
Abstract
Introduction
In 2010, it was estimated that 4.7 million living Americans had undergone a total knee arthroplasty (TKA). 1 While the majority of TKA patients heal without issue, the 10-year revision rate is reported to be between 6.2% and 12%.2–4 Given the volume of the procedure, many patients experience complications and require revision surgery (rTKA), with an estimated 56,000 to 73,000 cases performed each year in the United States. 5 The two most common indications for revision are aseptic and septic implant loosening. 6 Despite advances in surgical techniques and implant materials, rTKA is associated with a higher risk of complications, particularly wound-related issues, compared to primary TKA. 5 Wound complications are not only painful and functionally debilitating, but may also necessitate additional surgical interventions, possibly leading to increased morbidity, costs, and reduced quality of life.5,7
In recent years, “prophylactic” plastic surgery—or preemptive surgical intervention performed concurrently with the index procedure—has become a valuable option in the prevention of wound complications following multiple operation types. The use of flap coverage during rTKA, which involves the transfer of autologous, vascularized tissue, has gained traction as a viable method for soft tissue coverage in complex cases.3,8,9 Although multiple studies have demonstrated the role of flap coverage in both limb salvage and prophylaxis of wound complications in high-risk primary TKA, there is a lack of national and multicenter studies regarding the utility of prophylactic flap coverage in rTKA, in which all patients are at high risk of wound complications. As such, this study aims to address this gap in knowledge by analyzing the American College of Surgeons National Surgery Quality Improvement Program (ACS NSQIP®) database. 10 The primary objective is to conduct a comprehensive analysis of wound complications following the application of flap coverage in rTKAs at the national level, and comparing those outcomes to patients without concomitant flap coverage. The secondary aim was to determine if there were differences in mild and severe systemic complications between the two groups.
Methods
Study Design and Setting
A retrospective study of the ACS NSQIP® database was conducted from the years 2012 to 2020. The Institutional Review Board (IRB) at our hospital determined that this study did not constitute human subject research (determination #: 2025D000227). All patients who underwent rTKA were queried from the national database and included in the study. From those, 2 cohorts were identified based on the concomitant use of soft tissue flap reconstruction at the time of rTKA (no flap and flap group). Current Procedural Terminology codes were used to identify the aforementioned procedures.
Variables
Sociodemographic characteristics such as age, race, and ethnicity were collected. Clinical characteristics including body mass index (BMI), functional status prior to surgery, smoking status, presence of dyspnea, diabetes mellitus, congestive heart failure, history of severe chronic obstructive pulmonary disease (COPD), ascites, hypertension requiring medication, ventilator dependence, dialysis preoperatively, acute renal failure preoperatively, presence of disseminated cancer, steroid use for chronic conditions, presence of bleeding disorders, malnutrition/weight loss, and preoperative transfusion of more or equal to one unit of whole/packed red blood cell in 72 h prior to surgery were also collected. American Society of Anesthesiologists (ASA) classification, wound classification (clean, contaminated, etc), operative time in minutes and length of hospital stay were also extracted. The modified 5-item frailty index (mfI-5) was calculated and included in the analysis.
Postoperative complications included wound complications, mild systemic complications, and severe systemic complications. Wound complications were surgical site infection (SSI), deep SSI, organ/space SSI, and wound dehiscence. Mild systemic complications were bleeding with transfusion, pneumonia, renal insufficiency, and deep venous thrombosis requiring therapy. Severe systemic complications included pulmonary embolism, renal failure, stroke/cerebrovascular accident, unplanned intubation, cardiac arrest, myocardial infarction, septic shock, and reoperation.
Data Analyses
To assess baseline differences between cases with soft tissue flap reconstruction and those without, univariable analyses with Fisher's exact test and unpaired t-test were used for categorical and continuous variables, respectively. Moreover, to evaluate differences in wound complication and systemic complications between groups, a multivariate logistic regression model adjusting for propensity score, operative time, reoperation, and wound classification was constructed. A propensity score was created by using the following covariates: age, gender, BMI, functional status, ASA classification, smoking status, diabetes mellitus, hypertension, disseminated cancer, history of severe COPD, bleeding disorders, malnutrition/weight loss, use of steroids for chronic conditions, dyspnea, ascites, ventilator dependence, dialysis preoperatively, and preoperative transfusion of more or equal to one unit of whole/packed red blood cell in 72 h prior to surgery. Statistical significance was set for P-value of .05. Stata statistical software (STATA Corp., College Station, TX version 17.0) was used to conduct all statistical analyses.
Results
Baseline Characteristics
A total of 33,922 patients who underwent rTKA were included in this study. Of those, 33,818 (99.7%) patients did not receive concomitant flap coverage, while 104 (0.3%) patients underwent flap reconstruction. This group consisted of 99 patients who received pedicled flaps, and 5 patients who received free flaps. Similar demographic distributions in BMI, race and ethnicity were found across groups. Notable demographic differences were in age (P-value = .0119), gender (P-value = .033), and functional status prior to surgery (P-value < .001). The mean age for the group without flap reconstruction was 65.5 (standard deviation (SD) 10.3), while the pedicled flap group was 63.4 (SD 13.3) and the free flap group was 54.8 (SD 15.0). Both the pedicled and free flap group had a higher portion of men than the nonflap group (P-value = .033), and were of worse functional status with a higher proportion of partially and totally dependent patients in both flap groups prior to surgery (P-value < .001). Demographic characteristics for all groups are illustrated in Table 1.
Demographic Characteristics.
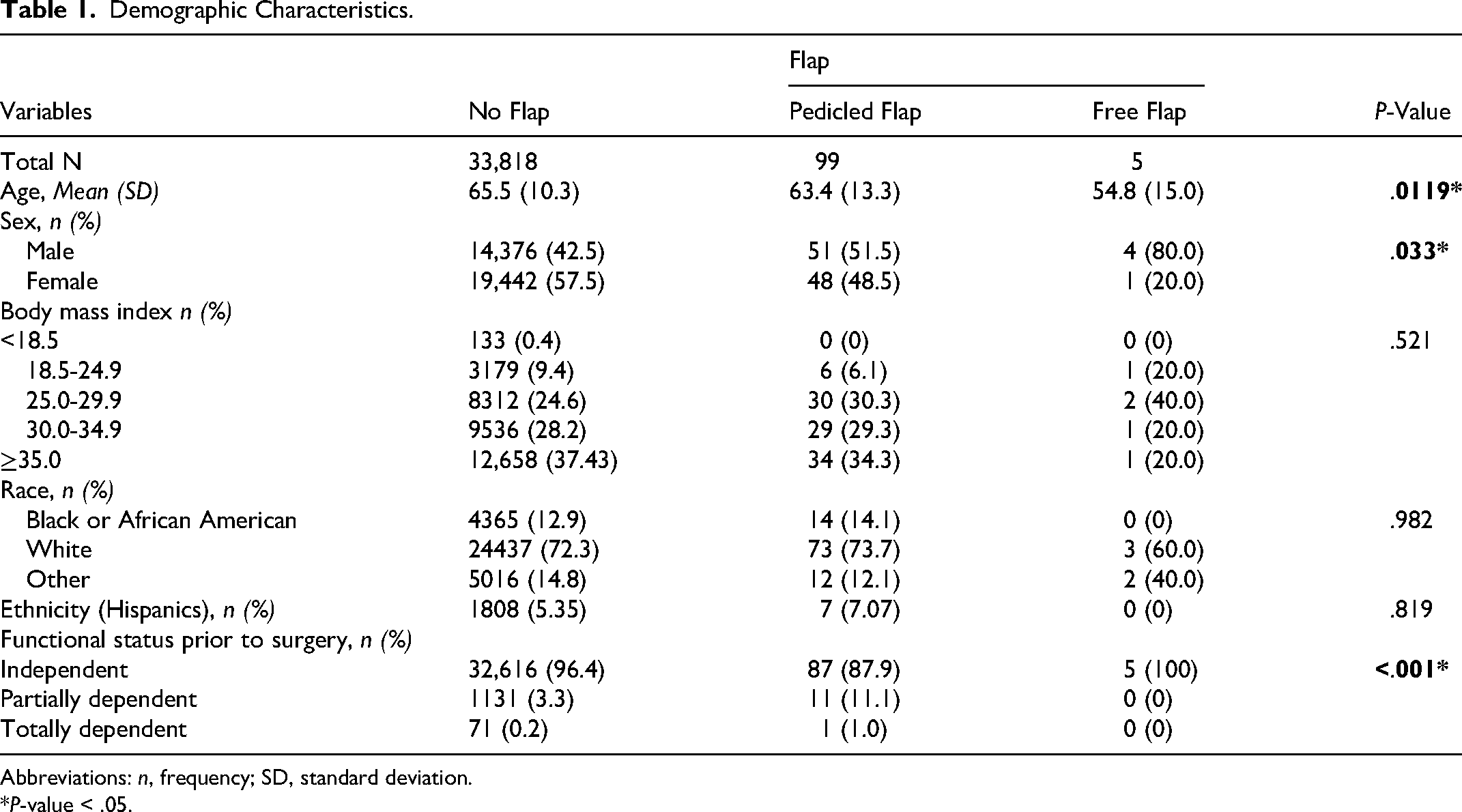
Abbreviations: n, frequency; SD, standard deviation.
*P-value < .05.
On examination of patient comorbidities, those who received flaps were unhealthier at baseline, with higher rates of acute renal failure preoperatively (P-value = .035), mfI-5 (P-value = .020), and higher rate of infected wounds (P-value < .001). Not surprisingly, patients who received flap reconstruction had longer operative times with free flaps averaging the longest at 441 min (SD 320.3), followed by pedicled flaps averaging 243.1 min (SD 103.7) and no flaps averaging the shortest operative time of 133.4 (SD 65.3) (P-value < .001). Those that underwent flaps also had longer lengths of hospital stay with patients with free flaps staying for an average of 10.4 days (SD 10.1), pedicled flaps staying for an average of 7.2 days (SD 5.5), and patients without flap reconstruction staying for an average of 3.5 days (SD 3.9) (P-value < .001). In this study cohort, no other significant differences between examined comorbidities and perioperative risk factors were present (Table 2).
Comorbidities and Perioperative Risk Factors.
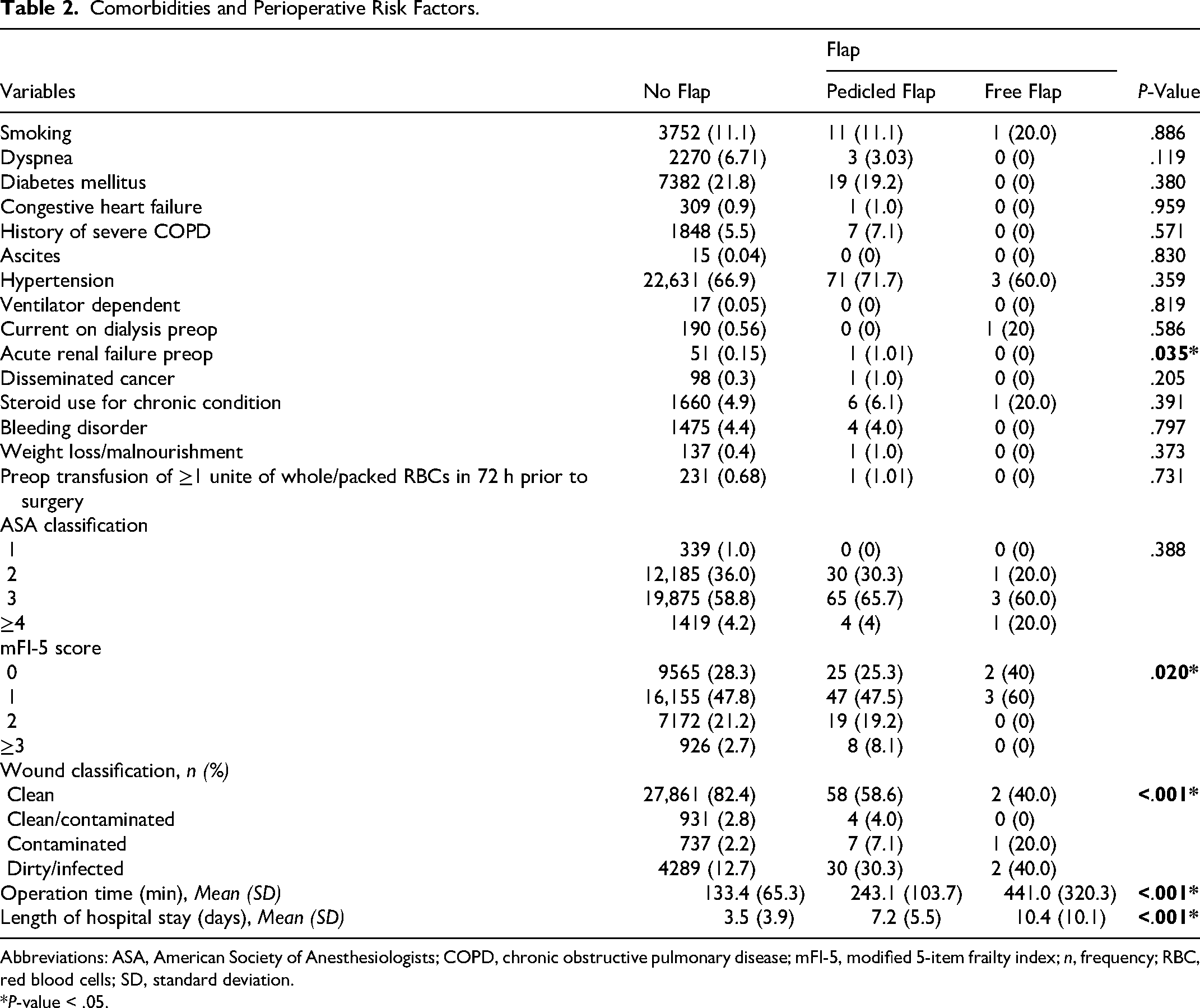
Abbreviations: ASA, American Society of Anesthesiologists; COPD, chronic obstructive pulmonary disease; mFI-5, modified 5-item frailty index; n, frequency; RBC, red blood cells; SD, standard deviation.
*P-value < .05.
On univariate logistic analysis, there were significant differences between patients who underwent flap reconstruction versus those who did not. Patients who received flaps had higher rates of superficial SSI (P-value < .001), organ/space SSI (P-value < .001), and wound dehiscence (P-value = .002), which were 3.8%, 10.3%, and 2.2% higher than the group who did not, respectively. With regard to mild systemic complications, flaps had a 17.1% (P-value < .001) higher rate of bleeding with transfusion. With regard to severe systemic complications, flaps had a 0.9% (P-value = .026) higher rate of cardiac arrest and an 8.5% (P-value < .001) higher rate of reoperation within 30-days. No other postoperative complications differed between groups as summarized in Table 3.
Postoperative Complications.
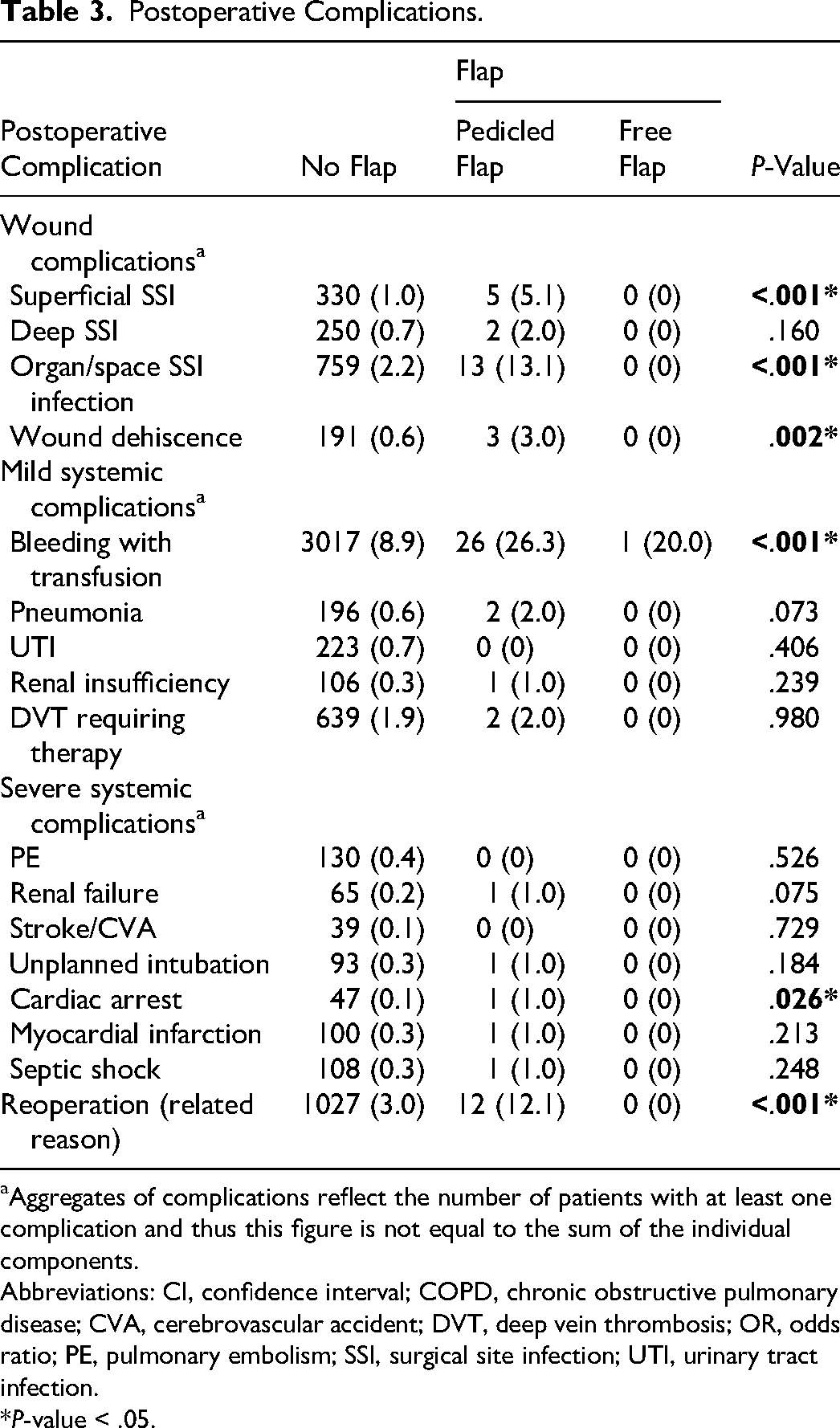
Aggregates of complications reflect the number of patients with at least one complication and thus this figure is not equal to the sum of the individual components.
Abbreviations: CI, confidence interval; COPD, chronic obstructive pulmonary disease; CVA, cerebrovascular accident; DVT, deep vein thrombosis; OR, odds ratio; PE, pulmonary embolism; SSI, surgical site infection; UTI, urinary tract infection.
*P-value < .05.
Multivariable Analysis
Adjusting for propensity score, operative time, reoperation, and wound classification, flap coverage during rTKA was not associated with statistically significant differences in the odds of developing mild systemic complications (odds ratio [OR] = 0.85, 95% confidence interval [CI] 0.52-1.41, P-value = .534), severe systemic complications (OR = 0.495, 95% CI 0.118-2.087, P-value = .338), dehiscence (OR = 0.58, 95% CI 0.16-2.1, P-value = .41), or superficial or deep incisional surgical site infection (OR = 1.88, 95% CI 0.79-4.47, P-value = .152). However, operative time was significantly associated with an increased risk of both mild and severe systemic complications, with each additional minute of operative time increasing the odds by 0.9% (OR = 1.008, 95% CI 1.008-1.009, P-value < .001) for mild systemic complications and each additional minute of operative time increasing the odds by 0.2% for severe systemic complications (OR = 1.002, 95% CI 1.001-1.003, P-value < .001).
Reoperation was a significant predictor of complications, associated with 1.83 times greater odds of mild systemic complications (OR = 1.85, 95% CI 1.58-2.16, P-value < .001) and severe systemic complications (OR = 4.65, 95% CI 3.60-6.02, P-value < .001). Interestingly, reoperation was associated with a significantly reduced risk of dehiscence (OR = 0.008, 95% CI 0.006-0.012, P-value < .001). However, reoperation dramatically increased the odds of developing superficial or deep incisional SSI, with patients who underwent reoperation having 16.26 times greater odds of developing this complication (OR = 16.26, 95% CI 13.52-19.56, P-value < .001).
Wound classification also had a significant impact on patient outcomes. Patients with contaminated, dirty, or infected wounds had 2.56 times greater odds of developing mild systemic complications (OR = 2.57, 95% CI 2.37-2.79, P-value < .001) and severe systemic complications (OR = 2.82, 95% CI 2.34-3.41, P-value < .001), compared to those with clean wounds. These patients also exhibited a 1.71-fold increase in the odds of developing superficial or deep incisional SSI (OR = 1.71, 95% CI 1.42-2.06, P-value < .001). The outcomes of the multivariate logistic regression model adjusting for propensity score matching are demonstrated in Table 4.
Multivariate Logistic Regression Model With Propensity Score Matching.
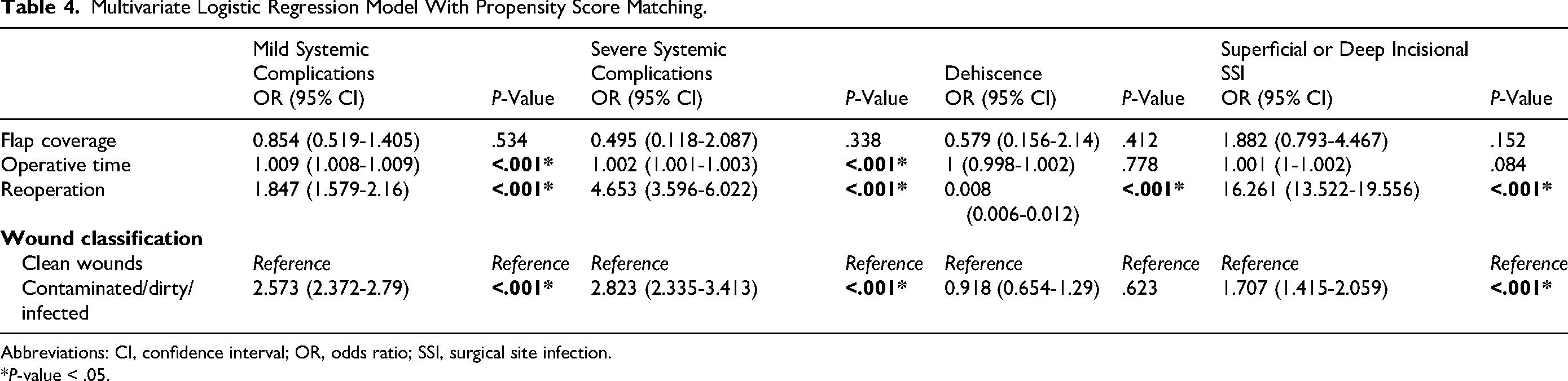
Abbreviations: CI, confidence interval; OR, odds ratio; SSI, surgical site infection.
*P-value < .05.
Discussion
Understanding the outcomes of patients undergoing rTKA with or without flap coverage is crucial for optimizing surgical approaches and patient care. Although TKA is a common procedure with a 6.2% to 12% 10-year revision rate and prophylactic flap reconstruction prior to primary TKA has been shown to provide superior patient outcomes in prior studies, there has been limited evidence of their utility in rTKA. 4 Our study aimed to evaluate the impact of flap coverage on wound complications and mild/severe systemic complications following rTKA on a national level using data from NSQIP. We observed that prophylactic flap coverage is uncommon in rTKA (0.3%), but when they are utilized, they are commonly used in cases with complex, contaminated, or infected wounds, and our findings provide nuanced insights into its effects on postoperative outcomes.
Flap coverage in rTKA was associated with several notable outcomes. On univariate analysis, patients who received flaps had more superficial skin infections, organ/space surgical site infections, wound dehiscence, cardiac arrest, episodes of bleeding requiring transfusion, and rates of reoperation. However, when adjusting for propensity score and controlling for wound classification, operative time, and reoperation on regression analysis, patients who underwent flap coverage during rTKA had no significant difference in odds of developing wound dehiscence. Flap coverage was also not a significant predictor of mild or severe systemic complications, or superficial or deep incisional surgical site infections on multivariate regression analysis. This finding suggests that the use of flaps in rTKA does not inherently lead to wound breakdown or greater risk of complications. This is a notable finding, as flap patients often had higher preoperative frailty scores and more contaminated or infected wounds, making them inherently more susceptible to postoperative infections.
On multivariate logistic regression with propensity score matching, while flap coverage was not a significant predictor of increased complications, dirty wound classification was. Patients with contaminated/dirty wounds had significantly increased odds of mild (OR = 2.57) and severe systemic complications (OR = 2.82), as well as surgical site infections (OR = 1.71), P-value < .001. Hence, our data suggests that the higher rate of systemic complications and surgical site infections seen in flap patients are likely due to the complexity of the original wound and possibly lack of adequate source control, rather than the reconstruction itself. These findings underline the complexity associated with cases in which flap coverage is employed, highlighting the need for meticulous preoperative and postoperative management.
The demographic characteristics of the flap group, such as younger age and higher proportion of men, along with poorer preoperative functional status and higher rates of infected wounds, further suggest that flap coverage is often reserved for more challenging cases. This supports the notion that flap coverage is employed in higher-risk scenarios where traditional wound management might be insufficient. Patients considered for prophylactic flap surgery in rTKA should undergo a careful risk and benefit analysis, and decision making should be shaped by thorough assessment of individual patient characteristics such as age, wound classification, and functional status.
These findings align with observations in other surgical specialties, such as vascular surgery, neurosurgery, thoracic surgery, and head and neck surgery, where the use of flap coverage is often reserved for complex wounds in patients with higher baseline risk of complications and greater comorbidity burden.11–18 Such parallels underscore the importance of interpreting complication rates in the context of patient and wound characteristics. As in other surgical fields, the increased complication rates in our study should not be viewed as a direct consequence of flap coverage itself but rather as a reflection of the high-risk nature of the cases in which it is employed.
Our results also align with previous studies that have demonstrated both benefits and challenges associated with flap coverage in TKA, reinforcing its role in complex knee reconstruction. For instance, Casey et al and other high-volume centers have shown improved outcomes with flap coverage, particularly in prophylactic settings as opposed to a salvage procedure.3,9,19–21 Although complications such as recipient site wound healing issues may still occur in association with the flap surgery, high risk patients who undergo prophylactic flap coverage have better outcomes than those who undergo reactive flap coverage as a salvage procedure. 9 Similarly, a 12-year retrospective review of all TKA and rTKA procedures with flap reconstruction between 2008 and 2019 in a high-volume tertiary arthroplasty hospital reported favorable functional and patient-reported outcomes in both scheduled noncomplicated and emergent noncomplicated cases. 4 However, this study included a heterogeneous patient population, varying in etiology, comorbidities, age, and rTKA versus TKA status, which limited direct comparison. 4 Further supporting the benefits of prophylactic flap reconstruction, Kwiecien et al found that patients without pre-existing soft tissue defects who underwent prophylactic flap coverage during rTKA demonstrated a trend toward better mental health scores and significantly better physical health scores, as self-reported on the Short Form-12 survey measured at follow up, compared with patients with pre-existing soft-tissue defects who required reactive flap reconstruction. 3
Additionally, our results indicating that each additional minute of operative time increases odds of mild systemic complications by 0.9% and severe systemic complications by 0.2% (P < .001), aligns with existing literature suggesting that longer procedures increase physiological stress and blood loss, and may be associated with the increased complexity of the surgical procedure.22–26 For the same reasoning, reoperation within 30 days postprocedure increasing the odds of mild (OR = 1.85) and severe systemic complications (OR = 4.65), as well as surgical site infections (OR = 16.261) (P-value < .001) is also expected as repeat procedures introduce additional trauma and infection risk. However, our data showed that reoperation was a significant negative predictor of dehiscence, where a reoperation decreased the odds of dehiscence (OR = 0.008, P-value < .001). This may be due to reoperations addressing wound instability early, through re-suturing or reinforcement and/or additional soft tissue coverage, reducing the likelihood of further dehiscence.
Our national-level analysis emphasizes the need for a balanced approach with multidisciplinary input from orthopedic surgery, infectious disease specialists, and early plastic surgery intervention. Prophylactic flap coverage should be considered primarily for patients with significant wound issues or high infection risk, but with a comprehensive preoperative assessment to mitigate potential complications. Additionally, this approach should be complemented by robust postoperative monitoring to manage and address complications promptly.
Our study has several limitations, including the retrospective design and the reliance on NSQIP data, which may lack detailed operative specifics such as indication of the revision procedure, the exact size and nature of wounds, patient history, and antibiotic history and culture data. The short-term follow-up period of 30 days may not capture long-term outcomes, and the study's retrospective nature introduces potential unmeasured confounding variables. Future research should aim to address these limitations through prospective studies and randomized controlled trials to better understand the role of flap reconstruction in rTKA, its cost-effectiveness, and long-term outcomes.
Conclusions
Flap coverage during rTKA is primarily utilized in high-risk patients with higher odds of having contaminated or infected wounds preoperatively, poorer baseline functional status and frailty scores, longer operative times, and longer hospital stays. While these patients inherently face greater surgical risks, our findings demonstrate that flap coverage itself is not an independent predictor of wound complications, dehiscence, or systemic complications after adjusting for key confounders. Instead, preoperative contaminated wound classification, operative time, and reoperation are drivers of mild and severe systemic complications, while surgical site infection is associated with contaminated wound classification and reoperation. Notably, reoperation is associated with lower odds of dehiscence, potentially due to early wound management interventions.
These findings underscore the importance of early multidisciplinary decision making, preoperative risk stratification, surgical site optimization, and vigilant postoperative care for high-risk rTKA patients. Given the significant impact of wound classification on postoperative outcomes, strategies to improve source control and wound bed preparation prior to flap coverage may further improve outcomes. Future studies should explore long-term functional outcomes and cost-effectiveness analyses of flap reconstruction in this patient population to refine decision-making criteria and improve care pathways.
Footnotes
Ethical Considerations
This article does not contain any studies with human or animal subjects. The Institutional Review Board (IRB) at Beth Israel Deaconess Medical Center determined that this study did not constitute human subject research (determination #: 2025D000227).
Author Contributions
MM and AAW: Conceptualization, methodology.
MM, AAW, JHL, VPB: Validation.
JHL: Formal analysis, data curation.
MM, AAW, JHL: Writing—original draft preparation.
MM, AAW, JHL, VPB, SJL, ASD: Writing—review and editing.
SJL, ASD: Supervision.
MM: Project administration.
All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available, but are available from the corresponding author on reasonable request.