
Abstract
Background
Diagnostic sural nerve biopsies can be taken as whole or fascicular nerve biopsies. It is unclear if this is associated with differences in diagnostic yield or procedural complications. We compared the clinical outcomes of fascicular versus whole sural nerve biopsies.
Methods
This was a retrospective chart review of sural nerve biopsies performed between 2011 and 2024 at 4 tertiary academic hospitals in Canada. The primary outcome was the incidence of postoperative nerve-related complications. The secondary outcome was the concordance between the biopsy and the final diagnosis. Fisher's exact test was used to compare the incidence of postoperative complications. Two-sided Cochran-Armitage trend test was used to compare concordance between groups.
Results
There were 75 patients who underwent whole sural nerve biopsies and 13 patients who underwent fascicular sural nerve biopsies; 54.6% of patients were male, with a mean age of 59.7 ± 15.9. The average nerve length sampled was 2.86 ± 1.3 cm in the whole nerve biopsy group and 2.35 ± 1.3 cm in the fascicular nerve biopsy group. Only a small proportion of patients had documented follow-up (whole: 26.7%; fascicular: 15.4%), among whom 40.0% in the whole nerve biopsy group and 0.0% in the fascicular group experienced complications (P = 1.00). The most common diagnosis was vasculitis in both groups (whole nerve biopsy: 17.0%, fascicular nerve biopsy: 36.4%). There was no statistically significant shift toward higher concordance in the whole nerve group (Z = 0.63, P = .53).
Conclusion
Fascicular and whole sural nerve biopsies demonstrated similar diagnostic concordance. Prospective studies with larger sample sizes are needed to more accurately characterize postoperative complication rates.
Introduction
Nerve biopsy is a diagnostic tool used to determine the etiology of various peripheral neuropathies for over 50 years.1,2 Advances in laboratory, neurophysiological, and genetic testing have decreased the indications for nerve biopsy. 2 Nonetheless, nerve biopsy continues to provide valuable information when non-invasive options have been exhausted and remains the only method of diagnosing vasculitic neuropathy.2,3
The sural nerve is the most commonly biopsied nerve, as its function is purely sensory. 3 The sensory deficits to the lateral dorsum of the foot caused by sural nerve biopsy are well-tolerated from a functional standpoint, and the nerve is easy to access surgically under local anesthetic in a minor procedure room setting. 3 The procedure is not without its complications however. Postoperative pain, dysesthesia, and paresthesia have been reported, in addition to standard surgical complications such as bleeding, infection, and wound healing complications.4,5
Sural nerves can be taken as a fascicular or whole nerve biopsy. Theoretically, the fascicular biopsy decreases the morbidity to the sural nerve compared to a whole biopsy by not excising all of the sensory nerve fascicles. However, there is limited and poor-quality evidence of increased nerve-related complications.4,6–8 The consensus in the literature is that whole nerve biopsy has greater diagnostic potential where there may be patchy pathology, 9 despite there being no published evidence to support this claim.
We compared the clinical outcomes of fascicular versus whole sural nerve biopsies using a retrospective chart review. We assessed the incidence of postoperative nerve-related complications and the concordance between biopsy and the final diagnosis, and the impact of the biopsy on final diagnosis.
Methods
This study was approved by the regional Research Ethics Board (HiREB; 18577). This manuscript was written according to the Strengthening the Reporting of Observational Studies in Epidemiology Statement guidelines. 10
Study Design
This was a retrospective chart review of sural nerve biopsies performed between January 2011 and December 2024 at 4 tertiary care centers.
Patient Population
All sural nerve biopsies performed at the included sites within the above timeframe were identified by the pathologist (MB) by searching for the keyword “sural” within pathology reports. These biopsies were linked to their corresponding patient medical record numbers to allow for clinical chart review.
Data Collection
Data was collected using a piloted data extraction form in duplicate by 2 members of the research team (PK, CW). Any disagreements were resolved via consensus. The following information was collected from the patient chart on Meditech (∼ April 2022) or Epic (after April 2022): age, sex, comorbidities, status of immunosuppression, reason for referral, referring provider, indication for biopsy, type of biopsy as per the operative note, operative details, final diagnosis, and postoperative complications. We extracted the following information concerning from each biopsy report: the entire text of the pathologic description, the pathologic diagnosis, and maximal length of biopsy. Patient consent was waived with research ethics board approval, given the necessary nature of the data, the impracticality of obtaining retroactive consent, safeguards in place to protect confidentiality, and minimal risk to participants.
Outcomes
The primary outcome was the incidence of postoperative nerve-related complications, which include pain, dysesthesias, and paresthesia as documented in the patient's chart. Patients without a recorded postoperative encounter were classified as having missing outcome data for complications. Given that routine follow-up is not standard practice at the included institutions, we additionally report the proportion of patients without documented follow-up. We also assessed the concordance between the biopsy findings and the final diagnosis. Concordance was categorized as the following: specific findings in concordance with final diagnosis (concordant), general findings not contradicting final diagnosis (partially concordant), and findings contradictory to final diagnosis (discordant). We also assessed how the biopsy may have affected the final diagnosis by indicating if the biopsy changed/specified previous diagnosis or confirmed previous diagnosis.
Statistical Analysis
We described patient characteristics and operative details with frequency, mean and standard deviation, and/or median and interquartile range (IQR) as appropriate. Fisher's exact test was used to compare the incidence of postoperative complications. Two-sided Cochran-Armitage trend test was used to compare concordance between groups. Concordance was converted to ordinal scores 2, 1, and 0 for concordant, partially concordant, and discordant, respectively. Statistical significance was defined as P-value < .05.
Results
A total of 113 patients who underwent sural nerve biopsy were identified within the study period. There were 75 patients who underwent whole sural nerve biopsies and 13 patients who underwent fascicular sural nerve biopsies, totaling 88 patients included in the study for analysis. The remaining 25 patients had insufficient information available to determine whether a fascicular or sural nerve biopsy was performed and were excluded from analysis. See Figure 1 for a flow diagram of patient inclusion.
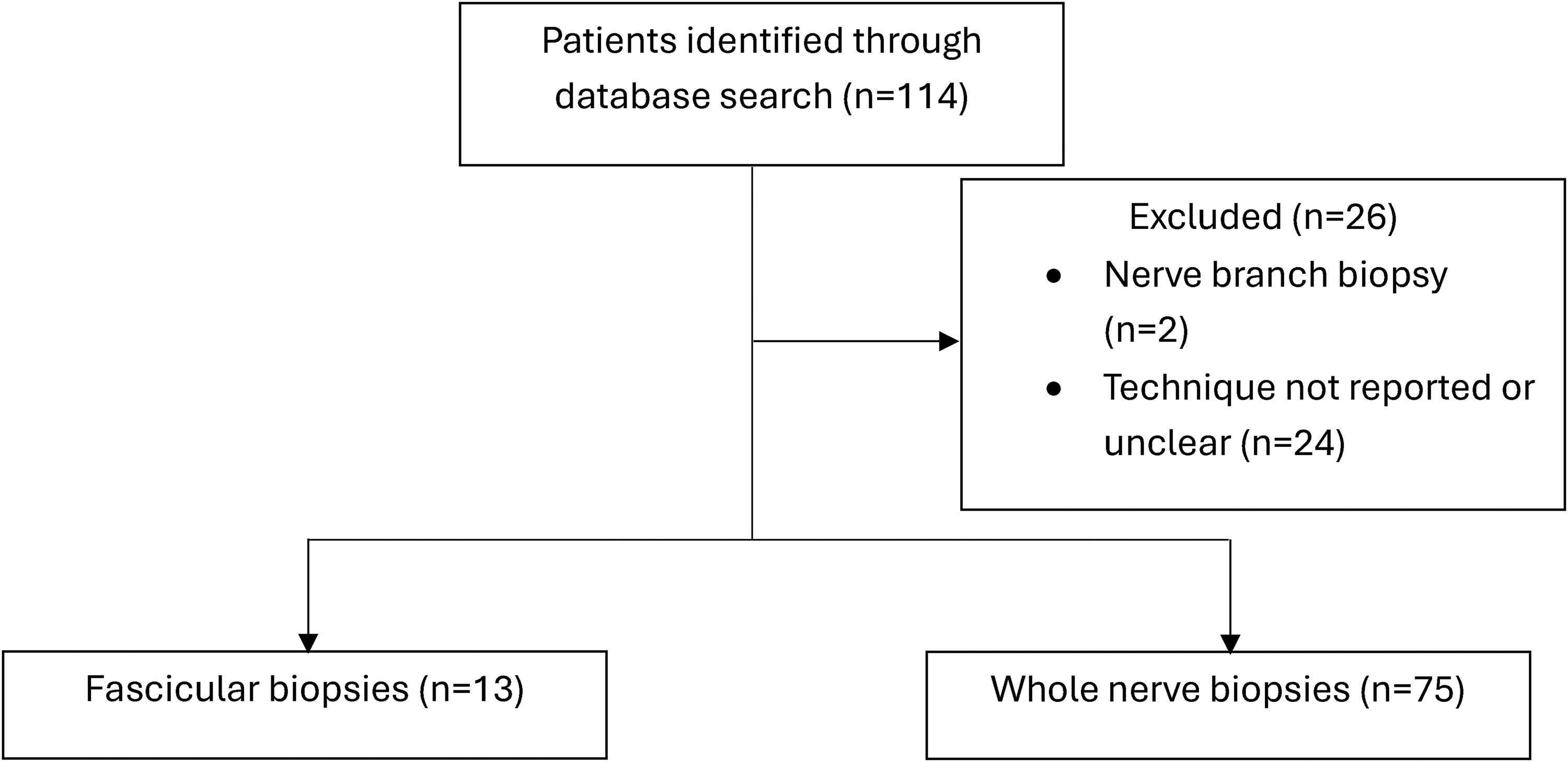
Flow diagram of patient Identification and exclusions.
Baseline Patient Characteristics
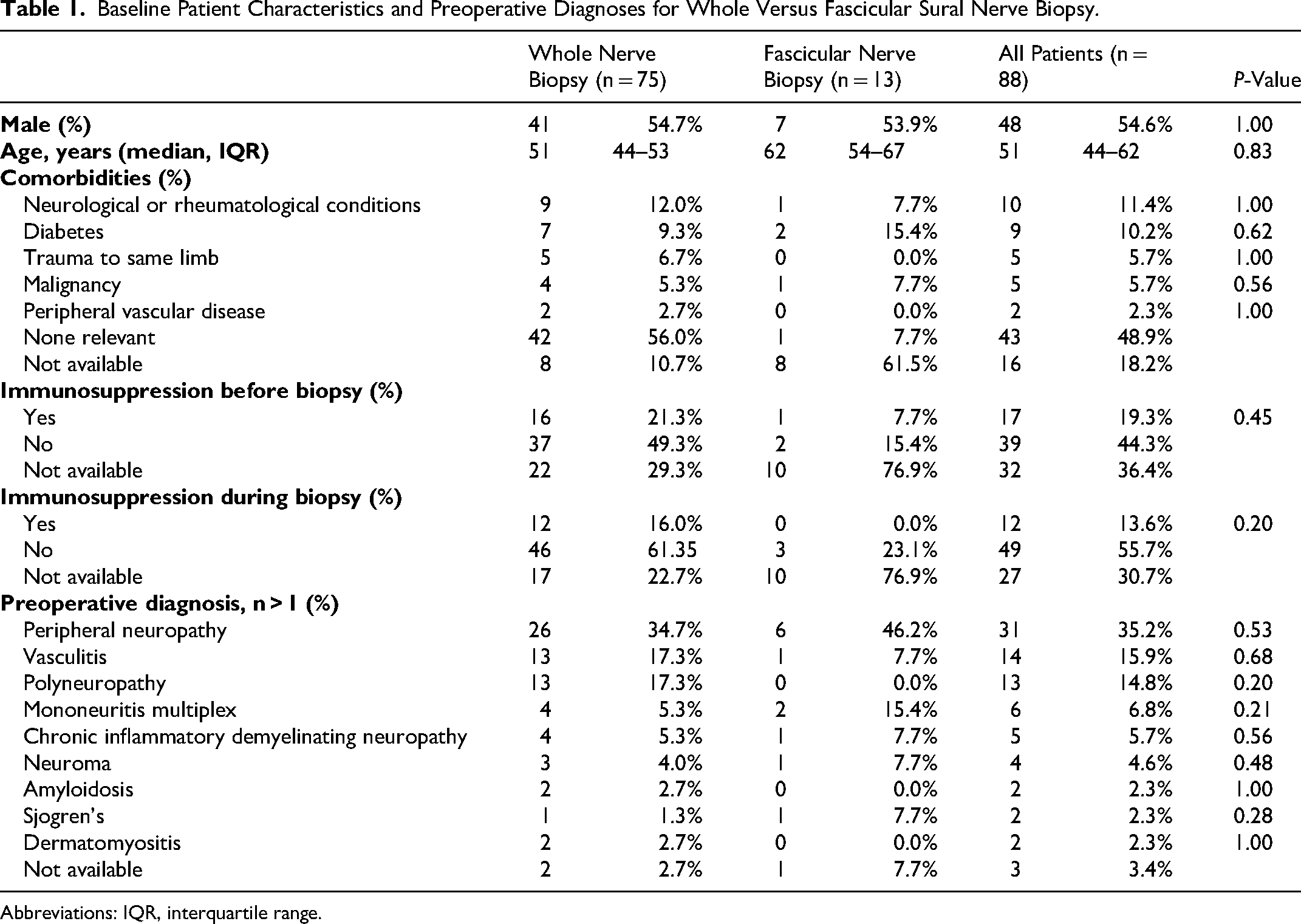
Within the cohort, 41 (54.6%) patients were male, with a mean age of 59.7 ± 15.9 (Table 1). Referrals were made most commonly by neurology (50.0%), followed by rheumatology (15.9%) and physiatry (14.8%). In the whole nerve biopsy group, 9 (12.0%) patients had known neurological/rheumatological conditions and 1 (7.7%) had them in the fascicular nerve biopsy group.
Baseline Patient Characteristics and Preoperative Diagnoses for Whole Versus Fascicular Sural Nerve Biopsy.
Abbreviations: IQR, interquartile range.
Preoperatively, 21.3% of patients in the whole nerve biopsy group were immunosuppressed pre-biopsy, and 16.0% were immunosuppressed at the time of biopsy. In the fascicular nerve biopsy group, 7.7% of patients were immunosuppressed pre-biopsy, and none were immunosuppressed at the time of biopsy. The most common immunosuppressant used was oral or intravenous glucocorticoids.
The most common preoperative diagnosis was peripheral neuropathy (not otherwise specified) in both groups (whole nerve biopsy: 34.7%, fascicular nerve biopsy: 46.2%). In the whole nerve biopsy group, patients presented most commonly with weakness (40.0%), numbness (30.7%), paresthesia (29.3%), and pain (28.0%). The fascicular nerve biopsy group commonly presented with weakness and numbness (each 30.8%), motor deficits (23.1%), and pain and issues with gait/coordination (each 15.4%). The median duration of symptoms was 12 (IQR: 3-24) months and 12 (IQR: 6-30) months in the whole and fascicular nerve biopsy groups, respectively.
Operative Details
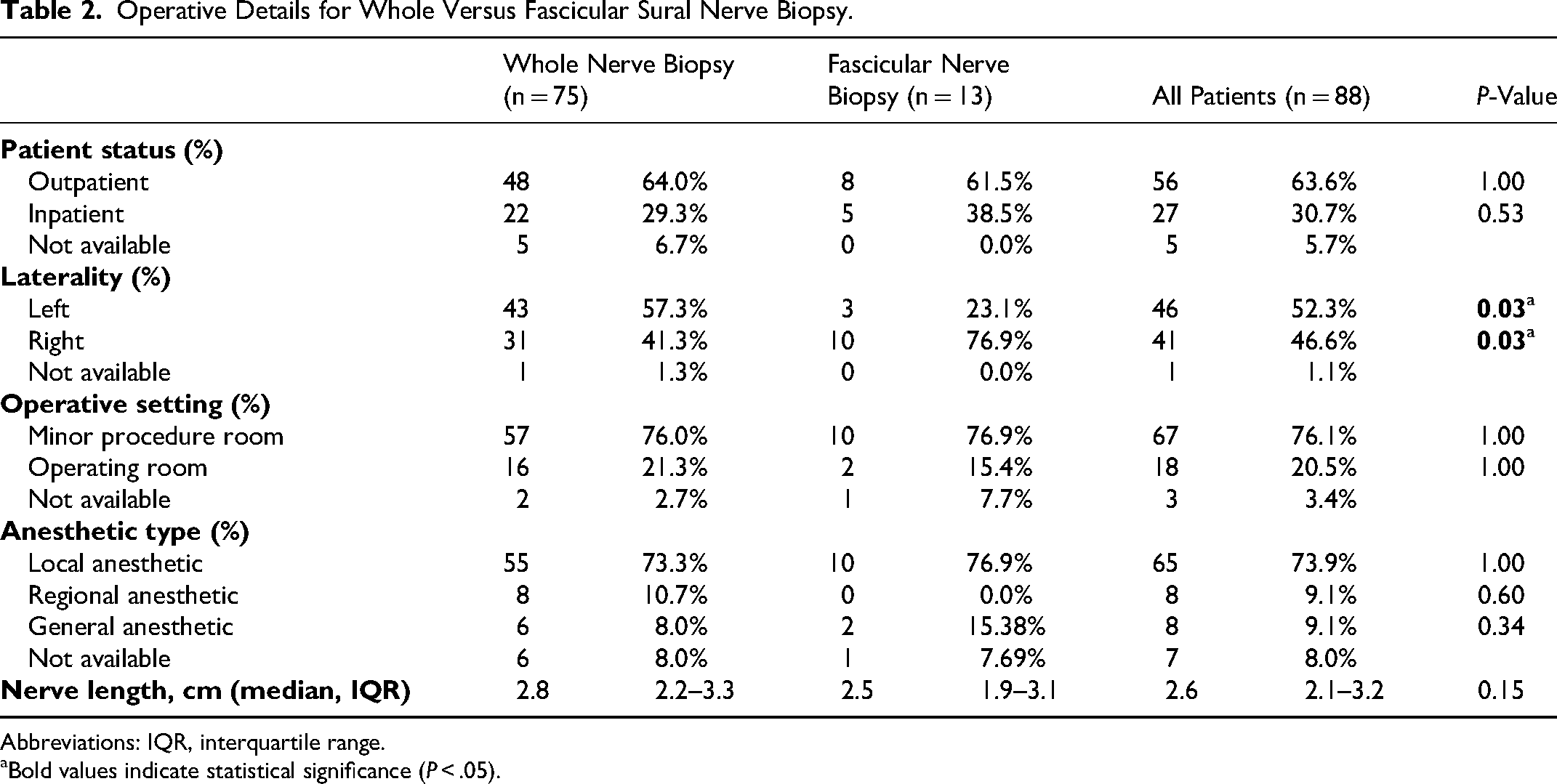
Biopsies were performed in the outpatient setting in 63.6% of patients and inpatient setting for 30.7% of patients (Table 2). Sural nerve biopsies were usually completed in the minor procedure room (whole nerve biopsy: 76.0%, fascicular nerve biopsy: 76.9%) under local anesthetic (whole nerve biopsy: 73.3%, fascicular nerve biopsy: 76.9%) in both groups. The biopsy was more commonly collected from the left leg in the whole nerve biopsy group (57.3%) and the right leg in the fascicular nerve biopsy group (76.9%).
Operative Details for Whole Versus Fascicular Sural Nerve Biopsy.
Abbreviations: IQR, interquartile range.
Bold values indicate statistical significance (P < .05).
The average nerve length sampled was 2.8 (IQR: 2.2-3.3) cm in the whole nerve biopsy group and 2.5 (IQR: 1.9-3.1) cm in the fascicular nerve biopsy group.
Complications
Among patients undergoing whole nerve biopsy, 20 (26.7%) had documented postoperative follow-up, of whom 8 (40.0%) had complications and 12 (60.0%) had no reported complications (Table 3). Reported complications included 3 infections requiring antibiotics and 5 cases of neurologic symptoms following biopsy. Nerve-related complications were further characterized by sensory and neuropathic outcomes. Three patients (15.0%) reported persistent sensory deficits (lateral foot numbness), 1 (5.0%) reported paresthesia, and 1 (5.0%) developed neuropathic pain requiring reoperation. The remaining 55 patients (73.3%) had no documented postoperative follow-up.
Postoperative Complications Following Whole Versus Fascicular Sural Nerve Biopsy out of Patients with Documented Follow-up.
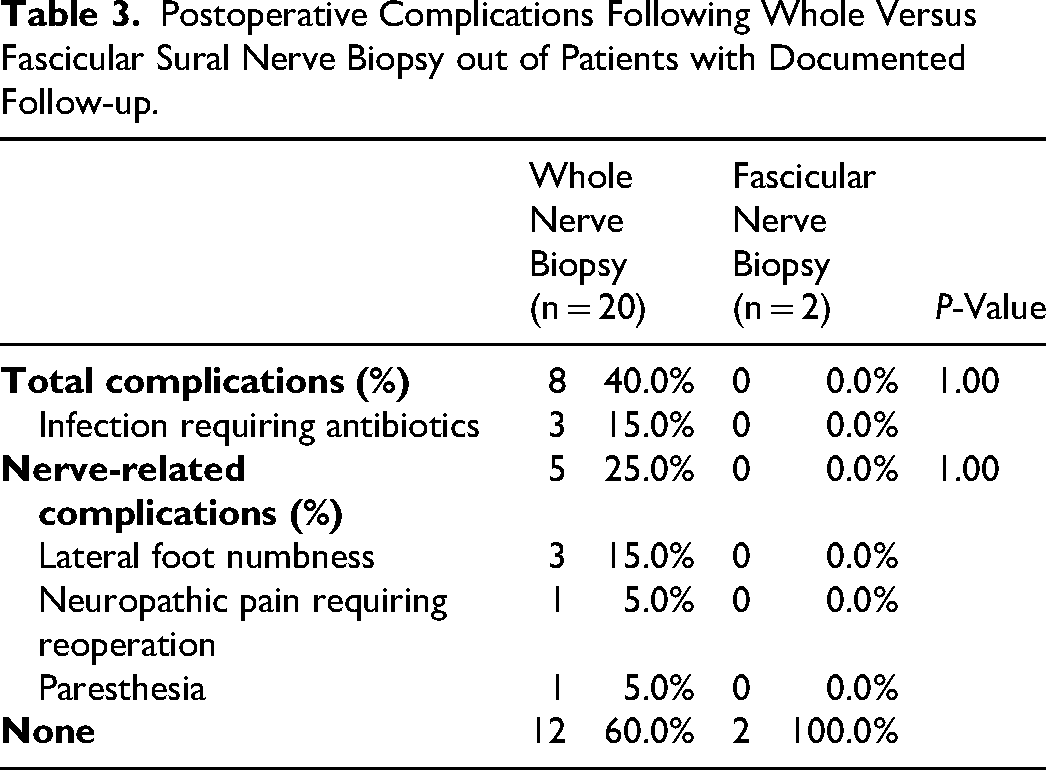
In the fascicular nerve biopsy group, 2 patients (15.4%) had documented follow-up, and no complications were reported in these patients, while 11 patients (84.6%) had no documented follow-up.
There was no statistically significant difference in nerve-related complication rates between whole and fascicular nerve biopsy groups (P = 1.00), though interpretation is limited by the small number of patients with follow-up, particularly in the fascicular group.
Post-Biopsy Outcomes
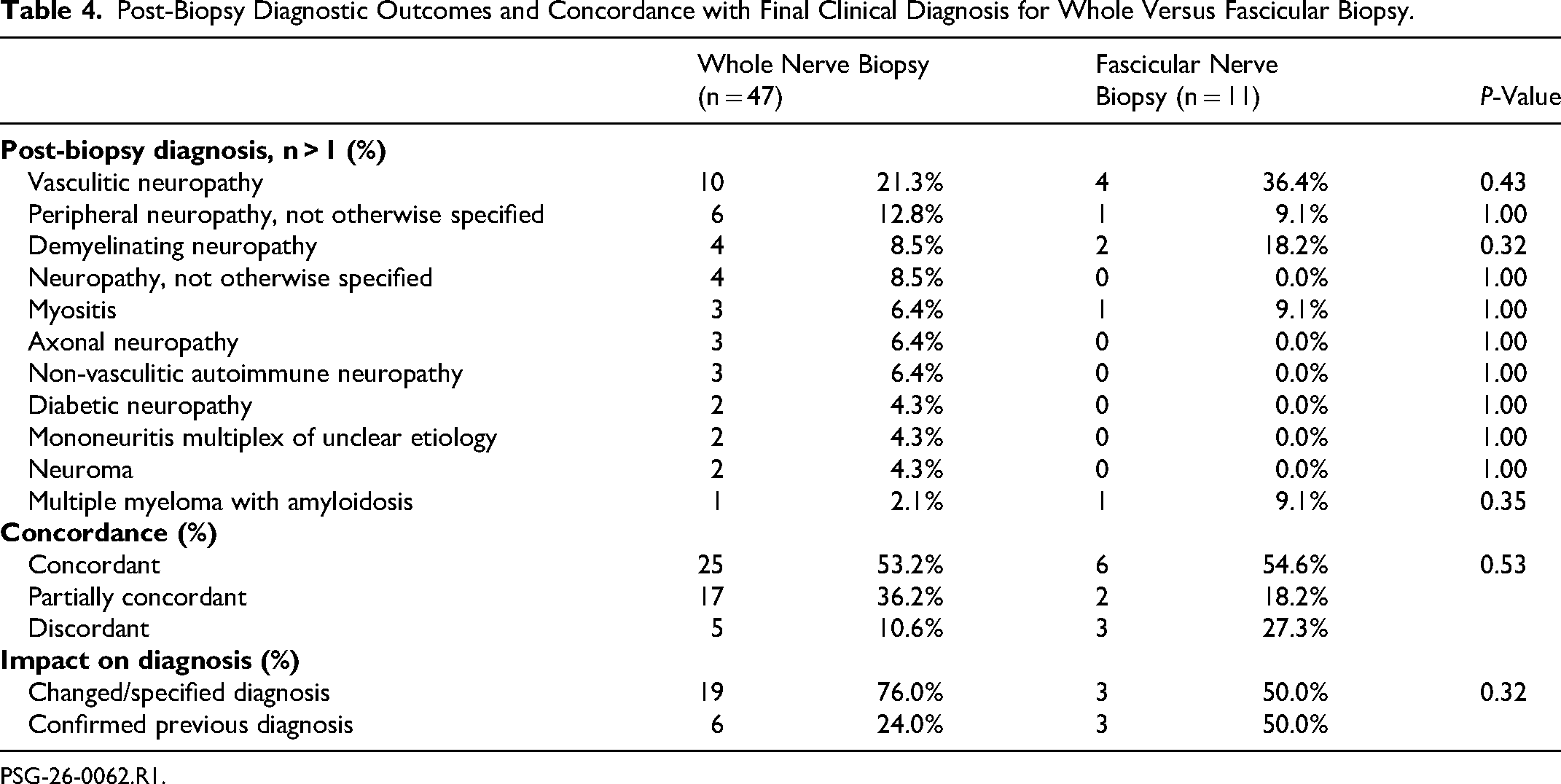
Clinical diagnoses post-biopsy were available in 47 (62.7%) of patients in the whole nerve biopsy group and 11 (23.9%) of patients in the fascicular nerve biopsy group (Table 4).
Post-Biopsy Diagnostic Outcomes and Concordance with Final Clinical Diagnosis for Whole Versus Fascicular Biopsy.
PSG-26-0062.R1.
In the whole nerve biopsy group, the most common clinical diagnoses were vasculitic neuropathy (17.0%), peripheral neuropathy (not otherwise specified; 12.8%), demyelinating neuropathy (8.5%), and neuropathy (not otherwise specified; 8.5%). The clinical diagnosis was concordant with the final diagnosis in 53.2% of cases, partially concordant in 36.2%, and discordant in 10.6%. Of the 25 concordant cases, the biopsy changed/specified the previous diagnosis in 76.0% of cases and confirmed the previous diagnosis in 24.0% of cases. Of the 10 cases diagnosed with vasculitic neuropathy, 8 were diagnosed via biopsy, and 2 cases failed to identify vasculitis on biopsy though not explicitly discordant. Biopsy was discordant from 1 of each of the following final clinical diagnoses: non-vasculitic autoimmune neuropathy, neuroma, multiple myeloma with amyloidosis, dermatomyositis, and conversion disorder.
The most common clinical diagnoses in the fascicular nerve biopsy group were vasculitic neuropathy (36.4%) and demyelinating neuropathy (18.2%). The clinical diagnosis was concordant with the final diagnosis in 54.6% of cases, partially concordant in 18.2%, and discordant in 27.3%. Of the 6 concordant cases, the biopsy changed/specified the previous diagnosis in 50.0% of cases and confirmed the previous diagnosis in 50.0% of cases. Of the 4 cases diagnosed with vasculitic neuropathy, 2 were diagnosed via biopsy and 2 confirmed the previous diagnosis of vasculitis. Biopsy was discordant from 1 of each of the following final clinical diagnoses: multiple myeloma with amyloidosis, demyelinating neuropathy, and peripheral neuropathy (not otherwise specified).
There was no statistically significant shift toward higher concordance in the whole nerve group (Z = 0.63, P = .53).
Discussion
Our study demonstrates that fascicular nerve biopsies have similar diagnostic yield as whole nerve biopsies. However, while the relatively small number of fascicular biopsies reflects real-world practice at participating centers, this limits statistical power for between-group comparisons. As such, the findings should be interpreted cautiously, as the present study may be underpowered to detect clinically meaningful differences in postoperative complications or diagnostic concordance. These findings are best viewed as hypothesis-generating and may help inform effect-size assumptions for future prospective studies.
There is limited evidence formally investigating postoperative outcomes of sural nerve biopsy. In a survey of 97 patients who completed whole sural nerve post-biopsy questionnaires 3- and 12- month post-procedure, 30% of patients had persistent mild nerve-related symptoms, and 10% had substantial pain or paresthesias.7,8 A 16-patient case series showed nerve-related complication rates of 60% and 45% in the whole and fascicular nerve biopsy groups, respectively. 4 A 50-patient prospective study reported that approximately two-thirds of patients had pain or other nerve-related complications with no significant differences between biopsy groups. 6
Our study demonstrated a similar proportion of nerve-related complications among patients with documented follow-up, with 40% of patients in the whole nerve biopsy group experiencing complications. The fascicular group only had 2 patients with documented postoperative follow-up and thus limits the ability to draw comparisons between techniques. Direct comparison with prior studies is also challenging due to differences in outcome ascertainment. At our institutions, routine postoperative follow-up after sural nerve biopsy is not standard practice unless clinically indicated, and complication rates were therefore calculated only among patients with documented follow-up. In contrast, prior studies which used patient-reported surveys are more likely to capture mild or transient sensory symptoms. Our findings may overestimate complication rates among followed patients and underestimate the true incidence at the population level, given the high proportion of patients without follow-up, which limits the ability to make definitive conclusions regarding relative complication rates and highlights the need for larger, prospective studies.
Another potential advantage of whole nerve biopsy is more complete sampling of a segment of a nerve, which may impact the ability to detect and diagnose “patchy” pathologies.6,9 Vasculitic neuropathy is a commonly cited example of such pathology, although the actual usefulness of sural nerve biopsy in its diagnosis is questionable, 11 and recent studies have shown higher diagnostic yield in the peroneal nerve and peroneus brevis muscle biopsy. 12 In our study, there were no significant differences in biopsy concordance with final diagnosis between groups, though the whole nerve biopsy group had more frequent rates of immunosuppression before and during biopsy. Notably, all 4 cases of vasculitic neuropathy in the fascicular nerve biopsy group were successfully identified on pathology, even in the absence of suspected pre-biopsy vasculitis.
One of the main limitations of this study was its retrospective nature. There was a sizable amount of missing data, especially in the postoperative period. It is possible that many patients did have nerve-related complications, but they were not clinically important enough for patients to schedule a follow-up visit in the context of their other ailments. It was also not possible to ascertain the cause-and-effect relationship between biopsy and final diagnosis or subsequent management. Many final diagnoses were also non-specific (eg, peripheral neuropathy, not otherwise specified), which limited the concordance of either biopsy type with the final diagnosis. The fascicular nerve biopsy group also had a small sample size, limiting the power of the study. Finally, the average biopsy nerve length was approximately 2 cm; histopathological guidelines typically recommend specimens of 4-5 cm for adequate diagnostic value, though our concordance rates were similar to other studies.13–15 The helpfulness (for diagnosis and/or management) of nerve biopsy in previous studies ranges from 20% to 60%. 13 Despite these limitations, this study provides important real-world insight into current practice patterns and identifies key gaps in outcome measurement, which may inform the design of future prospective studies with standardized follow-up.
Conclusion
The present multi-center retrospective review compared outcomes following fascicular and whole sural nerve biopsies and did not identify a statistically significant difference in nerve-related complication rates or concordance with the final diagnosis. Given the limited follow-up, comparisons of complication rates should be interpreted with caution. Diagnostic concordance appeared similar between techniques, suggesting that both approaches may be clinically equivocal, despite the theoretical increased diagnostic utility of whole nerve biopsies. This work identifies key gaps in outcome ascertainment and underscores the need for prospective studies with standardized follow-up and patient-reported outcome measures to better inform clinical decision-making.
Footnotes
ORCID iDs
Ethical Considerations
This study was approved by the Hamilton Integrated Research Ethics Board (Study #18577).
Author Contributions
Study conceptualization was done by HR. Investigation was done by PJK, CW, MB, and ATC. Formal analysis was done by PJK and CW. Manuscript writing was done by PJK. Manuscript review and editing was done by PJK, CW, MB, ATC, JQL, MJ, AT, and HR. Supervision was done by MB, JQL, MJ, AT, and HR.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.