
Abstract
Cloud computing has been adopted by many healthcare firms throughout the world especially in developed countries to enhance their service levels. The main objective of this study was to find the constructs from the prior literature review which influence the adoption of cloud computing from the prospering nation’s perspective. The main pillars of the theoretical framework are technology, organizational, environmental and ethical factors. The responses were collected from the employees or staff who were working in this sector with the help of a structured questionnaire. The analysis was performed utilizing SPSS 20.0 and AMOS 22.0. The hypothesis developed was tested utilizing a structural equation modelling approach. The findings indicated that the assumed variables each under technology, organization, environment and ethics have an impact on the dependent variable that is cloud computing adoption in the healthcare segment, thereby increasing the efficiency. The study is unique when compared to past studies as it considered ethical factors, thereby extending the cloud computing literature. It also provides a base for future studies and cloud technology development for a prospering nation perspective.
Keywords
Introduction
This century is witnessing a lot of advancements and growth in information technology (IT). Cloud computing (CC) is considered a new innovative development and achievement in the IT field (Armbrust et al., 2010; Luo et al., 2018). CC provides utility services to clients as a service (Lee, 2019; Miao et al., 2017). John McCarthy, who was Stanford computer researcher and an artificial intelligence pioneer, and Douglas Parkhill, at that point Canada’s Assistant Deputy Minister for research, missioned in its beginning of the 1960s where calculation may sometime need to be available as an open service like water and power (McCarthy, 1961; Novais et al., 2019; Parkhill, 1966). It provides several advantages like providing a virtual platform for information storage, getting rid of physical IT infrastructures and flexibility in the accessibility of data (Brender & Markov, 2013; Mezgár & Rauschecker, 2014; Wang & He, 2014; Yazdani et al., 2020). The primary purposes of the relocation to CC is to access world-class IT services without high investment in IT infrastructure (Vu et al., 2020), for example, clients utilizing the cloud can get the services anyplace and pay as per usage.
CC has been adopted in both prospered and prospering nations, but prospered nations are well advanced when compared to prospering nations worldwide. Despite multiple benefits, the prospering nations need to realize their advantages. To date, most of the studies are done in prospered nations like the United States, United Kingdom, and so on and a negligible number of studies are done in prospering nation context. Even the technological, organizational and environmental (TOE) perspective, for developed countries, differs from the developing countries. An ethical context that has been identified in this study will also affect the cloud computing adoption (CCA) for developing countries. For instance, if we consider technological perspectives (TPs) in the United States or United Kingdom, which is a prospered nation is more advancing when we compare it with a prospering nation like India. As a result, the findings of a study performed in a prospered nation will not apply to the prospering nation (Avgerou, 2001; Effah, 2014; Heeks, 2002; Senyo et al., 2016). At present, there are no such studies in the Indian healthcare context. The current study provides a clear understanding of influencing technological, organizational, environmental and ethical (TOEE) factors to adopt CC in Indian healthcare firms.
This study examines the factors for CCA in the Indian healthcare context which is a developing nation with the help of a survey method. The proposed TOEE context in this study will be very helpful because most of the prior studies only consisted of TOE perspectives but the ethical perspective (ETP) was neglected and hence the various sub-factors for ETP are also included in this study for CCA in the Indian context. As ethics play an important part in adopting any new kind of technology, it is an equally important factor along with the other three factors. As CC is in the infant stage, so exploring this area is advantageous. As per the prior literature, most of the prior studies have been done in the manufacturing sector and the health sector is neglected, hence, in this study healthcare sector is chosen as the area of research. This study consists of TOEE framework that makes it more valuable due to the presence of ethical context in it. Ethical parameters are compliment to the prior TOE framework. This study will also help the decision-makers of the healthcare firms, while considering CCA in various Indian healthcare firms.
Rest of the paper is as follows: The second section discusses the literature survey. The third section discusses the research model and hypothesis development. The fourth section discusses the research methodology which includes sampling techniques utilized for collecting data and demographics of respondents. The fifth section discusses the data analysis which includes reliability, exploratory factor analysis (EFA), confirmatory factor analysis (CFA) and structural equation modelling (SEM) approach for establishing the model fit. The sixth section contains discussion of the current study, contribution to research and practice and managerial implications and finally the seventh section contains the conclusion, scope and future research directions.
Literature Review
For a long time, IT has been referred to as a product, but now the notion has changed and it is now claimed to be a service. CC can be described in broader contexts. CC is described by the NIST as ‘a model for enabling ubiquitous, convenient, on-demand network access to a shared pool of configurable computing resources (e.g., networks, servers, storage, applications and services) that can be rapidly provisioned and released with minimal management effort or service provider interaction’ (Kong et al., 2015; Manuel Maqueira et al., 2019). CC has been referred to as a technology that can help in scaling IT-related capabilities as a service to the clients who are using the cloud services from the providers and are charged as per the usage (Senyo et al., 2016).
Delivery and Deployment Models of Cloud
CC gives three distinct kinds of services: software-as-a-service (SaaS), infrastructure-as-a-service (IaaS) and platform-as-a-service (PaaS) (Armbrust et al., 2010). SaaS enables purchasers to get applications on interest over the system, in light of the pay-per-utilize (Chen et al., 2010; Saldanha & Krishnan, 2012). The distinction between PaaS and SaaS is that the PaaS can convey both finished and in-advance applications, whereas SaaS can have just the finished cloud applications. Instances of SaaS are Google Mail and Salesforce.com (Dillon et al., 2010; Kopanaki et al., 2018). IaaS offers distinctive kinds of the principal asset (e.g., storage, operating systems, database and networking) as a service for clients, who can control these assets. Be that as it may, the clients are unfit to deal with the basic cloud framework (Chen et al., 2010; Mell & Grance, 2009). The instances of the IaaS model is GoGrid (Chen et al., 2010). Next is PaaS, which gives the entire programming lifecycle as an administration for clients (Addo-Tenkorang & Helo, 2016; Dillon et al., 2010). It is intended to support programming designers to manufacture and build up their applications on the cloud utilizing distinctive dialects and apparatuses (Zissis & Lekkas, 2012). The instance of the PaaS model is Google App Engine (Foster et al., 2008).
There are four deployment models through which cloud services are offered: private, public, community and hybrid. To begin with, the private cloud offers interior usage of innovations that are kept up in house. Private cloud is restrictive to a firm and managed by the firm itself. Next cloud is public which gives services to the overall population which includes firms and people. Public cloud are generally owned and then directed by third-party organizations. Some prominent public cloud administrations are SalesForce.com, Google AppEngine, S3 (Simple Storage Service) and Amazon EC2 (Elastic Cloud). Community cloud provides cloud service to gathering of firms with tantamount trade aim, security and contract document requirements. Participation of gathering is compared to a network where mutual interest individuals share. Cloud benefits that the community expands are to individuals. The hybrid cloud gives a mix of all the three, that is, community, public or private deployment empowered by a regulated innovation which guarantees portability of information and application (Jula et al., 2014; Mell & Grance, 2009; Senyo et al., 2016; Wai-Ming et al., 2013; Yang & Tate, 2012). Apart from these main service delivery models, various varieties are, as of now, found in the writing. In any case, it is important that there are three-principle models only for delivery of service and rest are all off-shoots from the three (Mujinga, 2012; Senyo et al., 2016).
Cloud Computing Adoption
CCA can be studied both from prospered and prospering nation perspectives. Relevant and significant contributions have been made from the perspective of prospered nations according to studies like Gangwar et al. (2015). Low et al. (2011) recommended a model setup on TOE framework. The reason for examination was distinguishing components and decides their effects on the choice to embrace CC in Taiwan for advanced education. The eight components recognized in this model are trading partner pressure, competitive pressure, compatibility, top management support, complexity, technology readiness, firm size and relative advantage. Chang et al. (2013) further concentrated that depending on the TOE framework and diffusion of innovation (DOI) theory, meaning to explore the variables that influence CC appropriation in Vietnamese organizations. In their examination, they distinguished various components, like the previous investigation. It is detectable that these investigations have not considered security factors that may influence the firms’ choice to receive CC, even though one of the principal worries for a firm is the security which needs attention. Likewise, Nkhoma and Dang (2013) built up a theoretical model utilizing the system of TOE to inspect the advantages and boundaries of receiving CC just as its effect of technological and environmental perspectives (EPs) on the adoption process. They distinguished various hindrances as variables that impact the expectation to utilize CC. One of these hindrances is security, which is the fundamental worry for the greater part of the undertakings because putting away their information under the control of another party makes them feels unreliable. Availability and reliability are another two variables. Any mistakes or defers that influence the accessibility or unwavering quality of the service providers may cost the firms a great deal of loss. Abdollahzadegan et al. (2013) examined organizational factors’ impact on CC reception in small and medium sized enterprises (SMEs). Three components were distinguished (higher administration backing, innovation availability and firm size) utilizing the TOE structure. There are three elements or factors like firm size, top administration support and innovation availability. Borgman et al. (2013) recommended a framework dependent on the TOE system for looking at elements that impact a firm’s expectation to embrace benefits of cloud just to recognize the effect of IT administration procedures and structures. The elements recognized in this model are competitive pressure, compliance with guidelines, top management support, firm size, compatibility, complexity and relative advantage. The information was gathered utilizing structured interviews in this study. The recommendation was given that just the three elements, that is, the relative advantage, the top management support and the competitive pressure, positively affect cloud adoption. Likewise, this examination disregarded the security viewpoints that may influence a firm’s choice.
Oliveira et al. (2014) build a model to surveying components impacting cloud selection in Portugal’s assembling and services divisions. They recognized various elements dependent on the DOI theory and the TOE structure. The information was gathered utilizing a questionnaire with Portugal firms in the study. Among the variables inspected, their discoveries demonstrated that higher authority support, firm size, technological readiness, relative advantage and complexity legitimately affected the selection of cloud in these firms. Gutierrez et al. (2015) recommended a model utilizing the TOE system to inspect elements which may affect the adoption of CC in the UK firms. The components distinguished in this examination were competitive pressure, firm size, trading partner pressure, technology readiness, top management support, compatibility, complexity and relative advantage. Their recommendations demonstrated that just four elements, which are trading partner pressure, competitive pressure, technology readiness and complexity, have a critical effect on the adoption of cloud decision. Senyo et al. (2016) contemplated CCA in various firms operating in Ghana utilizing the framework of the TOE system. The discoveries from the investigation showed that CCA determinants such as security, relative advantage, technology readiness, higher administration support, trading partners and competitive pressure were found to be a significant contributor of CCA. Miao et al. (2017) conducted a study on adoption intentions on mobile health where SEM approach has been utilized to identify the factors which may be useful for the adoption process of m-health for patients suffering from chronic diseases. The study on each sector may be unique from the other. Singh et al. (2017) discussed the challenges and reasons faced by Indian healthcare firms for adopting CC. The study theoretically stated that the healthcare centres are interested in adopting this advanced technology. But due to lack of IT infrastructure and change from the traditional system, they are hesitating to accept the change. Sharma et al. (2020) conducted a study on CCA for higher educational institutes of India where a fuzzy Analytic Hierarchy Process (AHP) approach was utilized to identify the factors which will be impacting its adoption where they discussed technology, organization and economic factors. They also stated that there is a need to conduct survey-based research which should include a large population as well as similar study should be conducted in other specific sectors (like manufacturing, healthcare, etc.) to understand the actual CCA circumstances.
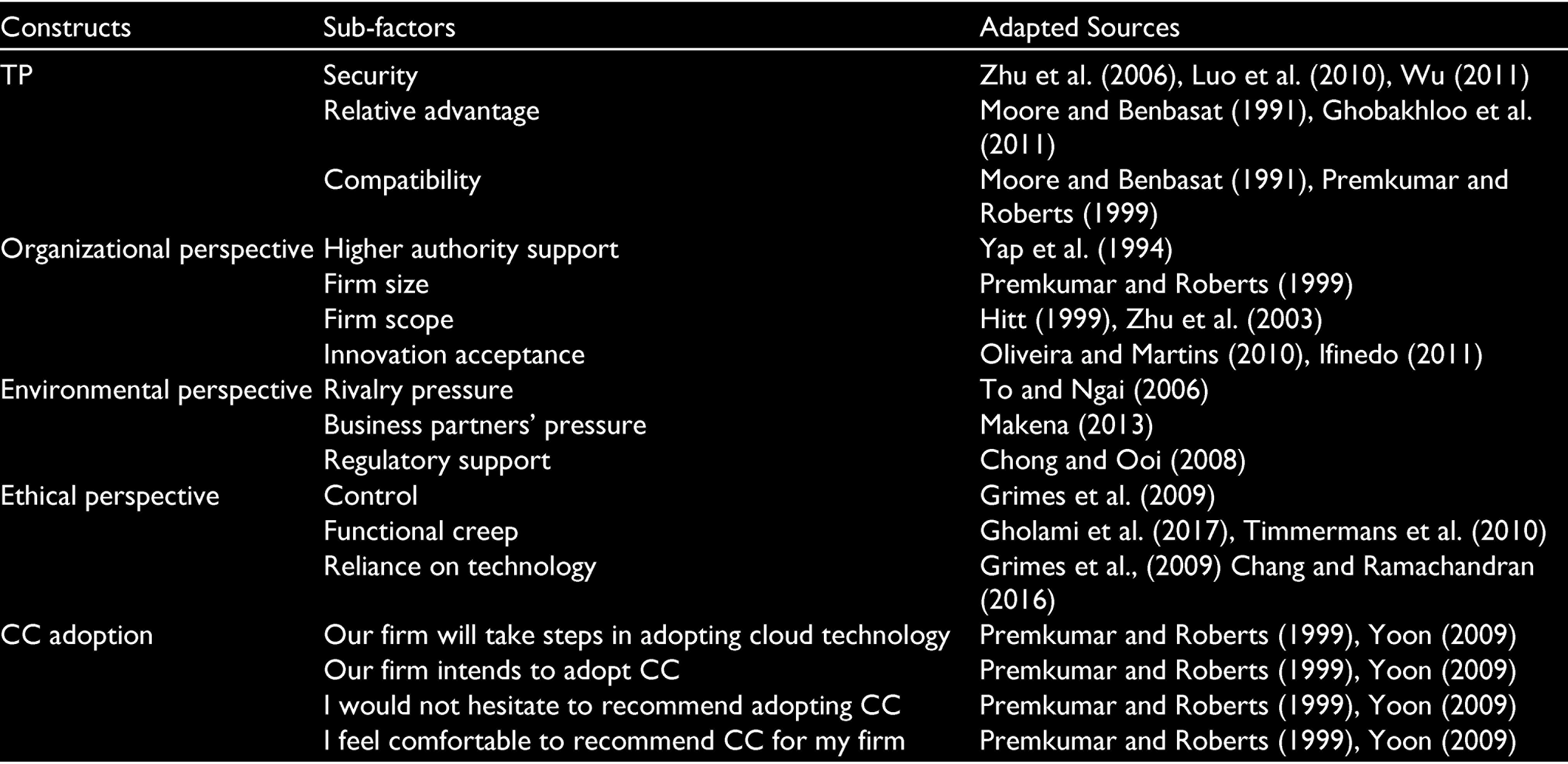
Prior studies have made a significant contribution in a few developing nations’ contexts (Low et al., 2011; Makena, 2013; Rawal, 2011; Senyo et al., 2016; Sharma et al., 2020). The study done by Senyo et al. (2016) stated that firm size is not a significant contributor to CCA. These prior studies have discussed only TOE framework for CCA in various segments whether the study is based on developing or developed context. ETP has been neglected and not discussed yet and hence along with the technological, organizational and environmental context in this study ethical context has been considered for CCA in the healthcare segment. Also, the prior studies have not considered specifically the healthcare segment which has been fulfilled in the current study. Table A1 provides the list of factors which are found from extant literature as determinants for CCA and Table A2 provides the list of adapted scales which are found from extant literatures.
Research Model and Development of Hypothesis
Prominent adoption of theories and frameworks such as the technology adoption model (TAM), the DOI, the grounded theory, migration theory, the theory of reasoned action (TRA), the TOE framework and so on are utilized in the existing literature of CC. Additionally, it has been seen that two different frameworks are utilized in the study of CCA, to be specific, firm adoption (meso-level adoption) and individual adoption (micro-level adoption). For example, DOI, TAM and TRA are evident in innovation adoption.
Different Frameworks
Davis (1989) created TAM which is an acknowledged model for understanding new technology adoption and its utilization across a worldwide context. This model tries to clarify the relationship between technological innovative acceptance and adoption accordingly, behavioural intension to utilize it (Gangwar et al., 2015). TOE was proposed by Tornatzky and Klein (1982) to break down the adoption of the new IT innovations at firm levels. It incorporated the effects of the three variables (technology, organization and environment) on a firm’s choice for embracing another innovation in the market. It incorporates technological, organizational and environmental factors which make it beneficial over other adoption models in studying technological innovation acceptance, innovation use and value creation from the innovation development (Gangwar et al., 2015; Ooi et al., 2018; Senyo et al., 2016). The theory of DOI states individuals receive new thought, behaviour or products as new or creative. Researchers found that individuals who adopt an innovation early have better qualities in comparison to individuals who adopt a development later. In any case, the constraint to the theory is adoption classes did not start in public health and it was not created to explicitly apply to the selection of new innovations or health innovators and it likewise does not consider a person’s assets or social help to adopt new innovation or behaviour. TRA explains relationships among behaviours within human action and attitudes, however this theory is restricted regarding having the capacity to foresee practices that expect access to specific chances, skills, conditions or assets. As this paper explores the CCA determinants among healthcare firms, the TOE framework addresses the factors of TOE and is treated as a suitable theoretical framework. This framework was produced to examine firms’ choice to accept and execute an inventive innovation contemplating the context of TOE (Tornatzky & Klein, 1982). Along with these three contexts in this study, ethical context has also been considered for CCA as it has been neglected part in prior studies. So, the TOEE context is proposed in this study.
TOEE Framework
The proposed model for the study is the TOEE model where technological, organizational, environmental and ethical perspectives are to be considered for identifying different factors which are critical for CCA in healthcare firms. In the current study, the TOEE perspective will be helpful as most of the prior studies only consisted of technological, organizational and environmental perspectives but the ethical perspective has been neglected and also various sub-factors for ETP are also included in the current study for CCA in Indian healthcare firms’ perspective. In todays’ scenario, ethics plays a very critical role in adopting any new kind of technology and it is an equally important factor along with the rest three factors. The TOE framework discusses relative advantage, security, compatibility, firm scope, firm size, technology readiness, top management support, regulatory support and trading partners’ pressure (Senyo et al., 2016) but the ethical factors like control, reliance on technology, proscriptive pressure and compliance are neglected in prior studies (de Bruin & Floridi, 2017). The factors that are identified under the ETP are also important for CCA in various healthcare firms. As a result, the TOEE framework is suggested in this study for ease of understanding the advantages of CCA in healthcare firms of prospering countries like India.
Development of Hypothesis
Based on TOEE and related literature in IT, the current study came out with a model which includes various components of technology, organizational, environmental and ethical for CCA in Indian healthcare firms.
Technological Perspectives
It involves the internal and external technologies that firms can use in their trade purpose. Advancements that are, as of now, being utilized by any firm effect choice of adopting CC as they decide the limit and extension of change in technology that a firm can acknowledge. It likewise grasps the software, networks, hardware and how they are adjusted in a compelling way to accomplish the accepted procedures of CCA (Awa et al., 2015; Kansal & Chana, 2012). There are deficiencies of studies that consider technological attributes while studying factors influencing IT adoption choice (Ooi et al., 2018). Following indicators were taken under TP: relative advantage (RA), security concern (SC) and compatibility (COM) and has been embraced from earlier studies such as Alshamaila et al. (2013) and Gao and Sunyaev (2019). As per prior studies, RA is characterized as the dimension to which an element is identified with technology that can provide more gain to the firms (Schneider & Sunyaev, 2016). CC guarantees different benefits to firms that embrace it, for example, proficient coordination among firms, speed of business communication, better client communication and approach to market information mobilization (Low et al., 2011). Different advantages of CC incorporate diminished costs, flexibility, scalability, portability, pay-per-utilize and shared assets (Miller, 2008; Gutierrez et al., 2015). The pay-per-use feature also is an added advantage of CCA (Senyo et al., 2016). SC is a prime concern for many firms as one feels that the information is not safe and secured in the cloud due to lack of direct control over them (Senyo et al., 2016; Sultan, 2014; Zissis & Lekkas, 2012). There is a lack of trust and confidence in most of the firms in the developing countries on these advanced technologies. Prior studies have not stressed this as a critical factor (Premkumar & Ramamurthy, 1995; Thong, 1999; Zhu et al., 2003). But the study done by Senyo et al. (2016) have fulfilled this gap. Hence, it is also considered for the current study. COM alludes to the advancement which fits the potential adopter’s previous practices, existing qualities and present needs (Rogers, 2003). It is considered as a fundamental factor for endorsement of new IS developments where the healthcare firms will probably adopt these advanced technologies if being compatible with existing applications and the firms’ esteem and convictions. It has been considered as an important element in prior studies done such as Gutierrez et al. (2015), Alharbi et al. (2017), Singh et al. (2017) and Ayoobkhan and Asirvatham (2017). As a result, all the indicators are also identified from various prior studies under TP and hence the proposed hypothesis is given as follows.
H1a: Technological perspective influences cloud computing adoption in healthcare.
Organizational Perspective
Organizational perspective (OP) consists of the internal characteristics and assets of a firm (Amini, 2014). New research identifies firm scope (FSC), firm size (FS), higher authority support (HAS) and innovation acceptance (IA) as variables that should be considered in the adoption of technology (Alshamaila et al., 2013; Gao, & Sunyaev, 2019; Low et al., 2011; Makena, 2013; Oliveira & Martins, 2010; Tornatzky & Klein, 1982). As per prior studies (Rogers, 2003), FS is a standout among the most basic determinants for CCA. Furthermore, Pan and Jang (2008) express that the huge firms had a greater inclination for receiving new innovative advancements, especially because of their prevalent flexibility, aptitude and risk-taking capacity. As per Senyo et al. (2016), various investigations are uncovering a positive correlation, while other investigation reports an adverse correlation. In general, it tends to have contended that bigger firms have the right stuff, experience and assets to endure any potential disappointments better than smaller firms. Be that as it may, smaller firms can be more innovative and flexible because of their size and lower levels of bureaucracy. The ‘pay-per-utilize’ highlight of CC makes it more demanding for littler firms to likewise embrace CC (Senyo et al., 2016). Therefore, it is considered in the current study. FSC means the operating area in which the firm or organization functions. CC disregards geological limitation. In this manner, firms with branches far and wide are most appropriate to adopt CC. There is a positive relationship between FSC and the adoption of IT in the past (Oliveira & Martins, 2010; Zhu et al., 2003). But a recent study has shown a negative relation between CCA and FSC (Senyo et al., 2016). Hence, it is considered as an indicator in the current study. HAS assumes a significant role in the beginning, implementing and accepting new technologies as they have a significant role in setting the organizational strategy and establishing functions and benefits for CC (Lian et al., 2014). CCA involves a lot of challenges like expense, risks and so on. As a result, HAS plays a major role before and after CCA in various firms. In the prior studies (e.g., Alshamaila et al., 2013; Pan & Jang, 2008; Premkumar et al., 1997; Zhu et al., 2003). HAS has been considered an important component and it has a positive impact. Hence, HAS has been considered as an indicator in the current study. IA means to grasp innovation for achieving objectives that are controlled by the general perspective coming about because of a gestalt of mental benefactors and inhibitors. It implies the preparation of the framework and human resources of IT who are required to support cloud selection. Firms can be divided into five enhanced gatherings reliant on their IA, from pioneers those are the first adopter of another development to slowpokes those are last adopters and are not motivated technologically (Parasuraman & Colby, 2001). Firms that have technological readiness are better prepared for CCA. Hence, IA is an important factor for CCA. As a result, all the indicators are also identified from prior studies under OP and hence the proposed hypothesis is as follows.
H1b: Organizational perspective influences cloud computing adoption in healthcare.
Environmental Perspective
It is imperative to consider issues on the environment relating to innovative selection choices of healthcare firms. Prior investigations (Chong & Ooi, 2008; Kung et al., 2015; Low et al., 2011; Oliveira & Martins, 2010; Wu and Subramaniam, 2009; Zhu et al., 2003) had recognized factors, for example, industrial pressure, rivalry, access to assets provided by others and bureaucracy matters as significant factors of adoption. The environmental factors utilized in this study include rivalry pressure (RP), business partners pressure (BPP) and regulatory support (RS). These factors are viewed as essential since they have a considerable impact on the accomplishment of healthcare firms. RP is the level of pressure that a firm faces from their rival firms in the same kind of industry. RP can expect positive employment in new innovation selection especially when the development impacts the opposition (Ramdani et al., 2009). Thus, firms that are first to CC adoption are required to infer gains in terms of survival and competitive advantage (Gangwar et al., 2015). Hence, RP is considered as one of the indicators in the current study. As per the prior study, BPP is a significant contributor (Chong & Ooi, 2008; Pan & Jang, 2008). BPP is distinguished as an instigator of acceptance (Laforet, 2011). This peer can expect positive employment in new innovation selection especially when the development impacts the opposition (Ramdani et al., 2009). Thus, firms that are first to adopt CC are required to infer gains in terms of survival and competitive advantage, which will influence other healthcare firms to CCA (Alharbi et al., 2017; Gangwar et al., 2015). Hence, BPP is considered as one of the indicators in the current study. RS come as legislation that tries to protect and promote healthcare firms that embrace development (Makena, 2013; Nkhoma & Dang, 2013). There is no regulation in India that specifically prohibits, restricts or governs CCA. CC challenges geological limits and is available in various nations. In this manner, legitimate support is regarded as critical to security firms that receive CC as laws change from nation to nation (Senyo et al., 2016). Hence, in this study, we have considered RP as an indicator. As a result, all the indicators are also identified from various prior studies under EP and the proposed hypothesis is as follows.
H1c: Environmental perspective influences cloud computing adoption in healthcare.
Ethical Perspective
In CCA, there are various factors that give rise to issues related to ethics. Prior studies have identified various factors related to ethics. The factors which are identified in previous theoretical studies are privacy and security, educational pressure, proscriptive pressure, compliance, functional creep and performance metrics (de Bruin & Floridi, 2017; Gholami et al., 2017; Timmermans et al., 2010). The factors which have been considered in this study are control (CO), functional creep (FC), reliance on technology (RT) and proscriptive pressure (PP). As per prior studies, CO has been considered as an important element as it assumes an imperative job in information protection and control (Timmermans et al., 2010). Any information that used to be secured locally is secured in the cloud. The client in this manner puts his calculation and information on machines he cannot directly control. In this way, to a substantial expand, clients or clients of a CC service give up authority over information and computation (Grimes et al., 2009; Haeberlen 2010). If something goes wrong, then due to loss of control on data, it becomes problematic. Hence, CO is considered as an indicator in the current study. FC means information collected for one purpose may be utilized for another purpose. For instance, a directory with biometric data of nationals may be expected for affirmation purposes, however may then end up being exceptionally useful for crime investigations (Timmermans et al., 2010). Hence, FC is considered an important element and is considered as an indicator for the current study. RT is an important element because there may be a possibility that data stored may be hacked by the hackers also there may be an involvement of cloud providers for the same. As data or information is not gathered locally, authority over the information is moved to the service providers. The service purchasers need to have trust in the cloud service providers. The offshoring of information likewise brings up the issue of who possesses the information a client stores in the cloud and what can the suppliers of cloud administrations do with this data. The two reasons infer that to users it will not generally be clear what they can anticipate from specialist organizations in the cloud concerning privacy (de Bruin & Floridi, 2017; Grimes et al., 2009; Murley, 2009; Timmermans et al., 2010). Hence, in the current study, RT has been considered as an indicator. As per prior studies, PP is also an important element for the study under ethical issues. Insignificant PP must be put on facilitating firms and suppliers of clouds, however that fairly broad PP might be applied on the business cloud. The case is not that developing clearly damaging innovation should be allowed; it does not immediately apply to nuclear power, say, the risks of which are to some degree clear to choose. On the other hand, possibly, the musing is that in a condition in which clear indications of real disadvantage threats are so far lacking, government bans are untimely. If we consider this viewpoint, the CC industry requires just minor proscriptive pressure. It is confined to the underlying phases of equipment advancement, since drawback dangers may wind up noticeable en route; and if that occurs, government strategy may be reconsidered (de Bruin & Floridi, 2017). Hence, PP is considered an important element and is considered as an indicator in the current study. As a result, all the indicators are also identified from various prior studies under ETP and the proposed hypothesis is as follows.
H1d: Ethical perspective influences cloud computing adoption in healthcare.
Research Methodology
Data were collected by secondary and primary sources. Secondary sources include a literature review and other reports, and the primary source includes a collection of data through a structured questionnaire. The reliability test of the questionnaire was also done. The target population was healthcare centres running in India. The respondents have been taken from the employees who had IT information about the present and future tasks of their healthcare firms. As SEM has been utilized in this analysis and for this 200 and above sample size is considered adequate (Anderson & Gerbing, 1988; Hair et al., 2010; Kline, 2011). Hence, the questionnaire was sent to 650 respondents individually but we only got 350 filled responses. A simple random sampling method has been used so that the results can be generalized more appropriately and allows the presence of various healthcare firms (Hair et al., 2010). After data cleaning in SPSS 20.0, the usable responses used for the analysis was 278.
To avoid common method bias, the research team has taken a few fundamental precautions during the pre-data collection stage. A note was mentioned at the beginning of the questionnaire that indicated that the survey is intended for academic research and confidentiality of data will be maintained. In the gathered data set, first cleansing was finished by case screening, trailed by factor screening, so clarification can be given for variations in the information. Information cleaning measure had been reasoned that missing information had been extremely sparse and in this way, they were not viewed as a principal supporter of any predisposition. No cases were therefore removed. However, after the data was collected, the research team applied Harman’s single factor test. EFA was performed and the results show that the first factor explains maximum covariance (35.813%) which is below the recommended value of 50% (Podsakoff et al., 2003). So, common method bias is not a concern in the current study.
SEM and EFA methods were adopted for data analysis. The data analysis was done in four stages: analysis of demographics, validity and reliability test, EFA and SEM approach. EFA was done to check the total variance explained to identify and group the variables using a rotated component matrix table. SPSS 20.0 was utilized for reliability tests and EFA on data collected. After that, CFA was implemented for testing and approving the applied models underlying. AMOS version 22.0 was being used for CFA on collected information for measuring model outcomes as CFA decides whether a validity test on an estimated model be replicated (Byrne, 2010; Hair et al., 2010). At last, the model fit was determined by SEM for testing the hypothesis.
Demographics of the Respondents
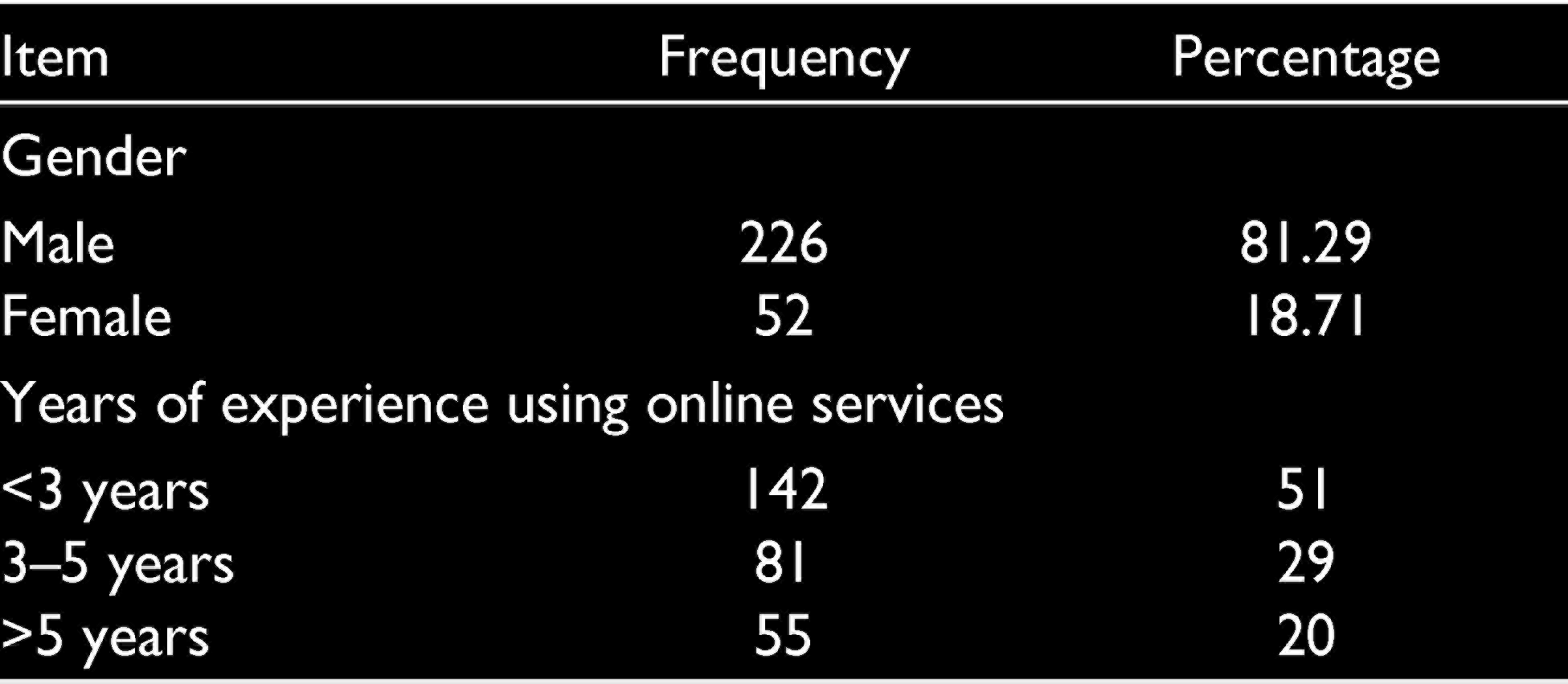
Table 1 shows the distribution of respondents based on gender and years of the online experience. 81.29% of the respondents who have participated in the survey are males and 18.71% of the respondents were females. 51% of the respondents are having experience of fewer than 3 years of using online services is concerned, while 29% of the respondents are having experience in between 3 and 5 years. Around 20% of the respondents are having more than 5 years of experience in using online service in their firms.
Respondents’ Demographics
Data Analysis
Reliability and Validity
Cronbach’s Alpha
Cronbach’s alpha was utilized to test the reliability of the data for all the constructs. The values for all the scales must be above the recommended level of 0.70 (Nunnally & Bernstein, 1994). Utilization of 7-point Likert scale was done in preparing the structured questionnaire. For analysing the information collected, SPSS 20.0 and AMOS 22.0 were used. The latent variable TP has three indicators: relative advantage, security and compliance and its α-value is 0.78. OP has four indicators: firm scope, firm size, higher authority support and innovation acceptance and its α-value is 0.867. EP has three indicators: rivalry pressure, business partners’ pressure and regulatory support and its α-value is 0.857. ETP had four indicators: control, functional creep, reliance on technology, and proscriptive pressure. But proscriptive pressure was removed as it was not satisfying the threshold value of α. Hence, three indicators were considered for the final analysis and the α-value for control, functional creep and reliance on technology is 0.73. Hence, all the values are within the threshold level. Hence, out of 14 indicators, only 13 were considered under the three constructs for further analysis and retention in the model because of reliability.
Exploratory Factor Analysis
The first step of the EFA was to evaluate the appropriateness of the sample size. SPSS 20.0 was utilized for EFA. The correlations between its items had been inspected utilizing Bartlett’s test of sphericity (Hair et al., 2010). Principal axis factoring was performed to identify meaningful bias and express the same qualities. For the interpretation of initial results, Promax rotation has been utilized, and there exists correlation within factors (Tabachnick & Fidell, 2007). With this test, the statistic had generated that should have been significant (p < 0.05) for EFA has been considered as an appropriate technique (Hair et al., 2010). Table 2 shows the KMO and Bartlett’s test output.
KMO and Bartlett’s Test
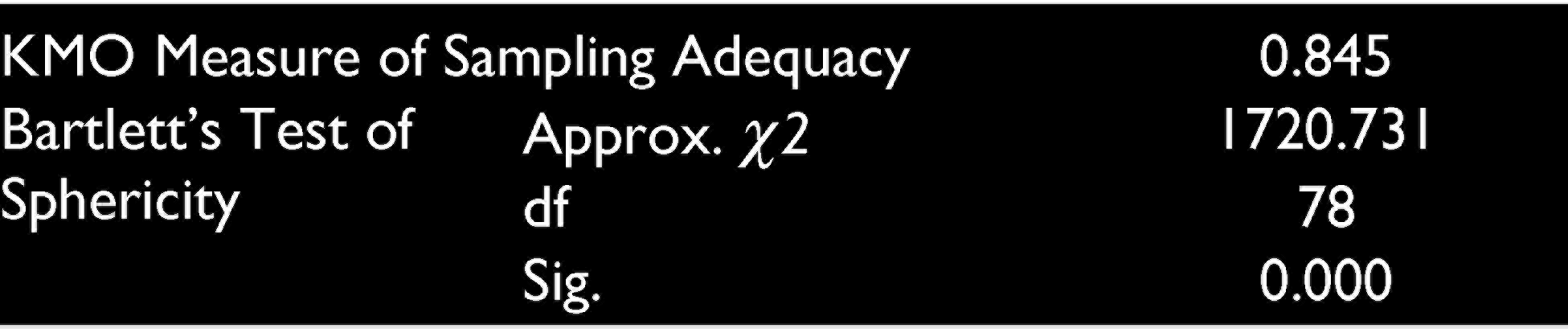
As a result, Kaiser–Meyer–Olkin (KMO) had been utilized to quantify whether those items are sufficiently correlated and to determine whether a factor analysis could be performed. KMO value for the current study is 0.736. The minimum level set for this statistic is 0.60 (Hair et al., 2010). The significant value is 0.000, which is less than 0.05, that is, the probability value level acceptable. Meyers et al. (2013) stated that the variance that has been accounted for its factor needs to meet the lower limits by 50%. The extraction method used was principal axis factoring. Only the eigenvalues which have values greater than 1 were extracted, as it explains the maximum variance. For the components, the percentage of total variance explained by rotation sum of square loadings is component 1 (19.041%), component 2 (15.926%), component 3 (13.183%) and component 4 (12.298%). The cumulative percentage of total variance explained by all three components is 60.448%.
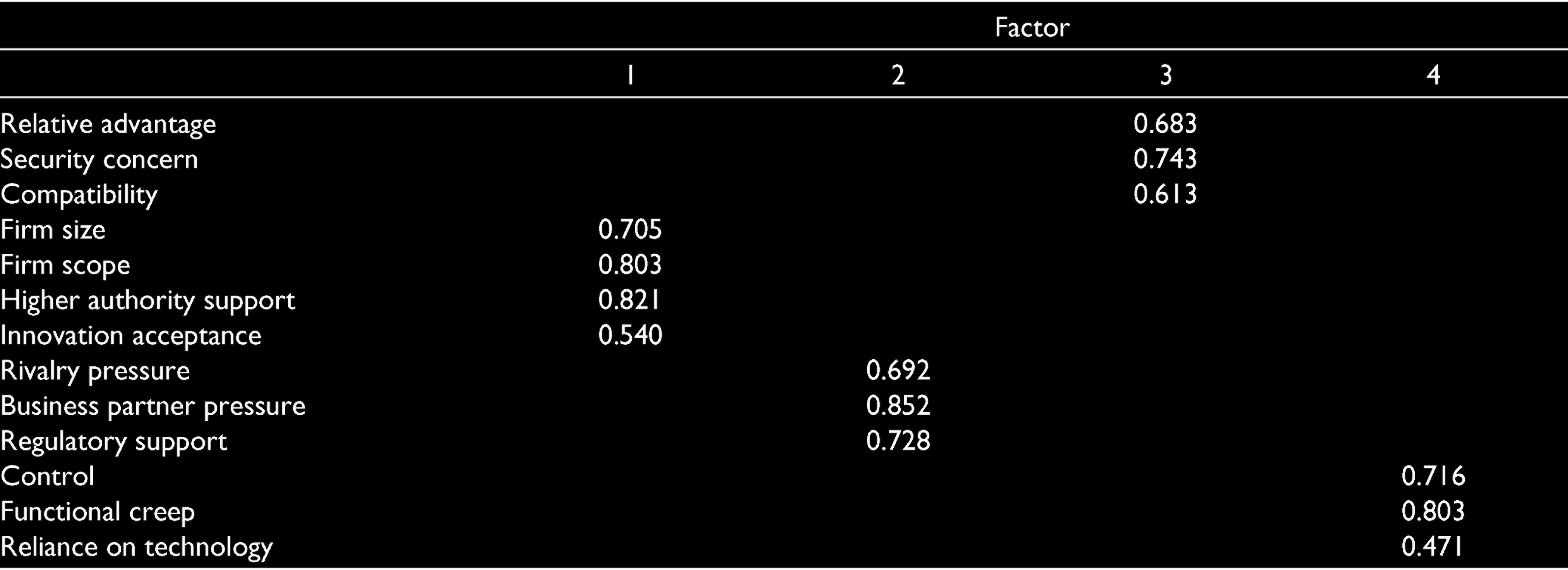
The rotated component matrix is important for interpreting the results of the analysis which is shown in Table 3. Rotation helps in grouping the items, and each group contains more than two items at least, which simplifies the structure. Hence, this is the goal of rotation. In this study, we have achieved it. This helps identify the cross-loadings on more than one group and then it can be corrected by removing those items which are cross-loaded. In this study, the loadings having less than |0.40| are suppressed because loadings more than |0.40| are typically considered high. So, in the end, we achieve a simple structure. Thirteen total variables were grouped under three different components. The rotation method used was Promax rotation. Firm size, firm scope, higher authority support and innovation acceptance are grouped under the first component with values of 0.705, 0.803, 0.821 and 0.540, respectively. Rivalry pressure, business partners’ pressure and regulatory support are grouped under the second component having values 0.692, 0.852 and 0.728, respectively. Relative advantage, security and compliance are grouped under the third component having values 0.683, 0.743 and 0.613, respectively, and control, functional creep and reliance on technology are grouped under the fourth component having values 0.716, 0.803 and 0.471, respectively. These 13 variables have been retained in the model while running it in AMOS 22.0 for getting the model fit measures.
Rotated Factor Matrix
CFA was performed in the next stage; here constructs identified from the literature survey can be tested and how well the variables represent the constructs. SEM was used for testing the model fit of the proposed research model (Byrne, 2010). At that point when their instrument shows the normal structures inside, this could have been demonstrative to construct validity (CV) (Moerdyk, 2009) and, explicitly, factorial validity.
CFA Results
To test the hypothesis, CFA was used (Byrne, 2010). AMOS 22.0 was utilized for this study because of its powerful graphic representations and user-friendly interfaces. The results of the model are shown here. Figure 1 represents the CFA, the latent variables, their indicators and a dependent variable. There are four latent variables. The latent variables along with its indicators are as follows. TP has three indicators: relative advantage, compliance, and security; OP has four indicators: firm size, firm scope, higher authority support and innovative acceptance; EP has three indicators: rivalry pressure, business partners’ pressure and regulatory support; ETP has three indicators: control, functional creep and reliance on technology.

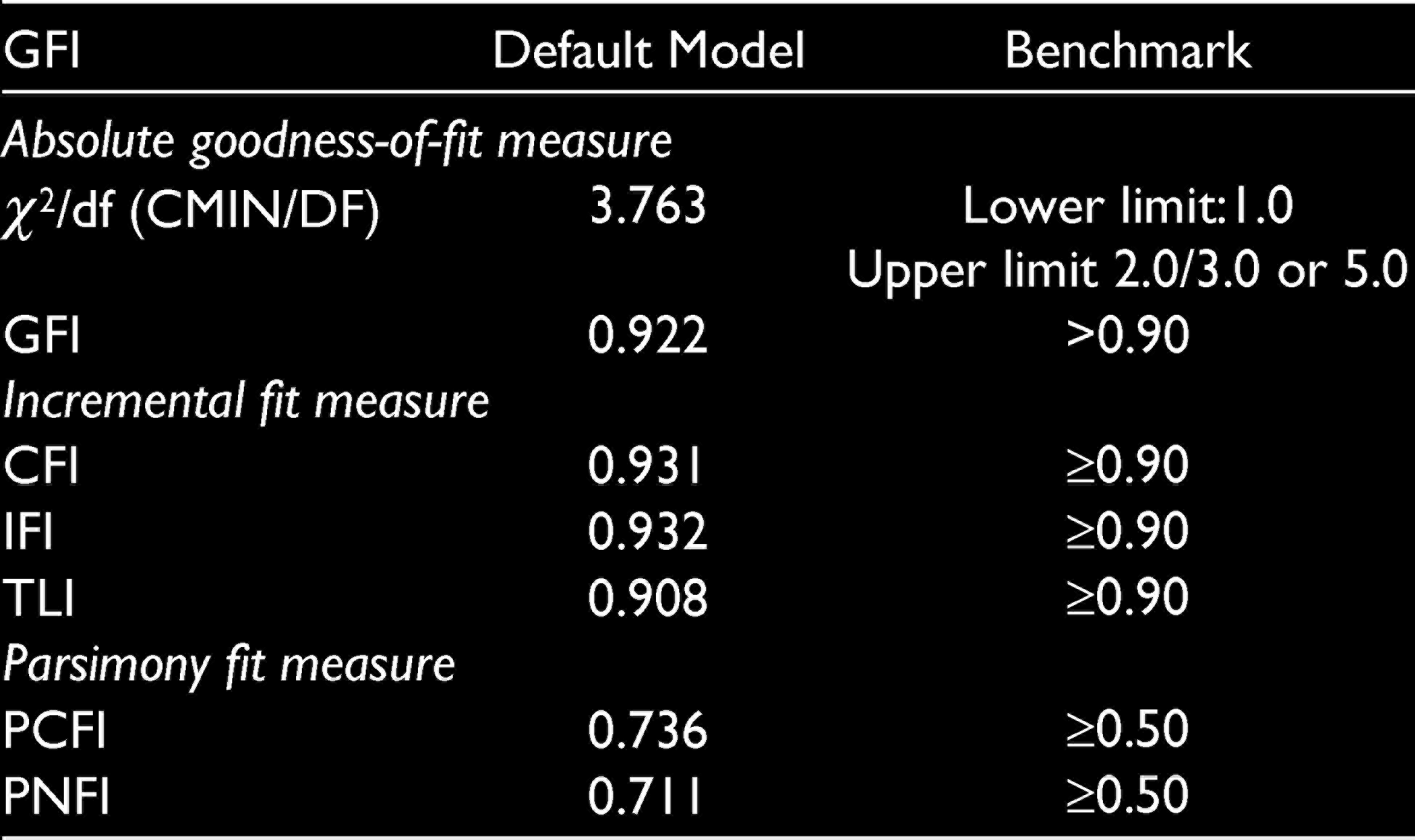
The model fit measures for CFA is shown in Table 4. The goodness-of-fit indices (GFI) is 0.922; comparative fit index (CFI) is 0.931; Tucker–Lewis coefficient (TLI) is 0.908; incremental fit index (IFI) is 0.932; parsimony comparative fit index (PCFI) is 0.736; and parsimony normed fit index (PNFI) is 0.711 is acceptable within the threshold level (Byrne 2010). Hence, the final model was developed by inserting the dependent variable along with its indicators in the next step to get the model fit.
Model Fit Measures for the CFA
Construct Validity
CV is the degree to which a test quantifies the idea or develop that it is expected to quantify. No cut-off characterizes CV (DeVellis et al., 2003). The primary goal of the current study is analysing structural components, a CV that includes investigation of internal connections within items or subscales speaking to a specific measure, utilizing various statistical techniques as correlations, EFA, CFA and reliability.
Composite Reliability
Composite reliability (CR) was also measured for all the components. It is measured for internal consistency reliability because of its ability to provide better results (Henseler et al., 2009). The construct TP has a CR value 0.721; the OP has a CR value of 0.813; the EP has a CR value of 0.803; and the ETP has a CR value of 0.710. All the four constructs’ CR values are >0.7, which indicates that the CR measures are reliable (Henseler et al., 2009).
Convergent Validity
It is measured with the help of the average variance extracted (AVE). According to Fornell and Larcker (1981), AVE > 0.5 for the convergent validity. Table 5 represents AVE values for the constructs. All the values are greater than 0.5, which satisfies convergent validity for all the constructs. This means that the indicators of all the four constructs converge to their respective constructs because of correlation.
Construct Correlation and AVE

Divergent or Discriminant Validity
To calculate this validity, Fornell and Larcker (1981) suggested that AVE of the construct must be more than square of correlation between that construct and the other constructs. Table 4 represents the values for construct correlation and AVE. The variance extracted and squared correlation for TP and OP is 0.488 and 0.204, respectively; TP and EP is 0.518 and 0.281, respectively; TP and ETP is 0.451 and 0.106, respectively; OP and EP is 0.544 and 0.268, respectively; OP and ETP is 0.477 and 0.226, respectively; EP and ETP is 0.506 and 0.116, respectively. Hence, the value of variance extracted is more than the squared correlation value (Cable & DeRue, 2002). As a result, divergent or discriminant validity is satisfied. This means that all the four constructs are not correlated and explains different facts.
Hence, both the validity parameters have been established which is required for excellent CV.
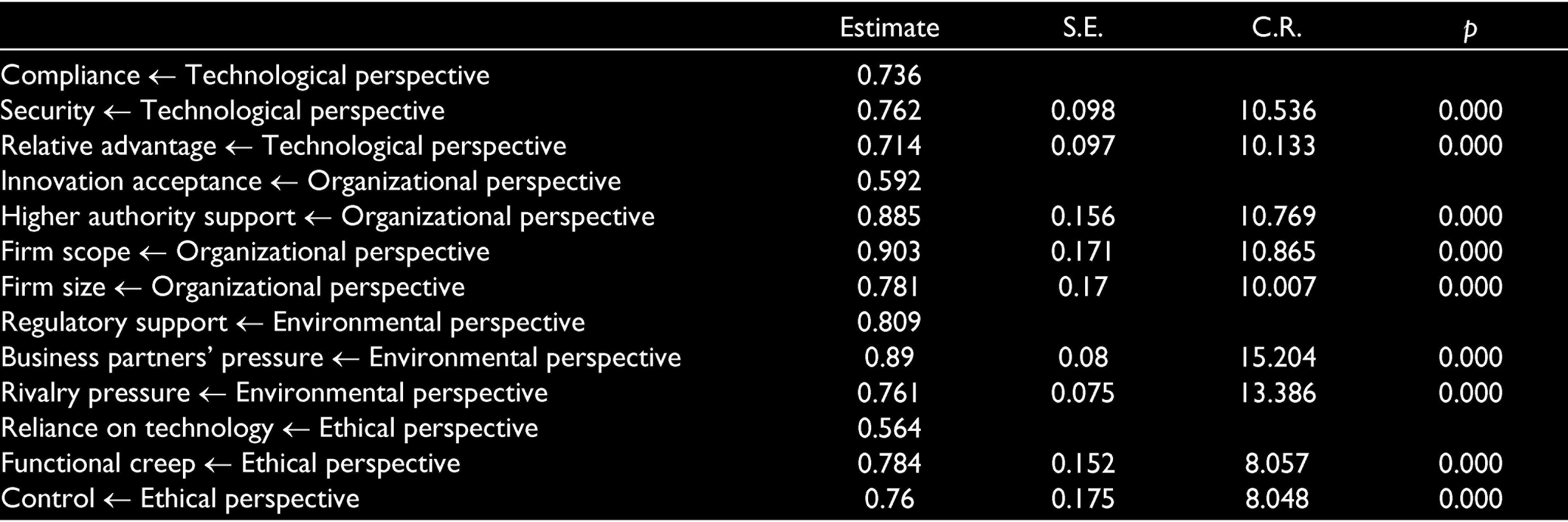
Table 6 shows the path analysis results for CFA. The estimate loadings are above the range of 0.50 (Hair et al., 2010), and the standard errors are less than ±2.5 which is with the threshold level. The critical ratios are greater than 1.96, as per Hair et al. (2010). The p-values are 0.000 which is less than the threshold of 0.05. The loadings are statistically significant. Hence, the conditions are satisfied and we can go for building the final model.
Path Analysis Result for CFA
Structural Model and Testing of Hypothesis
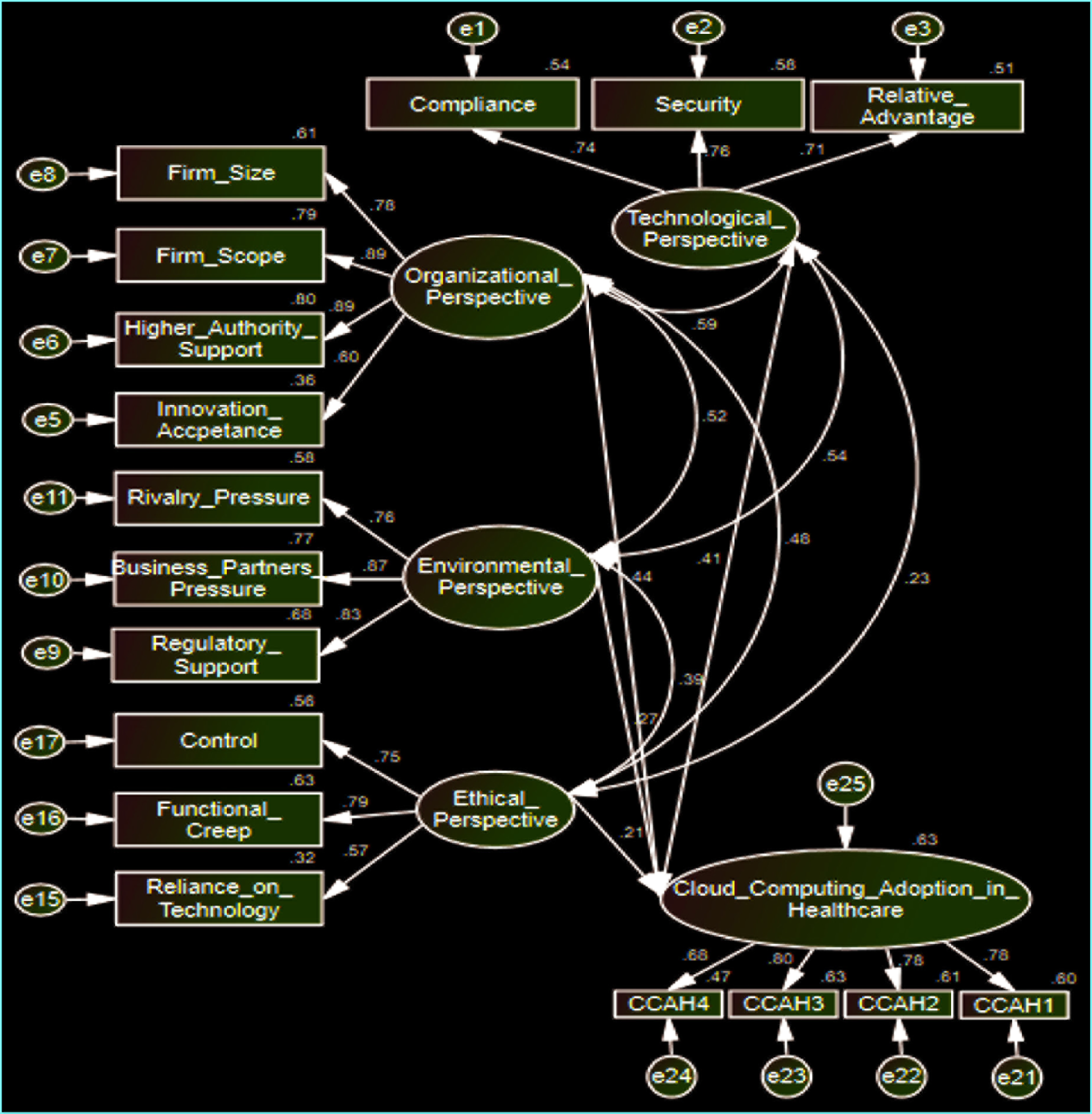
To test the hypothesis, SEM was used (Byrne, 2010). AMOS 22.0 was utilized for this study because of its powerful graphic representations and user-friendly interfaces. The results of the model are shown here. Figure 1 presents the final model, the latent variables, their indicators and a dependent variable. The latent variables along with its indicators are as follows. TP has three indicators: relative advantage, compliance and security; OP has four indicators: firm size, firm scope, higher authority support and innovative acceptance; EP has three indicators: rivalry pressure, business partners’ pressure and regulatory support; ETP has three indicators: control, functional creep and reliance on technology. The dependent variable is CCA in healthcare with indicators CCAH1, CCAH2, CCAH3, and CCAH4.
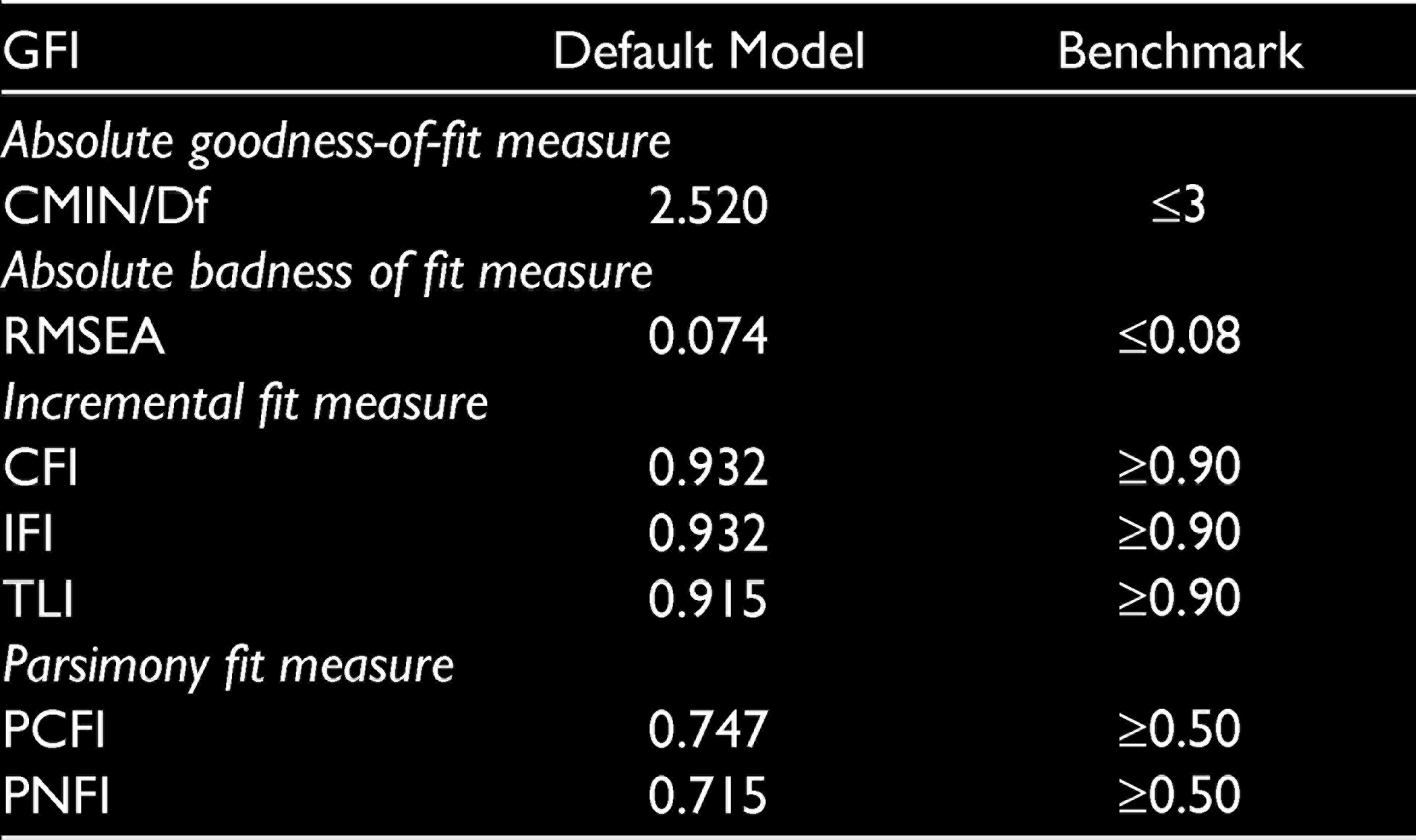
Table 7 shows the model fit values and fit indices. The value of chi-square is 256.949, and the degree of freedom is 84. The estimations of absolute fit indices are: CMIN/Df 2.520, where CMIN represents the chi-square value and Df represents the degree of freedom, and the value is less than 3, which is the accepted threshold value (McIver & Carmines, 1981). Root mean square error of approximation (RMSEA) value is 0.074 which is within the threshold value of 0.08. The CFI is 0.932; IFI is 0.932; TLI is 0.915; PCFI is 0.747; PNFI is 0.715 are having values in the threshold level and is acceptable (Byrne, 2010). Figure 2 shows the SEM output generated after analysis in AMOS 22.0.
Final GFI for the Structural Model
Hence, the supported indicators for the four constructs are: relative advantage, security, compliance, firm size, firm scope, higher authority support, rivalry pressure, business partners’ pressure, regulatory support, control, functional creep and reliance on technology.
Table 8 shows the structural model results. The result demonstrates that the three hypotheses are supported by the p-value (Hair et al., 2010). Hence, constructs TOEE perspectives have a positive impact on CCA in healthcare. The square multiple correlations (R2) helps measure how well a regression line estimates the real data points between 0 and 1, which states how well one variable is predicting another (Hair et al., 2010). The more the value closer to 1, the better is the model’s ability to predict that technology (Kline, 2015). The proposed model is able to explain 63% of the variance of CCA.
Structural Model Results

Discussion
The primary reason for the current study was to decide whether the elements recommended by the TOEE framework impacted CCA in Indian healthcare firms. The consequences of the study showed that the four components suggested by the framework performed a job in the choice of CCA in different Indian healthcare firms. The outcome of the current study will definitely contribute to empirical validity to the theory and managerial implications for the determined constructs for CCA in healthcare.
The current study found that the TOEE perspective plays a significant role in CCA in Indian healthcare firms. The latent variable TP consists of three indicators: relative advantage, security and compliance. All three indicators contributed significantly towards the latent variable TP. RA’s significance in CCA is rational with the prior study done (e.g., Low et al., 2011; To & Ngai, 2006; Wang et al., 2010). The reason being Indian IT has become advanced in the last decade and as a result, many experts are available in the nation itself who can help transform the firms utilizing traditional technology to advance IT like CC for better performance and efficiency. Relative advantage is a significant contributor in the current study for CCA in healthcare also. Security additionally had a critical effect on CCA and this is likewise in concurrence with surviving general research perspectives (e.g., Chebrolu, 2011; Schneider & Sunyadev, 2016; Zissis & Lekkas, 2012). But in the case of healthcare, security is different as it mainly focuses on the manipulation of patient record or medication details (Sultan, 2014). Hence, manipulation of medications prescribed for patients may result in bad service quality and other medical errors. So, security plays an important role in gathering healthcare information for patients. The earlier investigations stressed the significance of security in the acceptance of a new development which consistent with the current findings. The study was done by Low et al. (2011), and Senyo et al. (2016) state that compliance is an insignificant contributor towards CCA in the general context. Prior studies (e.g., Jeyaraj et al., 2006; Oliveira & Martins, 2010; Schneider & Sunyadev, 2016; Wang et al., 2010) brought up compliance as a critical contributor for selecting cloud. In the case of healthcare, compliance will play an important role because it provides treatment to patients. CC is a compatible technology and will help in many ways if adopted in the healthcare segment as it has given in different sectors like service, manufacturing, education, and so on (Senyo et al., 2016). Also, the current study got enough evidence from the analysis and prior studies that compliance is a significant contributor towards the CCA in Indian healthcare firms and it contributed significantly towards the overall model fit. Also, in the final structural model, the TP and CCA in healthcare were supported (β = 0.41, p = 0.000) in the current study. As a result, these three indicators also contribute significantly to the overall model fit. Hence, there was no statistical evidence to reject the first hypothesis.
The latent variable OP consists of four indicators: firm size, firm scope, higher authority support and innovation acceptance. All the four indicators contributed significantly towards the latent variable OP. According to Rogers (2003), firm size is one of the critical components for the innovator profile. Pan and Jang (2008) state that the larger size firms have more inclinations to receive new innovative achievements, especially because of their predominant flexibility, aptitude and risk-taking capacity. As per a recent study by Senyo et al. (2016), firm size and firm scope are not significant contributors for CCA. According to Vahtera (2008), various studies are uncovering a positive connection, while different investigations report a negative relationship. It is a fact that bigger firms will have better skills, assets, finance and experience to face any disappointments more than little firms. Regardless, more diminutive firms can be progressively versatile and creative due to their size and lesser measurements of services. Initially, CC was more alluring to SMEs (Sultan, 2014), and late industry reports recommend that bigger firms have a greater probability to embrace cloud administrations than littler associations. The findings are similar to prior findings (e.g., Dholakia & Kshetri, 2004; Low et al., 2011; Pan & Jang, 2008) as if a firm is large and has a broader scope of operations, then it will have a greater need and as a result, will be more flexible in adopting CC especially if it is a healthcare firm. The reason being the healthcare firms are emergency service providers and the staff and doctors will always try to save the life of patients and try to cure them. The significance of higher authority support is reliable with different studies (e.g., Alshamaila et al., 2013; Dholakia & Kshetri, 2004; Low et al., 2011; Pan & Jang, 2008) as it has been identified as a critical element in technology acceptance. The higher authorities, if have a medical background, will be able to understand the needs and requirement of medical and business needs. Prior empirical studies demonstrated that the healthcare firms which are having medical background administrators have better service and efficiency and as a result, the patients are satisfied (Goodall, 2011). Hence, higher authority support has an impact on CCA in healthcare as it will help in service improvisation. Business process reengineering and designation of assets might be required because of an innovation acceptance, in this way; top management’s backing is required. Along these lines, higher authority support is fundamental in the CCA in healthcare. Innovation acceptance is another factor that had a huge effect on the appropriation of CC from a developing nation point of view. Its essentialness is per past studies (e.g., Oliveira & Martins, 2010; Senyo et al., 2016; Zhu et al., 2003). The reason the healthcare staff and other employees are being trained is for utilizing these advanced technologies like other segments. They acknowledged that once they fully get acquainted with these technologies, it will reduce their manual efforts which they are facing at present. Hence, IA is a critical factor that has shown an impact on CCA in healthcare. Also, in the final structural model, the OP and CCA in healthcare were supported (β = 0.44, p = 0.000) in the current study. As a result, all four indicators have contributed significantly to the model fit. Hence, the second hypothesis also could not be rejected.
The latent variable EP consists of three indicators: rivalry pressure, business partners’ pressure and regulatory support. All three indicators contributed significantly towards the latent variable EP. Prior studies (e.g., Oliveira & Martins, 2010; Pan & Jang, 2008; Senyo et al., 2016; Wang et al., 2010) also state that significant determinants in technology adoption are competitors and trading partners. The discoveries in this research additionally affirm this position. Be that as it may, this discovery is banter to discoveries in which rivalry pressure was detected as an insignificant contributor to CCA from the perspective of a prospered nation (Alshamaila et al., 2013). This demonstrates firms to react diversely to CCA from developing and developed contexts. CCA may give healthcare firms a better approach to work and outflank their rivals. Then again, business partners’ pressure may drive trade to adopt a development with the end goal to keep up a helpful association with these accomplices. Hence, rivalry pressure and business partners’ pressure have a significant impact on CCA in healthcare. The verdict on regulatory support is steady with outcomes from past investigations (Kung et al., 2015; Makena, 2013; Nkhoma & Dang, 2013; Zhu et al., 2003). However, according to Senyo et al. (2016), regulatory support is not a significant contributor. In the current study, regulatory support is a critical element because it is important to have the nations’ governmental involvement while adopting any advanced technology because of various security reasons and data theft issues. The reason being when government involvement is there, then it may help in the case of any bad circumstances. Also, CC technology is still not matured fully and but then to increase huge thought for strategy control, particularly in developing nations. Hence, regulatory support is a critical factor that has shown an impact on CCA in healthcare. Also, in the final structural model, the EP and CCA in healthcare was supported (β = 0.27, p = 0.000) in the current study. As a result, all three indicators have contributed significantly to the model fit. Hence, the third hypothesis could not be rejected.
The latent variable ETP consists of three indicators: control, functional creep and reliance on technology. Proscriptive pressure was removed due to a lesser value of Cronbach’s alpha. As CC entails outsourcing of data to the third-party service providers, the direct control over the data is lost by the user. It may lead to many risks like unauthorized access, infrastructure failure, and so on. So, control is one of the important factors which lead to CCA. Another threat that comes is functional creep which means data stored for one purpose may become useful for another different purpose over some time (Liu et al., 2016; Timmermans et al., 2010). The data stored in the cloud can be hacked by hackers, as a result reliance on technology is an important factor. There may be a chance that the involvement of a cloud provider. Consumers at that point need to confide in the cloud provider that the specific individual data will not be uncovered. However, in addition to the fact that the diverse CC providers are likely being conclusive on protection, to the clients it will not generally clear with which the provider is managing. In the CC, different services have increasingly become intertwined: a facilitated use of one organization, for example, may be based on an improvement/arrangement system of another. As per a prior study (de Bruin & Floridi, 2017), proscriptive pressure is not a significant contributor in CCA and the current study of healthcare also it is the same. Hence, it is not considered in the model building. Also, in the final structural model, the ETP and CCA in healthcare was supported (β = 0.21, p = 0.000) in the current study. As a result, all three indicators have contributed significantly to the model fit. Hence, the fourth hypothesis also could not be rejected.
Ethical issues are very crucial nowadays, especially because of daily advancement in technologies. The current study considered various ethical parameters along with the existing TOE parameters. As CC is a very new technology and still is in the developing phase, there is a need to consider the ethical parameters before adopting it, especially in the healthcare sector. The reason being the patients’ data which are available in healthcare firms or hospitals are very confidential and they do not like to discuss their health-related issues in front of the whole world. As a result, the patients’ needs to have faith in the new advanced technology that their identity or health-related data or information are hidden from society. Hence, patients should have a reliance on these new technologies, and their medical data should not be used for any other purpose without taking their opinion. So, in the current study ethical issues has been discussed and also during analysis all the four factors have been considered together for running the model and it has been found empirically that the model has shown a good fit and satisfying all the validity measures. This study is the first to implement a statistical method in an ethical context along with the other three perspectives of CCA in Indian healthcare which is the unique contribution. Also, the current study has given empirical evidence by adding a new perspective which can help in providing a new research direction for the future which is a complement to the prior TOE framework.
Contribution to Research and Practice
The current study has contributed significantly to research and practice. When we consider research, it has made a significant contribution to the knowledge of CC by testing and by validating the TOEE framework concerning Indian healthcare firms’ perspective which is a prospering country. Also, empirical evidence provides that this study cannot be studied only from just technological or organizational or environmental perspectives, as the output states the significant impact of ethical factors also in CCA which is a compliment to the prior TOE framework. This study also bridges the gap on CC among prospered and prospered nation. The study highlights the ignored ETPs and has provided empirical validity for a healthcare firm while adopting CC technologies.
This study draws the attention of practitioners to the critical factors impacting CCA in Indian healthcare firms. Indian healthcare firms who are planning to adopt CC should consider the sub-components relative advantage, security, compliance, firm size, firm scope, higher authority support, rivalry pressure, business partners’ pressure, regulatory support, control, functional creep and reliance on technology. This study likewise exhibits that making a great ICT condition will have a positive effect on CCA in healthcare firms. The empowering condition as enactment, ICT policies and infrastructures will engender the CC agenda. The current study stressed the importance of regulatory support and various ethical parameters like reliance on technology, control and functional creep before CCA in Indian healthcare firms. Hence, the authorities in the healthcare firms will get an understanding and positive vibe in CCA in their centres or firms which will provide benefits in the long-run.
Managerial Implications
This study adds to rehearse by illustration consideration of managers or decision-makers to the essential factors of CCA. The benefits of CC over existing or traditional system upgrade association with clients and partners and encourage managers to better frame their administration structure and strategies. This investigation endeavours to test the recommended TOEE model associated with one another and fundamentally impact the choice of Indian firms for CCA. The managers and decision-makers need to concentrate on budgetary and technological assets, for example, physical frameworks, elusive information and procuring employees with IT aptitudes. Likewise, the managers need to comprehend that utilizing a particular IT workforce with ranges of abilities over the regular IT condition and the cloud stage and developing vital undertakings to help business development empower CCA. They also need to consider the significant ethical factors, that is, control, functional creep and reliance on technology discussed before CCA in their firms. The reason being when a firm migrates to this new technology of cloud, the functionality varies from the traditional system which they were using and as a result they need to consider all the significant factors before migrating or adopting CC. As the managers are the decision-makers for the firms, they will have to consider the pros and cons of CCA in healthcare firms. With the assistance of this examination, officers can get to whether the assistances are in reality with their frameworks and how complex is the assistance to complete and get it.
Conclusion
The current study helps in determining and understanding the factors of CCA in Indian healthcare firms. Hence, the objective of the current study was achieved. In terms of research, it has contributed to the body of knowledge on CC by testing and validating the TOEE framework from an Indian healthcare perspective which is a prospering country. Ultimately, this investigation bridges the ostensible writing gap on CC among prospering and prospered nations. The study considered ethical perspectives also along with technological, organizational and environmental perspectives. These four constructs were validated using the SEM approach. The TP includes reliance on technology, security and compliance; OP includes firm size, firm scope, higher authority support and innovative acceptance; EP includes rivalry pressure, business partners’ pressure and regulatory support; the ETP includes control, functional creep and reliance on technology. The current study provides an add-on to the theory by utilizing the TOEE framework to recognize critical success factors for CCA in Indian healthcare firms. This study encourages healthcare centres to adopt cloud technology. To access and test the developed model, a quantitative method was utilized for CCA. In the current study, no hypothesis was rejected. This will help the decision-makers by focusing on key factors identified in the current study while CCA in Indian healthcare firms. This study also states that ethical issues are also critical and significant contributor along with technological, organizational and environmental perspectives for adopting any advanced technology like CC.
Therefore, it is suggested that the healthcare firms should consider the significant contributors particularly in the perspective of a prospering nation, especially to all the ethical considerations which have been ignored by prior studies and it is complementary to the existing TOE framework.
Scope and Future Recommendations
The current study focused on the healthcare firms of India which is a prospering nation. Hence, similar kind of studies can be further done for other developing countries around the world and this study can be taken as a base for the future. Research works can also be done in a specific sector. Further research is suggested for ethical context along with TOE which has been ignored by other studies because it is also an important factor for adopting cloud technologies. It can be tested in every sector from both prospered and prospering nation perspectives as they have different results.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Annexure I
List of Adapted Scales which are Found from Extant Literatures
| Constructs | Sub-factors | Adapted Sources |
| TP | Security | Zhu et al. (2006), Luo et al. (2010), Wu (2011) |
| Relative advantage | Moore and Benbasat (1991), Ghobakhloo et al. (2011) | |
| Compatibility | Moore and Benbasat (1991), Premkumar and Roberts (1999) | |
| Organizational perspective | Higher authority support | Yap et al. (1994) |
| Firm size | Premkumar and Roberts (1999) | |
| Firm scope | Hitt (1999), Zhu et al. (2003) | |
| Innovation acceptance | Oliveira and Martins (2010), Ifinedo (2011) | |
| Environmental perspective | Rivalry pressure | To and Ngai (2006) |
| Business partners’ pressure | Makena (2013) | |
| Regulatory support | Chong and Ooi (2008) | |
| Ethical perspective | Control | Grimes et al. (2009) |
| Functional creep | Gholami et al. (2017), Timmermans et al. (2010) | |
| Reliance on technology | Grimes et al., (2009) Chang and Ramachandran (2016) | |
| CC adoption | Our firm will take steps in adopting cloud technology | Premkumar and Roberts (1999), Yoon (2009) |
| Our firm intends to adopt CC | Premkumar and Roberts (1999), Yoon (2009) | |
| I would not hesitate to recommend adopting CC | Premkumar and Roberts (1999), Yoon (2009) | |
| I feel comfortable to recommend CC for my firm | Premkumar and Roberts (1999), Yoon (2009) |
Questionnaire
Please rate the following factors for your firm on the scale of 1–7: 1 for strongly disagree, 2 for disagree, 3 for partially disagree, 4 for neutral, 5 for partially agree, 6 for agree and 7 for strongly agree.