
Abstract
Peri-implant health is regarded as existence of adequate bone support around implants which is clinically characterized by the absence of erythema, bleeding on probing, swelling, and suppuration. Implant survival is evident by presence of implant and fixed prosthesis independent of biological and technical complications. Peri-implantitis is signified by following signs like presence of bleeding and/or suppuration on probing, increased probing depth and presence of bone loss beyond implant crest rather than initial bone remodeling. Various literatures have discussed about the classifications of peri-implantitis and peri-implant mucositis and established some criteria for the diagnosis and treatment of these implant-related complications. Periimplantitis are classified mainly by case definitions, bone defects, peri-implant soft tissue changes, peri-implant probing depth and radiographic bone loss. To simplify the classification based on clinical findings, this novel classification system aims to address the implant thread exposure and distinguished it based on extent and number of thread exposure consistent with percentage of peri-implant bone loss. This classification also focused on categorization based on interproximal implant thread exposure and treatment options for each class.
Introduction
Peri-implant disease is a biological complication associated with dental implants, leading to inflammatory conditions in the soft tissues and bone surrounding the implants and their restorative components. These conditions arise due to biofilm formation containing harmful microorganisms. The two primary forms of peri-implant disease are peri-implant mucositis and peri-implantitis. The diagnosis of peri-implantitis requires the presence of the following criteria:
Inflammatory changes in peri-implant soft tissues, with bleeding on probing and/or suppuration. Increasing probing pocket depths. Progressive radiographic bone loss observed after one year of implant-supported prosthesis delivery. Radiographic evidence of bone loss ≥3 mm and/or probing depths ≥6 mm in conjunction with profuse bleeding.
Several cross-sectional studies report the frequency of peri-implant disease to be between 13% and 26%. Peri-implantitis can develop early during follow-up, progressing in a non-linear and accelerated manner. The transition from peri-implant mucositis to peri-implantitis remains unclear, both histologically and clinically.1,2
Albrektsson and Isidor (1994) proposed the following definitions:
Peri-implant mucositis: A reversible inflammatory condition affecting the soft tissues around the implant. Peri-implantitis: Involvement of supporting bone around a functioning dental implant.
3
Over time, different classification systems have been proposed to categorize peri-implant disease based on bone loss progression.
Seventh European Workshop on Periodontics (2011)
4
Peri-implant mucositis: Defined by the presence of bleeding on probing. Peri-implantitis: Characterized by changes in bone crest level along with bleeding on probing. Disadvantage: This classification focuses primarily on clinical signs without considering radiographic assessment for a more comprehensive diagnosis.
2017 American Academy of Periodontology & European Federation of Periodontology 5
Peri-implant conditions were classified into:
Peri-implant health Peri-implant mucositis Peri-implantitis
Disadvantage: This classification does not provide specific thresholds for bone loss or pocket depth, which may lead to inconsistencies in diagnosis.
Proposed Classifications Based on Bone Defect Morphology
Schwarz et al. classification:
6
Intraosseous Class I: Bone defects located at the implant crest. Supra-alveolar Class II: Bone loss extending above the alveolar ridge.
Disadvantage: Lacks detailed assessment of defect severity, which can affect treatment planning.
Spiekermann classification:
7
Class I: Horizontal bone loss. Class II: Key-shaped bone defects. Class IIIa, IIIb: Funnel- and gap-like bone loss. Class IV: Horizontal–circular bone defects.
Disadvantage: This classification does not incorporate functional considerations such as implant mobility or soft tissue involvement
Vanden et al. classification (based on defect anatomy & regenerative process):
8
Closed defects: Characterized by intact surrounding bone walls. Open defects: Defined by the absence of one or more bone walls.
Disadvantage: Lacks statistical validation for clinical and radiographic assessment, making it less reliable for predicting regenerative outcomes.
These classification systems help define the extent of peri-implant disease based on defect morphology, emphasizing the need for three-dimensional radiographic investigations for precise diagnosis and treatment planning. However, each system has limitations, highlighting the need for a more comprehensive and universally accepted classification method.
Jovanovic (1995) classification (based on horizontal bone loss and defect type):
9
Class I: Slight horizontal bone loss with minimal peri-implant defects. Class II: Moderate bone loss with isolated vertical defects. Class III: Moderate to advanced bone loss with broad, circular bony defects. Class IV: Advanced bone loss with broad, circumferential vertical defects and loss of the oral/vestibular bony wall.
Disadvantage: Does not include peri-implant soft tissue involvement, limiting its diagnostic utility.
The biggest drawback of the categorization is that it does not include any etiological aspects, such as bacterial or trauma, and it is a bit confusing and lengthy to read.
Monje et al. (2019) 11 classifications based on defect morphology are as follows: Class I infra-osseous defects, Class II supra-crestal/horizontal defects, and Class III combined defects. Sub-classifications A (buccal dehiscence), B (two to three wall defects), and C (circumferential configurations). The limitations of this classification are investigating the influence of defect morphology upon reconstructive and resective outcomes.
Implant topography acts as a determinant factor in the success of implants which requires further investigation. Implant design has been discussed extensively regarding osseointegration, but only few literatures have inspected its role in disease onset.
Macro- and micro-design of implants determines the implant topography, respectively. The macro design refers to the form of the implant body, as well as the design and number of threads, and is a proven important component for osseointegration as a critical aspect for primary implant stability and perhaps for bone-to-implant contact. 12
Ravida et al. found in a retrospective study that exposed interproximal threads of implants after physiologic bone remodeling may be a distinct risk indicator for incident peri-implantitis, so it should be recognized as an important clinical finding for assessing peri-implantitis. Therefore, when planning implant treatment, it is critical to consider all possible measures to prevent the development of exposed threads. 13
In the above-mentioned classifications, all the factors depend on clinical and radiographical investigations which hinders a practical difficulty for general dentistry practitioners. Hence, this novel classification system for peri-implantitis provides a practical framework that is highly beneficial for clinicians. It is easy to apply in daily practice, offering clear criteria for diagnosis and treatment planning. Its clinically relevant categories ensure consistent communication and decision-making, ultimately aiding in personalized patient care (Tables 1 and 2).
Lang NP et al. Classification Included Treatment Part in Its Classification.

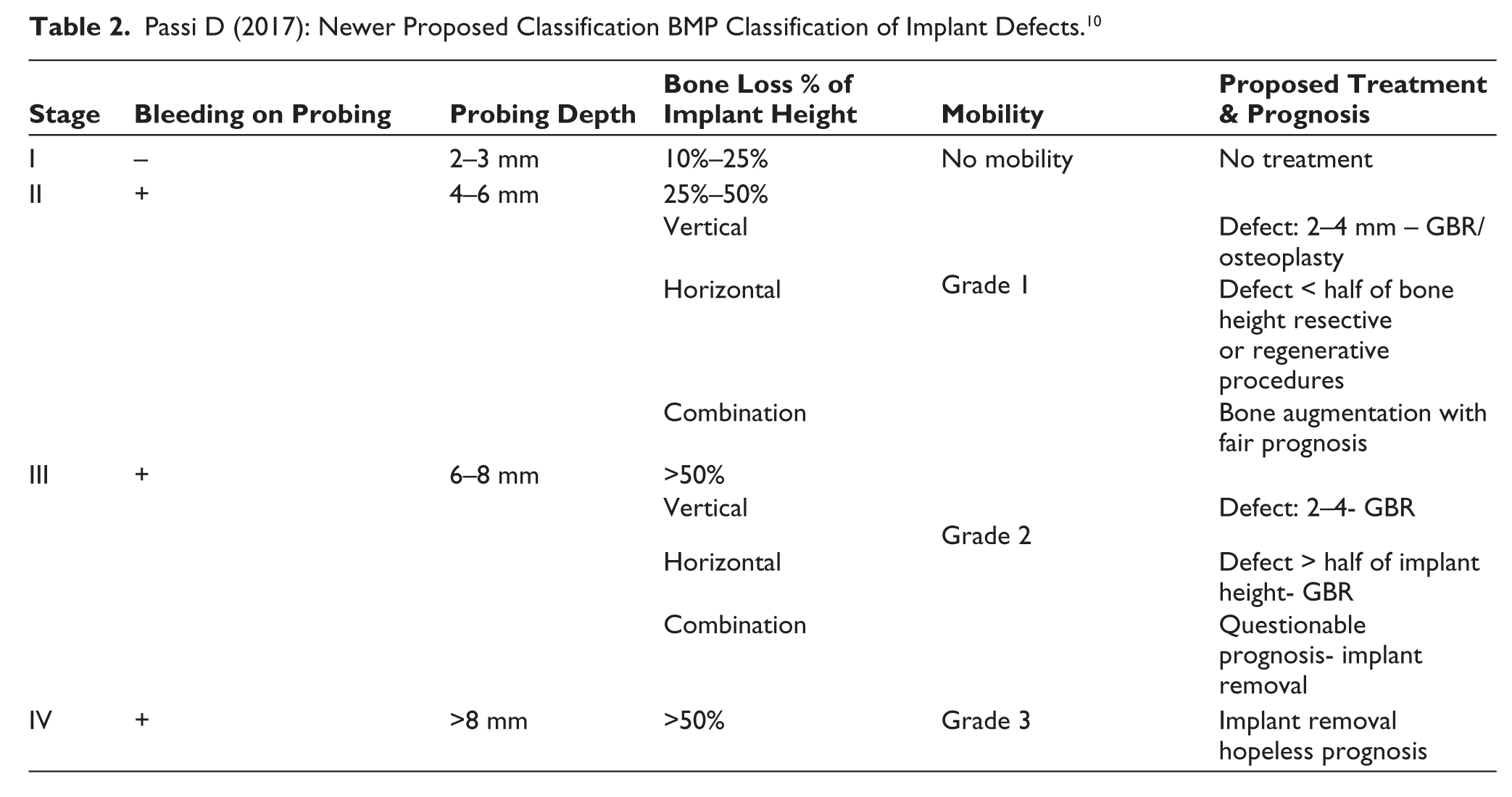
Passi D (2017): Newer Proposed Classification BMP Classification of Implant Defects. 10
Mari’s New Classification System for Periimplantitis
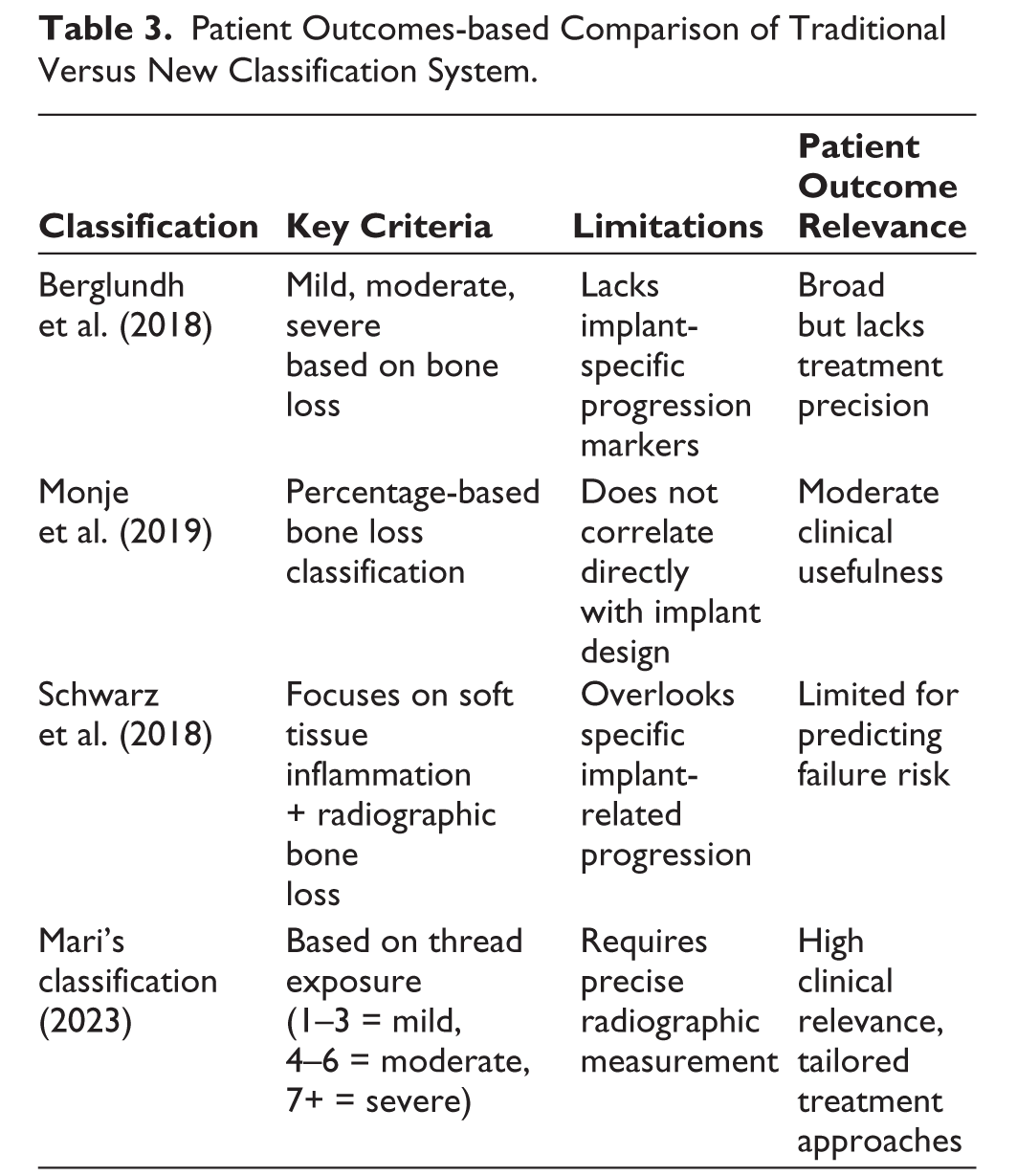
Several existing classifications categorize peri-implantitis based on parameters such as bone loss, probing depth, bleeding on probing, and radiographic findings. Common classifications include (Table 3):
Patient Outcomes-based Comparison of Traditional Versus New Classification System.
Patient outcomes in traditional classifications:
Varying disease progression stages allow for generalized treatment planning. Lacks precision in defining treatment urgency based on implant structure. Does not address the specific relationship between implant thread exposure and disease severity.
Moraschini et al. 16 and Lee et al. 17 have analysed the prevalence of peri-implantitis based on amount and degree of bone loss and design of implants for peri-implant disease.
This new classification aims to consider the above risk factor as diagnostic criteria in classifying the peri-implantitis based on extent of thread exposure which enables clinician ability to classify the disease and discuss it with specialist for patient management and motivation. The classification of periimplantitis is as follows:
Class I (Mild)—Implant exposure of <25% or one to three threads exposure without interproximal involvement (Figure 1).
Class I. Implant Exposure of <25% or One to Two Threads Exposure Without Interproximal Involvement.

Subclass A—with <3 interproximal thread exposure (Figure 2).
Class I Subclass A. Thread Exposure <25% with <3 Interproximal Thread Exposure.

Subclass B—with >3 interproximal thread exposure (Figure 3). 18
Class II Subclass B. Thread Exposure <25% with >3 Interproximal Thread Exposure.

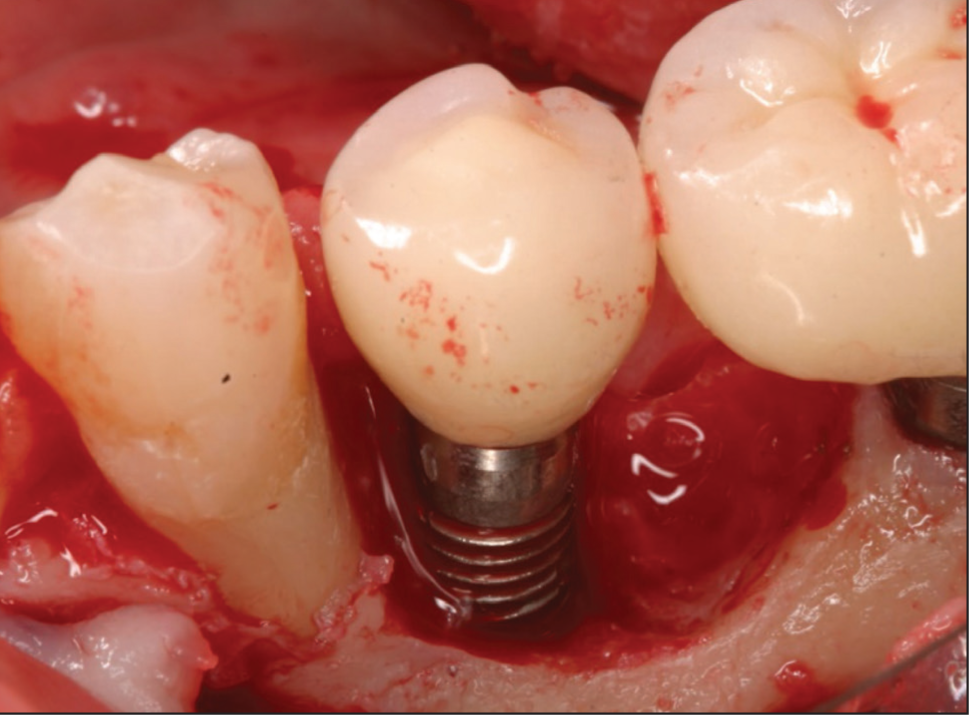
Class II (Moderate)—25%–50% of implant thread exposure or four to six thread exposure without interproximal involvement (Figure 4). 19
Class II. 25%–50% of Implant Thread Exposure or Four to Six Thread Exposure Without Interproximal Involvement.
Subclass A—with <3 interproximal thread exposure (Figure 5). 20
Class II Subclass A. 25%–50% of Implant Thread Exposure with <3 Interproximal Thread Exposure.

Su6bclass B—with >3 interproximal thread exposure (Figure 6).
Class III Subclass B. 25%–50% of Implant Thread Exposure with >3 Interproximal Thread Exposure.
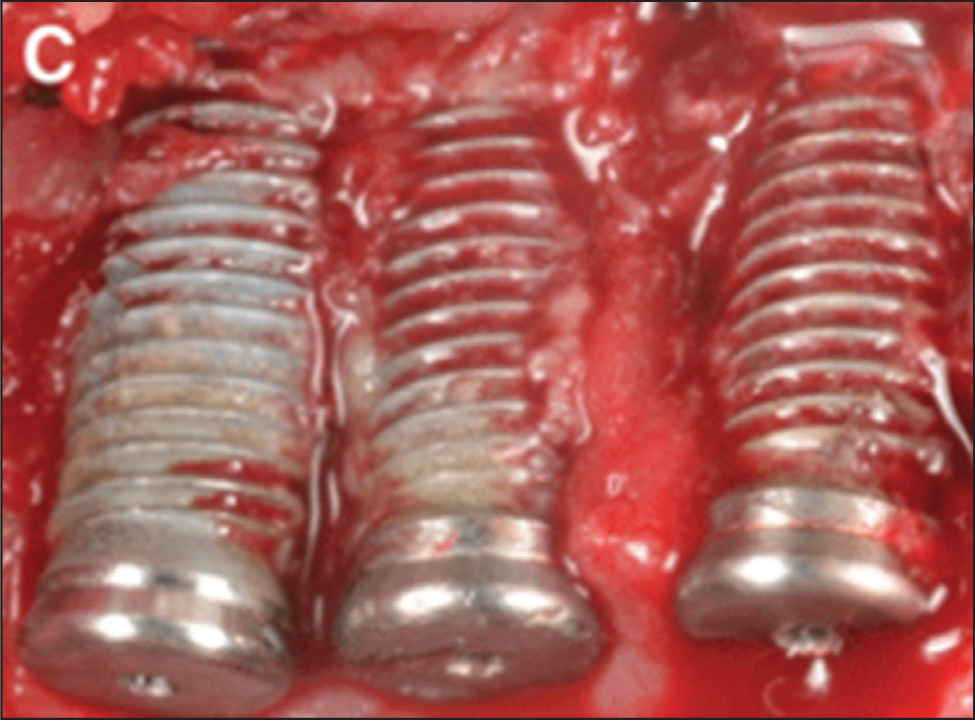
Class III (severe)—>50% implant thread exposure or >6 implant threads (Figure 7). 15
Class III. >50% Implant Thread Exposure or >6 Implant Threads.

Class IV (complete dehiscence)—Complete implant thread exposure (Figure 8).
Class IV. Complete Implant Thread Exposure.
Treatment Options for Various Classes
The treatment options based on severity and extent of implant thread exposure are as follows:
Class I—The nonsurgical phase, which includes debridement by mechanical means, ultrasonic, or laser devices, either alone or combined with antiseptic and/or antibiotic agents. 21
Class I subclass A & B—Non-surgical option in aesthetic zone and surgical non-augmentative treatment of peri-implantitis in aesthetically non-demanding areas based on patient needs and satisfaction. The surgical technique involves performing an access flap for proper mechanical and chemical decontamination of the implant surface. 22
Class II subclass A—Access flap involving decontamination procedures with or without resective approach. Resective surgery aims to eliminate peri-implant pocket and apical repositioning of the flap with or without bone contouring. 23
Class II subclass B—Access flap with resective or regenerative procedure based on wall defect after surgical exposure
Augmentative procedure involves the use of bone fillers with biologically active material or guided bone regeneration (GBR) with the use of barrier membranes. The goal is to initiate re-osseointegration, limit peri-implant mucosal defects, and regenerate bone defects. 24
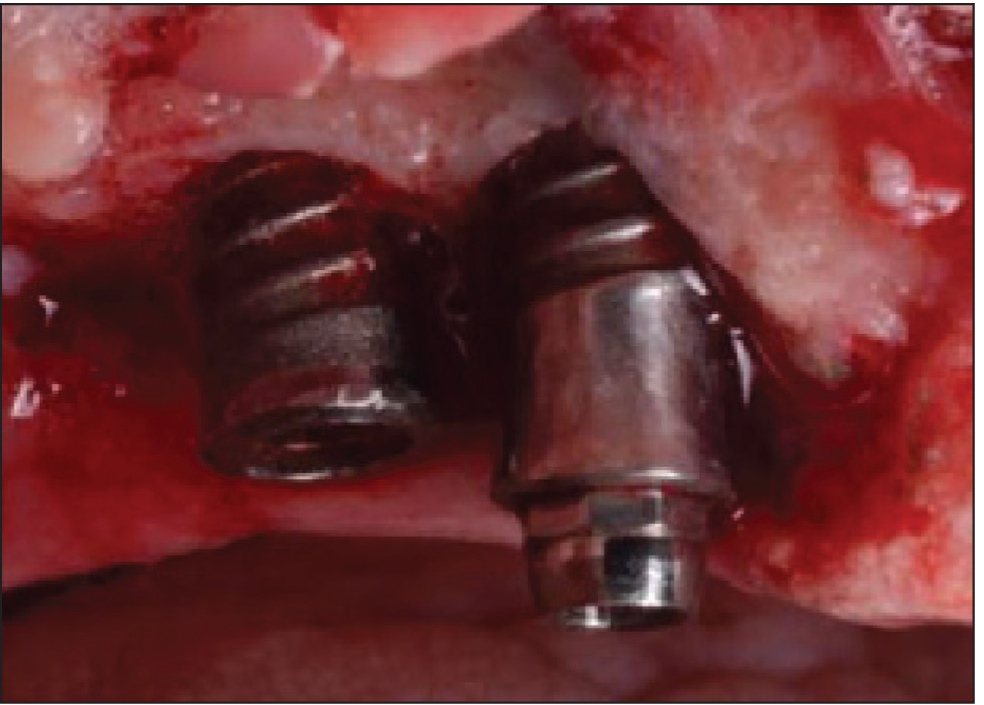
Class III & IV—Explantation: If there is extensive bone loss and the implant cannot be preserved, it must be removed. Based on clinical findings, if the choice has been reached to remove the implant, explantation trephines are available for the implant system in issue (Figure 9). 25
Evidence-based Decision Tree for Managing Peri-implantitis Based on the Extent of Thread Exposure.
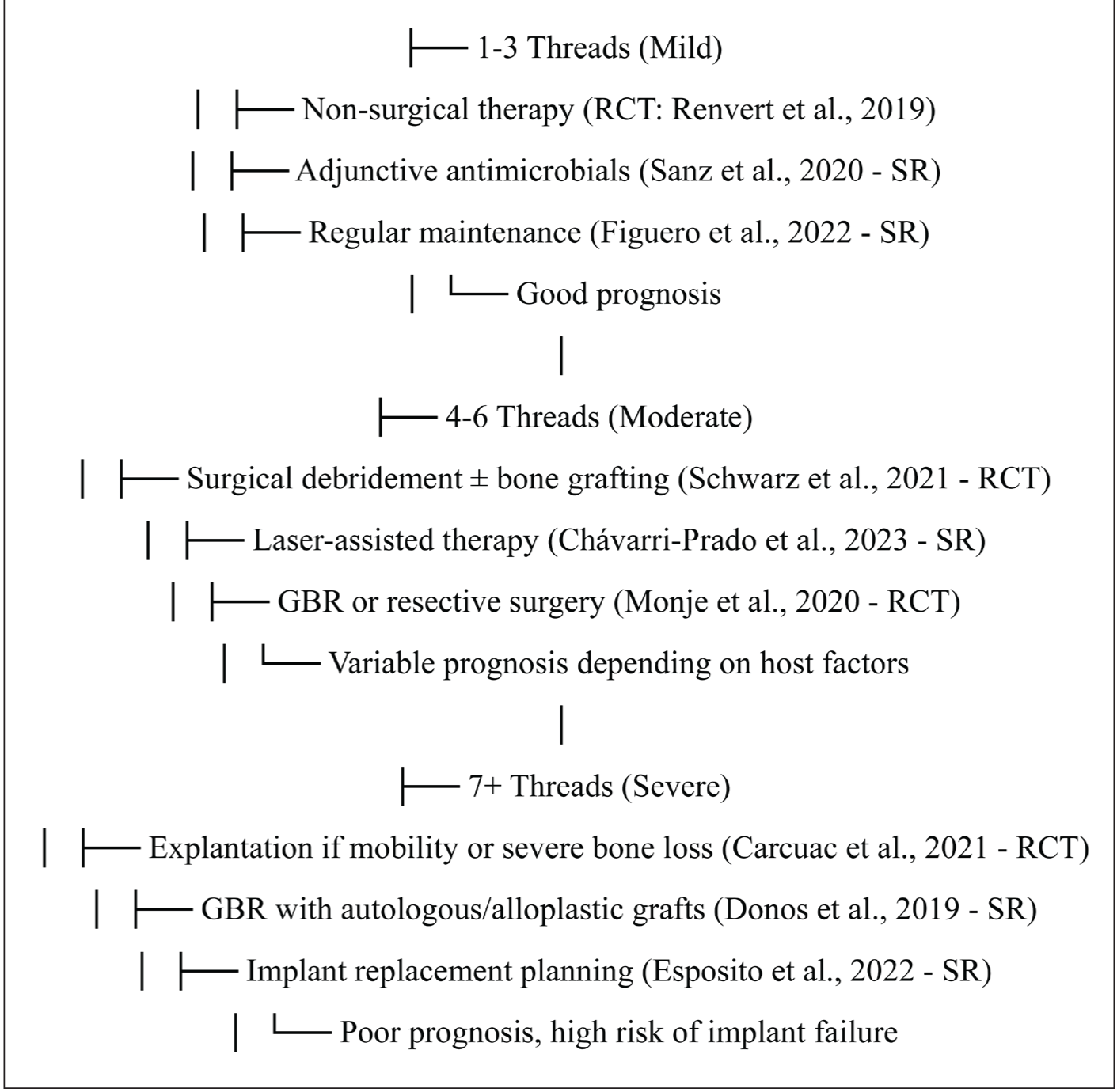
Supporting Evidence from RCTs & Systematic Reviews
Mild (1–3 Threads Exposed)
Non-surgical therapy + mechanical debridement shows significant reduction in inflammation (Renvert et al. 2019, Randomized controlled clinical trial [RCT]). Figuero et al. 2022, Systematic Review reported that antimicrobial adjuncts (e.g., chlorhexidine, minocycline) improve outcomes in early-stage peri-implantitis and that regular maintenance therapy significantly reduces disease progression and implant failure risk. 26
Moderate (4–6 Threads Exposed)
Schwarz et al. (2021, RCT) found that surgical therapy improves clinical attachment and reduces pocket depth compared to non-surgical approaches. Also, laser therapy, when used as an adjunctive treatment, enhances bacterial decontamination and soft-tissue healing. Monje et al. (2020, RCT) demonstrated that GBR combined with resective therapy effectively manages bone loss and stabilizes implants. 27
Severe (7+ Threads Exposed)
Carcuac et al. (2021, RCT) found that severe peri-implantitis cases with more than seven exposed threads have a high risk of failure, often requiring explantation. Mahato et al., in a systematic review, reported that bone regeneration using autografts or alloplasts provides partial bone recovery but does not fully reverse the damage. Evidence concluded that implant replacement strategies achieve better long-term success than attempting to salvage heavily compromised implants.28,29
Limitations
In this classification, the type of peri-implant bone defects is not considered which is an important criterion in deciding the augmentative and non-augmentative procedures. There can be differences in the extent of implant thread exposure after surgical exposure which could influence the treatment plan for peri-implantitis management.
Conclusion
This more succinct categorization facilitates a simpler and more efficient diagnosis of periimplantitis and treatment approach. This categorization may be used in clinical diagnosis to increase speed and clarity and offers a clearer framework for comprehending the consequences of thread exposure in periimplantitis. Subsequent studies may concentrate on improving the subcategories or investigating how this categorization might be used in situations.
Footnotes
Authors’ Contributions
Conceptualization and classification design was given by Ranjith Mari, Drafting categorization, writing and editing was given by Rudhra Kannan, Review was done by all other authors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Not applicable.