00% (n = 9) were medium ROB, and 20.00% (n = 5) were high ROB (Table 2).
ROB Assessment.
Discussion
Changing Definitions of Surgical Culture Training
Surgical culture encompasses the shared values, beliefs, and behaviors guiding how surgeons think, act, and interact, emphasizing technical excellence, resilience, hierarchy, and accountability. Historically, training stressed endurance, personal sacrifice, rigid hierarchies, and occasional arrogance, 11 but it is shifting toward collaboration, psychological safety, and coaching-based education. 36 In Canada, surgical culture increasingly emphasizes inclusivity, wellness, and holistic support, with yearly publications since 2017 and a peak in 2025. COVID-19 accelerated this shift: Among 122 residents, reduced in-person teaching and increased free time highlighted alternative educational approaches and resident well-being. 12 UBC's initiatives, including wellness programs, mandatory PPE training, and virtual teaching, emphasized community support. 3
Gender and minority equity are gaining attention. Female residents still report stereotyping. 13 Mocanu found 21% of female minority residents felt unsupported facing discrimination, versus 3% of male non-minority residents. 16 Trends show gradual improvement: Ying observed rising completion rates among female trainees (2000–2010), 24 though ElHawary reported that 39% of female plastic surgery residents perceived gender-based disadvantage versus 3.6% of males despite identical case volumes. 27 This highlights a paradox: inequity perceptions persist even as measurable performance gaps narrow.
Psychological well-being is increasingly prioritized. At McGill, 75% of residents reported shaming, and 78% witnessed it, 1 yet awareness of its harm is shifting culture toward constructive, coaching-based feedback. Seemann noted that traditional expectations of emotional invulnerability limited discussion of stress, a barrier now addressed. 22 Interventions like mindfulness-based cognitive therapy reduce anxiety, enhance confidence, and foster holistic professional development, 15 while Patel highlighted residents’ awareness of cultural pressures to appear perpetually competent. 18 Collectively, these trends indicate movement toward inclusivity, psychological safety, and emotional resilience.
Work-life integration and parental support also shape surgical culture. Jiang found that while all Canadian programs reported parental leave, only 35% mentioned lactation policies, and none covered fertility treatments. 14 Scallan showed that maternity leave can enhance professional growth, improving communication, empathy, and confidence. 21 Institutional support for family responsibilities thus benefits both well-being and professional competence.
Generational shifts and structural reforms further illustrate transformation. Contemporary residents report fewer planned workdays (7.4% vs 44.8% for faculty), reduced call frequency, and limited post-call duties, with female residents more likely to plan parental leave. 4 Romanchuk described a shift from volume-based exposure to structured mentorship and competency-based evaluation, 20 while White emphasized differentiating competency from proficiency, prioritizing graduated autonomy and readiness for independent practice. 23 Together, these trends reflect a profession evolving toward wellness, equity, mentorship, and holistic professional development, redefining surgical excellence beyond endurance.
Duty-Hour Reforms
Canadian surgical training has evolved in duty-hour policies and resident wellness standards, reflecting a cultural shift toward sustainability and work-life integration. Historically, residents, especially interns, endured 24-h or continuous on-call schedules with minimal recovery, valuing endurance as commitment. In Quebec, consecutive call hours were reduced from 36 to 24 h in 1990 and to 16-h in-house calls by 2012 after legal challenges redefined acceptable working conditions.2,26 These reforms influenced national policies, introducing limits on in-house and home call hours, mandatory post-call relief, and protected educational time, emphasizing structured learning and patient safety. 20 The 2018 Fatigue Management Toolkit further promoted strategies to reduce fatigue, optimize performance, and support well-being. 36
Medical residents are represented nationally by Provincial Housestaff Organizations such as (Ontario), Resident Doctors of BC (Alberta), and PARIM (Manitoba), collectively forming Resident Doctors of Canada. Quebec is unique with the Fédération des médecins résidents du Québec, a province-wide union under a single collective agreement securing strong protections, including 16-h call limits, guaranteed post-call leave, defined academic time, and robust parental and grievance policies. These reforms foster a fatigue-conscious, rights-driven training environment emphasizing resident well-being, safety, and learning quality.
Resident experiences reflect both traditional expectations and emerging norms. At McGill, 43% exceeded maximum call limits, and 36% reported institutional noncompliance1. Residents working over 80 h weekly had higher compassion fatigue, 22 highlighting tensions between historic endurance models and modern priorities of safety, balance, and support. Positive experiences were linked to staff recognition of workload barriers. 11 While some residents and program directors remain hesitant about strict duty-hour limits, 28 competency-based cardiac surgery programs show autonomy and technical proficiency can be achieved without prolonged hours.23,25 Senior residents are more likely than juniors to view duty-hour restrictions as hindering Royal College objectives, 29 reflecting ongoing negotiation between tradition and reform.
Parental leave illustrates this cultural evolution. Female residents average 36 weeks of leave versus 4 weeks for males. 27 National standards provide 17–52 weeks maternity and 24–72 weeks paternity leave, with paid leave in 82% of programs and salary supplementation of 84%–95%. 14 Persistent barriers like scheduling, breastfeeding, and childcare are increasingly addressed, with phased return-to-work programs recommended. 21 Residents now anticipate fewer workdays, reduced post-call duties, and a greater willingness to use parental leave. 4 Structural supports, including equitable leave and accessible childcare, enhance retention and inclusivity, benefiting women and minority trainees. 16
COVID-19 accelerated these changes. At UBC, rotations were reorganized, residents centralized, and a Resident Reserve Unit established. 3 Virtual teaching and weekly town halls strengthened feedback and engagement. These adaptive strategies, combined with improved duty-hour policies, parental leave, mentorship, and union support, contributed to a decline in female surgical trainee attrition from 12.4% to 6.1% (2000–2010). 24 Overall, Canadian surgical education is shifting toward a sustainable, wellness-oriented, inclusive culture that balances training rigors with resident well-being and professional growth.
Wellness and Mental Health Initiatives
Wellness and mental health are central in Canadian surgical education, reflecting recognition of their impact on learning, performance, and retention. Despite growing research, gaps remain. Across 17 medical schools, trainees with darker skin reported isolation, microaggressions, and verbal abuse harming mental health, while female residents faced additional family-career balance challenges, worsened by poor work environments and sleep deprivation. 11 Gendered experiences intensify stress: at Calgary, 83% of women residents reported monthly gender-based discrimination versus 27% of men. 13 Female plastic surgery and visible minority residents noted restricted surgical exposure, reduced collegiality, diminished belonging, and consideration of leaving residency.16,27 However, emerging data suggest shaming and negative teaching, rather than gender alone, are stronger burnout predictors. 1
Structural factors strongly affect well-being. Excessive duty hours extended post-call work, and lack of protected rest reduce quality of life and learning.2,26,28 Quebec's reduction of continuous on-call shifts from 36 to 16 h illustrates progressive wellness reform linking workload, fatigue, and patient safety.
Shame-based teaching, reported by 75% of residents, contributes to anxiety, isolation, and burnout, though higher grit and resilience improve coping. 1 COVID-19 highlighted wellness disparities: 41% reported increased anxiety, 61% heightened loneliness, and only 14% accessed institutional resources. UBC's Resident Reserve Unit introduced weekly town halls, virtual workouts, and meal support, fostering community and resilience. 3 Residents also used personal coping strategies, including optimism (42%) and enjoyable activities (40%), 25 reflecting adaptive, self-sustaining approaches complementing institutional support.
Formal wellness initiatives now underpin surgical training, shifting from endurance-based education to holistic professional development. Mindfulness programs reduce anxiety and enhance confidence. 15 Peer mentorship improves goal setting, work-life balance, and confidence. 19 Tiered mentorship pairing junior residents with senior peers and faculty lowers stress, reducing Perceived Stress Scale scores from 18.5 to 6.8 and Maslach Burnout Inventory emotional exhaustion from 47.6 to 13.3. Work-hour restrictions and post-call relief improve fatigue, collegiality, and workplace civility, 4 linking systemic reform with psychological well-being.
Parental leave and phased return-to-work policies further reflect cultural evolution. Canadian programs universally offer maternity, paternity, and adoption leave, with 82% paid, 71% lactation facilities, and 88% mental health coverage. 14 Mentorship and peer support facilitate reintegration. 21 Duty-hour reforms, including 1-in-4 in-house call and guaranteed post-call relief, balance workloads, protect study and technical practice time, and enhance both resident wellness and patient care. 20 Collectively, these initiatives promote psychological safety, resilience, and holistic professional growth, signaling a sustained cultural shift toward a healthier, supportive surgical training environment.
Equity, Diversity, and Inclusion
Equity, diversity, and inclusion (EDI) are central in Canadian surgical education, though disparities persist. By 2010, women made up nearly 40% of trainees, yet among 4891 academic surgeons, only 6% were women or people of color, compared with 56% White males. 12 These gaps reflect enduring intersectional barriers limiting access, mentorship, and advancement. Calls for structured national mentorship, holistic applicant review, and mandatory antiracism training aim to promote equity. 11 Yet women and gender minorities still face reduced operative autonomy, biased feedback, and systemic inequities. 13 Female residents report restricted surgical exposure, gender-influenced career goals, 27 and continued experiences of shame-based learning, 1 showing cultural hierarchies still shape educational opportunities.
Female visible minority residents experience lower mentorship, support, and workplace belonging. 16 Inconsistent parental leave policies continue to create barriers despite maternity, paternity, and adoption provisions.3,4,14 Encouragingly, open dialogue, enhanced wellness benefits, and formal mentorship improve confidence, goal setting, and work-life balance, 19 signaling early cultural shifts toward inclusivity. However, female residents remain hesitant to request lactation breaks or fear faculty disapproval, 21 contributing to higher attrition than male peers (12.4% vs 6.1%). 24 Representation alone is insufficient, achieving equity requires structural, cultural, and behavioral change at institutional and national levels.
Inequities also extend to educational materials and structural supports. Darker skin tones are underrepresented in plastic surgery curricula, with only 16.8% of teaching images depicting Fitzpatrick IV-VI, 31 limiting diagnostic exposure and cultural competence. International medical graduates report higher stress and fewer mentorship opportunities than Canadian-trained peers. 25 These findings emphasize that equity efforts must go beyond demographic representation to ensure inclusive curricula, equitable mentorship, and culturally competent teaching. Strengthening EDI across surgical education fosters a more supportive, representative, and high-performing learning environment, benefiting trainees and patients.
Feedback and Learning Environment
Feedback and the learning environment are pivotal for resident development, well-being, and professional identity. Historically, trainees lacked psychologically safe spaces, structured mentorship, and consistent advocacy, complicating navigation of surgical hierarchies. Honesty, confidentiality, and advocacy influenced learning more than racial or gender concordance, 11 yet trainees of color reported isolation, microaggressions, and limited mentorship. 11 Stressors like exams, competing clinical and academic demands, and extended duty hours despite formal limits further discouraged some from pursuing surgery.11,25 Positive experiences arose when faculty acknowledged barriers and fostered collegiality, 11 signaling a shift toward supportive, psychologically safe environments.
Equity in feedback reflects evolving inclusivity. Female and visible minority residents often received subjective, personality-focused feedback and less mentorship, while structured peer mentorship improved confidence, performance, and work-life balance.13,16,19 Resident engagement, not gender, predicted operative exposure, showing agency increasingly drives learning. 27 Despite formal maternity leave, women faced structural and interpersonal barriers, though many reported enhanced communication, empathy, and organizational skills, valued alongside technical mastery.13,17,18,31
Shame-based learning persists, undermining safety, confidence, and contributing to burnout. 1 Residents sometimes avoided questions to appear competent. 18 Interventions like the MiST mindfulness program improved operating room confidence, reduced anxiety, and promoted reflection and peer support. 15
COVID-19 accelerated adaptability. Canadian residents faced training disruptions but benefited from flexible, self-directed learning and digital integration. 12 At UBC, rotation restructuring, Resident Reserve Units, and virtual sessions-maintained continuity while emphasizing wellness and communication. 3
Inclusive learning is increasingly prioritized. Surgical curricula underrepresented medium and dark skin tones but growing diversity in teaching materials signals commitments to equity. 31 Gender-conscious cultures improve retention and satisfaction, with rising female representation and declining attrition over the past decade.24,31 Structured feedback and safe learning environments enhance skill development, confidence, and overall well-being.
Global Transferability
The transferability of Canadian surgical training findings is shaped by legal, cultural, and institutional contexts. Quebec's duty-hour reforms, driven by provincial labor laws and arbitration, illustrate how local factors limit broader applicability. Most other provinces cap shifts at 24 h with 2 h for handover.26,36,37
Jurisdictional comparisons show wide variation. The U.S. ACGME prioritizes patient safety, New Zealand limited hours in 1985 to 72 weekly with rest between shifts and every second weekend off, and Australia allows longer shifts but generally aligns residents with the workforce. 2 Canada's province-led system complicates reforms, though Royal College accreditation standards provide national leverage.2,38,39
Context-specific variation also affects workload and outcomes. Canadian residents often have more regulated duty hours than U.S. and E.U. peers, 4 with lower female trainee attrition reported. 24 Skills-transfer courses and curriculum diversity remain institution-specific, requiring multi-site validation.20,31 Even with Canada-wide standards, findings may resist cross-specialty transfer.25,28,29
The transition to Competence by Design (CBD), the Royal College's competency-based framework, emphasizes observable skills, individualized progression, and continuous feedback. Structured Entrustable Professional Activities and workplace-based assessments enable advancement based on competence rather than fixed time, fostering accountability, transparency, and readiness for independent practice.
Complementing this, the Canadian Excellence in Residency Accreditation (CanERA) framework introduced standards emphasizing continuous quality improvement, learner experience, educational culture, and wellness, shifting evaluation from compliance-based to outcomes-based and promoting a coaching-oriented culture.
Together, CBD and CanERA have improved the quality, safety, and adaptability of Canadian surgical training.
Recommendations are shown in Supplemental Figure 3.
Future Directions
Future research should use longitudinal studies to evaluate how scheduling, simulation-based learning, and wellness initiatives affect resident competence, team communication, and patient outcomes. This includes expanding the Canadian consensus framework to examine the integration of fatigue management plans into training. Studies should also assess how leadership, institutional support, and resident empowerment influence the adoption of sustainable workload reforms. Additionally, Canadian research should evaluate the long-term impact of CBD training on operative proficiency, faculty engagement, and resident well-being to guide ongoing improvements in competency-based surgical education.
Conclusion
Canadian surgical training is evolving through duty-hour reforms, wellness programs, parental leave, and equity initiatives. Duty-hour and leave policies support balanced, sustainable training, while wellness programs address burnout, discrimination, and excessive workloads via mentorship, mindfulness, and psychological safety. Equity, diversity, and inclusion are increasingly prioritized. Structured feedback, competency-based training, mindfulness, and digital learning create safer, more supportive learning environments. Although transfer beyond Canada is limited, multi-site validation is valuable. Ongoing research, cross-provincial collaboration, and culturally responsive reforms are essential to sustain learner-centered training that balances education, well-being, and patient care.
Supplemental Material
sj-pdf-1-psg-10.1177_22925503261457119 - Supplemental material for From Tradition to Wellness: A Systematic Review of Changing the Surgical Training Culture in Canada
Supplemental material, sj-pdf-1-psg-10.1177_22925503261457119 for From Tradition to Wellness: A Systematic Review of Changing the Surgical Training Culture in Canada by Sara B. A. Morel, Rawan Elabd, Joshua Vorstenbosch, Dino Zammit, Gaby Doumit and Stephanie Thibaudeau in Plastic Surgery
Supplemental Material
sj-pdf-2-psg-10.1177_22925503261457119 - Supplemental material for From Tradition to Wellness: A Systematic Review of Changing the Surgical Training Culture in Canada
Supplemental material, sj-pdf-2-psg-10.1177_22925503261457119 for From Tradition to Wellness: A Systematic Review of Changing the Surgical Training Culture in Canada by Sara B. A. Morel, Rawan Elabd, Joshua Vorstenbosch, Dino Zammit, Gaby Doumit and Stephanie Thibaudeau in Plastic Surgery
Supplemental Material
sj-pdf-3-psg-10.1177_22925503261457119 - Supplemental material for From Tradition to Wellness: A Systematic Review of Changing the Surgical Training Culture in Canada
Supplemental material, sj-pdf-3-psg-10.1177_22925503261457119 for From Tradition to Wellness: A Systematic Review of Changing the Surgical Training Culture in Canada by Sara B. A. Morel, Rawan Elabd, Joshua Vorstenbosch, Dino Zammit, Gaby Doumit and Stephanie Thibaudeau in Plastic Surgery
Footnotes
Author Contributions
Conceptualization: S.Morel, R.ElAbd, J.Vorstenbosch, D.Zammit, G.Doumit, S.Thibaudeau. Data curation: S.Morel, R.ElAbd. Formal analysis: S.Morel, R.ElAbd. Methodology: S.Morel, R.ElAbd, J.Vorstenbosch, D.Zammit, G.Doumit, S.Thibaudeau. Project administration: S.Morel, R.ElAbd. Supervision: R.ElAbd, J.Vorstenbosch, D.Zammit, G.Doumit, S.Thibaudeau. Validation: S.Morel, R.ElAbd, J.Vorstenbosch, D.Zammit, G.Doumit, S.Thibaudeau. Writing: Original draft: S.Morel, R.ElAbd. Writing: Review & editing: S.Morel, R.ElAbd, J.Vorstenbosch, D.Zammit, G.Doumit, S.Thibaudeau.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.